The Impact of Health Literacy Status on the Comparative Validity and Sensitivity of an Interactive Multimedia Beverage Intake Questionnaire


Abstract
:1. Introduction
2. Materials and Methods
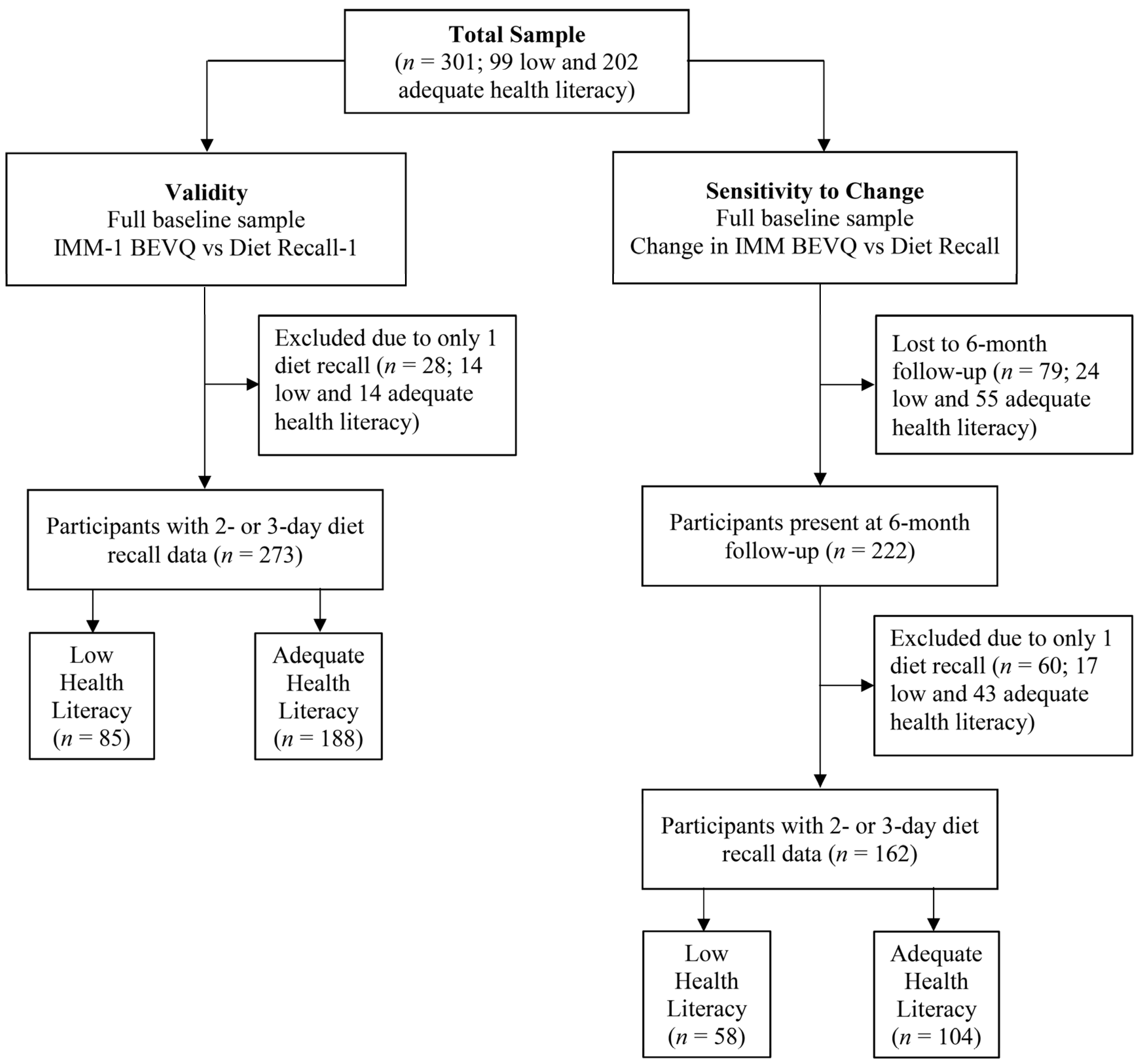
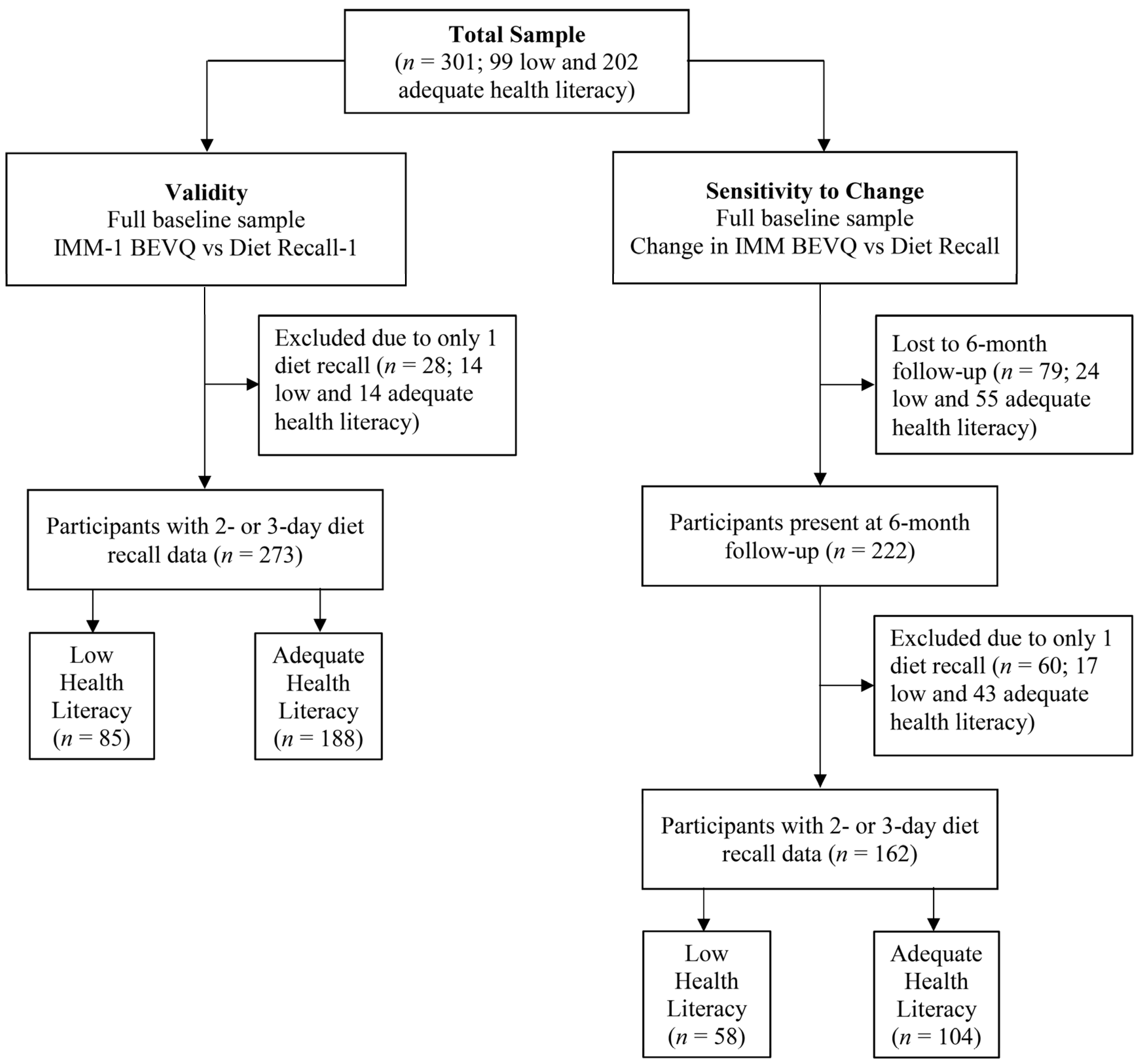
2.1. Recruitment and Trial Details
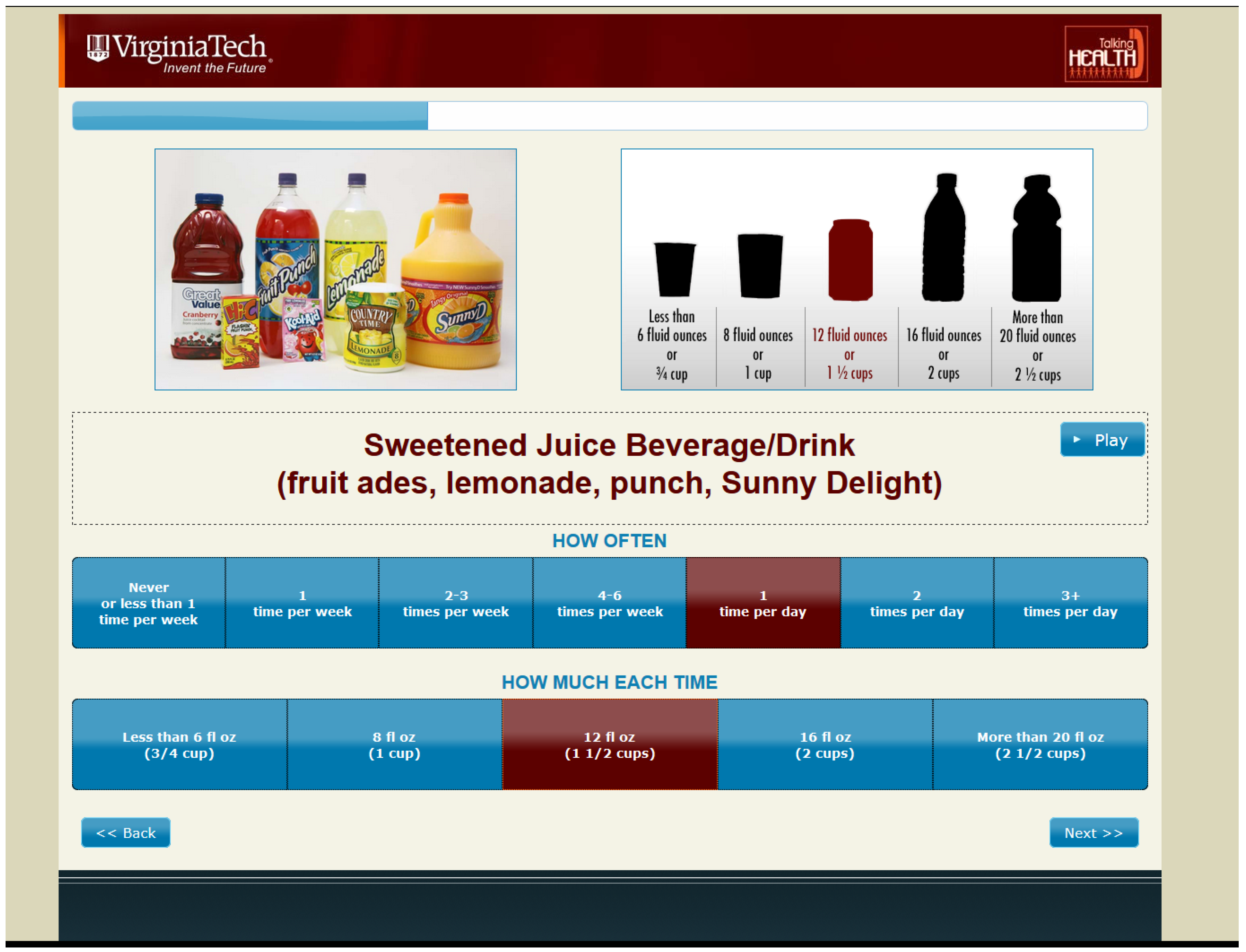
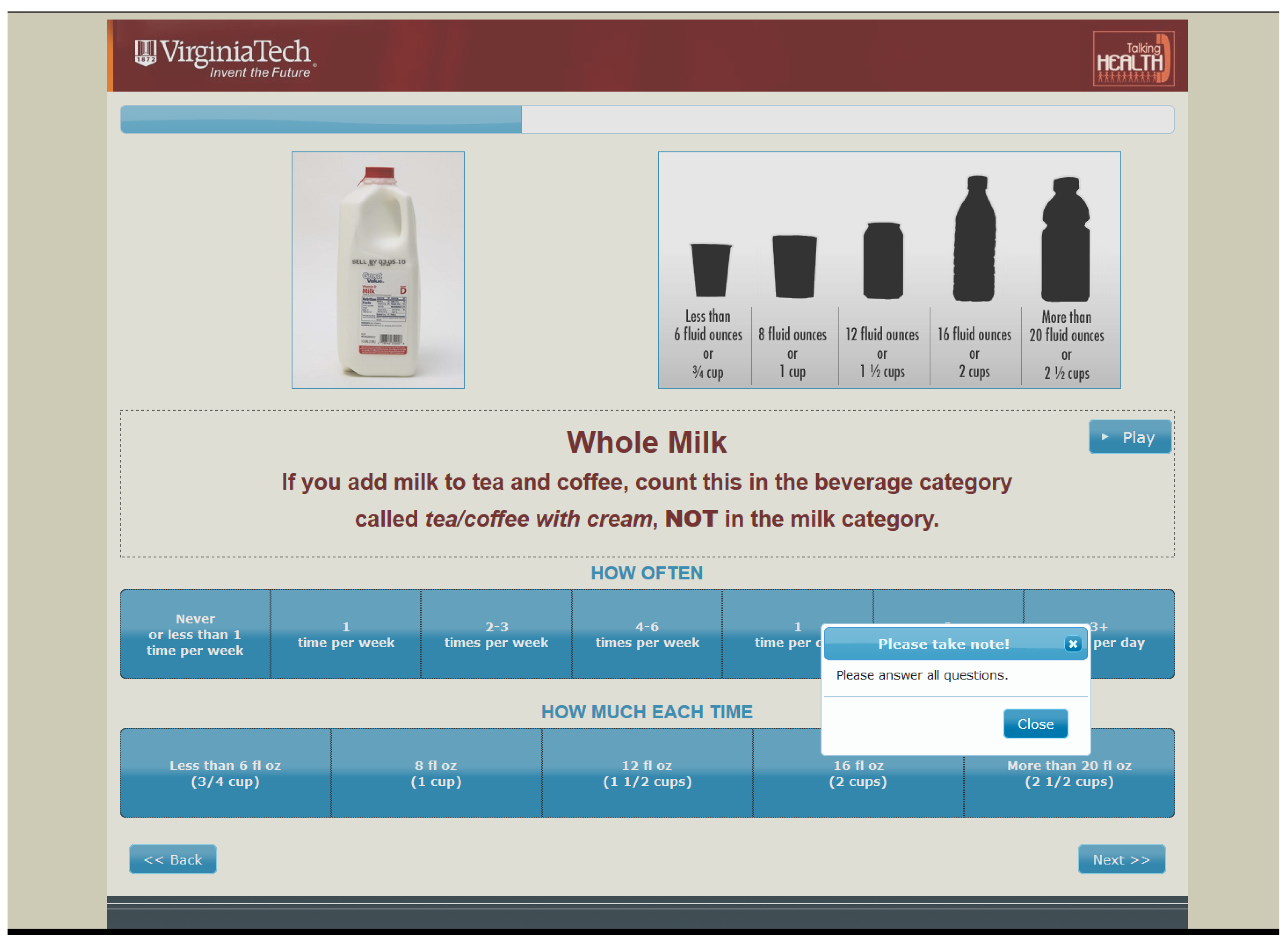
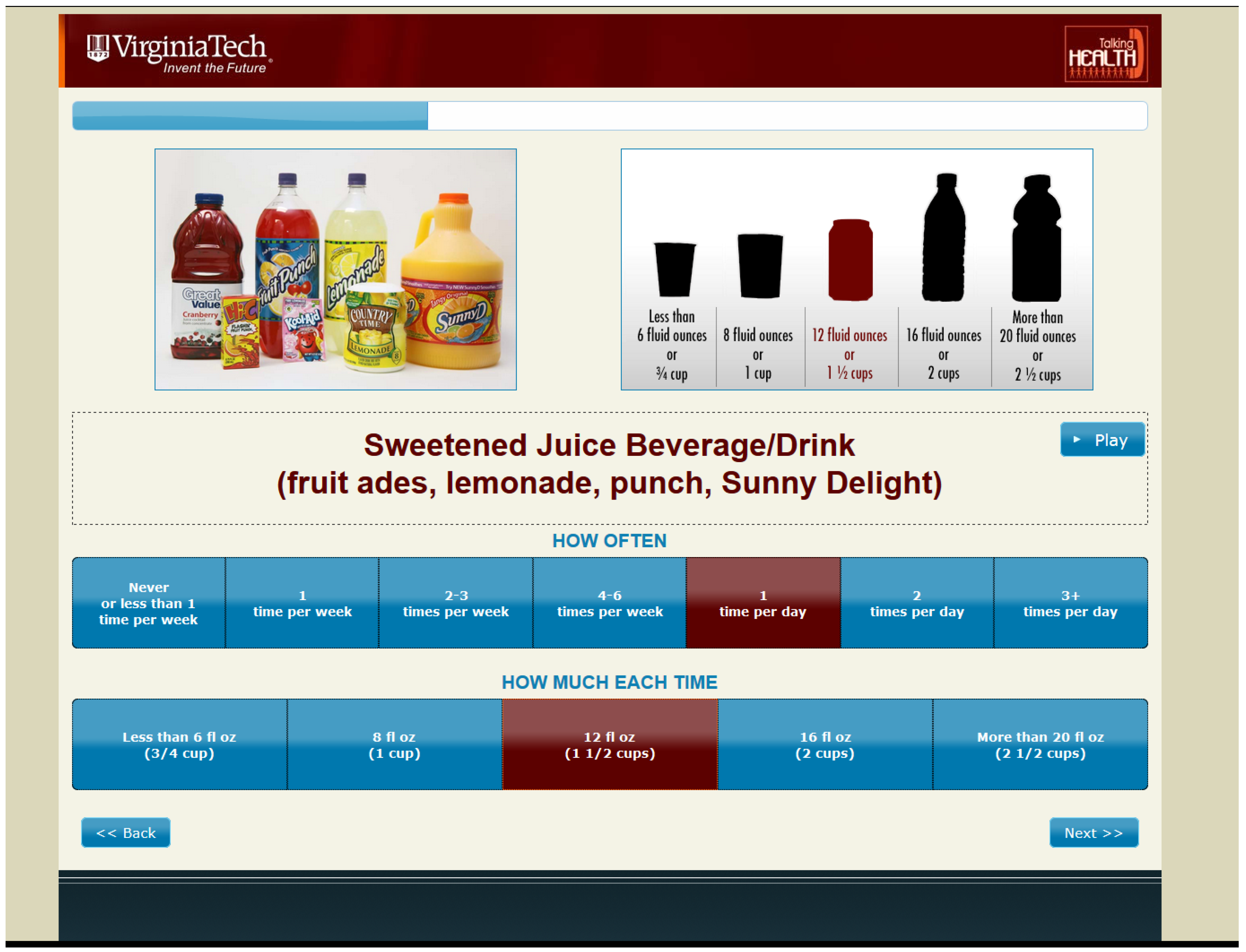
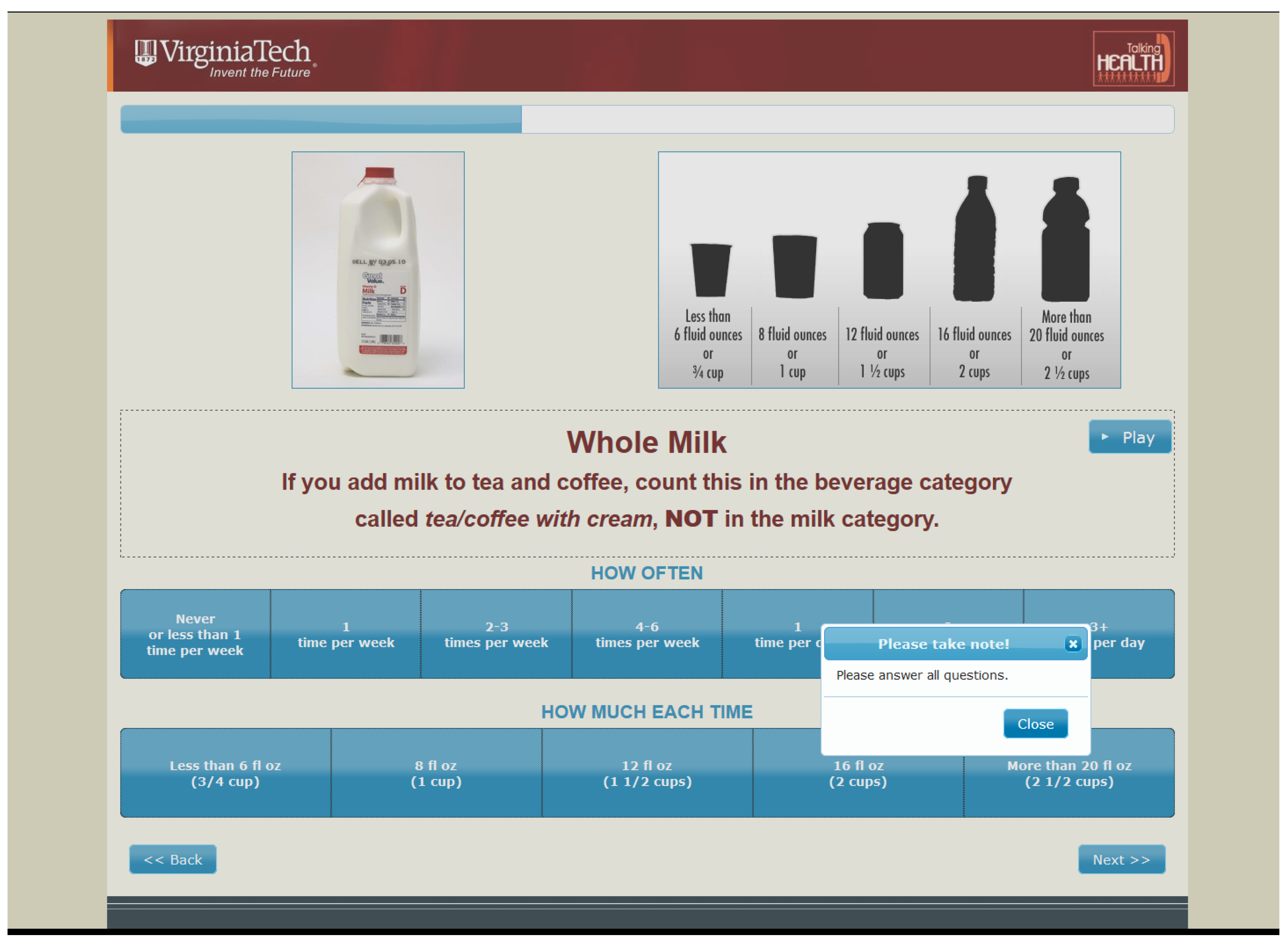
2.2. IMM-BEVQ
2.3. Dietary Recalls
2.4. Assessment of Health Literacy Status
2.5. Demographics and Anthropometrics
2.6. Ethics
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics
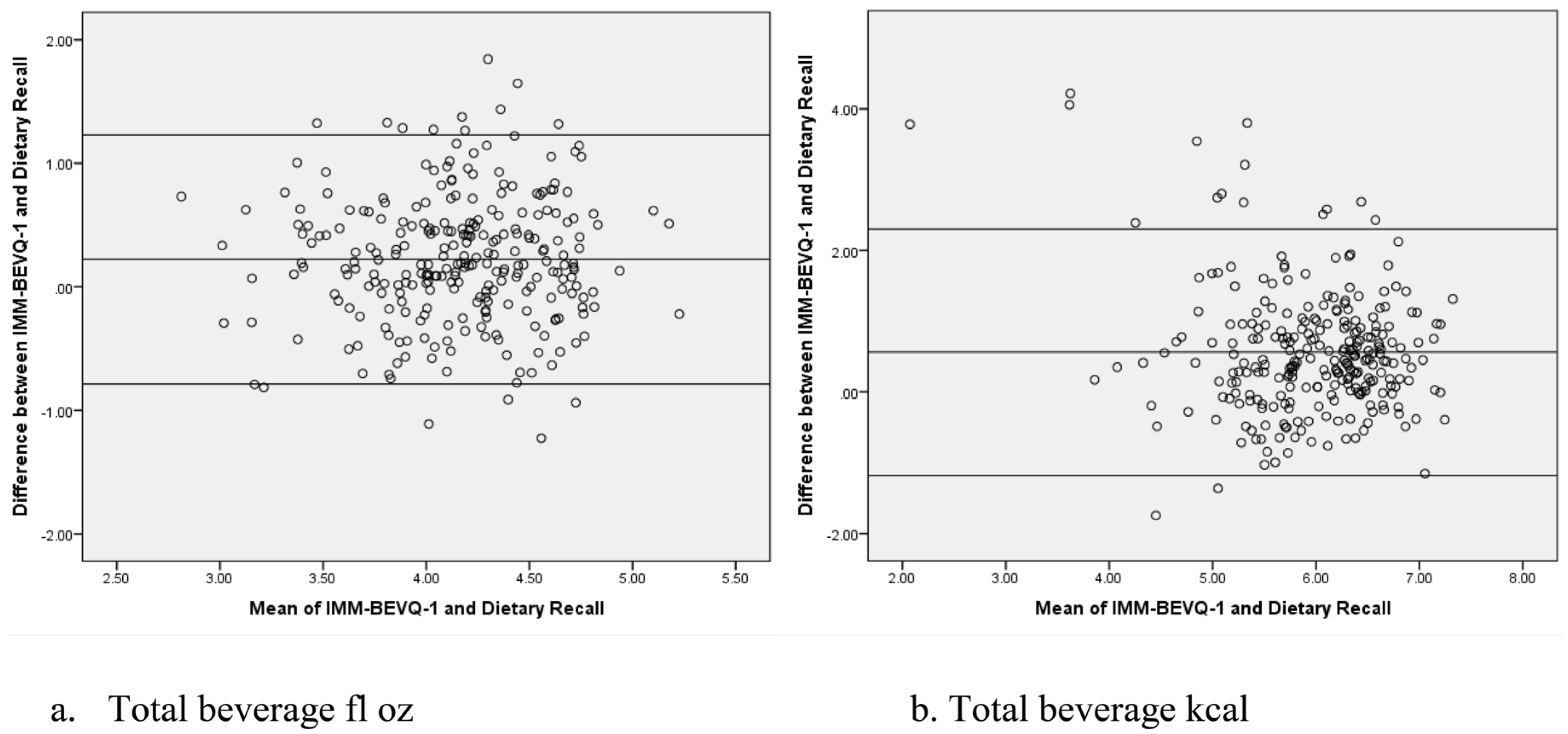
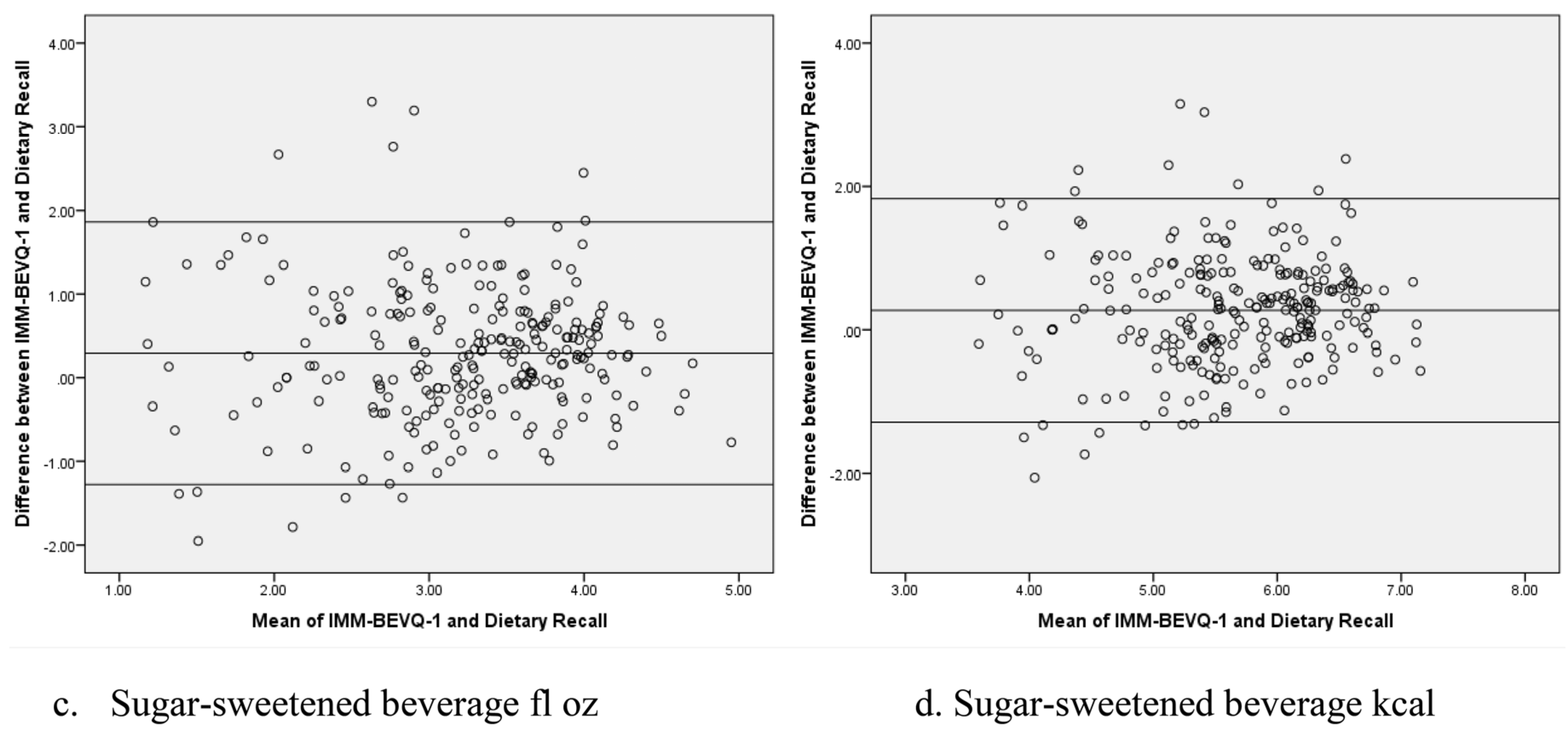
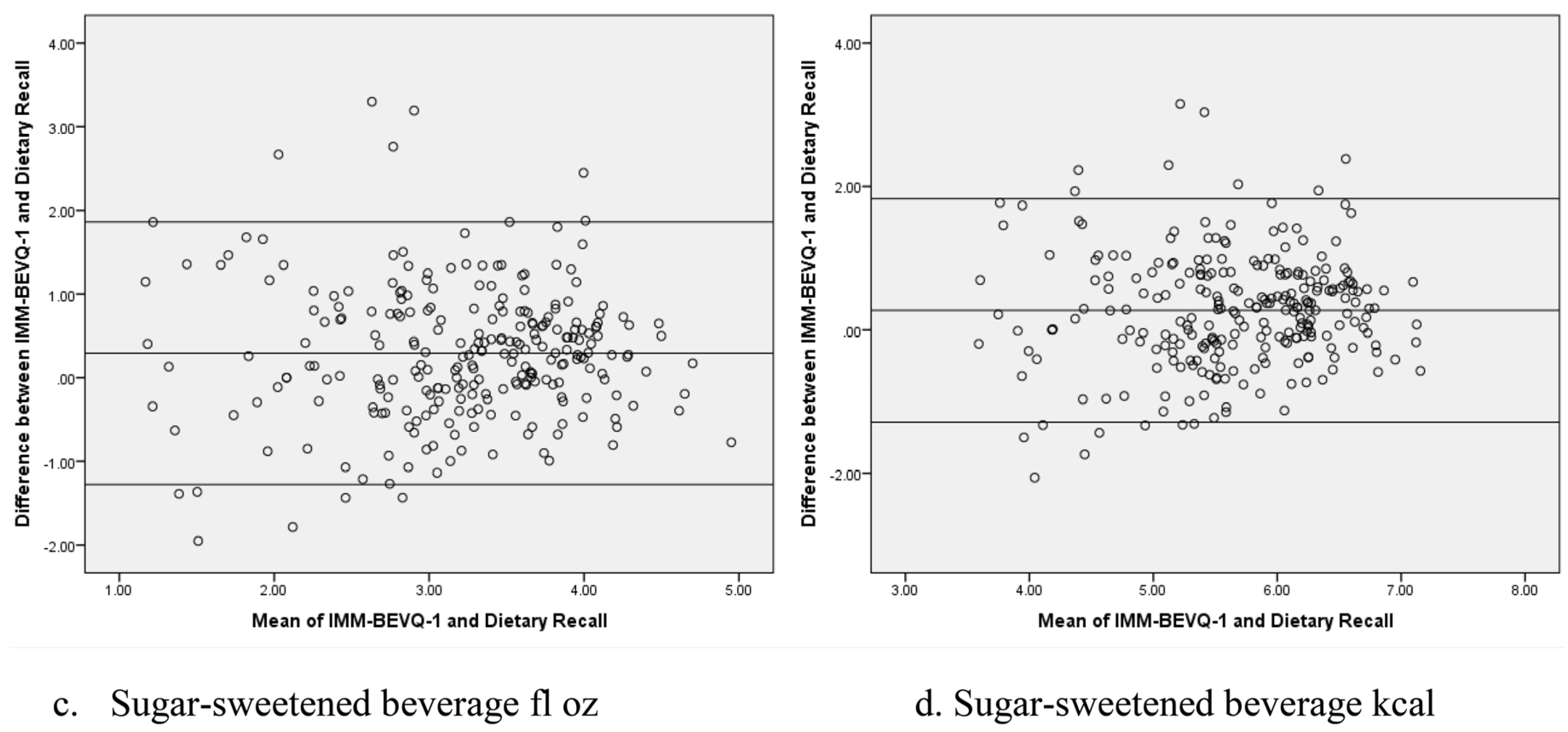
3.2. Comparative Validity
3.2.1. All Participants
3.2.2. Low versus Adequate Health Literate Participants
3.3. Sensitivity to Change
3.3.1. All Participants
3.3.2. Low versus Adequate Health Literate Participants
4. Discussion
4.1. Comparative Validity
