Enteral Immunomodulatory Diet (Omega-3 Fatty Acid, γ-Linolenic Acid and Antioxidant Supplementation) for Acute Lung Injury and Acute Respiratory Distress Syndrome: An Updated Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. End Points and Data Extraction
2.4. Quality Assessment
2.5. Data Processing and Statistical Analysis
3. Results
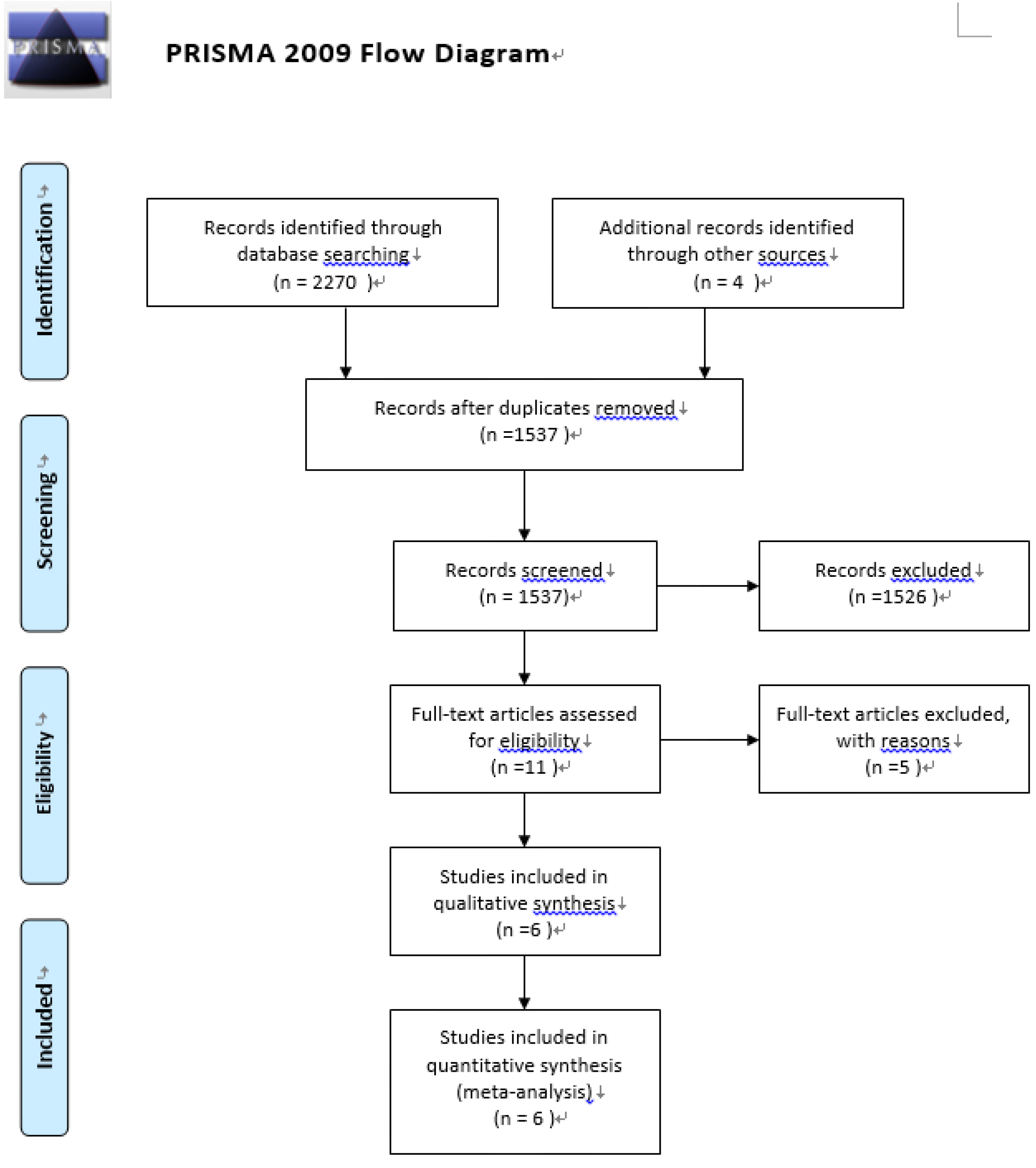
3.1. Study Selection and Quality Assessment


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Gadek et al., 1999 | Singe et al., 2006 | Pontes-Arda et al., 2006 | Grau-Carmona et al., 2011 | Rice et al., 2011 | Elamin et al., 2012 |
|---|---|---|---|---|---|---|
| Interventions | EPA + GLA + antioxidants | EPA + GLA + antioxidants | EPA + DHA + GLA + antioxidants | EPA + DHA + GLA + antioxidants | EPA + DHA + GLA + antioxidants | EPA + DHA + GLA + antioxidants |
| Control Diet | Isonitrogenous andisocaloric control diet | Isonitrogenous and isocaloric control diet | Isonitrogenous and isocaloric control diet | Isocaloric control diet | Isocaloric and isovolemic control diet | Isonitrogenous and isocaloric control diet |
| Treatment Duration | N/A | 14 days | N/A | N/A | 21 days | 7 days |
| Route | Gastric, duodenal, jejunalfeeding tube | Nasogastric, duodenal, jejunal tube | Eneral feeding | Gastric, jejunal tube | Bolus delivery | Nasogastric, nasoduodenal, nasojejunal, jejunostomytubes |
| Sample Size | ||||||
| Treatment Group | 51 | 46 | 55 | 61 | 143 | 9 |
| Control Group | 47 | 49 | 48 | 71 | 129 | 8 |
| Sex Ratio (Male:Female) | 52:46 | NA | 61:42 | 30:132 | 133:139 | 8:9 |
| Average Age (years) | 51 | 59.7 | 65.1 | 63 | 54.1 | 52.4 |
| No. of Participants Drop-out or Withdrawal | 48 | 5 | 62 | 28 | 0 | 5 |
| Blind Type | Double-blind | Unblind | Double-blind | Single-blind | Double-blind | Double-blind |
| Mordified Jadad Scale | 7 | 5 | 5 | 5 | 7 | 5 |
| Primary End Point | Time receiving ventilatorysupport | Change in oxygenation and breathing patterns | 28-day mortality | New organ dysfunction | Ventilator-free days | Oxygenation and modified Lung Injury Scores |
| Mortality Outcome Type | Mortality | 28-day mortality | 28-day mortality | 28-day mortality | 60-day or hospital mortality | 28-day mortality |
| Mortality | ||||||
| Treatment Group | 6/51 | 13/46 | 18/55 | 11/61 | 38/143 | 0/9 |
| Control Group | 9/47 | 28/49 | 25/48 | 11/71 | 21/129 | 1/8 |
| Mortality Rate of Control Group | 9/47 (19.15%) | 28/49 (57.14%) | 25/48 (52.08) | 11/71 (15.49) | 21/129 (16.28) | 1/8 (12.5) |
| PaO2/FiO2 Ratio (Day 7) | ||||||
| Treatment Group | N/A | 296.5 ± 165.3 (SD) | 224.4 | 217 | N/A | 178 |
| Control Group | N/A | 236.3 ± 79.8 (SD) | 150.5 | 190 | N/A | 201 |
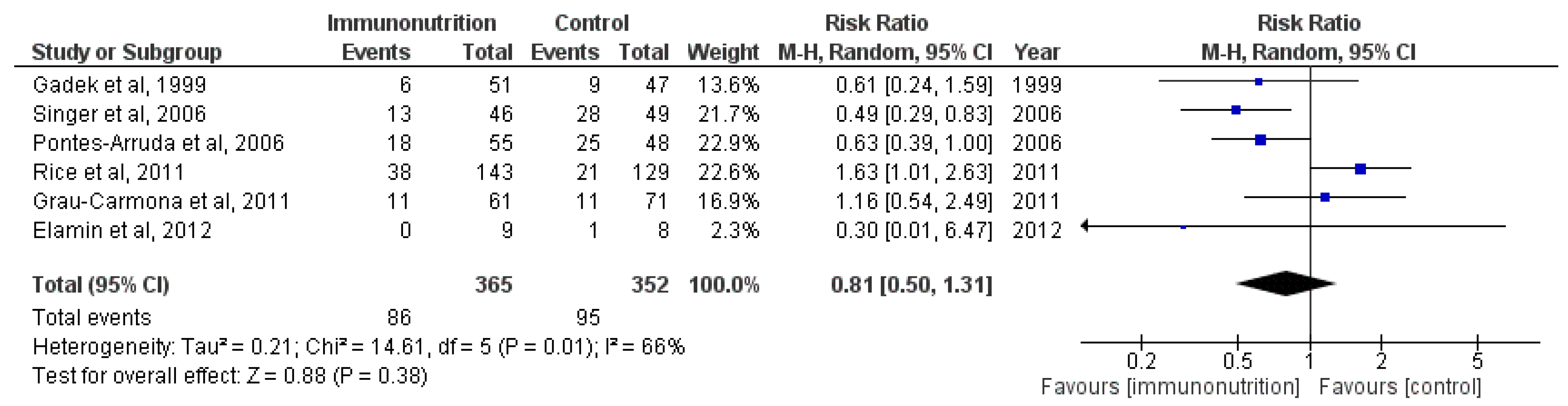
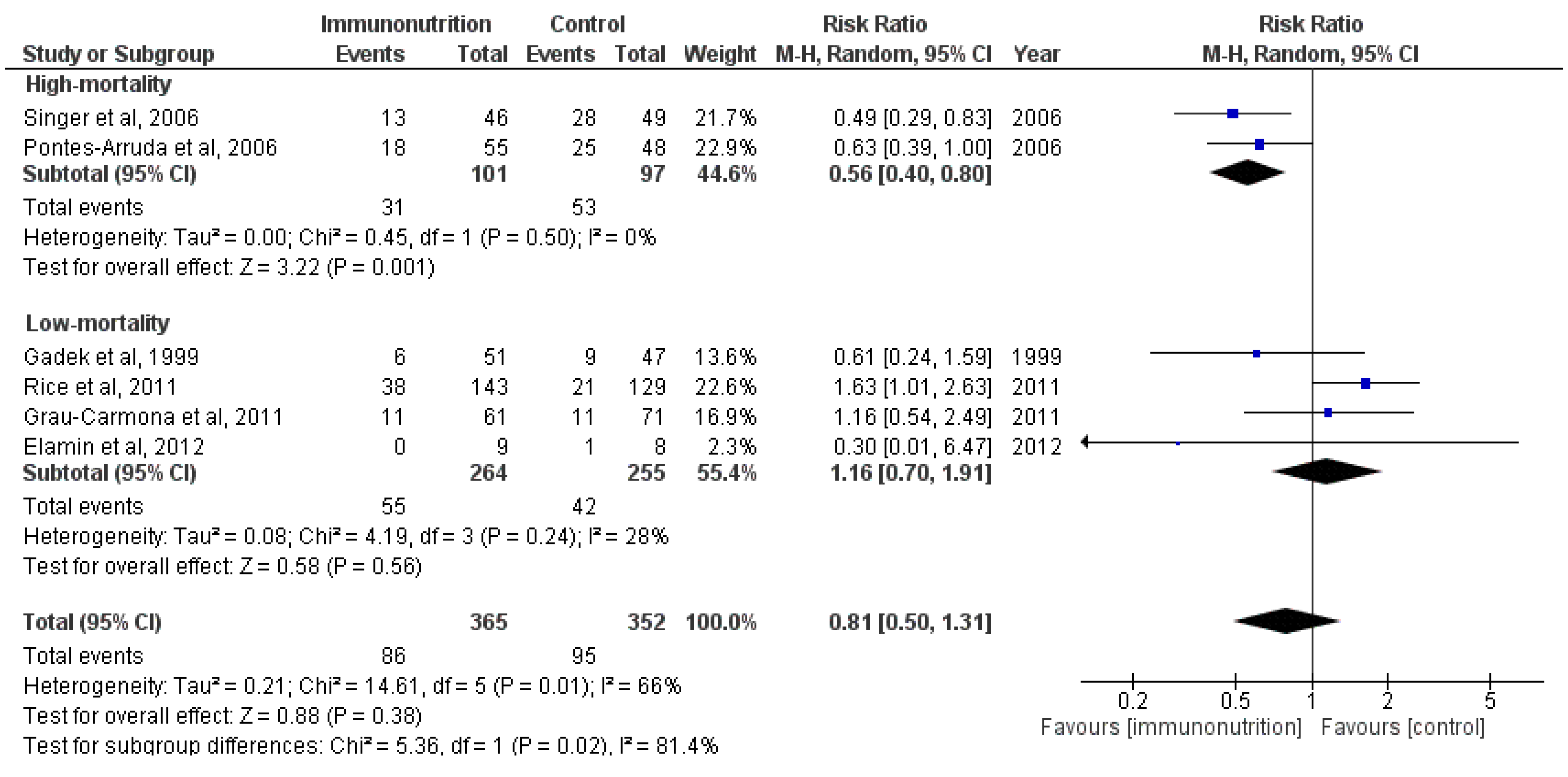
3.2. Effect on Mortality

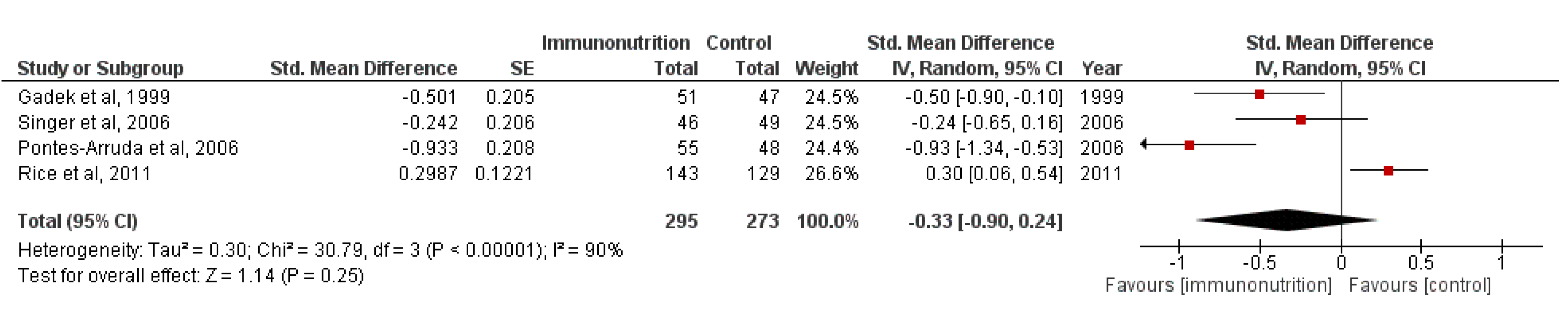
3.3. Effect on 28-Day Ventilator-Free Days and 28-Day ICU-Free Days



3.4. Sensitivity Analyses
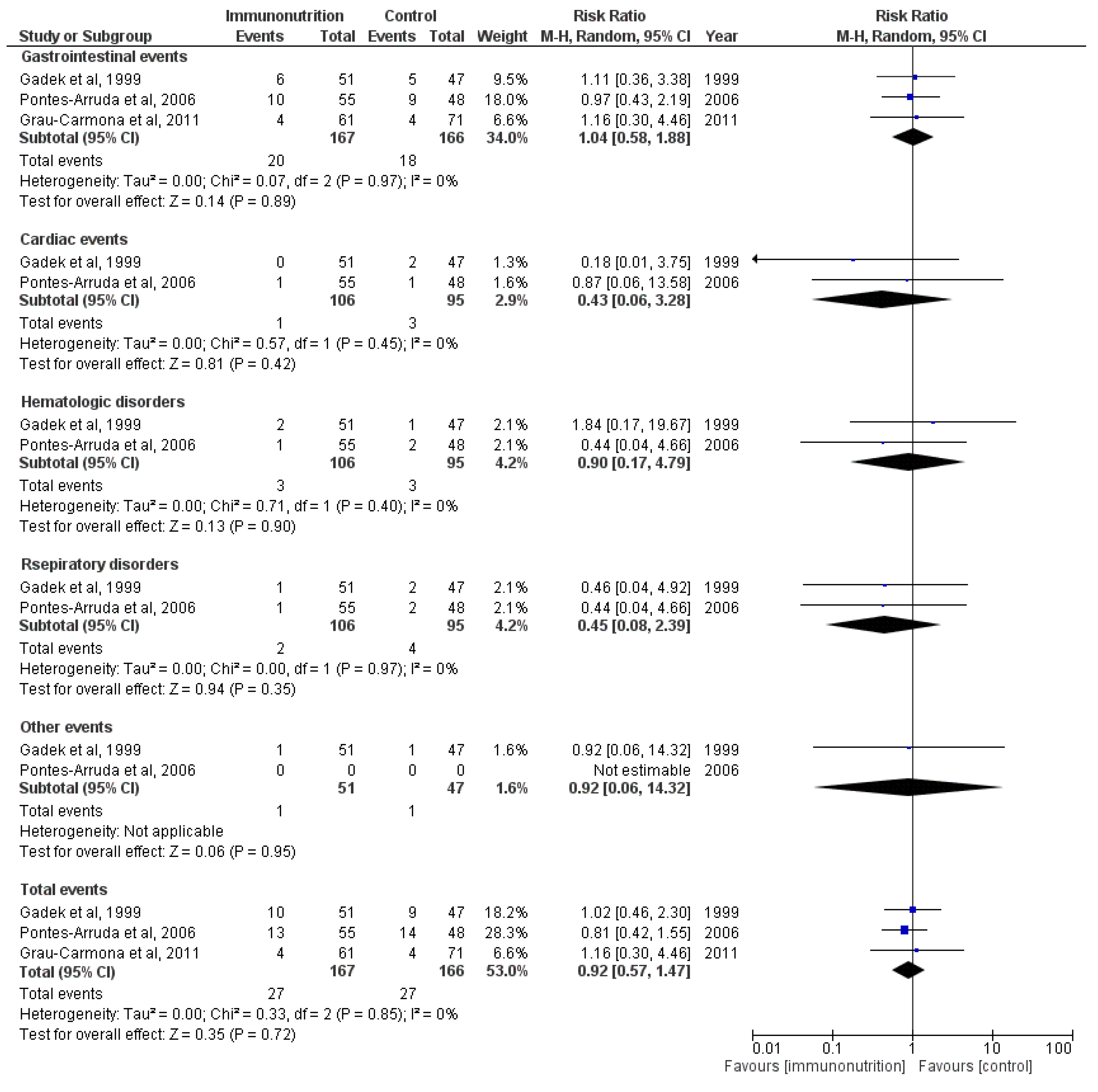
3.5. Adverse Effects

3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Information
