Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Automated Multiple-Pass Method (AMPM)
2.2. Development of the Organized Food List
2.3. Search Engine
2.4. Reminders and Assistance
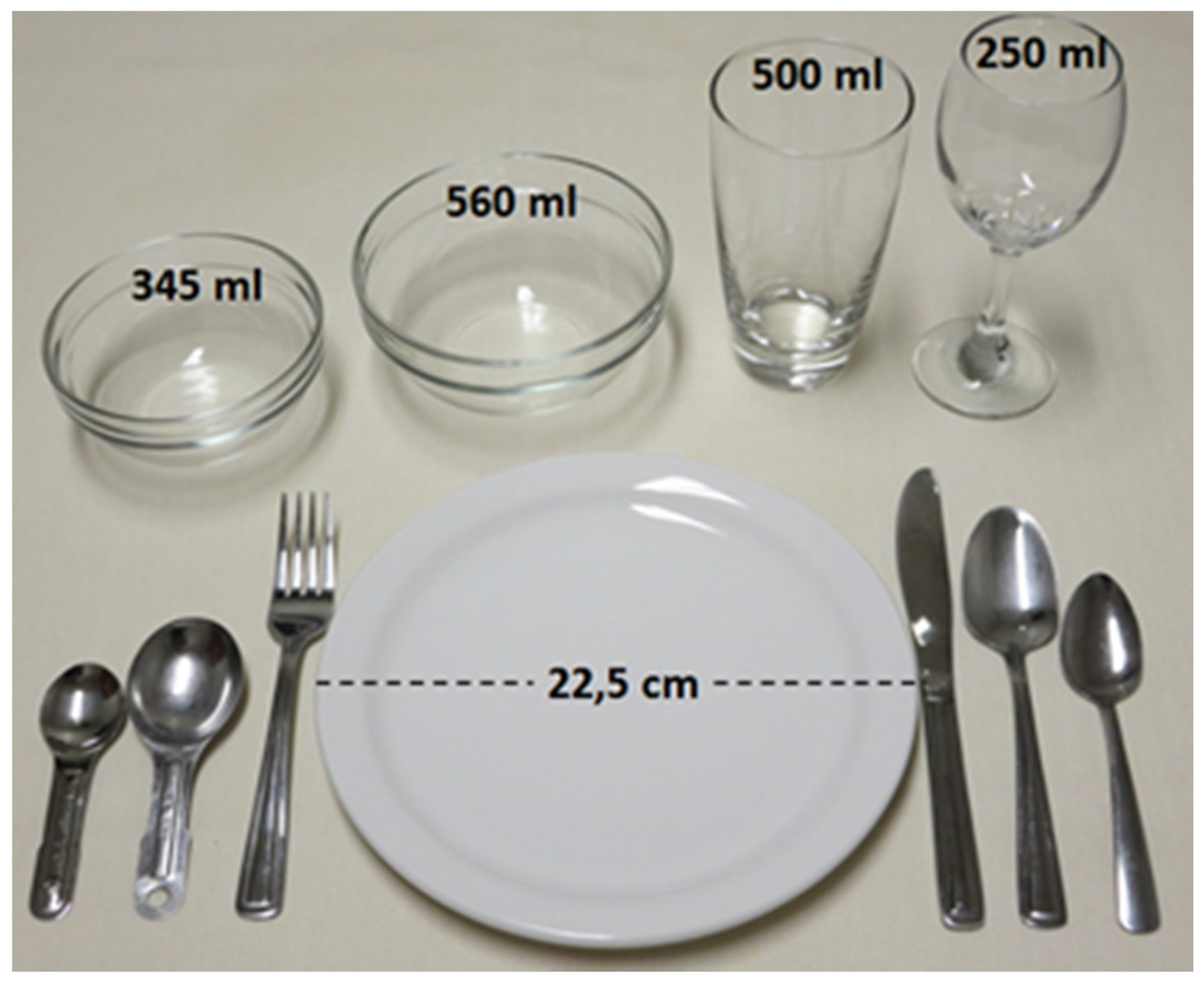
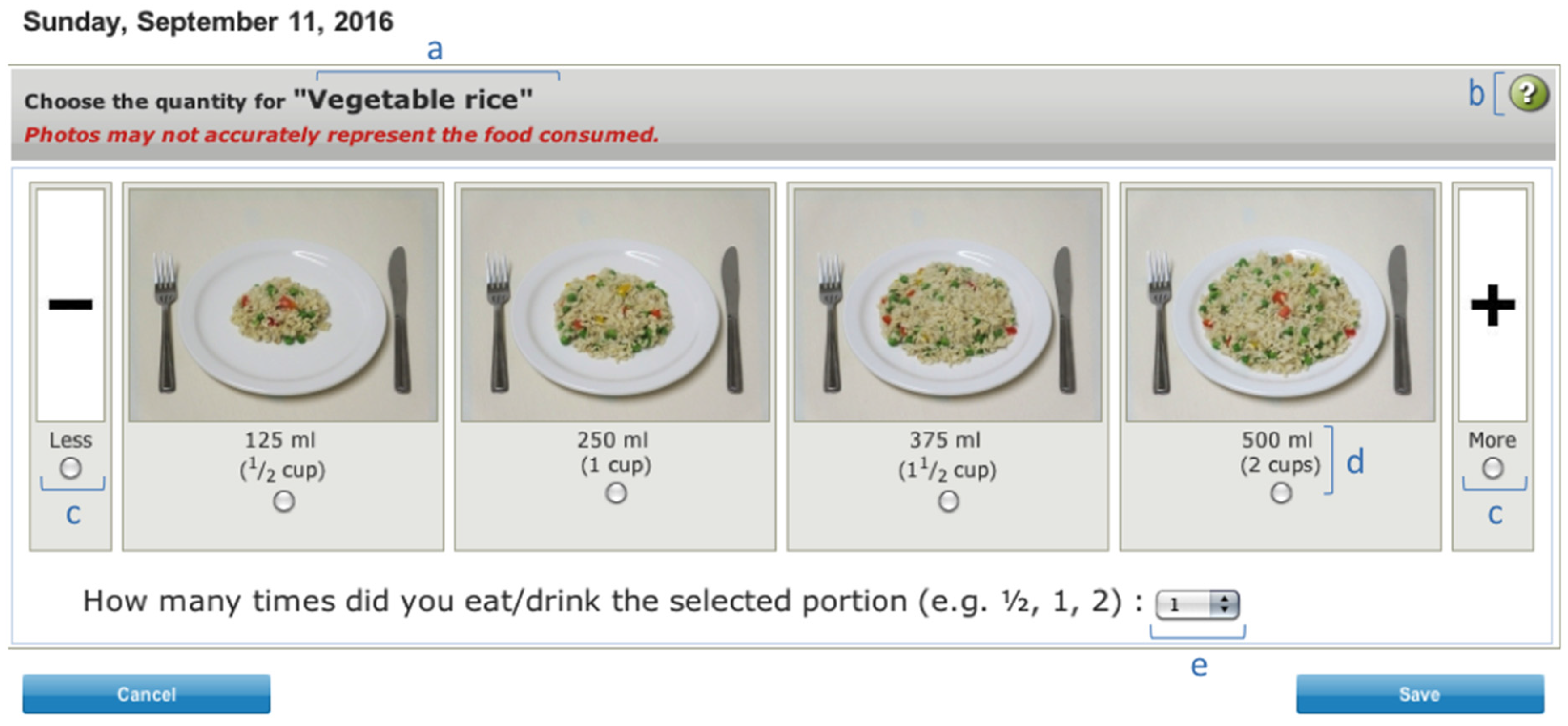
2.5. Portion-Size Estimation
2.6. Frequently Forgotten Food
2.7. Strategies for Automatic Coding
2.8. Supplementary Questionnaire
2.9. Pre-Test
3. Results
Pre-Test
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bingham, S.A.; Luben, R.; Welch, A.; Wareham, N.; Khaw, K.T.; Day, N. Are imprecise methods obscuring a relation between fat and breast cancer? Lancet 2003, 362, 212–214. [Google Scholar] [CrossRef]
- Kipnis, V.; Midthune, D.; Freedman, L.; Bingham, S.; Day, N.E.; Riboli, E.; Ferrari, P.; Carroll, R.J. Bias in dietary-report instruments and its implications for nutritional epidemiology. Public Health Nutr. 2002, 5, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, V.; Midthune, D.; Freedman, L.S.; Bingham, S.; Schatzkin, A.; Subar, A.; Carroll, R.J. Empirical evidence of correlated biases in dietary assessment instruments and its implications. Am. J. Epidemiol. 2001, 153, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Illner, A.K.; Freisling, H.; Boeing, H.; Huybrechts, I.; Crispim, S.P.; Slimani, N. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int. J. Epidemiol. 2012, 41, 1187–1203. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T. 24-h recall and diet record methods. In Nutritional Epidemiology, 3rd ed.; Willett, W., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 49–69. [Google Scholar]