4.2. Sensitivity to Change
4.3. Strengths & Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease; Boushey, C.J., Coulston, A.M., Rock, C.L., Monsen, E.R., Eds.; Academic Press: San Diego, CA, USA, 2001; Chapter 1; pp. 3–14. [Google Scholar]
- Johnson, R.; Soultanakis, R.; Matthews, D. Literacy and Body Fatness are Associated with Underreporting of Energy Intake in US Low-Income Women Using the Multiple-Pass 24-h Recall: A Doubly Labeled Water Study. J. Am. Diet. Assoc. 1998, 98, 1136–1140. [Google Scholar] [CrossRef]
- Smith, A.F. Cognitive psychological issues of relevance to the validity of dietary reports. Eur. J. Clin. Nutr. 1993, 47, S6–S18. [Google Scholar] [PubMed]
- Jonnalagadda, S.S.; Mitchell, D.C.; Smiciklas-Wright, H.; Meaker, K.B.; van Heel, N.; Karmally, W.; Ershow, A.G.; Kris-Etherton, P.M. Accuracy of energy intake data estimated by a multiple-pass, 24-h dietary recall technique. J. Am. Diet. Assoc. 2000, 100, 303–308. [Google Scholar] [CrossRef]
- Huizinga, M.M.; Carlisle, A.J.; Cavanaugh, K.L.; Davis, D.L.; Gregory, R.P.; Schlundt, D.G.; Rothman, R.L. Literacy, numeracy, and portion-size estimation skills. Am. J. Prev. Med. 2009, 36, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Falomir, Z.; Arregui, M.; Madueño, F.; Corella, D.; Coltell, Ó. Automation of Food Questionnaires in Medical Studies: A state-of-the-art review and future prospects. Comput. Biol. Med. 2012, 42, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Kristal, A.R.; Kolar, A.S.; Fisher, J.L.; Plascak, J.J.; Stumbo, P.J.; Weiss, R.; Paskett, E.D. Evaluation of web-based, self-administered, graphical food frequency questionnaire. J. Acad. Nutr. Diet. 2014, 114, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.L.; Swartzendruber, A.; DiClemente, R.J. Application of Audio Computer-Assisted Self-Interviews to Collect Self-Reported Health Data: An Overview. Caries Res. 2013, 47, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Riebl, S.K.; Paone, A.C.; Hedrick, V.E.; Zoellner, J.M.; Estabrooks, P.A.; Davy, B.M. The comparative validity of interactive multimedia questionnaires to paper-administered questionnaires for beverage intake and physical activity: Pilot study. JMIR Res. Protoc. 2013, 2, e40. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.F.; Jobe, J.B.; Mingay, D.J. Question-induced cognitive biases in reports of dietary intake by college men and women. Health Psychol. 1991, 10, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Greenlaw, C.; Brown-Welty, S. A comparison of web-based and paper-based survey methods: Testing assumptions of survey mode and response cost. Eval. Rev. 2009, 33, 464–480. [Google Scholar] [CrossRef] [PubMed]
- Ekman, A.; Dickman, P.W.; Klint, A.; Weiderpass, E.; Litton, J.-E. Feasibility of using web-based questionnaires in large population-based epidemiological studies. Eur. J. Epidemiol. 2006, 21, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Jantz, C.; Anderson, J.; Gould, S.M. Using computer-based assessments to evaluate interactive multimedia nutrition education among low-income predominantly Hispanic participants. J. Nutr. Educ. Behav. 2002, 34, 252–260. [Google Scholar] [CrossRef]
- Long, J.D.; Littlefield, L.A.; Estep, G.; Martin, H.; Rogers, T.J.; Boswell, C.; Shriver, B.J.; Roman-Shriver, C.R. Evidence review of technology and dietary assessment. Worldviews Evid. Based. Nurs. 2010, 7, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Ratzan, S.C.; Parker, R.M. Introduction. In National Library of Medicine Current Bibliographies in Medicine: Health Literacy; Selden, C., Zorn, M., Ratzan, S.C., Parker, R.M., Eds.; National Institutes of Health, U.S. Department of Health and Human Services: Bethesda, MD, USA, 2000. [Google Scholar]
- Yin, H.S.; Johnson, M.; Mendelsohn, A.L.; Abrams, M.A.; Sanders, L.M.; Dreyer, B.P. The health literacy of parents in the United States: A nationally representative study. Pediatrics 2009, 124, S289–S298. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, D.; Grumbach, K.; Piette, J.; Wang, F.; Osmond, D.; Daher, C.; Palacios, J.; Sullivan, G.D.; Bindman, A.B. Association of health literacy with diabetes outcomes. JAMA 2002, 288, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.M.; Ratzan, S.C.; Lurie, N. Health literacy: A policy challenge for advancing high-quality health care. Health Aff. 2003, 22, 147–153. [Google Scholar] [CrossRef]
- Kristal, A.R.; Feng, Z.; Coates, R.J.; Oberman, A.; George, V. Associations of race/ethnicity, education, and dietary intervention with the validity and reliability of a food frequency questionnaire: The Women’s Health Trial Feasibility Study in Minority Populations. Am. J. Epidemiol. 1997, 146, 856–869. [Google Scholar] [CrossRef] [PubMed]
- Marks, G.C.; Hughes, M.C.; van der Pols, J.C. Relative validity of food intake estimates using a food frequency questionnaire is associated with sex, age, and other personal characteristics. J. Nutr. 2006, 136, 459–465. [Google Scholar] [PubMed]
- Tooze, J.A.; Vitolins, M.Z.; Smith, S.L.; Arcury, T.A.; Davis, C.C.; Bell, R.A.; DeVellis, R.F.; Quandt, S.A. High levels of low energy reporting on 24-h recalls and three questionnaires in an elderly low-socioeconomic status population. J. Nutr. 2007, 137, 1286–1293. [Google Scholar] [PubMed]
- Johansson, G.; Wikman, Å.; Åhrén, A.-M.; Hallmans, G.; Johansson, I. Underreporting of energy intake in repeated 24-h recalls related to gender, age, weight status, day of interview, educational level, reported food intake, smoking habits and area of living. Public Health Nutr. 2001, 4, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, B.L. The influence of fatness, weight change, slimming history and other lifestyle variables on diet reporting in Danish men and women aged 35–65 years. Int. J. Obes. Relat. Metab. Disord. 1993, 17, 329–336. [Google Scholar] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The beverage intake questionnaire: Determining initial validity and reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Savla, J.; Comber, D.L.; Flack, K.D.; Estabrooks, P.A.; Nsiah-Kumi, P.A.; Ortmeier, S.; Davy, B.M. Development of a brief questionnaire to assess habitual beverage intake (BEVQ-15): Sugar-sweetened beverages and total beverage energy intake. J. Acad. Nutr. Diet. 2012, 112, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Ferguson, K.E.; Estabrooks, P.A.; Savla, J.; Dietrich, A.M.; Serrano, E.; Davy, B.M. A rapid beverage intake questionnaire can detect changes in beverage intake. Eat. Behav. 2013, 14, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.; Chen, Y.; Davy, B.; You, W.; Hedrick, V.; Corsi, T.; Estabrooks, P. Talking health, a pragmatic randomized-controlled health literacy trial targeting sugar-sweetened beverage consumption among adults: Rationale, design & methods. Contemp. Clin. Trials 2014, 37, 43–57. [Google Scholar] [PubMed]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Medically Underserved Areas/Populations: Guidelines for MUA and MUP Designation. Available online: https://bhw.hrsa.gov/shortage-designation/muap (accessed on 2 October 2014).
- Zoellner, J.M.; Hedrick, V.E.; You, W.; Chen, Y.; Davy, B.M.; Porter, K.J.; Bailey, A.; