Sleep Duration and Chronic Fatigue Are Differently Associated with the Dietary Profile of Shift Workers



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Processing and Statistical Analysis
3. Results
3.1. Participants
3.2. Daily Energy Intake
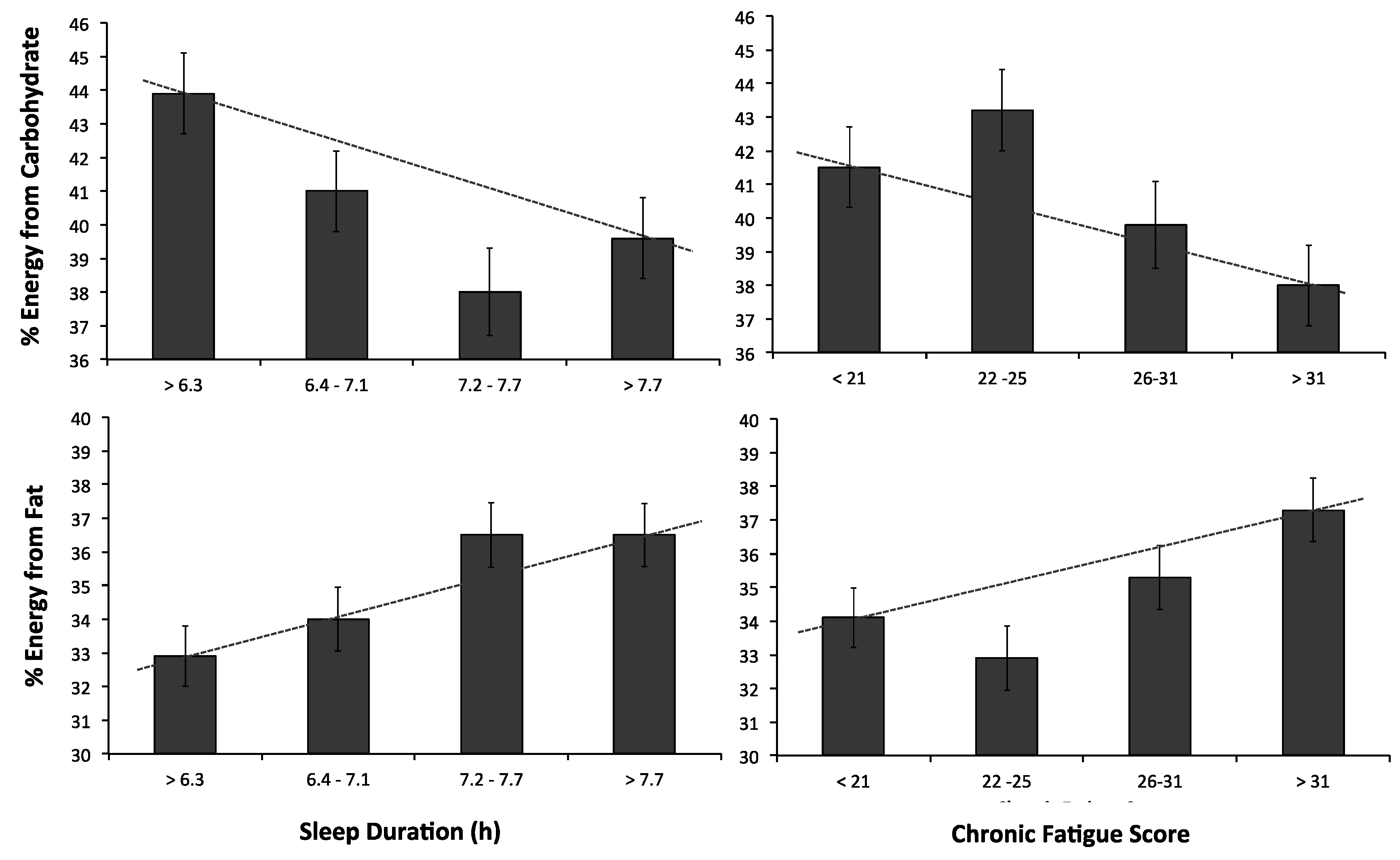
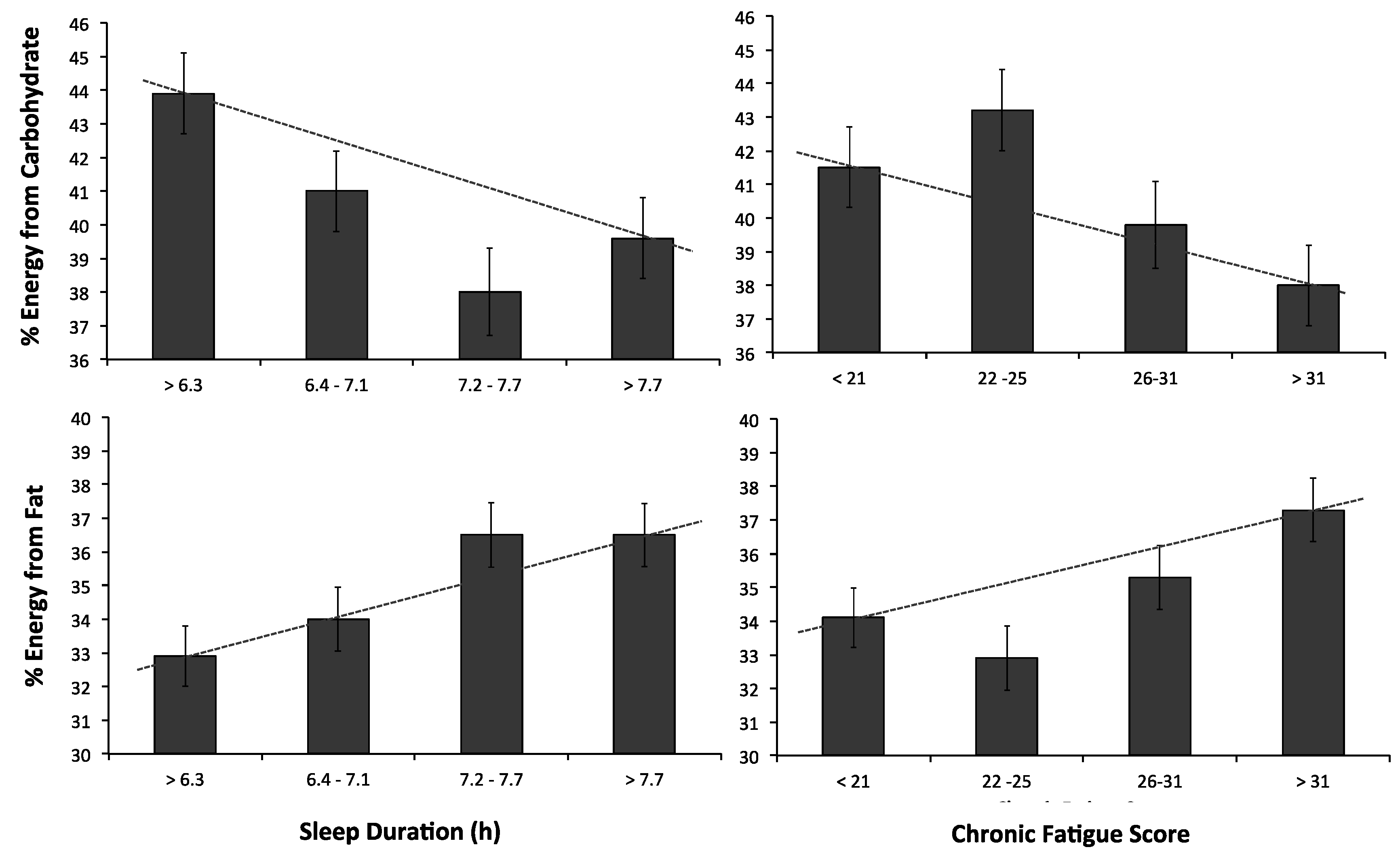
3.3. Carbohydrate as a Percentage of Daily Energy Intake
3.4. Protein as a Percentage of Daily Energy Intake
3.5. Fat as a Percentage of Daily Energy Intake
3.6. Saturated Fat as a Percentage of Daily Energy Intake
3.7. Alcohol as a Percentage of Daily Energy Intake
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CHO | Carbohydrate |
| FFQ | Food frequency questionnaire |
| SSI | Standard shift work index |
| ANOVA | Analysis of variance |
| kJ | Kilojoules |
| SFA | Saturated fat |
| R | Rotating |
| g | Grams |
| SE | Standard error |
| LLCI | Lower limit confidence interval |
| ULCI | Upper limit confidence interval |
| Cum | Cumulative |
| kg | Kilograms |
| m2 | Meters squared |
References
- Australian Bureau of Statistics. Working Time Arrangements, Australia, November 2012. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/6342.0 (accessed on 18 November 2016).