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wheeler, A.P.; Bernard, G.R. Acute lung injury and the acute respiratory distress syndrome: A clinical review. Lancet 2007, 369, 1553–1564. [Google Scholar] [CrossRef]
- Pierrakos, C.; Karanikolas, M.; Scolletta, S.; Karamouzos, V.; Velissaris, D. Acute respiratory distress syndrome: Pathophysiology and therapeutic options. J. Clin. Med. Res. 2012, 4, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Muller-Redetzky, H.C.; Felten, M.; Hellwig, K.; Wienhold, S.M.; Naujoks, J.; Opitz, B.; Kershaw, O.; Gruber, A.D.; Suttorp, N.; Witzenrath, M. Increasing the inspiratory time and I:E ratio during mechanical ventilation aggravates ventilator-induced lung injury in mice. Crit. Care 2015, 19, 23. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, N.; Burns, K.E.; Meade, M.O. Pharmacologic treatments for acute respiratory distress syndrome and acute lung injury: Systematic review and meta-analysis. Treat Respir. Med. 2004, 3, 307–328. [Google Scholar] [CrossRef] [PubMed]
- Gadek, J.E.; DeMichele, S.J.; Karlstad, M.D.; Pacht, E.R.; Donahoe, M.; Albertson, T.E.; Van Hoozen, C.; Wennberg, A.K.; Nelson, J.L.; Noursalehi, M. Effect of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in patients with acute respiratory distress syndrome. Crit. Care Med. 1999, 27, 1409–1420. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Theilla, M.; Fisher, H.; Gibstein, L.; Grozovski, E.; Cohen, J. Benefit of an enteral diet enriched with eicosapentaenoic acid and gamma-linolenic acid in ventilated patients with acute lung injury. Crit. Care Med. 2006, 34, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Pontes-Arruda, A.; Aragao, A.M.; Albuquerque, J.D. Effects of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Crit. Care Med. 2006, 34, 2325–2333. [Google Scholar] [CrossRef] [PubMed]
