Dietary Patterns, Alcohol Consumption and Risk of Coronary Heart Disease in Adults: A Meta-Analysis

Abstract
:1. Introduction
2. Methods
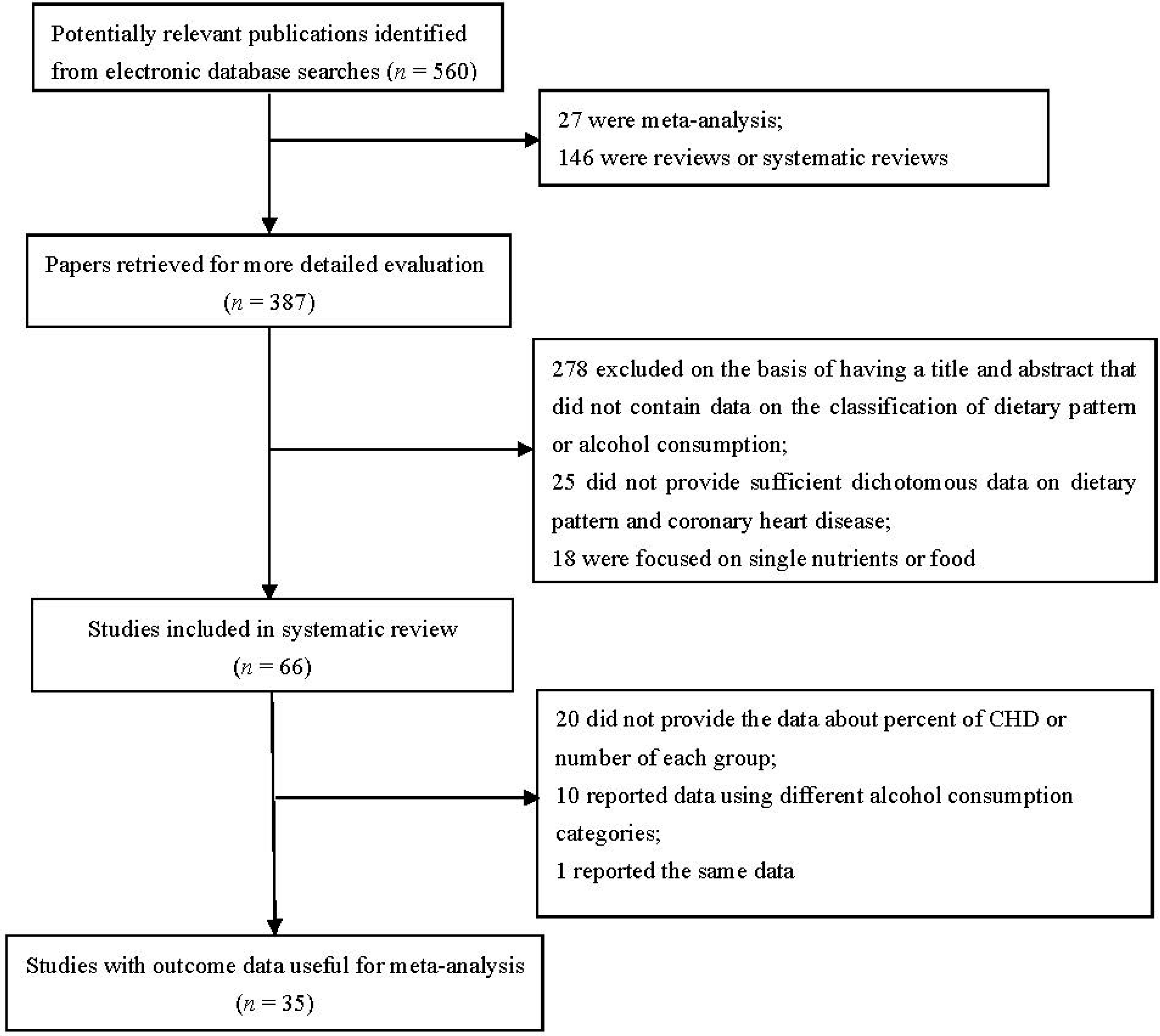
2.1. Literature Search Strategy
2.2. Study Included Criteria
2.3. Data Extraction
2.4. Definition of “High Intake”
2.5. Quality Assessment
2.6. Assessment of Heterogeneity
2.7. Statistical Analysis
3. Results
3.1. Overview of Included Studies for the Systematic Meta-Analysis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Publication Year | Location | Study Design | Total Number of Subjects | Age (Year)/Sex | Diet Assessment Method | Dietary Patterns Identified | Factors Adjusted for in Analyses |
|---|---|---|---|---|---|---|---|
| Osler et.al., 2002 [8] | Danish | Cohort | 5834 | 30–60 years both | FFQ | “prudent food” “Western food” | Smoking, exercise, education, BMI and alcohol intake |
| Fung et.al., 2001 [11] | US | Cohort | 69,017 | 38–63 years women | FFQ | “Prudent” “Western” | Age, period, smoking, BMI, hormone replacement therapy, aspirin use, caloric intake, family history, history of hypertension, multivitamin and vitamin E supplement use, physical activity |
| Iqbal et.al., 2008 [13] | 52 countries | Case-control | 5761/10,646 | 41–70 years both | FFQ | Oriental, Western, prudent | Age, sex, region, education, BMI, physical activity, smoking |
| Hoffmann et.al., 2004 [14] | Germany | Case-control | 200/255 | 30–80 years women | FFQ | “Western” | Age, cigarette smoking, hormone replacement therapy, hypertension, education level, physical activity level and sport |
| Stricker et.al., 2012 [15] | Dutch | Cohort | 40,011 | 50–69 years both | FFQ | “Prudent” “Western” | Age, gender, physical activity, smoking status, education, systolic- and diastolic blood pressure and energy intake |
| Weikert et.al., [16] (CORA) 2005 | Germany | Case-control | 200/255 | 30–80 years women | FFQ | “Simplified food pattern” | Age, cigarette smoking, education attainment, BMI, physical activity level, total energy intake, hormone replacement therapy, hypertension, dyslipidemia, and diabetes |
| Weikert et.al., [16] (EPIC-Potsdam) 2005 | Germany | Cohort | 26,795 | 35–65 years both | FFQ | “Simplified food pattern” | Age, cigarette smoking, education attainment, BMI, physical activity level, total energy intake, hormone replacement therapy, hypertension, dyslipidemia, and diabetes |
| Lipoeto et.al., 2004 [17] | Indonesia | Case-control | 93/189 | men and women | FFQ | “Animal foods” | Age, physical activity and stress level, total energy |
| Tucker et.al., 2005 [18] | US | Cohort | 501 | 34–80 years men | 7-day diet records | “Low SF and high FV” | Age,, total energy intake, BMI, smoking, alcohol use, physical activity score, dietary supplement use |