- Akerstedt, T. Shift work and disturbed sleep/wakefulness. Occup. Med. 2003, 53, 89–94. [Google Scholar] [CrossRef]
- Costa, G. Shift work and occupational medicine: An overview. Occup. Med. 2003, 53, 83–88. [Google Scholar] [CrossRef]
- Paley, M.J.; Tepas, D.I. Fatigue and the shiftworker: Firefighters working on a rotating shift schedule. J. Hum. Factors Ergon. Soc. 1994, 36, 269–284. [Google Scholar]
- Åkerstedt, T.; Wright, K.P. Sleep loss and fatigue in shift work and shift work disorder. Sleep Med. Clin. 2009, 4, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Arendt, J. Shift work: Coping with the biological clock. Occup. Med. 2010, 60, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Tolley, C.; Lamond, N.; van den Heuvel, C.; Pincombe, J.; Rogers, A.E.; Drew, D. Sleep and errors in a group of australian hospital nurses at work and during the commute. Appl. Ergon. 2008, 39, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Rajaratnam, S.M.; Arendt, J. Health in a 24-h society. Lancet 2001, 358, 999–1005. [Google Scholar] [CrossRef]
- Karlsson, B.; Knutsson, A.; Lindahl, B. Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people. J. Occup. Environ. Med. 2001, 58, 747–752. [Google Scholar] [CrossRef]
- Knutsson, A.; Bøggild, H. Gastrointestinal disorders among shift workers. Scand. J. Work Environ. Health 2010, 36, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Puttonen, S.; Härmä, M.; Hublin, C. Shift work and cardiovascular disease—Pathways from circadian stress to morbidity. Scand. J. Work Environ. Health 2010, 36, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; Haus, E.; Stevens, R. Shift work and cancer—Considerations on rationale, mechanisms, and epidemiology. Scand. J. Work Environ. Health 2010, 36, 163–179. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Diet Physical Activity and Health 2015. Available online: http://www.who.int/dietphysicalactivity/diet/en/ (accessed on 18 November 2016).
- Bonham, M.P.; Bonnell, E.K.; Huggins, C.E. Energy intake of shift workers compared to fixed day workers: A systematic review and meta-analysis. Chronobiol. Int. 2016, 33, 1086–1100. [Google Scholar] [CrossRef] [PubMed]
- Hulsegge, G.; Boer, J.; van der Beek, A.; Verschuren, W.; Sluijs, I.; Vermeulen, R.; Proper, K. Shift workers have a similar diet quality but higher energy intake than day workers. Scand. J. Work Environ. Health 2016, 42, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Padilha, H.G.; Crispim, C.A.; Zimberg, I.Z.; Folkard, S.; Tufik, S.; de Mello, M.T. Metabolic responses on the early shift. Chronobiol. Int. 2010, 27, 1080–1092. [Google Scholar] [CrossRef] [PubMed]
- Schiavo-Cardozo, D.; Lima, M.M.; Pareja, J.C.; Geloneze, B. Appetite-regulating hormones from the upper gut: Disrupted control of xenin and ghrelin in night workers. Clin. Endocrinol. 2013, 79, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Hemiö, K.; Puttonen, S.; Viitasalo, K.; Härmä, M.; Peltonen, M.; Lindström, J. Food and nutrient intake among workers with different shift systems. J. Occup. Environ. Med. 2015, 72, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Miura, K.; Sasaki, S.; Yoshita, K.; Yoneyama, S.; Sakurai, M.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y. Evaluation of the effects of shift work on nutrient intake: A cross-sectional study. J. Occup. Health 2008, 50, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Balieiro, L.C.T.; Rossato, L.T.; Waterhouse, J.; Paim, S.L.; Mota, M.C.; Crispim, C.A. Nutritional status and eating habits of bus drivers during the day and night. Chronobiol. Int. 2014, 31, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Esquirol, Y.; Bongard, V.; Mabile, L.; Jonnier, B.; Soulat, J.-M.; Perret, B. Shift work and metabolic syndrome: Respective impacts of job strain, physical activity, and dietary rhythms. Chronobiol. Int. 2009, 26, 544–559. [Google Scholar] [CrossRef] [PubMed]
- Pilcher, J.J.; Lambert, B.J.; Huffcutt, A.I. Differential effects of permanent and rotating shifts on self-report sleep length: A meta-analytic review. Sleep 2000, 23, 155–163. [Google Scholar] [PubMed]
- Ingre, M.; Kecklund, G.; Åkerstedt, T.; Söderström, M.; Kecklund, L. Sleep length as a function of morning shift-start time in irregular shift schedules for train drivers: Self-rated health and individual differences. Chronobiol. Int. 2008, 25, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Martensson, J. Situations influencing habits in diet and exercise among nurses working night shift. J. Nurs. Manag. 2006, 14, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Markwald, R.R.; Melanson, E.L.; Smith, M.R.; Higgins, J.; Perreault, L.; Eckel, R.H.; Wright, K.P. Impact of insufficient sleep on total daily energy expenditure, food intake, and weight gain. Proc. Natl. Acad. Sci. USA 2013, 110, 5695–5700. [Google Scholar] [CrossRef] [PubMed]
- Brondel, L.; Romer, M.A.; Nougues, P.M.; Touyarou, P.; Davenne, D. Acute partial sleep deprivation increases food intake in healthy men. Am. J. Clin. Nutr. 2010, 91, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Schmid, S.M.; Hallschmid, M.; Jauch-Chara, K.; Wilms, B.; Benedict, C.; Lehnert, H.; Born, J.; Schultes, B. Short-term sleep loss decreases physical activity under free-living conditions but does not increase food intake under time-deprived laboratory conditions in healthy men. Am. J. Clin. Nutr. 2009, 90, 1476–1482. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, A.M.; Dinges, D.F.; Goel, N. Sex and race differences in caloric intake during sleep restriction in healthy adults. Am. J. Clin. Nutr. 2014, 100, 559–566. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Roberts, A.L.; Chen, J.; Kelleman, M.; O’Keeffe, M.; RoyChoudhury, A.; Jones, P.J. Short sleep duration increases energy intakes but does not change energy expenditure in normal-weight individuals. Am. J. Clin. Nutr. 2011, 94, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Nea, F.M.; Kearney, J.; Livingstone, M.B.E.; Pourshahidi, L.K.; Corish, C.A. Dietary and lifestyle habits and the associated health risks in shift workers. Nutr. Res. Rev. 2015, 28, 143–166. [Google Scholar] [CrossRef] [PubMed]
- Ursin, R.; Bjorvatn, B.; Holsten, F. Sleep duration, subjective sleep need, and sleep habits of 40-to 45-year-olds in the hordaland health study. Sleep 2005, 28, 1260. [Google Scholar] [PubMed]
- Dashti, H.S.; Scheer, F.A.; Jacques, P.F.; Lamon-Fava, S.; Ordovás, J.M. Short sleep duration and dietary intake: Epidemiologic evidence, mechanisms, and health implications. Adv. Nutr. Res. 2015, 6, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Boivin, D.B.; Tremblay, G.M.; James, F.O. Working on atypical schedules. Sleep Med. 2007, 8, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Nakagawa, H.; Miura, K.; Soyama, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nogawa, K. Effect of shift work on body mass index and metabolic parameters. Scand. J. Work Environ. Health 2007, 33, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Knutson, A.; Andersson, H.; Berglund, U. Serum lipoproteins in day and shift workers: A prospective study. Br. J. Ind. Med. 1990, 47, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Devine, C.M.; Olson, C.M. Women’s perceptions about the way social roles promote or constrain personal nutritional care. Women Health 1992, 19, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Devine, C.M.; Wolfe, W.S.; Frongillo, E.A., Jr.; Bisogni, C.A. Life-course events and experiences: Association with fruit and vegetable consumption in 3 ethnic groups. J. Am. Diet. Assoc. 1999, 99, 309–314. [Google Scholar] [CrossRef]
