Effects of Low versus High Glycemic Index Sugar-Sweetened Beverages on Postprandial Vasodilatation and Inactivity-Induced Impairment of Glucose Metabolism in Healthy Men

Abstract
:1. Introduction
2. Materials and Methods
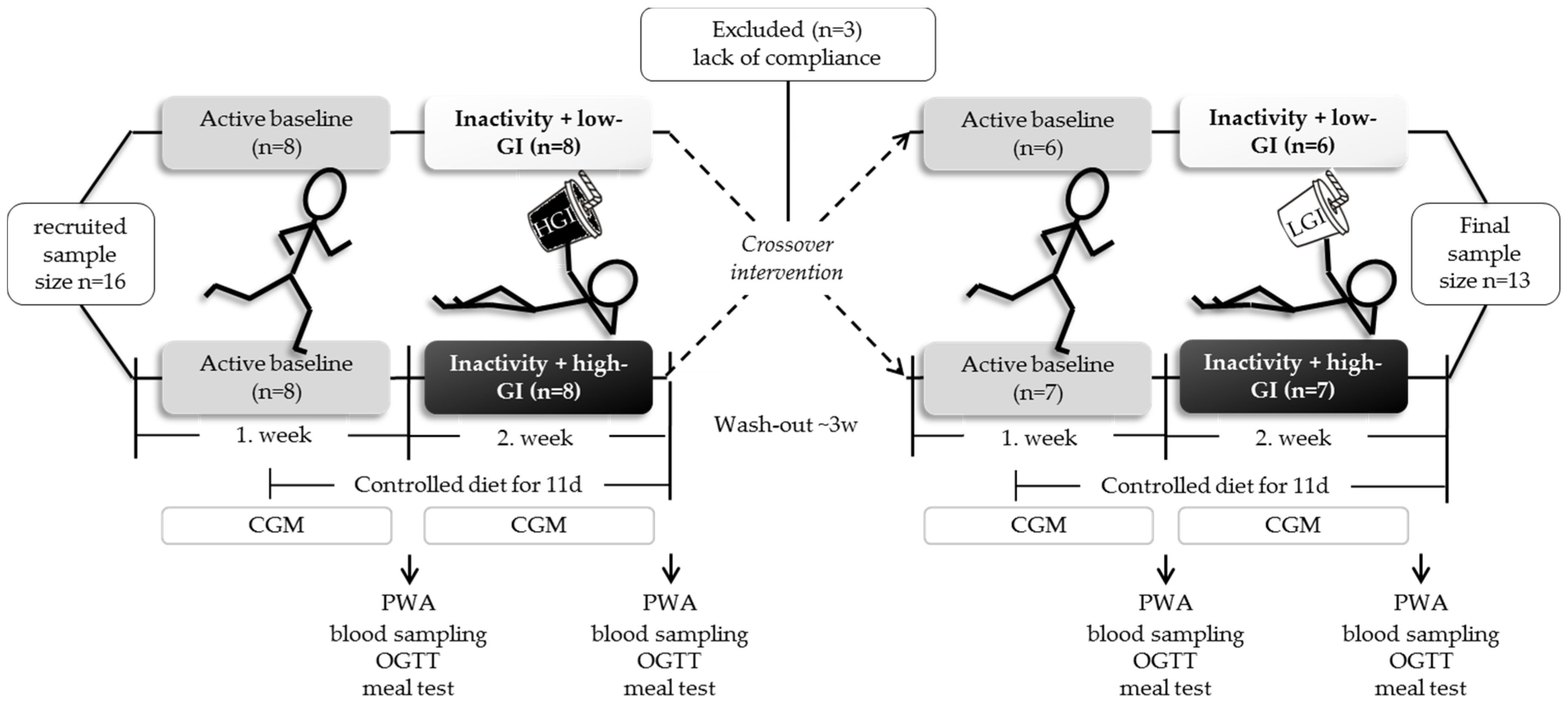
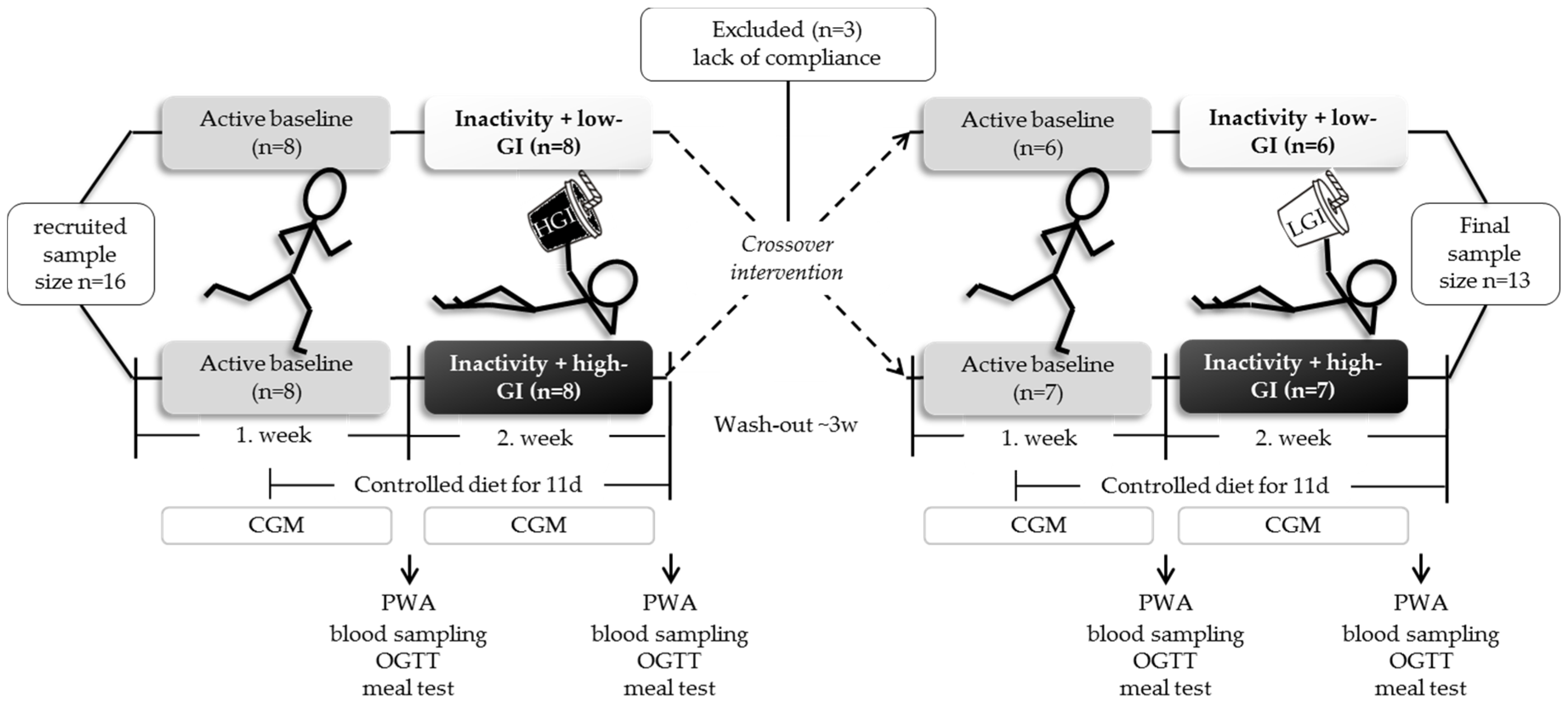
2.1. Study Protocol
2.2. Diet Intervention
2.3. Physical Activity
2.4. Body Composition
2.5. Blood Pressure, Pulse Wave Analysis and Pulse Wave Velocity (PWV)
2.6. Fasting and Postprandial Glucose Metabolism
2.7. Blood Sampling and Analytical Methods
2.8. Statistical Analysis
3. Results
3.1. Effect of Low vs. High-GI SSB Intake on Postprandial GLP-1 Secretion and Parameters of Arterial Stiffness
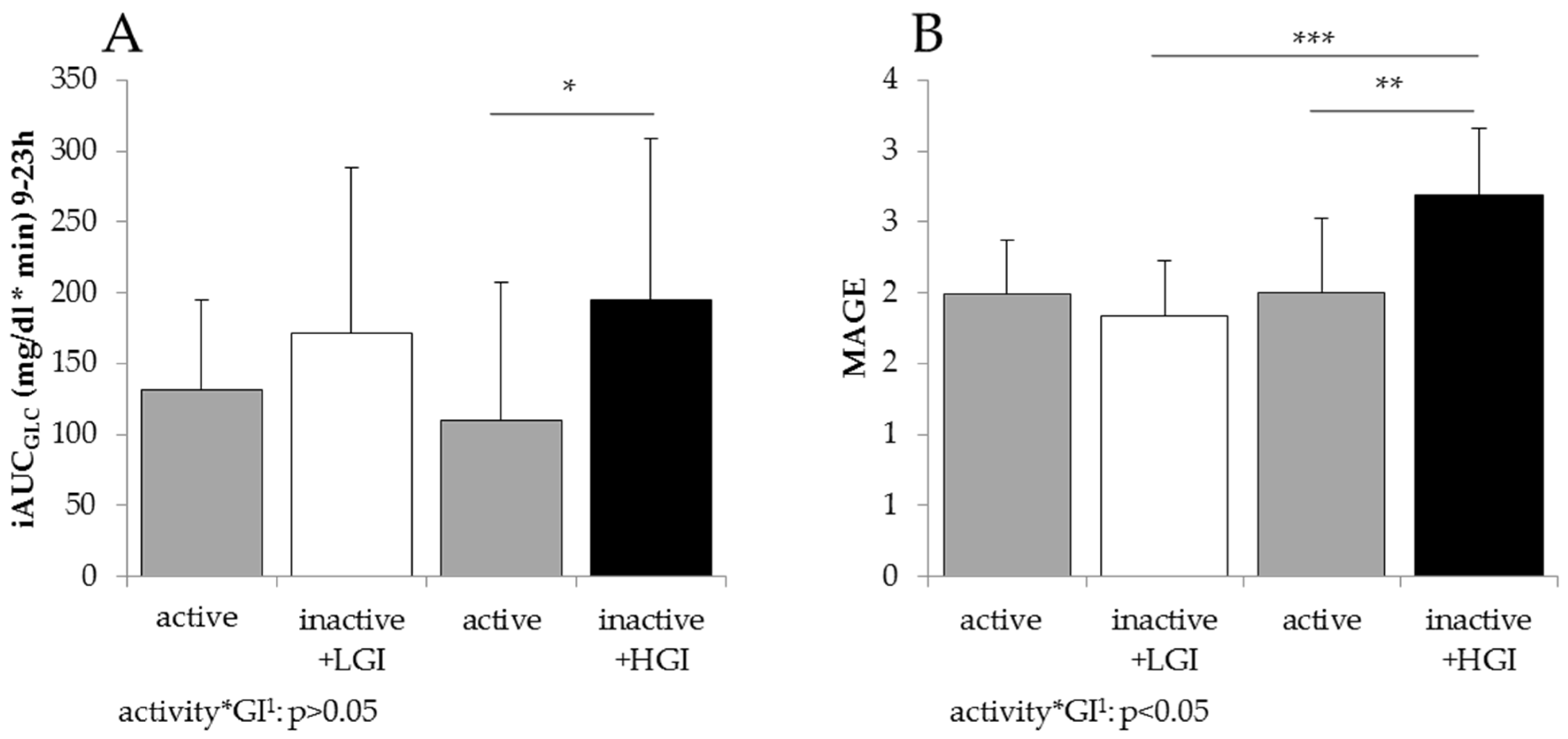
3.2. Effect of Low-GI vs. High-GI Intervention on Low Physical Activity-Induced Changes in Glucose Homeostasis
3.3. Impact of Low-GI vs. High-GI SSB Intake on Low Physical Activity-Induced Changes in BP and Parameters of Arterial Stiffness
4. Discussion
4.1. Acute Effect of Low- vs. High-GI SSB Intake on Insulin, GLP-1 and Associated Endothelial Function
4.2. Effect of GI Intervention on Low Physical Activity-Induced Changes in Glucose Metabolism and Arterial Stiffness
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Reducing Consumption of Sugar-Sweetened Beverages to Reduce the Risk of Unhealthy Weight Gain in Adults. 2014. Available online: http://www.who.int/elena/bbc/ssbs_adult_weight/en/ (accessed on 18 February 2016).
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2015, 4, 174–186. [Google Scholar] [CrossRef]
- Malik, V.S.; Hu, F.B. Sweeteners and risk of obesity and type 2 diabetes: The role of sugar-sweetened beverages. Curr. Diabetes Rep. 2012, 12, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.A.; Howatson, A.J.; Jones, R.M.; Mann, J. Dietary sugars and cardiometabolic risk: Systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am. J. Clin. Nutr. 2014, 100, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Stamler, J.; van Horn, L.; Robertson, C.E.; Chan, Q.; Dyer, A.R.; Huang, C.C.; Rodriguez, B.L.; Zhao, L.; Daviglus, M.L.; et al. Sugar-sweetened beverage, sugar intake of individuals, and their blood pressure: International study of macro/micronutrients and blood pressure. Hypertension 2011, 57, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.A.; Sharma, A.; Cunningham, S.A.; Vos, M.B. Consumption of added sugars and indicators of cardiovascular disease risk among US adolescents. Circulation 2011, 123, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Duffey, K.J.; Huybrechts, I.; Mouratidou, T.; Libuda, L.; Kersting, M.; De Vriendt, T.; Gottrand, F.; Widhalm, K.; Dallongeville, J.; Hallström, L.; et al. Beverage consumption among European adolescents in the HELENA study. Eur. J. Clin. Nutr. 2012, 66, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.A.; Swain, J.; Goldfine, A.B.; Rifai, N.; Ludwig, D.S. Effects of a low-glycemic load diet on resting energy expenditure and heart disease risk factors during weight loss. JAMA 2004, 292, 2482–2490. [Google Scholar] [CrossRef] [PubMed]
- Philippou, E.; Bovill-Taylor, C.; Rajkumar, C.; Vampa, M.L.; Ntatsaki, E.; Brynes, A.E.; Hickson, M.; Frost, G.S. Preliminary report: The effect of a 6-month dietary glycemic index manipulation in addition to healthy eating advice and weight loss on arterial compliance and 24-hour ambulatory blood pressure in men: A pilot study. Metabolism 2009, 58, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.; Popkin, B.; Bray, G.; Després, J.-P.; Hu, F. Sugar Sweetened Beverages, Obesity, Type 2 Diabetes and Cardiovascular Disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Rask-Madsen, C.; King, G.L. Mechanisms of Disease: Endothelial dysfunction in insulin resistance and diabetes. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Nystrom, F.H.; Ravichandran, L.V.; Cong, L.N.; Kirby, M.; Mostowski, H.; Quon, M.J. Roles for insulin receptor, PI3-kinase, and Akt in insulin-signaling pathways related to production of nitric oxide in human vascular endothelial cells. Circulation 2000, 101, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.A.; Montagnani, M.; Kwang, K.K.; Quon, M.J. Reciprocal relationships between insulin resistance and endothelial dysfunction: Molecular and pathophysiological mechanisms. Circulation 2006, 113, 1888–1904. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.D.; Bierbrier, G.S. Insulin-mediated vasodilation: Impairment with increased blood pressure and body mass. Lancet 1993, 342, 707–709. [Google Scholar] [CrossRef]
- Kahlhöfer, J.; Karschin, J.; Silberhorn-Bühler, H.; Breusing, N.; Bosy-Westphal, A. Effect of low-glycemic-sugar-sweetened beverages on glucose metabolism and macronutrient oxidation in healthy men. Int. J. Obes. 2016, 40, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Lina, B.A.R.; Jonker, D.; Kozianowski, G. Isomaltulose (Palatinose): A review of biological and toxicological studies. Food Chem. Toxicol. 2002, 40, 1375–1381. [Google Scholar] [CrossRef]
- Atkinson, F.; Foster-Powell, K.; Brand-Miller, J.C. Glycemic Load Values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Van Nieuwenhoven, M.A.; Brouns, F.; Kovacs, E.M.R. The effect of two sports drinks and water on GI complaints and performance during an 18-km run. Int. J. Sports Med. 2005, 26, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Maeda, A.; Miyagawa, J.I.; Miuchi, M.; Nagai, E.; Konishi, K.; Matsuo, T.; Tokuda, M.; Kusunoki, Y.; Ochi, H.; Murai, K.; et al. Effects of the naturally-occurring disaccharides, palatinose and sucrose, on incretin secretion in healthy non-obese subjects. J. Diabetes Investig. 2013, 4, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Charkoudian, N.; Schrage, W.; Rizza R, A.; Basu, R.; Joyner, M.J. Beneficial effects of GLP-1 on endothelial function in humans: Dampening by glyburide but not by glimepiride. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E1289–E1295. [Google Scholar] [CrossRef] [PubMed]
- Nyström, T.; Gutniak, M.K.; Zhang, Q.; Zhang, F.; Holst, J.J.; Ahrén, B.; Sjöholm, Å. Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E1209–E1215. [Google Scholar] [CrossRef] [PubMed]
- Krogh-Madsen, R.; Thyfault, J.P.; Broholm, C.; Mortensen, O.H.; Olsen, R.H.; Mounier, R.; Plomgaard, P.; van Hall, G.; Booth, F.W.; Pedersen, B.K. A 2-week reduction of ambulatory activity attenuates peripheral insulin sensitivity. J. Appl. Physiol. 2010, 108, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Marcos, M.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Agudo-Conde, C.; Lasaosa-Medina, L.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; García-Ortiz, L.; EVIDENT Group. Relationship between objectively measured physical activity and vascular structure and function in adults. Atherosclerosis 2014, 234, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Nosova, E.V.; Yen, P.; Chong, K.C.; Alley, H.F.; Stock, E.O.; Quinn, A.; Hellmann, J.; Conte, M.S.; Owens, C.D.; Spite, M.; et al. Short-term physical inactivity impairs vascular function. J. Surg. Res. 2014, 190, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.R.; Granados, K.; Zderic, T.W.; Hamilton, M.T.; Braun, B. Effects of 1 day of inactivity on insulin action in healthy men and women: Interaction with energy intake. Metabolism 2011, 60, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Brown, W.J.; Clemes, S.A.; De Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.M.; Mutrie, N.; et al. How many steps/day are enough? For adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mark, T. Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar]
- Hickson, S.S.; Butlin, M.; Broad, J.; Avolio, A.P.; Wilkinson, I.B.; McEniery, C.M. Validity and repeatability of the Vicorder apparatus: A comparison with the SphygmoCor device. Hypertens. Res. 2009, 32, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- McGreevy, C.; Barry, M.; Bennett, K.; Williams, D. Repeatability of the measurement of aortic pulse wave velocity (aPWV) in the clinical assessment of arterial stiffness in community-dwelling older patients using the Vicorder® device. Scand. J. Clin. Lab. Investig. 2013, 73, 269–273. [Google Scholar] [CrossRef] [PubMed]
- McGreevy, C.; Barry, M.; Davenport, C.; Byrne, B.; Donaghy, C.; Collier, G.; Tormey, W.; Smith, D.; Bennett, K.; Williams, D. The effect of vitamin D supplementation on arterial stiffness in an elderly community-based population. J. Am. Soc. Hypertens. 2014, 9, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Service, F.J.; Molnar, G.D.; Rosevear, J.W.; Ackerman, E.; Gatewood, L.C.; Taylor, W.F. Mean amplitude of glycemic excursions, a measure of diabetic instability. Diabetes 1970, 19, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Standl, E.; Schnell, O.; Ceriello, A. Postprandial Hyperglycemia and Glycemic Variability. Diabetes Care 2011, 34, S120–S127. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.N.; Altman, D.G.; Campbell, M.J.; Royston, P. Analysis of serial measurements in medical research. BMJ 1990, 300, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, I.; Daniel, J.W. The bio-availability of isomaltulose in man and rat. Nutr. Rep. Int. 1983, 28, 1083–1090. [Google Scholar]
- Kong, M.F.; Chapman, I.; Goble, E.; Wishart, J.; Wittert, G.; Morris, H.; Horowitz, M. Effects of oral fructose and glucose on plasma GLP-1 and appetite in normal subjects. Peptides 1999, 20, 545–551. [Google Scholar] [CrossRef]
- Baggio, L.L.; Drucker, D.J. Biology of Incretins: GLP-1 and GIP. Gastroenterology 2007, 132, 2131–2157. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, U.; Randin, D.; Vollenweider, P.; Vollenweider, L.; Nicod, P. Nitric oxide release accounts for insulin’s vascular effects in humans. J. Clin. Investig. 1994, 94, 2511–2515. [Google Scholar] [CrossRef] [PubMed]