| McNaughton et.al., 2009 [19] | UK | Cohort | 7314 | 35–55 years both | FFQ | “Dietary pattern 1” “Dietary pattern 2” | Age, sex, energy misreporting, ethnicity, smoking, alcohol, physical activity, blood pressure and BMI |
| Fitzgerald et.al., 2012 [20] | US | Cohort | 34,827 | ≥45 years women | FFQ | “DASH” | Randomization status, age, smoking, time-varying postmenopausal status, time-varying hormone therapy use, alcohol intake, energy intake, physical activity, cigarettes per day, BMI, and highest education level |
| Martínez-Gonzlez et.al., 2011 [21] | Spain | Cohort | 13,609 | 34–43 years both | FFQ | “Mediterranean” | Age, sex, family history of coronary heart disease, total energy intake, physical activity, smoking, BMI, diabetes at baseline, use of aspirin, history of hypertension and history of hypercholesterolemia |
| Maruyama et.al., 2013 [22] | Japan | Cohort | 64,037 | 40–79 years both | FFQ | “Vegetable” “Animal food” “Dairy product” | Age, BMI, smoking category, walking time, hours of sports, perceived mental stress, total energy intake, history of hypertension and diabetes |
| Hu et.al., 2000 [23] | US | Cohort | 44,874 | 40–75 years men | FFQ | “Prudent”, “Western” | Age, BMI, time period, cigarette smoking, parental history of myocardial infarction before age 60, multivitamin and vitamin E supplement use, alcohol consumption, history of hypertension, physical activity, total energy intake, and profession |
| Guallar-Castillón et.al., 2012 [28] | Spain | Cohort | 40,757 | 29–69 years both | Dietary history | “Mediterranean”, “Westernized” | BMI, waist circumference, education, smoking, physical activity at work, physical activity at home, physical activity during leisure time, diabetes, hypertension, hypercholesterolemia, cancer, oral contraceptives, menopausal status, hormone replacement therapy, total energy intake, and stratified by age at recruitment, sex, and center. |
| Martínez-González et.al., 2002 [29] | Spain | Case-control | 171/171 | ≤80 years both | FFQ | “Priori pattern” “Mediterranean” “Post hoc pattern” | Smoking, BMI, high blood pressure, high blood cholesterol, diabetes, leisure-time activity, family history of CHD before 60y, aspirin intake and socioeconomic status |
| Shimazu et.al., 2007 [30] | Japan | Cohort | 40,547 | 40–79 years both | FFQ | “Japanese pattern” “Animal food” | Age, sex, smoking status, walking duration, education, total energy intake, BMI, and history of hypertension |
| Arriola et.al., 2010 [31] | Spain | Cohort | 41,438 | 29–69 years both | Dietary history questionnaire | Alcohol intake | Centre, smoking status, height and educational level, stratified by age, physical activity index, waist/hip ratio, vitamin E, antithrombotic and antihemorrhagic drugs and energy intake |