- Rolls, B.J.; Fedoroff, I.C.; Guthrie, J.F. Gender differences in eating behavior and body weight regulation. Health Psychol. 1991, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Heitmann, B.L. Dietary fat and obesity: Evidence from epidemiology. Eur. J. Clin. Nutr. 1995, 49, 79. [Google Scholar] [PubMed]
- Murphy, S.P.; Rose, D.; Hudes, M.; Viteri, F.E. Demographic and economic factors associated with dietary quality for adults in the 1987–88 nationwide food consumption survey. J. Am. Diet. Assoc. 1992, 92, 1352–1357. [Google Scholar] [PubMed]
- The Cancer Council Victoria. Dietary Questionnaire for Epidemiological Studies, version 2; The Cancer Council Victoria: Melbourne, Australia, 1996. [Google Scholar]
- Xinying, P.X.; Noakes, M.; Keogh, J. Can a food frequency questionnaire be used to capture dietary intake data in a 4 week clinical intervention trial? Asia Pac. J. Clin. Nutr. 2004, 13, 318–323. [Google Scholar] [PubMed]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The anti cancer council of victoria ffq: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Folkard, S.; Smith, L.; Spelten, E.; Totterdell, P. Standard shiftwork index manual. J. Appl. Psychol. 1993, 60, 159–170. [Google Scholar]
- Spelten, E.; Barton, J.; Folkard, S. Have we underestimated shiftworkers’ problems? Evidence from a ‘reminiscence’ study. Ergonomics 1993, 36, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Gibby, R.; Zickar, M.; Crossley, C.; Robie, C.; Folkard, S.; Tuker, P.; Barton, J. Measurement properties of the shiftwork survey and standard shiftwork index. J. Hum. Ergol. 2001, 30, 191–196. [Google Scholar]
- Field, A.P. Discovering Statistics Using ibm spss Statistics: And Sex and Drugs and Rock ‘n’ Roll, 4th ed.; Sage: Los Angeles, CA, USA, 2013. [Google Scholar]
- Cohen, J. Set correlation and contingency tables. Appl. Psychol. Meas. 1988, 12, 425–434. [Google Scholar] [CrossRef]
- Hosmer, D.; Lemeshow, S.; May, S. Applied Survival Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3. [Google Scholar] [CrossRef] [PubMed]
- Pasqua, I.; Moreno, C. The nutritional status and eating habits of shift workers: A chronobiological approach. Chronobiol. Int. 2004, 21, 949–960. [Google Scholar] [CrossRef] [PubMed]
- De Assis, M.A.A.; Kupek, E.; Nahas, M.V.C.; Bellisle, F. Food intake and circadian rhythms in shift workers with a high workload. Appetite 2003, 40, 175–183. [Google Scholar] [CrossRef]
- Geliebter, A.; Gluck, M.E.; Tanowitz, M.; Aronoff, N.J.; Zammit, G.K. Work-shift period and weight change. Nutrition 2000, 16, 27–29. [Google Scholar] [CrossRef]
- Wurtman, R.J.; Wurtman, J.J. Carbohydrates and depression. Sci. Am. 1989, 260, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Thayer, R. Energy, tiredness, and tension effects of a sugar snack versus moderate exercise. J. Personal. Soc. Psychol. 1987, 52, 119–125. [Google Scholar] [CrossRef]
- Stewart, A.J.; Wahlqvist, M.L. Effect of shiftwork on canteen food purchase. J. Occup. Environ. Med. 1985, 27, 552–554. [Google Scholar] [CrossRef]
- Australian Government National Health and Medical Research Council Nutrient Reference Values for Australia and New Zealand. Available online: https://www.nrv.gov.au/ (accessed on 18 November 2016).
- Australian Bureau of Statistics Australian Health Survey: Nutrition First Results-Food and Nutrients. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/4364.0.55.009main+features12011-12 (accessed on 18 November 2016).