- Falomir, Z.; Arregui, M.; Madueno, F.; Corella, D.; Coltell, O. Automation of food questionnaires in medical studies: A state-of-the-art review and future prospects. Comput. Biol. Med. 2012, 42, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Arab, L.; Wesseling-Perry, K.; Jardack, P.; Henry, J.; Winter, A. Eight self-administered 24-h dietary recalls using the internet are feasible in african americans and whites: The energetics study. J. Am. Diet. Assoc. 2010, 110, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Mejean, C.; Szabo de Edelenyi, F.; Touvier, M.; Kesse-Guyot, E.; Julia, C.; Andreeva, V.A.; Hercberg, S. Motives for participating in a web-based nutrition cohort according to sociodemographic, lifestyle, and health characteristics: The nutrinet-sante cohort study. J. Med. Internet Res. 2014, 16, e189. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Dixit-Joshi, S.; Potischman, N.; Dodd, K.W.; Kirkpatrick, S.I.; Kushi, L.H.; Alexander, G.L.; Coleman, L.A.; Zimmerman, T.P.; Sundaram, M.E.; et al. Comparison of interviewer-administered and automated self-administered 24-h dietary recalls in 3 diverse integrated health systems. Am. J. Epidemiol. 2015, 181, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Frankenfeld, C.L.; Poudrier, J.K.; Waters, N.M.; Gillevet, P.M.; Xu, Y. Dietary intake measured from a self-administered, online 24-h recall system compared with 4-day diet records in an adult us population. J. Acad. Nutr. Diet. 2012, 112, 1642–1647. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, S.I.; Subar, A.F.; Douglass, D.; Zimmerman, T.P.; Thompson, F.E.; Kahle, L.L.; George, S.M.; Dodd, K.W.; Potischman, N. Performance of the automated self-administered 24-h recall relative to a measure of true intakes and to an interviewer-administered 24-h recall. Am. J. Clin. Nutr. 2014, 100, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Arab, L.; Tseng, C.H.; Ang, A.; Jardack, P. Validity of a multipass, web-based, 24-h self-administered recall for assessment of total energy intake in blacks and whites. Am. J. Epidemiol. 