- Pontes-Arruda, A.; Demichele, S.; Seth, A.; Singer, P. The use of an inflammation-modulating diet in patients with acute lung injury or acute respiratory distress syndrome: A meta-analysis of outcome data. JPEN J. Parenter. Enter. Nutr. 2008, 32, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Dee, B.M.; Bruno, J.J.; Lal, L.S.; Canada, T.W. Effects of immune-enhancing enteral nutrition on mortality and oxygenation in acute lung injury and acute respiratory distress syndrome a meta-analysis. Hosp. Pharm. 2011, 1, 33–40. [Google Scholar] [CrossRef]
- El, K.D.; Gjorstrup, P.; Filep, J.G. Resolvin E1 promotes phagocytosis-induced neutrophil apoptosis and accelerates resolution of pulmonary inflammation. Proc. Natl. Acad. Sci. USA 2012, 109, 14983–14988. [Google Scholar]
- Khan, S.A.; Ali, A.; Khan, S.A.; Zahran, S.A.; Damanhouri, G.; Azhar, E.; Qadri, I. Unraveling the complex relationship triad between lipids, obesity, and inflammation. Mediat. Inflamm. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Gong, X.; Wan, J.Y.; Zhang, L.; Zhang, Z.; Li, H.Z.; Min, S. Resolvin D1 protects mice from LPS-induced acute lung injury. Pulm. Pharmacol. Ther. 2011, 24, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.R.; Phillips, O.; Fukumoto, J.; Fukumoto, I.; Tamarapu, P.P.; Arias, S.; Cho, Y.; Lockey, R.F.; Kolliputi, N. Aspirin-Triggered Resolvin D1 Treatment Enhances Resolution of Hyperoxic Acute Lung Injury. Am. J. Respir. Cell Mol. Biol. 2015. [Google Scholar] [CrossRef]