- Harada, H.; Suwazono, Y.; Sakata, K.; Okubo, Y.; Oishi, M.; Uetani, M.; Kobayashi, E.; Nogawa, K. Three-shift system increases job-related stress in japanese workers. J. Occup. Health 2005, 47, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Puttonen, S.; Kivimäki, M.; Elovainio, M.; Pulkki-Råback, L.; Hintsanen, M.; Vahtera, J.; Telama, R.; Juonala, M.; Viikari, J.S.; Raitakari, O.T. Shift work in young adults and carotid artery intima–media thickness: The cardiovascular risk in young finns study. Atherosclerosis 2009, 205, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, L.; De Pergola, G.; Zocchetti, C.; L’Abbate, N.; Basso, A.; Pannacciulli, N.; Cignarelli, M.; Giorgino, R.; Soleo, L. Effect of shift work on body mass index: Results of a study performed in 319 glucose-tolerant men working in a southern Italian industry. Int. J. Obes. 2003, 27, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Skinner, N. Alcohol consumption patterns of shiftworkers compared with dayworkers. Chronobiol. Int. 2012, 29, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Paterson, J.; Dawson, D.; Pincombe, J.; Grech, C.; Rogers, A.E. Sleep, stress and compensatory behaviors in Australian nurses and midwives. Rev. Saude Publica 2011, 45, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Gold, D.R.; Rogacz, S.; Bock, N.; Tosteson, T.D.; Baum, T.M.; Speizer, F.E.; Czeisler, C.A. Rotating shift work, sleep, and accidents related to sleepiness in hospital nurses. Am. J. Public Health 1992, 82, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Härmä, M.; Tenkanen, L.; Sjöblom, T.; Alikoski, T.; Heinsalmi, P. Combined effects of shift work and life-style on the prevalence of insomnia, sleep deprivation and daytime sleepiness. Scand. J. Work Environ. Health 1998, 24, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Howland, J.; Mangione, T.W.; Kuhlthau, K.; Bell, N.; Heeren, T.; Lee, M.; Levine, S. Work-site variation in managerial drinking. Addiction 1996, 91, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S. Alcohol use in the service industry. Addiction 1994, 89, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.; Tsai, S.; Gibson, R. Anatomy of the healthy worker effect: A critical review. JOM-J. Occup. Med. 1983, 25, 283–289. [Google Scholar]
- Skinner, N.; Dorrian, J. A work-life perspective on sleep and fatigue—Looking beyond shift workers. Ind. Health 2015, 53, 417. [Google Scholar] [CrossRef] [PubMed]
- Goris, A.H.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Undereating and underrecording of habitual food intake in obese men: Selective underreporting of fat intake. Am. J. Clin. Nutr. 2000, 71, 1130–1134. [Google Scholar]
- Taren, D.; Tobar, M.; Hill, A.; Howell, W.; Shisslak, C.; Bell, I.; Ritenbaugh, C. The association of energy intake bias with psychological scores of women. Eur. J. Clin. Nutr. 1999, 53, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Rebro, S.M.; Patterson, R.E.; Kristal, A.R.; Cheney, C.L. The effect of keeping food records on eating patterns. J. Am. Diet. Assoc. 1998, 98, 1163–1165. [Google Scholar] [CrossRef]
- Erdman, J.W., Jr.; MacDonald, I.A.; Zeisel, S.H. Present Knowledge in Nutrition; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Thomson, T.; Subar, A. Dietary assessment methdology. In Nutrtion in the Prevention and Treatment of Disease; Coulston, A., Rock, C., Mondsen, E., Eds.; Academic Press: London, UK, 2001; pp. 3–30. [Google Scholar]

{kind=link}
| Morning n = 33 | Night n = 27 | 8-h R n = 29 | 12-h R n = 29 | F3113 | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years) | 44.8 (9.9) | 42.7 (9.9) | 41.2 (11.7) | 44.17 (7.9) | 0.58 |
| Female (%) | 21.2 | 37.0 | 65.5 | 3.6 | |
| BMI (kg/m2) | 25.8 (2.8) | 26.8 (5.1) | 27.5 (5.5) | 28.3 (4.0) | 1.68 |
| Married (%) | 81.8 | 74.1 | 85.7 | 93.1 | |
| Education | |||||
| Postgrad (%) | 12.5 | 7.4 | 32.1 | 17.2 | |
| Undergrad (%) | 21.9 | 14.8 | 32.1 | 3.4 | |
| Vocational (%) | 21.9 | 7.4 | 14.3 | 44.8 | |
| Secondary (%) | 43.8 | 70.4 | 21.4 | 34.5 | |
| Sleep/Fatigue | |||||
| Sleep duration (h) | 7.5 (1.0) | 7.0 (1.1) | 7.4 (0.9) | 6.3 (1.0) | 8.42 *,a |
| Chronic Fatigue (10–50) | 25.9 (5.9) | 28.1(8.4) | 28.0 (7.8) | 25.1 (7.7) | 1.42 |
| Work | |||||
| Work hours (h) | 40.4 (16.1) | 35.9 (9.6) | 38.9 (10.0) | 44.0 (7.2) | 2.44 |
| Shift work (years) | 18.7 (11.5) | 9.0 (5.9) | 13.5 (10.5) | 18.5 (8.8) | 6.37 *,b |
| Industry | |||||
| Printing (%) | 18.2 | 14.8 | 20.7 | 0 | |
| Postal (%) | 63.6 | 77.8 | 0 | 0 | |
| Nursing (%) | 15.2 | 7.4 | 75.9 | 0 | |
| Oil and Gas (%) | 3 | 0 | 3.4 | 100 | |
| Morning n = 33 | Night n = 27 | 8-h R n = 29 | 12-h R n = 29 | F3113 | ||
|---|---|---|---|---|---|---|
| Energy (kJ/1000) | 7954 (2979) | 8816 (3616) | 8530 (3080) | 9318 (2852) | 1.0 | |
| CHO | % | 40.7 (6.8) | 41.8 (6.1) | 41.3 (6.8) | 38.7 (6.9) | 1.1 |
| g | 196.5 (81.2) | 211.2 (86.5) | 208.5 (87.3) | 213.3 (78.8) | ||
| Protein | % | 19.0 (2.6) | 19.2 (3.7) | 20.7 (3.2) | 19.6 (3.6) | 1.3 |
| g | 89.4 (34.3) | 99.9 (43.4) | 101.9 (37.6) | 105.5 (33.0) | ||
| Fat | % | 33.0 (6.0) | 35.9 (5.0) | 34.3 (5.3) | 34.5 (4.0) | 1.4 |
| g | 71.0 (28.8) | 85.8 (38.9) | 79.9 (34.1) | 87.2 (30.5) | ||
| SFA | % | 12.9 (2.7) | 15.5 (3.1) | 13.8 (2.8) | 14.1 (2.4) | 4.2 *,a |
| g | 30.0 (13.2) | 37.3 (16.9) | 32.0 (15.1) | 33.2 (12.9) | ||
| Alcohol | % | 8.8 (9.24) | 5.5 (6.79) | 6.5 (5.52) | 10.1 (8.88) | 2.0 |
| g | 17.7 (17.28) | 14.1 (21.18) | 12.3 (10.53) | 24.8 (23.04) | ||
| Independent Variable | Parameter Estimate | SE | p | 95% LLCI | 95% ULCI | ΔR2 |
|---|---|---|---|---|---|---|
| Energy Intake (kJ) | ||||||
| Sleep duration | −185.80 | 256.26 | 0.47 | −693.93 | 322.32 | 0.01 |
| Female (ref = male) | −2164.12 | 611.96 | <0.01 | −3377.54 | −756.12 | 0.07 |
| Age (years) | −69.94 | 28.04 | 0.01 | −125.55 | −14.33 | 0.04 |
| Hours worked (h) | −60.03 | 23.78 | 0.01 | −107.19 | −12.86 | 0.05 |