- Vilsbøll, T.; Krarup, T.; Deacon, C.F.; Madsbad, S.; Holst, J.J. Reduced postprandial concentrations of intact biologically active glucagon-like peptide 1 in type 2 diabetic patients. Diabetes 2001, 50, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Ang, M.; Linn, T. Comparison of the effects of slowly and rapidly absorbed carbohydrates on postprandial glucose metabolism in type 2 diabetes mellitus patients: A randomized trial 1–3. Am. J. Clin. Nutr. 2014, 100, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Lind, L. Endothelium-dependent Vasodilation in Hypertension: A Review. Blood Press. 2000, 9, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Ussher, J.R.; Drucker, D.J. Cardiovascular biology of the incretin system. Endocr. Rev. 2012, 33, 187–215. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Kohl, H.W.; Paffenbarger, R.S.; Clark, D.G.; Cooper, K.H.; Gibbons, L.W. Physical fitness and all-cause mortality: A prospective study of healthy men and women. JAMA 1989, 262, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- Restaino, R.M.; Holwerda, S.W.; Credeur, D.P.; Fadel, P.J.; Padilla, J. Impact of prolonged sitting on lower and upper limb micro- and macrovascular dilator function. Exp. Physiol. 2015, 100, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Thosar, S.S.; Bielko, S.L.; Mather, K.J.; Johnston, J.D.; Wallace, J.P. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med. Sci. Sports Exerc. 2015, 47, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Hamburg, N.M.; McMackin, C.J.; Huang, A.L.; Shenouda, S.M.; Widlansky, M.E.; Schulz, E.; Gokce, N.; Ruderman, N.B.; Keaney, J.F.; Vita, J.A. Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2650–2656. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, P.J.; Scheen, A.J. The postprandial state and risk of cardiovascular disease. Diabet. Med. 1998, 15, S63–S68. [Google Scholar] [CrossRef]
- Henry, R.M.A.; Kostense, P.J.; Spijkerman, A.M.W.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Kamp, O.; Westerhof, N.; Bouter, L.M.; Stehouwer, C.D. Arterial stiffness increases with deteriorating glucose tolerance status: The Hoorn study. Circulation 2003, 107, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, H.; Saitoh, S.; Takagi, S.; Ohata, J.; Isobe, T.; Kikuchi, Y.; Takeuchi, H.; Shimamoto, K. Pulse Wave Velocity as an Indicator of Atherosclerosis in Impaired Fasting Glucose. Diabetes Care 2003, 26, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Urbina, E.M.; Gao, Z.; Khoury, P.R.; Martin, L.J.; Dolan, L.M. Insulin resistance and arterial stiffness in healthy adolescents and young adults. Diabetologia 2012, 55, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Cavarape, A.; Martinelli, L.; Da Ros, R.; Marra, G.; Quagliaro, L.; Piconi, L.; Assaloni, R.; Motz, E. The post-prandial state in Type 2 diabetes and endothelial dysfunction: Effects of insulin aspart. Diabet. Med. 2004, 21, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Mas, E.; Ginet, C.; Michel, F.; Villon, L.; Cristol, J.-P.; Colette, C. Activation of Oxidative Stress by Acute Glucose Fluctuations Compared With Sustained Chronic Hyperglycemia in Patients With Type 2 Diabetes. JAMA 2006, 295, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, C.; Schwinger, R.H.G.; Brixius, K. Physical activity and endothelial dysfunction in type 2 diabetic patients: The role of nitric oxide and oxidative stress. Wien Med. Wochenschr. 2011, 161, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Kilic-Erkek, O.; Kilic-Toprak, E.; Caliskan, S.; Ekbic, Y.; Akbudak, I.H.; Kucukatay, V.; Bor-Kucukatay, M. Detraining reverses exercise-induced improvement in blood pressure associated with decrements of oxidative stress in various tissues in spontaneously hypertensive rats. Mol. Cell. Biochem. 2016, 412, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Colagiuri, S. Health potential of a low glycaemic index diet. BMJ 2015, 350, h2267. [Google Scholar] [CrossRef] [PubMed]
- Hosseininasab, M.; Norouzy, A.; Nematy, M.; Bonakdaran, S. Low-Glycemic-Index Foods Can Decrease Systolic and Diastolic Blood Pressure in the Short Term. Int. J. Hypertens. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
 ) vs. high glycemic index (
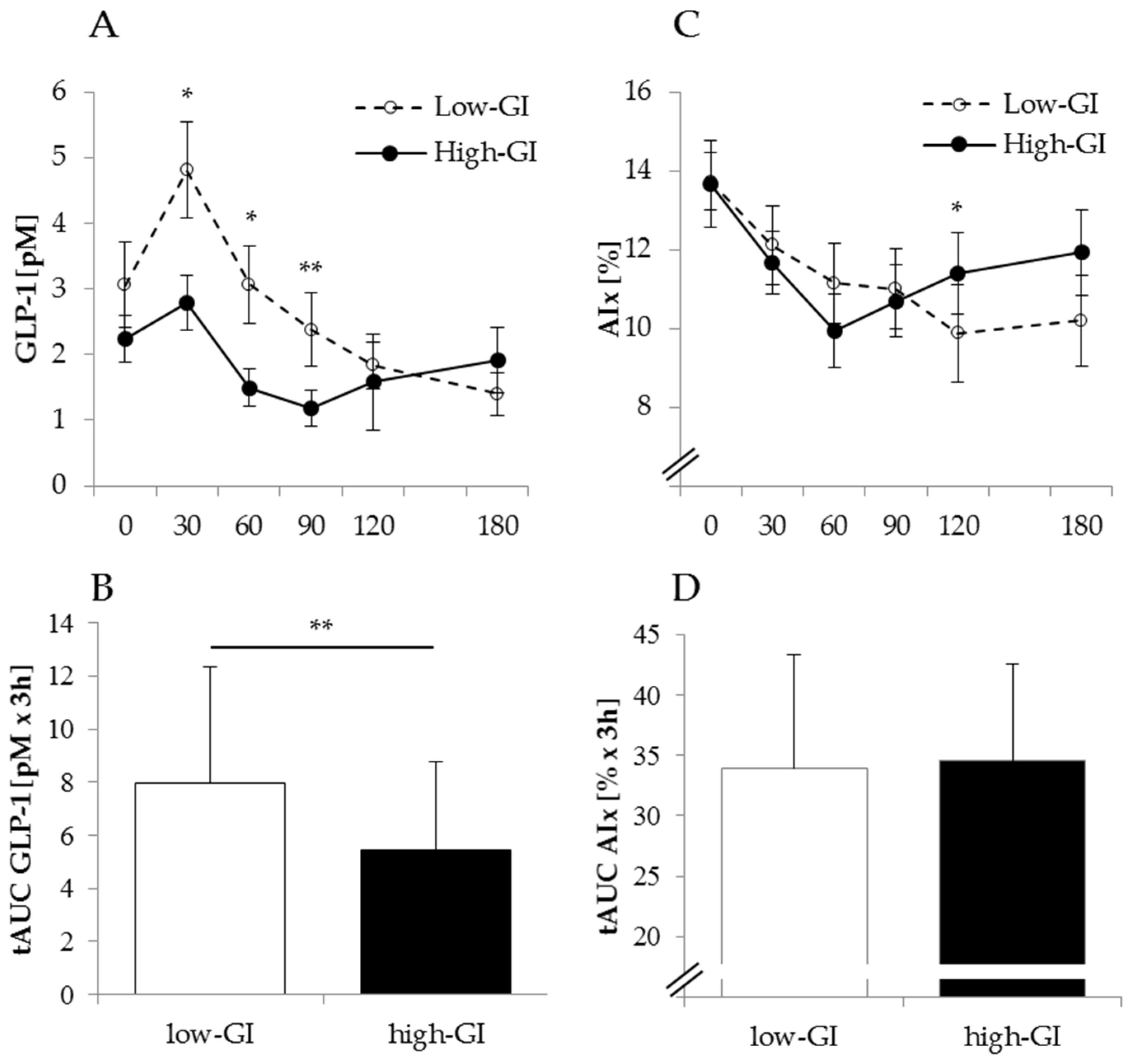
) vs. high glycemic index (  ) SSB at the end of one week of low physical activity. AIx, augmentation index; GLP1, glucagon-like peptide-1; SSB: sugar-sweetened beverages; tAUC, total area under the curve; upper panel: mean ± SEM, lower panel: mean ± SD; differences between tAUC for low-GI and high-GI SSB were tested using paired t-test, * p < 0.05; ** p < 0.01.
) vs. high glycemic index ( ) SSB at the end of one week of low physical activity. AIx, augmentation index; GLP1, glucagon-like peptide-1; SSB: sugar-sweetened beverages; tAUC, total area under the curve; upper panel: mean ± SEM, lower panel: mean ± SD; differences between tAUC for low-GI and high-GI SSB were tested using paired t-test, * p < 0.05; ** p < 0.01.
) SSB at the end of one week of low physical activity. AIx, augmentation index; GLP1, glucagon-like peptide-1; SSB: sugar-sweetened beverages; tAUC, total area under the curve; upper panel: mean ± SEM, lower panel: mean ± SD; differences between tAUC for low-GI and high-GI SSB were tested using paired t-test, * p < 0.05; ** p < 0.01.
) vs. high glycemic index ( ) SSB at the end of one week of low physical activity. AIx, augmentation index; GLP1, glucagon-like peptide-1; SSB: sugar-sweetened beverages; tAUC, total area under the curve; upper panel: mean ± SEM, lower panel: mean ± SD; differences between tAUC for low-GI and high-GI SSB were tested using paired t-test, * p < 0.05; ** p < 0.01.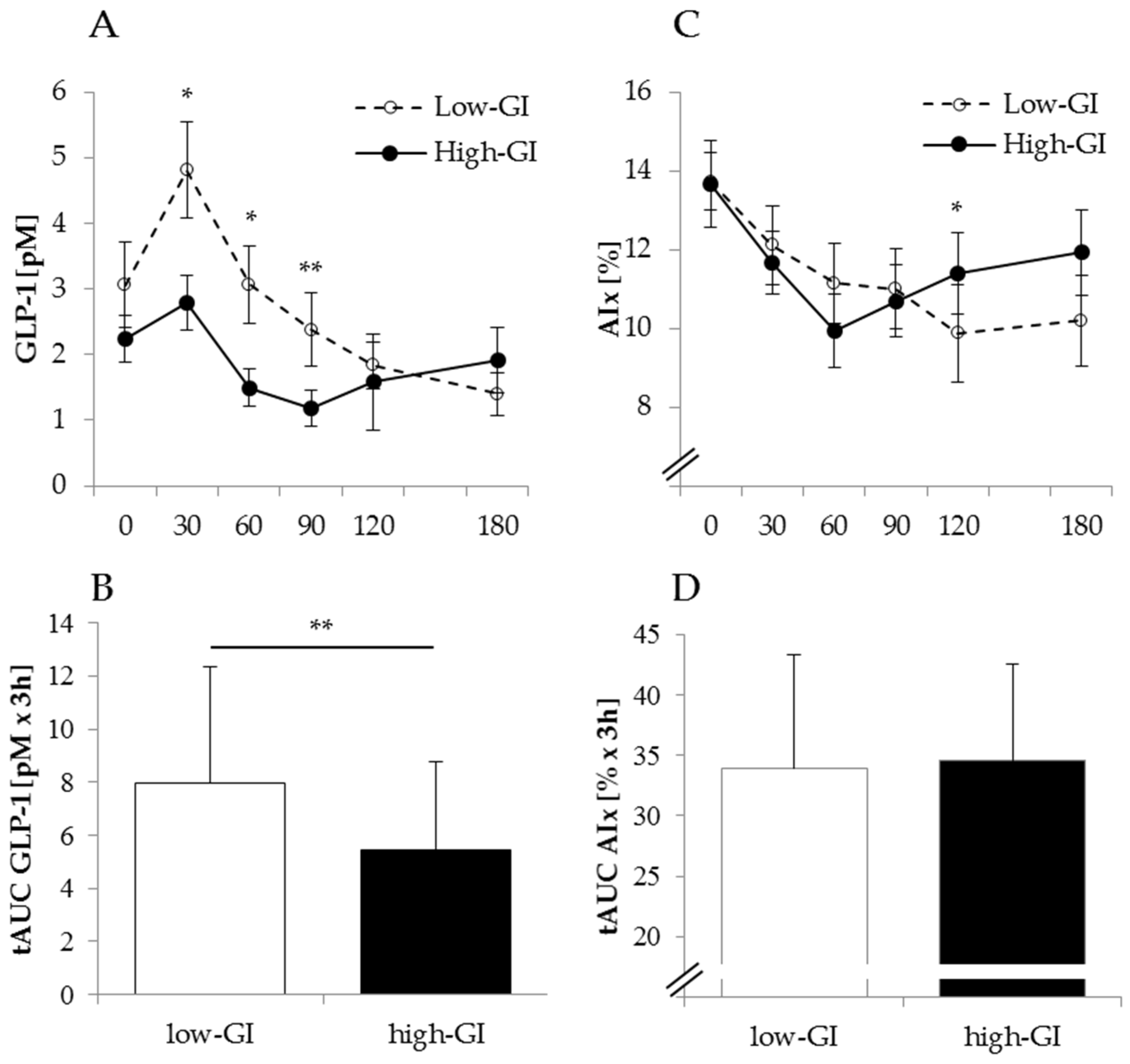


{kind=link}
{kind=link}
{kind=link}
| Activity 1 | Low Physical Activity + Low-GI | Activity 2 | Low Physical Activity + High-GI | ∆ Low Physical Activity + Low-GI—Activity 1 1 | ∆ Low Physical Activity + High-GI—Activity 2 1 | Difference Between Changes Upon Low Physical Activity 2 | |
|---|---|---|---|---|---|---|---|
| Age | 24 ± 7 | ||||||
| BMI (kg/m2) | 23.4 ± 2.3 | ||||||
| Weight | 78.8 ± 9.8 | 78.7 ± 9.8 | 78.7 ± 9.2 | 78.2 ± 9.3 | −0.1 ± 0.6 | −0.5 ± 0.7 * | n.s. |
| FM (%) | 13.8 ± 6.4 | 14.3 ± 6.2 | 13.4 ± 5.7 | 14.1 ± 5.6 | 0.5 ± 0.8 * | 0.7 ± 0.7 ** | n.s. |
| Steps per day | 11,051 ± 3064 | 2263 ± 861 | 11,699 ± 3748 | 2463 ± 1008 | −8788 ± 3131 *** | −9236 ± 3940 *** | n.s. |
| Lipid profile | |||||||
| TG (mg/dL) | 63.2 ± 22.1 | 94.7 ± 28.1 | 65.3 ± 17.2 | 115.3 ± 52.6 | 31.5 ± 36.4 * | 50.0 ± 53.1 ** | n.s. |
| Cholesterin (mg/dL) | 152 ± 24 | 157 ± 23 | 156 ± 24 | 156 ± 28 | 5.5 ± 16.9 | −0.2 ± 13.1 | n.s. |
| HDL (mg/dL) | 45.8 ± 6.2 | 41.5 ± 7.0 | 47.4 ± 7.0 | 42.2 ± 7.4 | −4.2 ± 5.7 * | −5.2 ± 4.3 ** | n.s. |
| LDL (mg/dL) | 93.9 ± 17.4 | 100.6 ± 15.5 | 97.6 ± 16.7 | 99.4 ± 21.8 | 6.7 ± 12.4 | 1.8 ± 10.4 | n.s. |
| Cholesterin/HDL | 3.4 ± 0.6 | 3.8 ± 0.7 | 3.3 ± 0.6 | 3.8 ± 0.8 | 0.5 ± 0.4 ** | 0.4 ± 0.5 ** | n.s. |
| Activity 1 | Low Physical Activity + Low-GI | Activity 2 | Low Physical Activity + High-GI | ∆ Low Physical Activity + Low-GI—Activity 1 1 | ∆ Low Physical Activity + High-GI—Activity 2 1 | Difference between Changes upon Low Physical Activity 2 | |
|---|---|---|---|---|---|---|---|
| Fasting insulin (mU/mL) | 4.1 ± 2.2 | 6.0 ± 2.6 | 3.8 ± 1.8 | 7.7 ± 4.9 | 1.9 ± 2.4 * | 3.9 ± 3.6 ** | <0.05 |