| Beulens et.al., 2007 [32] | US | Cohort | 11,711 | 40–75 years men | FFQ | Alcohol intake | Age, smoking, BMI, physical activity, diabetes, hypercholesterolemia, family history of MI, aspirin use, lipid-lowering therapy, energy intake, and energy-adjusted quintiles of saturated fat, trans fatty acids, sodium, potassium, magnesium, folate, vitamin E, n-3 fatty acids, and dietary fiber. |
| Bos et.al., 2010 [33] | Dutch | Cohort | 10,530 | 49–70 years women | FFQ | Alcohol intake | Age, smoking, BMI, menopausal status, physical activity, education level, hypercholesterolemia, diabetes, antihypertensive medication, daily energy intake, vitamin E, vitamin C, saturated fat, and fiber intake |
| Fernández-Jarne et.al., 2003 [34] | Spain | Case-control | 171/171 | Mean 62 years Both | FFQ | Total alcohol intake | Total energy intake, smoking, BMI, high blood pressure, high blood cholesterol, diabetes, leisure-time physical activity, aspirin use, family history of coronary heart disease, marital status, occupation, study level, olive oil consumption, ratio of monounsaturated to saturated fat, folic acid, and total fiber intake. |
| Fuchs et.al., 2004 [35] | US | Cohort | 14,506 | 45–64 years men | Dietary questionnaire | Alcohol intake | Age, cigarette-years of smoking, BMI, LDL- and HDL-cholesterol level, waist/hip ratio, educational level, income, sport index, diabetes mellitus, systolic blood pressure, use of antihypertensive medication. |
| Ikehara et.al., 2009 [36] | Japan | Cohort | 19,356 | 40–69 years men | Self-administered questionnaire | Alcohol consumption | Age, smoking status, body mass index, history of hypertension and diabetes, sports of leisure time, levels of mental stress, presence of flushing and job, marital status, medical checkups and area. |
| Ikehara et.al., 2008 [37] | Japan | Cohort | 83,682 | 40–79 years both | Self-administered questionnaire | Ethanol intake | Age, smoking status, BMI, history of hypertension and diabetes, frequency of exercise, perceived mental stress, education level, and intake of vegetables, fish, and fruit |
| Ikehara et.al., 2013 [38] | Japan | Cohort | 47,100 | 40–69 years women | Self-reported questionnaire | Alcohol consumption | Age, smoking status, body mass index, history of diabetes, sports at leisure time, flushing after drinking alcohol, mental stress, menopausal status and area, history of hypertension |
| Mukamal et.al., 2006 [39] | US | Cohort | 38,077 | 40–75 years men | FFQ | Alcohol consumption | Age, smoking status, body mass index, the presence or absence of diabetes, hypertension, hypercholesterolemia, and a parental history of myocardial infarction, use or nonuse of aspirin, physical activity, intake of energy, and energy-adjusted intake of folate, vitamin E, saturated fat, trans fat, and fiber. |