- Chen, S.; Zheng, S.; Liu, Z.; Tang, C.; Zhao, B.; Du, J.; Jin, H. Endogeous sulfur dioxide protects against oleic acid-induced acute lung injury in association with inhibition of oxidative stress in rats. Lab. Investig. 2015, 95, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; DeBoisblanc, B.P.; Steingrub, J.; Rock, P. Enteral omega-3 fatty acid, gamma-linolenic acid, and antioxidant supplementation in acute lung injury. JAMA 2011, 306, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banares, R.; Albillos, A.; Rincon, D.; Alonso, S.; Gonzalez, M.; Ruiz-del-Arbol, L.; Salcedo, M.; Molinero, L.M. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: A meta-analysis. Hepatology 2002, 35, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Grau-Carmona, T.; Moran-Garcia, V.; Garcia-de-Lorenzo, A.; Heras-de-la-Calle, G.; Quesada-Bellver, B.; Lopez-Martinez, J.; Gonzalez-Fernandez, C.; Montejo-Gonzalez, J.C.; Blesa-Malpica, A.; Albert-Bonamusa, I.; et al. Effect of an enteral diet enriched with eicosapentaenoic acid, gamma-linolenic acid and anti-oxidants on the outcome of mechanically ventilated, critically ill, septic patients. Clin. Nutr. 2011, 30, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Elamin, E.M.; Miller, A.C.; Ziad, S. Immune enteral nutrition can improve outcomes in medical-surgical patients with ARDS: A prospective randomized controlled trial. J. Nutr. Disord. Ther. 2012, 2, 109. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.L.; DeMichele, S.J.; Pacht, E.R.; Wennberg, A.K. Effect of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants on antioxidant status in patients with acute respiratory distress syndrome. JPEN J. Parenter. Enter. Nutr. 2003, 27, 98–104. [Google Scholar] [CrossRef]
- Pacht, E.R.; DeMichele, S.J.; Nelson, J.L.; Hart, J.; Wennberg, A.K.; Gadek, J.E. Enteral nutrition with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants reduces alveolar inflammatory mediators and protein influx in patients with acute respiratory distress syndrome. Crit. Care Med. 2003, 31, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Theilla, M.; Singer, P.; Cohen, J.; Dekeyser, F. A diet enriched in eicosapentanoic acid, gamma-linolenic acid and antioxidants in the prevention of new pressure ulcer formation in critically ill patients with acute lung injury: A randomized, prospective, controlled study. Clin. Nutr. 2007, 26, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Pontes-Arruda, A.; Martins, L.F.; de Lima, S.M.; Isola, A.M.; Toledo, D.; Rezende, E.; Maia, M.; Magnan, G.B. Enteral nutrition with eicosapentaenoic acid, gamma-linolenic acid and antioxidants in the early treatment of sepsis: Results from a multicenter, prospective, randomized, double-blinded, controlled study: The INTERSEPT study. Crit. Care 2011, 15. [Google Scholar] [CrossRef] [PubMed]
- Schott, C.K.; Huang, D.T. omega-3 fatty acids, gamma-linolenic acid, and antioxidants: Immunomodulators or inert dietary supplements? Crit. Care 2012, 16, 325. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zhou, S.; Yao, W.; Gan, X.; Su, G.; Yuan, D.; Hei, Z. Propofol prevents lung injury after intestinal ischemia-reperfusion by inhibiting the interaction between mast cell activation and oxidative stress. Life Sci. 2014, 108, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Jiang, H.; Zhou, Z.Y.; Tao, Y.X.; Cai, B.; Liu, J.; Yang, H.; Lu, C.D.; Zeng, J. Is omega-3 fatty acids enriched nutrition support safe for critical ill patients? A systematic review and meta-analysis. Nutrients 2014, 6, 2148–2164. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Bo, L.; Liu, W.; Lu, X.; Jin, F. Enteral Immunomodulatory Diet (Omega-3 Fatty Acid, γ-Linolenic Acid and Antioxidant Supplementation) for Acute Lung Injury and Acute Respiratory Distress Syndrome: An Updated Systematic Review and Meta-Analysis. Nutrients 2015, 7, 5572-5585. https://doi.org/10.3390/nu7075239
Li C, Bo L, Liu W, Lu X, Jin F. Enteral Immunomodulatory Diet (Omega-3 Fatty Acid, γ-Linolenic Acid and Antioxidant Supplementation) for Acute Lung Injury and Acute Respiratory Distress Syndrome: An Updated Systematic Review and Meta-Analysis. Nutrients. 2015; 7(7):5572-5585. https://doi.org/10.3390/nu7075239
Chicago/Turabian StyleLi, Congcong, Liyan Bo, Wei Liu, Xi Lu, and Faguang Jin. 2015. "Enteral Immunomodulatory Diet (Omega-3 Fatty Acid, γ-Linolenic Acid and Antioxidant Supplementation) for Acute Lung Injury and Acute Respiratory Distress Syndrome: An Updated Systematic Review and Meta-Analysis" Nutrients 7, no. 7: 5572-5585. https://doi.org/10.3390/nu7075239