| Carbohydrate Intake (%) | ||||||
| Chronic fatigue | −0.19 | 0.08 | 0.02 | −0.37 | −0.02 | 0.04 |
| Shift schedule | ||||||
| Night (ref = morning) | −1.21 | 1.89 | 0.52 | −4.97 | 2.55 | |
| 8-h R | −8.33 | 1.74 | 0.63 | −4.28 | 2.61 | |
| 12-h R | −5.26 | 1.88 | <0.01 | −9.00 | −1.15 | 0.03 |
| Sleep duration | −1.59 | 0.64 | 0.01 | −2.86 | 0.32 | 0.05 |
| Protein Intake (%) | ||||||
| Female (ref = male) | 1.33 | 1.16 | 0.04 | 0.02 | 2.63 | 0.03 |
| Fat Intake (%) | ||||||
| Female(ref = male) | 1.94 | 1.66 | 0.10 | −0.37 | 4.26 | 0.01 |
| Shift schedule | ||||||
| Night (ref = morning) | 1.48 | 1.41 | 0.29 | −1.32 | 4.29 | |
| 8-h R | −0.90 | 1.38 | 0.51 | −3.65 | 1.85 | |
| 12-h R | 1.86 | 1.39 | 0.18 | −0.91 | 4.64 | 0.03 |
| BMI (kg/m2) | 0.28 | 0.10 | 0.01 | 0.07 | 0.49 | 0.11 |
| Chronic fatigue (10–50) | 0.15 | 0.06 | 0.01 | 0.03 | 0.28 | 0.06 |
| Sleep Duration (h) | 1.04 | 0.47 | 0.03 | 0.10 | 1.99 | 0.01 |
| Saturated Fat Intake (%) | ||||||
| Age | −0.05 | 0.02 | 0.05 | −0.10 | 0.00 | <0.01 |
| Married (ref = not married) | 1.19 | 0.74 | 0.11 | −0.27 | 2.67 | <0.01 |
| Industry | ||||||
| Postal (ref = oil and gas) | −3.48 | 2.64 | 0.19 | −8.75 | 1.77 | |
| Printing | −3.10 | 2.61 | 0.23 | −8.29 | 2.09 | |
| Nursing | −1.13 | 2.50 | 0.65 | −6.11 | 3.85 | 0.01 |
| Hours worked (h) | 0.03 | 0.02 | 0.16 | −0.01 | 0.08 | <0.01 |
| Chronic Fatigue | 0.05 | 0.03 | 0.14 | −0.01 | 0.11 | 0.04 |
| BMI (kg/m2) | 0.15 | 0.05 | <0.01 | 0.03 | 0.26 | 0.10 |
| Night (ref = morning) | 2.76 | 0.76 | <0.01 | 1.12 | 4.27 | |
| 8-h R | −0.95 | 0.99 | 0.34 | −2.93 | 1.03 | |
| 12-h R | −2.28 | 2.69 | 0.39 | −7.63 | 3.06 | 0.11 |
| Sleep duration (h) | 0.54 | 0.25 | 0.04 | 0.02 | 1.05 | 0.05 |
| Alcohol (%) | ||||||
| Married (ref = not married) | 2.44 | 1.98 | 0.22 | −1.49 | 6.37 | <0.01 |
| Shift work history (years) | −0.03 | 0.07 | 0.64 | −0.18 | −0.11 | 0.02 |
| Female (ref = male) | −4.38 | 1.92 | 0.02 | −8.20 | −0.56 | 0.06 |
| Industry | ||||||
| Postal (ref = oil and gas) | −4.33 | 1.92 | 0.02 | −8.14 | 0.51 | |
| Printing | −1.45 | 2.49 | 0.56 | −6.41 | 3.50 | |
| Nursing | −2.11 | 2.37 | 0.37 | −6.83 | 2.59 | 0.02 |
| Hours worked (h) | −0.18 | 0.07 | 0.01 | 0.33 | −0.04 | 0.06 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heath, G.; Coates, A.; Sargent, C.; Dorrian, J. Sleep Duration and Chronic Fatigue Are Differently Associated with the Dietary Profile of Shift Workers. Nutrients 2016, 8, 771. https://doi.org/10.3390/nu8120771
Heath G, Coates A, Sargent C, Dorrian J. Sleep Duration and Chronic Fatigue Are Differently Associated with the Dietary Profile of Shift Workers. Nutrients. 2016; 8(12):771. https://doi.org/10.3390/nu8120771
Chicago/Turabian StyleHeath, Georgina, Alison Coates, Charli Sargent, and Jillian Dorrian. 2016. "Sleep Duration and Chronic Fatigue Are Differently Associated with the Dietary Profile of Shift Workers" Nutrients 8, no. 12: 771. https://doi.org/10.3390/nu8120771