| Keil et.al., 1997 [40] | Germany | Cohort | 62/1071 | 45–64 years both | 7-day recall | Alcohol intake | Age, smoking, hypertension, BMI |
| Kono et.al., 1991 [41] | Japan | Case-control | 89/271 | 40–69 years both | Self-administered questionnaire | Alcohol intake | Age, smoking, strenuous exercise, BMI, systemic hypertension, diabetes mellitus, heart disease in parent, job class |
| Schröder et.al., 2007 [42] | Spain | Case-control | 224/1270 | 25–74 years both | Questionnaire | Alcohol intake | Age, smoking, educational level, leisure-time physical activity, total cholesterol, LDL- and HDL-cholesterol, diabetes, hypercholesterolemia drug treatment, and diagnosed hypertension |
| Wells et.al., 2004 [43] | New Zealand | Case-control | 1381/1892 | 35–74 years both | Questionnaire | Alcohol intake | Age group, history of CHD, tobacco smoking, leisure-time physical activity, current antihypertensive drug treatment, family history of premature cardiovascular disease, BMI, diabetes, socioeconomic status, income and low education. |
| Kitamura et.al., 1998 [44] | Japan | Cohort | 8476 | 40–59 years men | Interview | Alcohol intake | Age, serum total cholesterol, cigarette smoking, BMI, left ventricular hypertrophy, and history of diabetes mellitus. |
| Mukamal et.al., 2006 (n = 2) [45] | US | Cohort | 4410 | ≥65 years both | Self-administered questionnaire | Alcohol use | Age, sex, race, education, marital status, smoking, exercise intensity, depression score, frequent aspirin use, BMI, and diabetes mellitus. |
| Solomon et.al., 2000 [46] | US | Cohort | 5103 | 30–55 years women | FFQ | Alcohol consumption | Age, time period, body mass index, cigarette smoking, parental history of MI before age 60 years, hypertension, hypercholesterolemia, menopausal status/postmenopausal hormone use, aspirin use, multivitamin use, vitamin E supplement use, and physical activity level. |
| Bazzano et.al., 2009 [47] | China | Cohort | 64,597 | ≥40 years men | Interviewer-administered questionnaire | Alcohol consumption | Age, body-mass index, average systolic blood pressure, physical activity, cigarette smoking, diabetes education, urban or rural residence, and living in North China |
| Hvidtfeldt et.al., 2010 [48] | Denmark | Cohort | 266,986 | ≥39 years both | FFQ or diet history questionnaire | Alcohol intake | Age, year of baseline questionnaire |
| Rajpathak et.al., 2010 [49] | US | Cohort | 3198 | 50–79 years women | FFQ | Alcohol intake | Age, race/ethnicity, BMI, smoking, hypertension, high cholesterol, hormone use, regular aspirin use, quintiles of physical activity, duration of DM, intake of saturated fat, PUFA, fiber. |
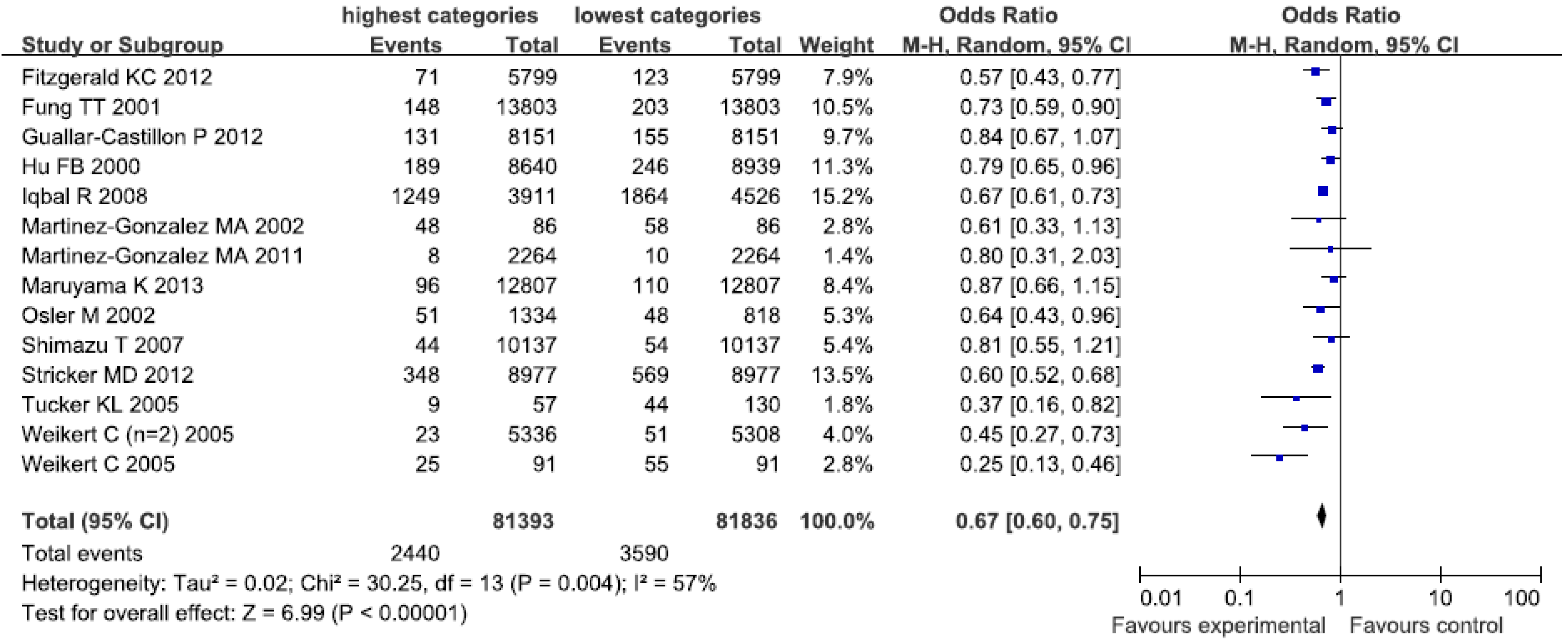
3.2. Healthy Dietary Pattern

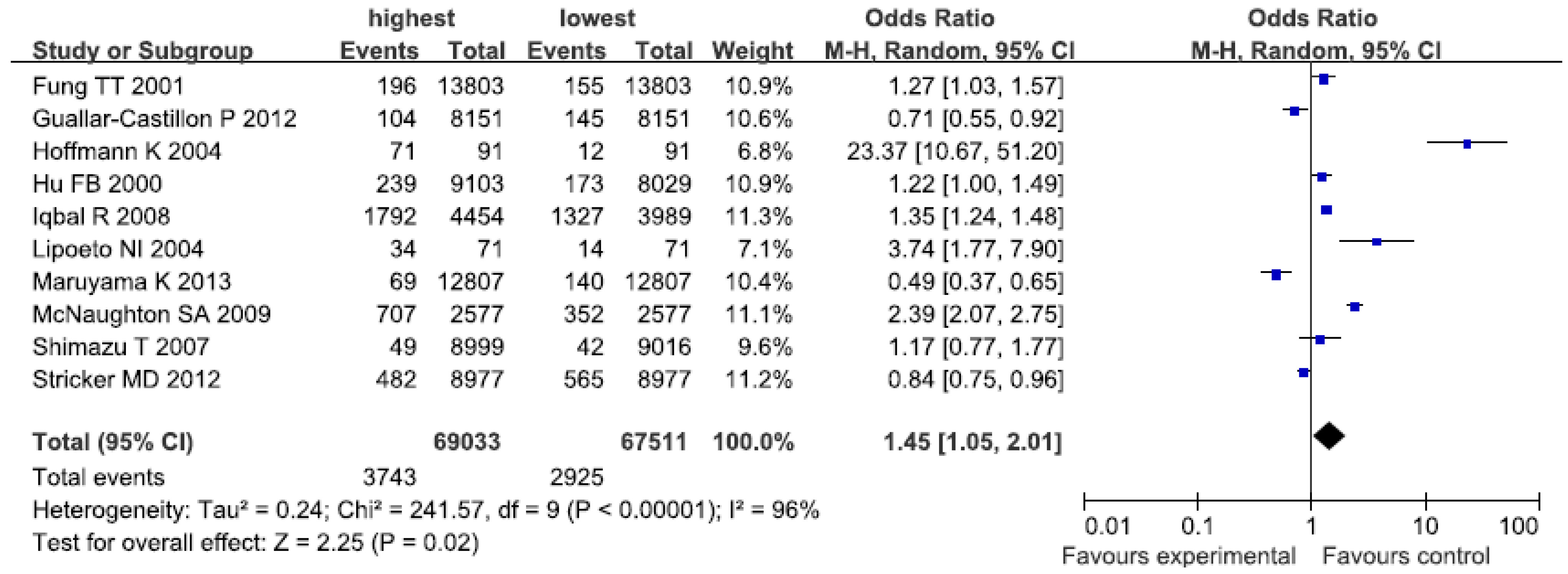
3.3. Western-Type Dietary Pattern

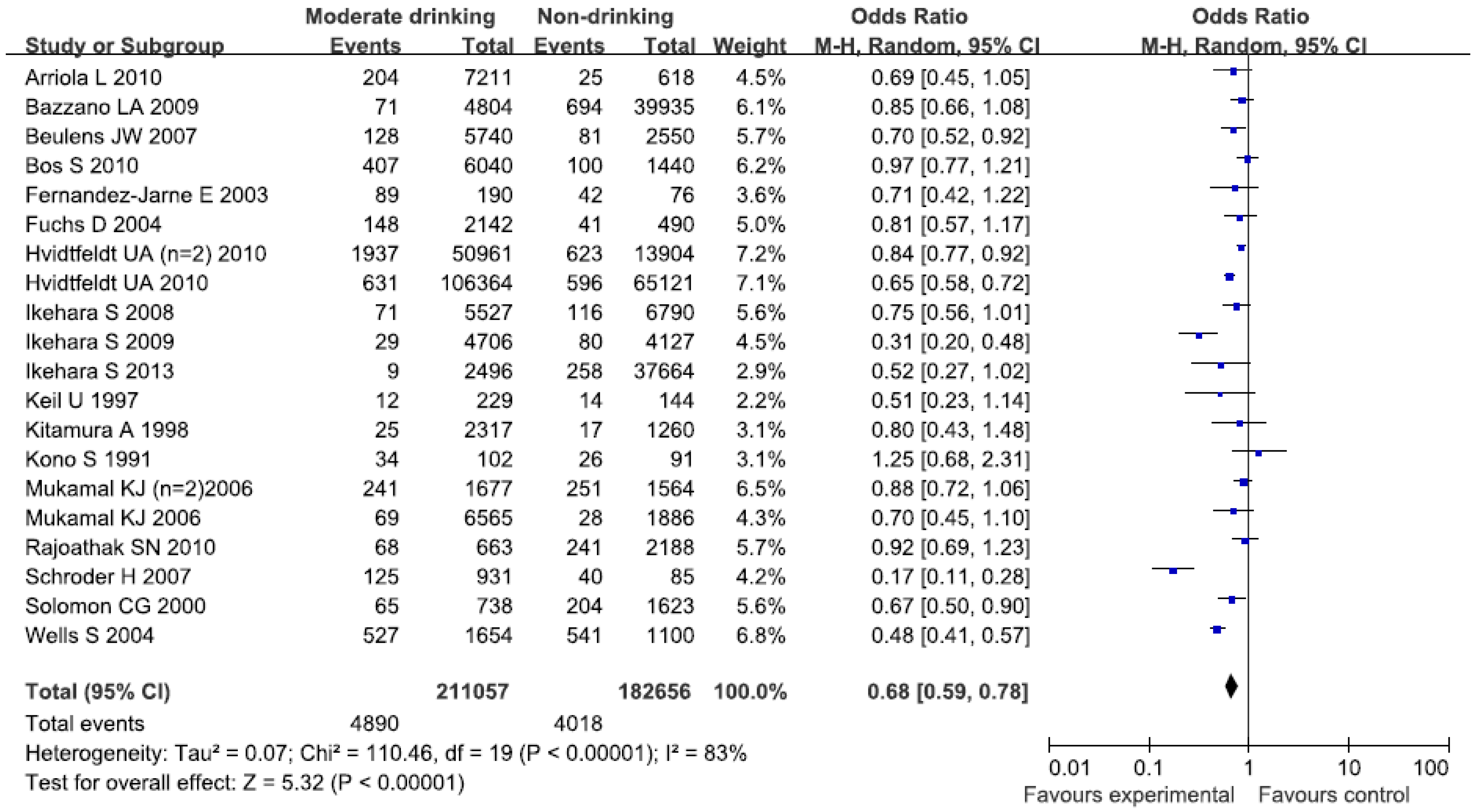
3.4. Alcohol Consumption

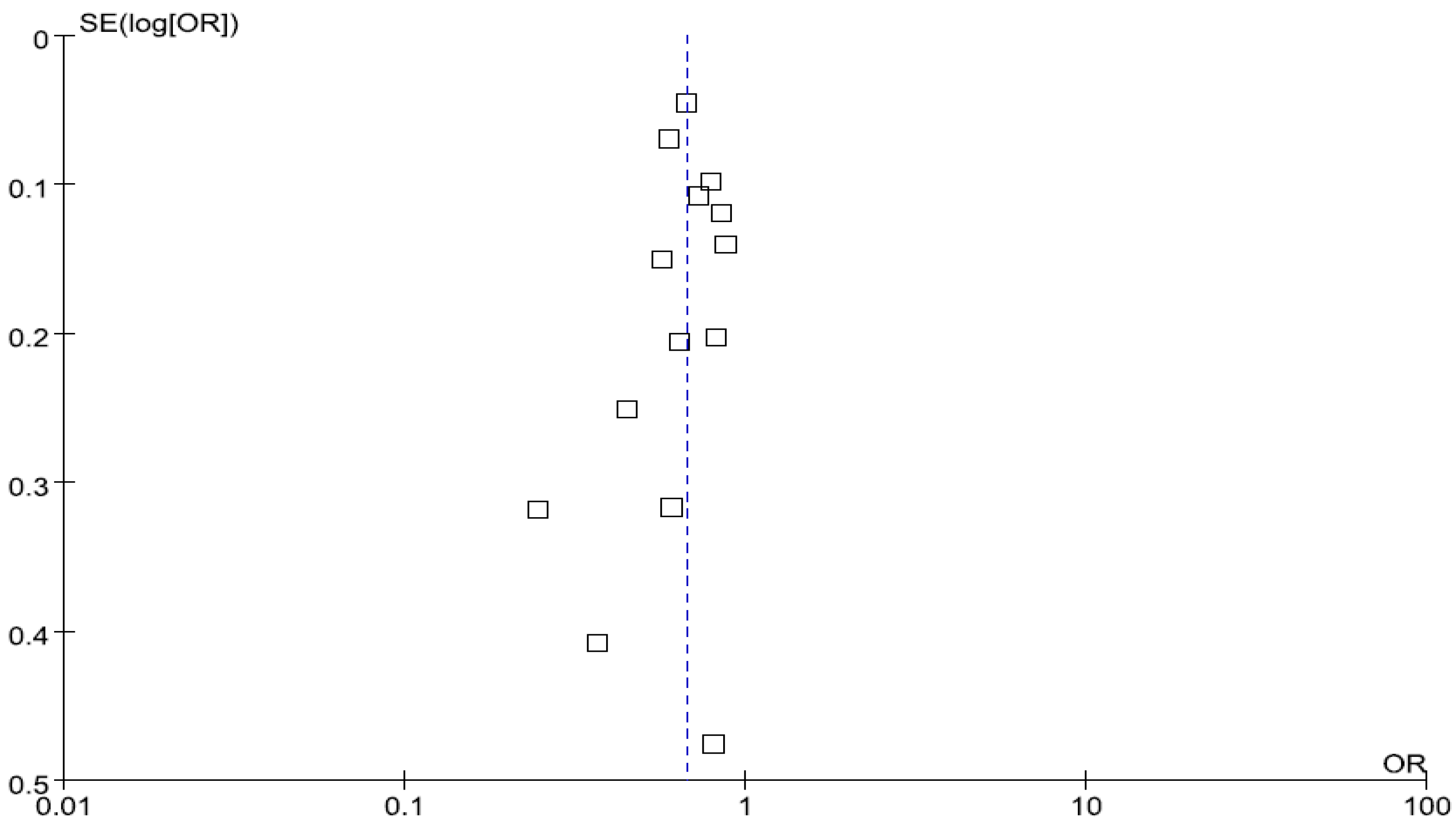
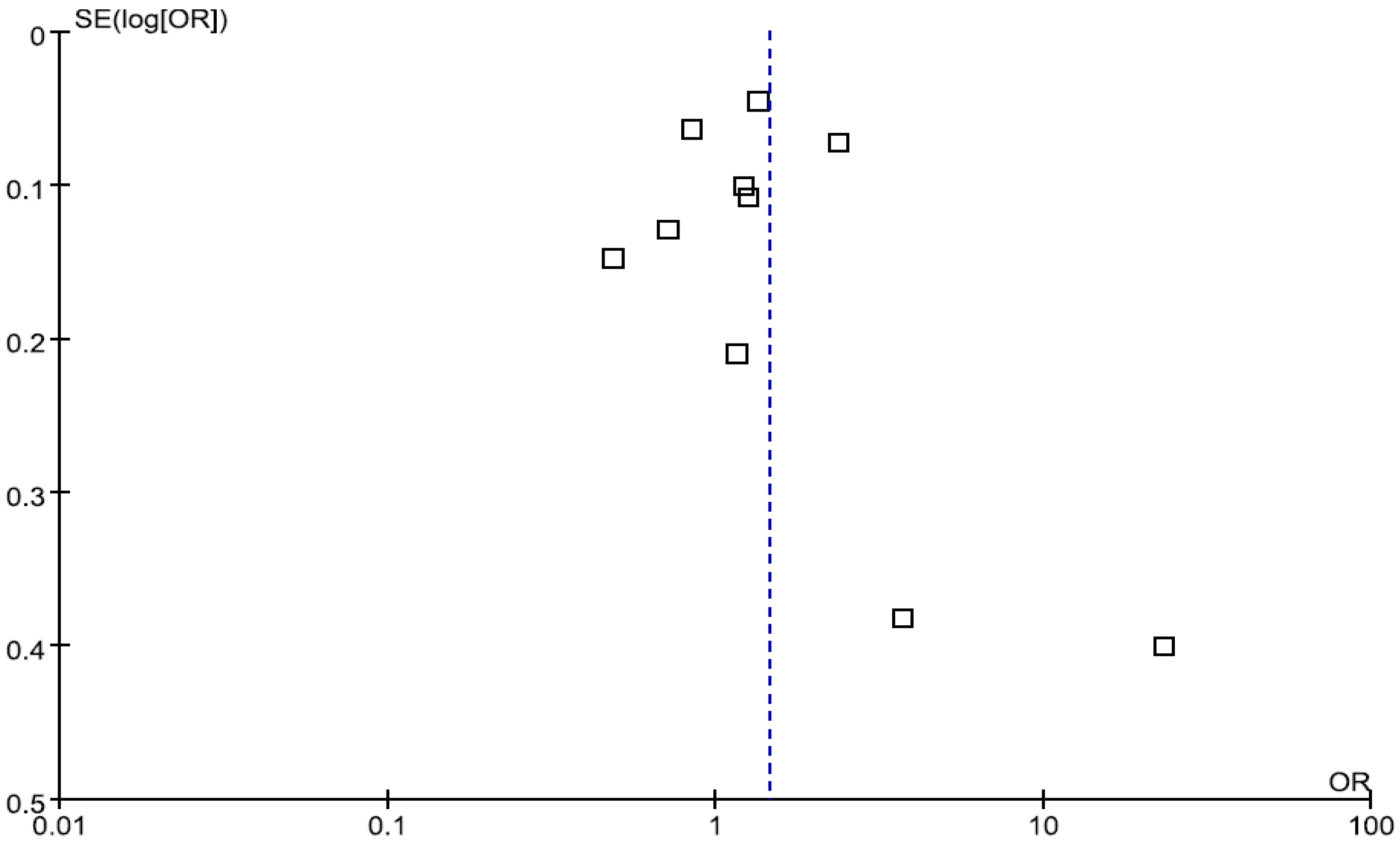
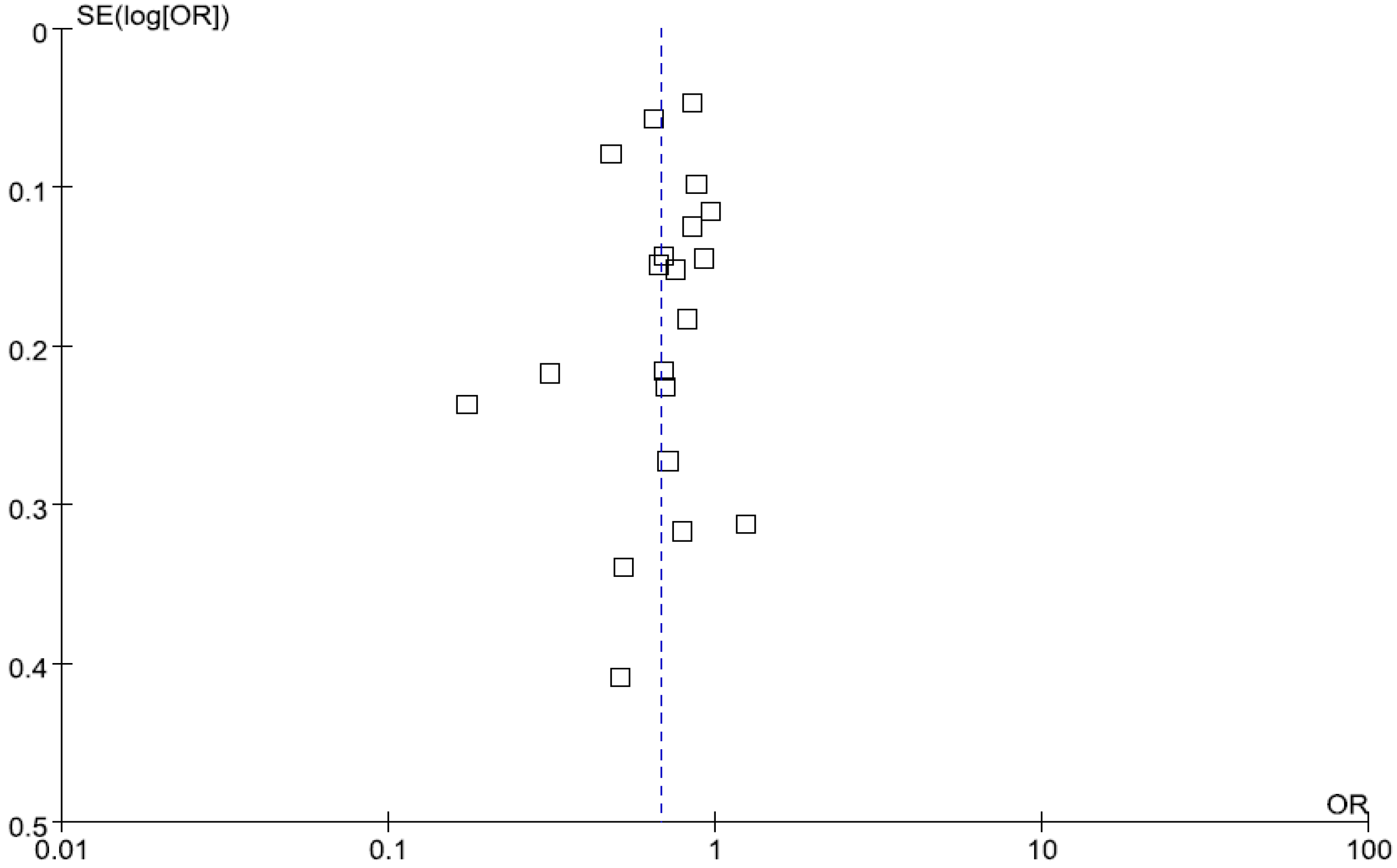
3.5. Publication Bias
3.6. Quality Assessment
3.7. Sensitivity Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A



Appendix B
| Studies | Selection | Comparability | Outcome | Score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5A | 5B | 6 | 7 | 8 | ||
| Cohort | ||||||||||
| Fung et al., 2001 [11] | * | * | * | * | * | * | * | * | ******** | |
| Fitzgerald et al., 2012 [20] | * | * | * | * | * | * | * | * | ******** | |
| Guallar-Castillón et al., 2012 [28] | * | * | * | * | * | * | * | ******* | ||
| Hu et al., 2000 [23] | * | * | * | * | * | * | * | * | * | ********* |
| Martínez-Gonzlez et al., 2011 [21] | * | * | * | * | * | * | * | ******* | ||
| Maruyama et al., 2013 [22] | * | * | * | * | * | ***** | ||||
| Osler et al., 2002 [8] | * | * | * | * | * | * | * | * | * | ********* |
| Shimazu et al., 2007 [30] | * | * | * | * | * | * | * | * | ******** | |
| Stricker et al., 2012 [15] | * | * | * | * | * | * | * | * | ******** | |
| Tucker et al., 2005 [18] | * | * | * | * | * | * | ****** | |||
| Weikert et al., 2005 [16] | * | * | * | * | * | * | * | * | * | ********* |
| McNaughton et al., 2009 [19] | * | * | * | * | * | * | * | * | ******** | |
| Arriola et al., 2010 [31] | * | * | * | * | * | * | * | ******** | ||
| Solomon et al., 2000 [46] | * | * | * | * | * | * | * | * | ******** | |
| Beulens et al., 2007 [32] | * | * | * | * | * | * | * | * | ******** | |
| Bos et al., 2010 [33] | * | * | * | * | * | * | * | * | * | ********* |
| Fuchs et al., 2004 [35] | * | * | * | * | * | ***** | ||||
| Ikehara et al., 2008 [37] | * | * | * | * | * | * | * | ******* | ||
| Ikehara et al., 2009 [36] | * | * | * | * | * | * | * | ******* | ||
| Ikehara et al., 2013 [38] | * | * | * | * | * | * | * | ******* | ||
| Keil et al., 1997 [40] | * | * | * | * | * | * | * | ******* | ||
| Mukamal et al., 2006 [39] | * | * | * | * | * | * | ****** | |||
| Mukamal et al., 2006 (n = 2) [45] | * | * | * | * | * | * | ****** | |||
| Bazzano et al., 2009 [47] | * | * | * | * | * | * | * | * | ******** | |
| Hvidtfeldt et al., 2010 [48] | * | * | * | * | * | * | * | ******* | ||
| Rajpathak et al., 2010 [49] | * | * | * | * | * | * | * | ******* | ||
| Kitamura et al., 1998 [44] | * | * | * | * | * | * | ****** | |||
| Case-control | ||||||||||
| Iqbal et al., 2008 [13] | * | * | * | * | * | * | * | ******* | ||
| Martínez-González et al., 2002 [29] | * | * | * | * | * | ***** | ||||
| Weikert et al. (CORA) 2005 [16] | * | * | * | * | * | * | * | ******* | ||
| Lipoeto et al., 2004 [17] | * | * | * | * | * | ***** | ||||
| Hoffmann et al., 2004 [14] | * | * | * | * | * | * | * | ******* | ||
| Fernández-Jarne et al., 2003 [34] | * | * | * | * | * | * | * | * | * | ********* |
| Kono et al., 1991 [41] | * | * | * | * | * | * | * | ******* | ||
| Schröder et al., 2007 [42] | * | * | * | * | * | ***** | ||||
| Wells et al., 2004 [43] | * | * | * | * | * | * | * | * | ******** | |
| Study Characteristic | Category | Healthy Dietary Pattern (95% CI) | Western-Style Dietary Pattern (95% CI) | Alcohol Consumption (95% CI) |
|---|---|---|---|---|
| Age | >50 | 0.65 (0.56, 0.76) | 1.31 (0.91, 1.88) | 0.72 (0.60, 0.86) |
| <50 | 0.75 (0.63, 0.90) | 1.49 (0.90, 2.45) | 0.59 (0.45, 0.79) | |
| Sample size | Large (>10,000) | 0.71 (0.64, 0.79) | 1.21 (0.87, 1.67) | 0.72 (0.62, 0.83) |
| Small (<10,000) | 0.56 (0.37, 0.86) | 1.77 (1.08, 2.88) | 0.64 (0.46, 0.87) | |
| Race | White | 0.67 (0.58, 0.77) | 1.53 (1.05, 2.22) | 0.68 (0.51, 0.80) |
| Asian and Other | 0.75 (0.60, 0.92) | 1.15 (0.63, 2.11) | 0.76 (0.57, 1.06) | |
| Study design | Case-control | 0.48 (0.28, 0.84) | 4.49 (0.73, 25.75) | 0.51 (0.37, 1.07) |
| Cohort | 0.72 (0.64, 0.81) | 1.08 (0.79, 1.48) | 0.74 (0.66, 0.83) | |
| Total energy | Adjusted | 0.67 (0.56, 0.80) | 1.05 (0.73, 1.51) | 0.78 (0.68, 0.90) |
| Unadjusted | 0.65 (0.61, 0.70) | 1.99 (1.27, 3.13) | 0.76 (0.55, 0.78) |
References
- Mackay, J.; Mensah, G. The Atlas of Heart Disease and Stroke. Available via World Health Organization. Available online: http://www.who.int/cardiovascular_diseases/resources/atlas/en/ (accessed on 29 September 2004).
- Levi, F.; Lucchini, F.; Negri, E.; La Vecchia, C. Trends in mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world. Heart 2002, 88, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Lee, E.T.; Peterson, L.E.; Devereux, R.B.; Rhoades, E.R.; Umans, J.G.; Best, L.G.; Howard, W.J.; Paranilam, J.; Howard, B.V. Differences in risk factors for coronary heart disease among diabetic and nondiabetic individuals from a population with high rates of diabetes: The Strong Heart Study. J. Clin. Endocrinol. Metab. 2012, 97, 3766–3767. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Gu, D.; Wu, X.; Reynolds, K.; Duan, X.; Yao, C.; Wang, J.; Chen, C.S.; Chen, J.; Wildman, R.P.; et al. Major causes of death among men and women in China. N. Engl. J. Med. 2005, 353, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics Annual, 2010. Available via World Health Organization. Available online: http://www.who.int/whosis/whostat/2010/en/index.html (accessed on 13 June 2011).
- Frankel, S.; Elwood, P.; Sweetnam, P.; Yarnell, J.; Smith, G.D. Birthweight, body-mass index in middle age, and incident coronary heart disease. Lancet 1996, 348, 1478–1480. [Google Scholar] [CrossRef]
- McKeigue, P.M.; Lithell, H.O.; Leon, D.A. Glucose tolerance and resistance to insulin-stimulated glucose uptake in mean aged 70 years in relation to size at birth. Diabetologia 1998, 41, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Osler, M.; Helms Andreasen, A.; Heitmann, B.; Høidrup, S.; Gerdes, U.; Mørch Jørgensen, L.; Schroll, M. Food intake patterns and risk of coronary heart disease: A prospective cohort study examining the use of traditional scoring techniques. Eur. J. Clin. Nutr. 2002, 56, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, K.J.; Smiciklas-Wright, H.; Weitzel, L.B.; Mitchell, D.C.; Friedmann, J.M.; Jensen, G.L. Hypertension-related dietary patterns of rural older adults. Prev. Med. 2004, 38, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Willett, W.C.; Stampfer, M.J.; Manson, J.E.; Hu, F.B. Dietary patterns and the risk of coronary heart disease in women. Arch. Intern. Med. 2001, 161, 1857–1862. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Li, W.; Wang, Y.; Chen, T.; Teo, K.; Liu, L.S.; Yusuf, S. Influence of dietary patterns on the risk of acute myocardial infarction in China population: The INTERHEART China study. Chin. Med. J. (Engl.) 2013, 126, 464–470. [Google Scholar] [PubMed]
- Iqbal, R.; Anand, S.; Ounpuu, S.; Islam, S.; Zhang, X.; Rangarajan, S.; Chifamba, J.; Al-Hinai, A.; Keltai, M.; Yusuf, S.; et al. Dietary patterns and the risk of acute myocardial infarction in 52 countries: Results of the INTERHEART study. Circulation 2008, 118, 1929–1937. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Zyriax, B.C.; Boeing, H.; Windler, E. A dietary pattern derived to explain biomarker variation is strongly associated with the risk of coronary artery disease. Am. J. Clin. Nutr. 2004, 80, 633–640. [Google Scholar] [PubMed]
- Stricker, M.D.; Onland-Moret, N.C.; Boer, J.M.; van der Schouw, Y.T.; Verschuren, W.M.; May, A.M.; Peeters, P.H.; Beulens, J.W. Dietary patterns derived from principal component- and k-means cluster analysis: Long-term association with coronary heart disease and stroke. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Hoffmann, K.; Dierkes, J.; Zyriax, B.C.; Klipstein-Grobusch, K.; Schulze, M.B.; Jung, R.; Windler, E.; Boeing, H. A homocysteine metabolism-related dietary pattern and the risk of coronary heart disease in two independent German study populations. J. Nutr. 2005, 135, 1981–1988. [Google Scholar] [PubMed]
- Lipoeto, N.I.; Agus, Z.; Oenzil, F.; Wahlqvist, M.; Wattanapenpaiboon, N. Dietary intake and the risk of coronary heart disease among the coconut-consuming Minangkabau in West Sumatra, Indonesia. Asia Pac. J. Clin. Nutr. 2004, 13, 377–378. [Google Scholar] [PubMed]
- Tucker, K.L.; Hallfrisch, J.; Qiao, N.; Muller, D.; Andres, R.; Fleg, J.L. The combination of high fruit and vegetable and low saturated fat intakes is more protective against mortality in aging men than is either alone: The Baltimore Longitudinal Study of Aging. J. Nutr. 2005, 135, 556–561. [Google Scholar] [PubMed]
- McNaughton, S.A.; Mishra, G.D.; Brunner, E.J. Food patterns associated with blood lipids are predictive of coronary heart disease: The Whitehall II study. Br. J. Nutr. 2009, 102, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.C.; Chiuve, S.E.; Buring, J.E.; Ridker, P.M.; Glynn, R.J. Comparison of associations of adherence to a Dietary Approaches to Stop Hypertension (DASH)-style diet with risks of cardiovascular disease and venous thromboembolism. J. Thromb. Haemost. 2012, 10, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Garcia-Lopez, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, K.; Iso, H.; Date, C.; Kikuchi, S.; Watanabe, Y.; Wada, Y.; Inaba, Y.; Tamakoshi, A. Dietary patterns and risk of cardiovascular deaths among middle-aged Japanese: JACC Study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 519. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, W.C. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [PubMed]
- US Government. Alcoholic Beverages: Dietary Guidelines for Americans 2005; US Government Printing Office: Washington, DC, USA, 2005.
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillon, P.; Rodriguez-Artalejo, F.; Tormo, M.J.; Sánchez, M.J.; Rodríguez, L.; Quirós, J.R.; Navarro, C.; Molina, E.; Martínez, C.; Marín, P.; et al. Major dietary patterns and risk of coronary heart disease in middle-aged persons from a Mediterranean country: The EPIC-Spain cohort study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Fernandez-Jarne, E.; Serrano-Martinez, M.; Marti, A.; Martinez J, A.; Martin-Moreno, J.M. Mediterranean diet and reduction in the risk of a first acute myocardial infarction: An operational healthy dietary score. Eur. J. Nutr. 2002, 41, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, T.; Kuriyama, S.; Hozawa, A.; Ohmori, K.; Sato, Y.; Nakaya, N.; Nishino, Y.; Tsubono, Y.; Tsuji, I. Dietary patterns and cardiovascular disease mortality in Japan: A prospective cohort study. Int. J. Epidemiol. 2007, 36, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Arriola, L.; Martinez-Camblor, P.; Larranaga, N.; Basterretxea, M.; Amiano, P.; Moreno-Iribas, C.; Carracedo, R.; Agudo, A.; Ardanaz, E.; Barricarte, A.; et al. Alcohol intake and the risk of coronary heart disease in the Spanish EPIC cohort study. Heart 2010, 96, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Beulens, J.W.; Rimm, E.B.; Ascherio, A.; Spiegelman, D.; Hendriks, H.F.; Mukamal, K.J. Alcohol consumption and risk for coronary heart disease among men with hypertension. Ann. Intern. Med. 2007, 146, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Bos, S.; Grobbee, D.E.; Boer, J.M.; Verschuren, W.M.; Beulens, J.W. Alcohol consumption and risk of cardiovascular disease among hypertensive women. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Jarne, E.; Martinez-Losa, E.; Serrano-Martinez, M.; Prado-Santamaria, M.; Brugarolas-Brufau, C.; Martinez-Gonzalez, M.A. Type of alcoholic beverage and first acute myocardial infarction: A case-control study in a Mediterranean country. Clin. Cardiol. 2003, 26, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.D.; Chambless, L.E.; Folsom, A.R.; Eigenbrodt, M.L.; Duncan, B.B.; Gilbert, A.; Szklo, M. Association between alcoholic beverage consumption and incidence of coronary heart disease in whites and blacks: The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2004, 160, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Ikehara, S.; Iso, H.; Yamagishi, K.; Yamamoto, S.; Inoue, M.; Tsugane, S. Alcohol consumption, social support, and risk of stroke and coronary heart disease among Japanese men: The JPHC Study. Alcohol. Clin. Exp. Res. 2009, 33, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Ikehara, S.; Iso, H.; Toyoshima, H.; Date, C.; Yamamoto, A.; Kikuchi, S.; Kondo, T.; Watanabe, Y.; Koizumi, A.; Wada, Y.; et al. Alcohol consumption and mortality from stroke and coronary heart disease among Japanese men and women: The Japan collaborative cohort study. Stroke 2008, 39, 2936–2942. [Google Scholar] [CrossRef] [PubMed]
- Ikehara, S.; Iso, H.; Yamagishi, K.; Kokubo, Y.; Saito, I.; Yatsuya, H.; Inoue, M.; Tsugane, S. Alcohol consumption and risk of stroke and coronary heart disease among Japanese women: The Japan Public Health Center-based prospective study. Prev. Med. 2013, 57, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J.; Chiuve, S.E.; Rimm, E.B. Alcohol consumption and risk for coronary heart disease in men with healthy lifestyles. Arch. Intern. Med. 2006, 166, 2145–2150. [Google Scholar] [CrossRef] [PubMed]
- Keil, U.; Chambless, L.E.; Doring, A.; Filipiak, B.; Stieber, J. The relation of alcohol intake to coronary heart disease and all-cause mortality in a beer-drinking population. Epidemiology 1997, 8, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Kono, S.; Handa, K.; Kawano, T.; Hiroki, T.; Ishihara, Y.; Arakawa, K. Alcohol intake and nonfatal acute myocardial infarction in Japan. Am. J. Cardiol. 1991, 68, 1011–1014. [Google Scholar] [CrossRef]
- Schroder, H.; Masabeu, A.; Marti, M.J.; Cols, M.; Lisbona, J.M.; Romagosa, C.; Carión, T.; Vilert, E.; Marrugat, J. Myocardial infarction and alcohol consumption: A population-based case-control study. Nutr. Metab. Cardiovasc. Dis. 2007, 7, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.; Broad, J.; Jackson, R. Alcohol consumption and its contribution to the burden of coronary heart disease in middle-aged and older New Zealanders: A population-based case-control study. N. Z. Med. J. 2004, 117, 793. [Google Scholar]
- Kitamura, A.; Iso, H.; Sankai, T.; Naito, Y.; Sato, S.; Kiyama, M.; Okamura, T.; Nakagawa, Y.; Iida, M.; Shimamoto, Y.; et al. Alcohol intake and premature coronary heart disease in urban Japanese men. Am. J. Epidemiol. 1998, 147, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J.; Chung, H.; Jenny, N.S.; Kuller, L.H.; Longstreth, W.T.; Mittleman, M.A.; Burke, G.L.; Cushman, M.; Psaty, B.M.; Siscovick, D.S. Alcohol consumption and risk of coronary heart disease in older adults: The Cardiovascular Health Study. J. Am. Geriatr. Soc. 2006, 54, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Solomon, C.G.; Hu, F.B.; Stampfer, M.J.; Colditz, G.A.; Speizer, F.E.; Rimm, E.B.; Willett, W.C.; Manson, J.E. Moderate alcohol consumption and risk of coronary heart disease among women with type 2 diabetes mellitus. Circulation 2000, 102, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Gu, D.; Reynolds, K.; Chen, J.; Wu, X.; Chen, C.S.; Duan, X.; Chen, J.; He, J. Alcohol consumption and risk of coronary heart disease among Chinese men. Int. J. Cardiol. 2009, 135, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Hvidtfeldt, U.A.; Tolstrup, J.S.; Jakobsen, M.U.; Heitmann, B.L.; Grønbaek, M.; O'Reilly, E.; Bälter, K.; Goldbourt, U.; Hallmans, G.; Knekt, P.; et al. Alcohol intake and risk of coronary heart disease in younger, middle-aged, and older adults. Circulation 2010, 121, 1589–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajpathak, S.N.; Freiberg, M.S.; Wang, C.; Wylie-Rosett, J.; Wildman, R.P.; Rohan, T.E.; Robinson, J.G.; Liu, S.; Wassertheil-Smoller, S. Alcohol consumption and the risk of coronary heart disease in postmenopausal women with diabetes: Women’s Health Initiative Observational Study. Eur. J. Nutr. 2010, 49, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Li, F.; Wang, Y.; Ou, Z.; Xu, D.; Tan, W.; Dai, A. Association between dietary patterns and coronary heart disease: A meta-analysis of prospective cohort studies. Int. J. Clin. Exp. Med. 2015, 8, 781–790. [Google Scholar] [PubMed]
- Li, F.; Hou, L.N.; Chen, W.; Chen, P.L.; Lei, C.Y.; Wei, Q.; Tan, W.L.; Zheng, S.B. Associations of dietary patterns with the risk of all-cause, CVD and stroke mortality: A meta-analysis of prospective cohort studies. Br. J. Nutr. 2014, 113, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [PubMed]
- Clarke, R. Lowering blood homocysteine with folic acid based supplements: Meta-analysis of randomized trials. Indian Heart J. 2000, 52 (Suppl. S7), S59–S64. [Google Scholar] [PubMed]
- Elkelboom, J.W.; Lonn, E.; Genest, J., Jr.; Hankey, G.; Yusuf, S. Homocysteine and cardiovascular disease: A critical review of the epidemiologic evidence. Ann. Intern. Med. 1999, 131, 363–375. [Google Scholar] [CrossRef]
- Pereira, M.A.; O’ Reilly, E.; Augustsson, K.; Fraser, G.E.; Goldbourt, U.; Heitmann, B.L.; Hallmans, G.; Knekt, P.; Liu, S.; Pietinen, P.; et al. Dietary fiber and risk of coronary heart disease: A pooled analysis of cohort studies. Arch. Intern. Med. 2004, 164, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Qian, Y.; Pan, Y.; Li, P.; Yang, J.; Ye, X.; Xu, G. Association between dietary fiber intake and risk of coronary heart disease: A meta-analysis. Clin. Nutr. 2015, 34, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Van Duyn, M.A.; Pivonka, E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: Selected literature. J. Am. Diet. Assoc. 2000, 10, 1511–1521. [Google Scholar] [CrossRef]
- Bazzano, L.A.; Serdual, M.K.; Liu, S. Dietary intake of fruits and vegetables and risk of cardiovascular disease. Curr. Atheroscler. Rep. 2003, 5, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Steffen, L.M.; Kroenke, C.H.; Yu, X.; Pereira, M.A.; Slattery, M.L.; Van Horn, L.; Gross, M.D.; Jacobs, D.R., Jr.; et al. Associations of plant food, dairy product, and meat intakes with 15-y incidence of elevated blood pressure in young black and white adults: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Clin. Nutr. 2005, 82, 1169–1177. [Google Scholar] [PubMed]
- Lakshmi, V.M.; Schut, H.A.; Zenser, T.V. 2-Nitrosoamino-3-methylimidazo [4,5-f] quinoline activated by the inflammatory response forms nucleotide adducts. Food Chem. Toxicol. 2005, 43, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Bogen, K.T.; Keating, G.A. U.S. dietary exposures to heterocyclic amines. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 155–168. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Effect of modest salt reduction on blood pressure: A meta-analysis ofrandomized trials. Implications for public health. J. Hum. Hypertens. 2002, 16, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Williams, P.; Fosher, K.; Criqui, M.; Stampfer, M.J. Moderate alcohol intake and lower risk of coronary heart disease: Meta-analysis of effects on lipids and haemostatic factors. BMJ 1999, 319, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Castelli, W.P.; Doyle, J.T.; Gordon, T.; Hames, C.G.; Hjortland, M.C.; Hulley, S.B.; Kagan, A.; Zukel, W.J. Alcohol and blood lipids. The Cooperative Lipoprotein Phenotyping Study. Lancet 1977, 2, 153–155. [Google Scholar] [CrossRef]
- Hulley, S.B.; Gordon, S. Alcohol and high-density lipoprotein cholesterol: Causal inference from diverse study designs. Circulation 1981, 64, 57–63. [Google Scholar]
- Moncada, S.; Randomski, N.W. The problems and the promise of prostaglandin influences in atherogenesis. Ann. N. Y. Acad. Sci. 1985, 454, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.; Sparrow, D.; Weiss, S.T. Alcohol intake and insulin levels: The Normative Aging Study. Am. J. Epidemiol. 1997, 145, 909–916. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.-Y.; Shu, L.; Si, C.-J.; Yu, X.-L.; Liao, D.; Gao, W.; Zhang, L.; Zheng, P.-F. Dietary Patterns, Alcohol Consumption and Risk of Coronary Heart Disease in Adults: A Meta-Analysis. Nutrients 2015, 7, 6582-6605. https://doi.org/10.3390/nu7085300
Zhang X-Y, Shu L, Si C-J, Yu X-L, Liao D, Gao W, Zhang L, Zheng P-F. Dietary Patterns, Alcohol Consumption and Risk of Coronary Heart Disease in Adults: A Meta-Analysis. Nutrients. 2015; 7(8):6582-6605. https://doi.org/10.3390/nu7085300
Chicago/Turabian StyleZhang, Xiao-Yan, Long Shu, Cai-Juan Si, Xiao-Long Yu, Dan Liao, Wei Gao, Lun Zhang, and Pei-Fen Zheng. 2015. "Dietary Patterns, Alcohol Consumption and Risk of Coronary Heart Disease in Adults: A Meta-Analysis" Nutrients 7, no. 8: 6582-6605. https://doi.org/10.3390/nu7085300