| HOMA-IR | 0.8 ± 0.4 | 1.2 ± 0.7 | 0.7 ± 0.5 | 1.6 ± 1.2 | 0.4 ±0.5 ** | 0.8 ± 0.9 * | <0.05 |
| Matsuda-ISI | 14.5 ± 5.9 | 9.4 ± 3.4 | 17.4 ± 8.0 | 7.8 ± 3.6 | −5.1 ± 5.5 * | −9.6 ± 5.1 ** | <0.01 |
| 24-h C-peptide excretion (µg/day) | 40.6 ± 20.7 | 45.0 ± 15.1 | 41.7 ± 18.3 | 64.8 ± 24.3 | 4.4 ± 15.1 | 23.1 ± 22.5 ** | <0.05 |
| Activity 1 | Low Physical Activity + Low-GI | Activity 2 | Low Physical Activity + High-GI | ∆ Low Physical Activity + Low-GI—Activity 1 1 | ∆ Low Physical Activity + High-GI—Activity 2 1 | Difference between Changes upon Low Physical Activity 2 | |
|---|---|---|---|---|---|---|---|
| sBP (mmHg) | 126 ± 8 | 124 ± 6 | 124 ± 8 | 125 ± 6 | −1.8 ± 6.9 | 0.8 ± 5.5 | n.s. |
| dBP (mmHg) | 66 ± 5 | 65 ± 4 | 65 ± 5 | 64 ± 6 | −1.0 ± 3.8 | −0.4 ± 6.3 | n.s. |
| cBP (mmHg) | 119 ± 8 | 117 ± 6 | 116 ± 7 | 117 ± 6 | −2.3 ± 5.9 | 0.6 ± 4.8 | n.s. |
| AIx (%) | 14 ± 3 | 14 ± 3 | 13 ± 4 | 14 ± 4 | 0.0 ± 2.9 | 0.1 ± 3.0 | n.s. |
| PWV (m/s) | 6.5 ± 0.6 | 6.5 ± 0.4 | 6.4 ± 0.6 | 6.6 ± 0.4 | 0.0 ± 0.3 | 0.2 ± 0.4 | n.s. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keller, J.; Kahlhöfer, J.; Peter, A.; Bosy-Westphal, A. Effects of Low versus High Glycemic Index Sugar-Sweetened Beverages on Postprandial Vasodilatation and Inactivity-Induced Impairment of Glucose Metabolism in Healthy Men. Nutrients 2016, 8, 802. https://doi.org/10.3390/nu8120802
Keller J, Kahlhöfer J, Peter A, Bosy-Westphal A. Effects of Low versus High Glycemic Index Sugar-Sweetened Beverages on Postprandial Vasodilatation and Inactivity-Induced Impairment of Glucose Metabolism in Healthy Men. Nutrients. 2016; 8(12):802. https://doi.org/10.3390/nu8120802
Chicago/Turabian StyleKeller, Judith, Julia Kahlhöfer, Andreas Peter, and Anja Bosy-Westphal. 2016. "Effects of Low versus High Glycemic Index Sugar-Sweetened Beverages on Postprandial Vasodilatation and Inactivity-Induced Impairment of Glucose Metabolism in Healthy Men" Nutrients 8, no. 12: 802. https://doi.org/10.3390/nu8120802