2011, 174, 1256–1265. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Diet quality in canada. Health Rep. 2009, 20, 41–52. [Google Scholar] [PubMed]
- Goulet, J.; Lamarche, B.; Nadeau, G.; Lemieux, S. Effect of a nutritional intervention promoting the mediterranean food pattern on plasma lipids, lipoproteins and body weight in healthy french-canadian women. Atherosclerosis 2003, 170, 115–124. [Google Scholar] [CrossRef]
- National Cancer Institute. Asa24-canada-2014. Available online: http://appliedresearch.cancer.gov/asa24/respondent/canada.html (accessed on 16 April 2015).
- Thompson, F.E.; Subar, A.F. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease; Academic Press: San Diego, CA, USA, 2013; pp. 4–46. [Google Scholar]
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of usda’s dietary intake data system. J. Food. Compos. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- Subar, A.F.; Thompson, F.E.; Potischman, N.; Forsyth, B.H.; Buday, R.; Richards, D.; McNutt, S.; Hull, S.G.; Guenther, P.M.; Schatzkin, A.; et al. Formative research of a quick list for an automated self-administered 24-h dietary recall. J. Am. Diet. Assoc. 2007, 107, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The automated self-administered 24-h dietary recall (ASA24): A resource for researchers, clinicians, and educators from the national cancer institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Nutrient File (cnf). Available online: http://webprod3.hc-sc.gc.ca/cnf-fce/language-langage.do?url=t.search.recherche&lang=eng (accessed on 24 March 2015).
- Zimmerman, T.P.; Hull, S.G.; McNutt, S.; Mittl, B.; Islam, N.; Guenther, P.M.; Thompson, F.E.; Potischman, N.A.; Subar, A.F. Challenges in converting an interviewer-administered food probe database to self-administration in the national cancer institute automated self-administered 24-h recall (ASA24). J. Food Compost. Anal. 2009, 22, S48–S51. [Google Scholar] [CrossRef] [PubMed]
- Touvier, M.; Kesse-Guyot, E.; Mejean, C.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Comparison between an interactive web-based self-administered 24 h dietary record and an interview by a dietitian for large-scale epidemiological studies. Br. J. Nutr. 2011, 105, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Nutrient Value of Some Common Foods-Booklet. Available online: http://www.hc-sc.gc.ca/fn-an/nutrition/fiche-nutri-data/nutrient_value-valeurs_nutritives-tc-tm-eng.php-a1 (accessed on 24 March 2015).
- Agriculture and Agri-Food Canada. The Specialty Food Market in North America. Available online: http://www.agr.gc.ca/eng/industry-markets-and-trade/statistics-and-market-information/agriculture-and-food-market-information-by-region/canada/the-specialty-food-market-in-north-america/?id=1410083148460 (accessed on 5 June 2016).
- Leblanc, V.; Begin, C.; Hudon, A.M.; Royer, M.M.; Corneau, L.; Dodin, S.; Lemieux, S. Gender differences in the long-term effects of a nutritional intervention program promoting the mediterranean diet: Changes in dietary intakes, eating behaviors, anthropometric and metabolic variables. Nutr. J. 2014, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute (N.C.I.). Automated Self-Administered 24-H Recall (asa24). Available online: http://appliedresearch.cancer.gov/asa24/ (accessed on 18 February 2015).
- Nelson, M.; Atkinson, M.; Darbyshire, S. Food photography. I: The perception of food portion size from photographs. Br. J. Nutr. 1994, 72, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Vigneault, J.; Lemieux, S.; Garneau, V.; Weisnagel, S.J.; Tchernof, A.; Robitaille, J. Association between metabolic deteriorations and prior gestational diabetes according to weight status. Obesity 2015, 23, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Allaire, J.; Couture, P.; Leclerc, M.; Charest, A.; Marin, J.; Lepine, M.C.; Talbot, D.; Tchernof, A.; Lamarche, B. Randomized, crossover, head-to-head comparison of epa and dha supplementation to reduce inflammation markers in men and women: The comparing epa to dha study. Am. J. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.P.; Gagnon, J.; Labonte, M.E.; Desroches, S.; Charest, A.; Grenier, G.; Dodin, S.; Lemieux, S.; Couture, P.; Lamarche, B. Impact of milk consumption on cardiometabolic risk in postmenopausal women with abdominal obesity. Nutr. J. 2015, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Labonte, M.E.; Cyr, A.; Abdullah, M.M.; Lepine, M.C.; Vohl, M.C.; Jones, P.; Couture, P.; Lamarche, B. Dairy product consumption has no impact on biomarkers of inflammation among men and women with low-grade systemic inflammation. J. Nutr. 2014, 144, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Baril-Gravel, L.; Labonte, M.E.; Couture, P.; Vohl, M.C.; Charest, A.; Guay, V.; Jenkins, D.A.; Connelly, P.W.; West, S.; Kris-Etherton, P.M.; et al. Docosahexaenoic acid-enriched canola oil increases adiponectin concentrations: A randomized crossover controlled intervention trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.P.; Gigleux, I.; Tremblay, A.J.; Poirier, L.; Lamarche, B.; Couture, P. Impact of dairy consumption on essential hypertension: A clinical study. Nutr. J. 2014, 13, 83. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, A.J.; Lamarche, B.; Deacon, C.F.; Weisnagel, S.J.; Couture, P. Effects of sitagliptin therapy on markers of low-grade inflammation and cell adhesion molecules in patients with type 2 diabetes. Metabolism 2014, 63, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Conway, V.; Couture, P.; Gauthier, S.; Pouliot, Y.; Lamarche, B. Effect of buttermilk consumption on blood pressure in moderately hypercholesterolemic men and women. Nutrition 2014, 30, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Paradis, M.E.; Couture, P.; Lamarche, B. A randomised crossover placebo-controlled trial investigating the effect of brown seaweed (ascophyllum nodosum and fucus vesiculosus) on postchallenge plasma glucose and insulin levels in men and women. Appl. Physiol. Nutr. Metab. 2011, 36, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Paradis, M.E.; Couture, P.; Gigleux, I.; Marin, J.; Vohl, M.C. Impact of systemic enzyme supplementation on low-grade inflammation in humans. Pharma Nutr. 2015, 3, 83–88. [Google Scholar] [CrossRef]
- Labonte, M.E.; Cyr, A.; Baril-Gravel, L.; Royer, M.M.; Lamarche, B. Validity and reproducibility of a web-based, self-administered food frequency questionnaire. Eur. J. Clin. Nutr. 2012, 66, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Canadian Community Health Survey 2004—User Guide for the Public Use Microdata. Available online: http://data.library.utoronto.ca/datapub/codebooks/cstdli/cchs/cycle2_2/guide_e.pdf (accessed on 28 September 2016).
- United States Department of Agriculture. National Nutrient Database for Standard Reference. Available online: http://ndb.nal.usda.gov/ndb/search (accessed on 23 March 2015).
- Laval University. Nutrific. Available online: https://nutrific.fsaa.ulaval.ca (accessed on 6 July 2015).
- Health Canada. Eating Well with Canada’s Food Guide. Available online: http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/view_eatwell_vue_bienmang-eng.pdf (accessed on 26 March 2015).
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; Otten, J.J., Hellwig, J.P., Meyers, L.D., Eds.; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Craig, M.R.; Kristal, A.R.; Cheney, C.L.; Shattuck, A.L. The prevalence and impact of 'atypical’ days in 4-day food records. J. Am. Diet. Assoc. 2000, 100, 421–427. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Hanning, R.M.; Lambraki, I.; Storey, K.E.; McCargar, L. Healthy eating index-c is compromised among adolescents with body weight concerns, weight loss dieting, and meal skipping. Body Image 2008, 5, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Islam, N.; Douglass, D.; Dadabhoy, H.; Beltran, A.; Baranowski, J.; Thompson, D.; Cullen, K.W.; Subar, A.F. Food intake recording software system, version 4 (firsst4): A self-completed 24-h dietary recall for children. J. Hum. Nutr. Diet. 2014, 27, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.; Hawkins, A.; Delve, J.; Adamson, A.J. Reducing the cost of dietary assessment: Self-completed recall and analysis of nutrition for use with children (SCRAN24). J. Hum. Nutr. Diet. 2014, 27, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Albar, S.A.; Morris, M.A.; Mulla, U.Z.; Hancock, N.; Evans, C.E.; Alwan, N.A.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S.; et al. Development of a uk online 24-h dietary assessment tool: Myfood24. Nutrients 2015, 7, 4016–4032. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.; Anderson, J.; Gould, S.M. Comparative validation of a bilingual interactive multimedia dietary assessment tool. J. Am. Diet. Assoc. 2005, 105, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- De Keyzer, W.; Huybrechts, I.; De Maeyer, M.; Ocke, M.; Slimani, N.; van’t Veer, P.; De Henauw, S. Food photographs in nutritional surveillance: Errors in portion size estimation using drawings of bread and photographs of margarine and beverages consumption. Br. J. Nutr. 2011, 105, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Kirkcaldy-Hargreaves, M.; Lynch, G.W. Assessment of the validity of four food models. J. Cancer Diet. Assoc. 1980, 41, 102–110. [Google Scholar]
- Subar, A.F.; Crafts, J.; Zimmerman, T.P.; Wilson, M.; Mittl, B.; Islam, N.G.; McNutt, S.; Potischman, N.; Buday, R.; Hull, S.G.; et al. Assessment of the accuracy of portion size reports using computer-based food photographs aids in the development of an automated self-administered 24-h recall. J. Am. Diet. Assoc. 2010, 110, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Masset, G.; Scarborough, P.; Rayner, M.; Mishra, G.; Brunner, E.J. Can nutrient profiling help to identify foods which diet variety should be encouraged? Results from the whitehall ii cohort. Br. J. Nutr. 2015, 113, 1800–1809. [Google Scholar] [CrossRef] [PubMed]
- Brody, R.A.; Byham-Gray, L.; Touger-Decker, R.; Passannante, M.R.; Rothpletz Puglia, P.; O’Sullivan Maillet, J. What clinical activities do advanced-practice registered dietitian nutritionists perform? Results of a delphi study. J. Acad. Nutr. Diet. 2014, 114, 718–733. [Google Scholar] [CrossRef] [PubMed]
- Probst, Y.C.; Tapsell, L.C. What to ask in a self-administered dietary assessment website: The role of professional judgement. J. Food Compos. Anal. 2007, 20, 696–703. [Google Scholar] [CrossRef]
- Liu, B.; Young, H.; Crowe, F.L.; Benson, V.S.; Spencer, E.A.; Key, T.J.; Appleby, P.N.; Beral, V. Development and evaluation of the oxford webq, a low-cost, web-based method for assessment of previous 24 h dietary intakes in large-scale prospective studies. Public Health Nutr. 2011, 14, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013; p. 529. [Google Scholar]
- Probst, Y.C.; Faraji, S.; Batterham, M.; Steel, D.G.; Tapsell, L.C. Computerized dietary assessments compare well with interviewer administered diet histories for patients with type 2 diabetes mellitus in the primary healthcare setting. Patient Educ. Couns. 2008, 72, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Islam, N.; Baranowski, J.; Martin, S.; Beltran, A.; Dadabhoy, H.; Adame, S.H.; Watson, K.B.; Thompson, D.; Cullen, K.W.; et al. Comparison of a web-based versus traditional diet recall among children. J. Acad. Nutr. Diet. 2012, 112, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.J.; Ells, L.J.; McLure, S.A.; Crooks, S.; Cumbor, D.; Summerbell, C.D.; Batterham, A.M. The development and evaluation of a novel computer program to assess previous-day dietary and physical activity behaviours in school children: The synchronised nutrition and activity program (SNAP). Br. J. Nutr. 2008, 99, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Covents, M.; Matthys, C.; Maes, L. Young adolescents' nutrition assessment on computer (yana-c). Eur. J. Clin. Nutr. 2005, 59, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Douglass, D.; Islam, N.; Baranowski, J.; Chen, T.A.; Subar, A.F.; Zimmerman, T.P.; Baranowski, T. Simulated adaptations to an adult dietary self-report tool to accommodate children: Impact on nutrient estimates. J. Am. Coll. Nutr. 2013, 32, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.J.; Midthune, D.; Subar, A.F.; Shumakovich, M.; Freedman, L.S.; Thompson, F.E.; Kipnis, V. Taking advantage of the strengths of 2 different dietary assessment instruments to improve intake estimates for nutritional epidemiology. Am. J. Epidemiol. 2012, 175, 340–347. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute (N.C.I.). Recommendations on Potential Approaches to Dietary Assessment for Different Research Objectives Requiring Group-Level Estimates. Available online: http://dietassessmentprimer.cancer.gov/approach/table.html (accessed on 26 March 2015).




{kind=link}
{kind=link}
{kind=link}
| Number of Pictures Used for the Portion-Size Estimation | Proportion of Food Items (%) |
|---|---|
| 0 | 17.7% |
| 1 | 2.8% |
| 2 | 3.3% |
| 3 | 2.6% |
| 4 | 72.8% |
| 8 | 0.8% |
| Characteristics | n (%) |
|---|---|
| Age (years) | 46.3 ± 14.1 1 |
| 16–24 | 1 (3) |
| 25–44 | 11 (38) |
| 45–64 | 13 (45) |
| 65 or older | 4 (14) |
| Sex | |
| Male | 13 (45) |
| Female | 16 (55) |
| Education level | |
| Less than high school | 1 (3) |
| High school | 6 (21) |
| College | 9 (31) |
| University | 13 (45) |
| Self-assessed computer skills | |
| Poor/medium | 7 (24) |
| Good | 7 (24) |
| Very good/excellent | 15 (52) |
| Involvement in meal preparation | |
| Never | 3 (10) |
| Rarely/sometimes | 3 (10) |
| Often/most of the time | 23 (79) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacques, S.; Lemieux, S.; Lamarche, B.; Laramée, C.; Corneau, L.; Lapointe, A.; Tessier-Grenier, M.; Robitaille, J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients 2016, 8, 724. https://doi.org/10.3390/nu8110724
Jacques S, Lemieux S, Lamarche B, Laramée C, Corneau L, Lapointe A, Tessier-Grenier M, Robitaille J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients. 2016; 8(11):724. https://doi.org/10.3390/nu8110724
Chicago/Turabian StyleJacques, Simon, Simone Lemieux, Benoît Lamarche, Catherine Laramée, Louise Corneau, Annie Lapointe, Maude Tessier-Grenier, and Julie Robitaille. 2016. "Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population" Nutrients 8, no. 11: 724. https://doi.org/10.3390/nu8110724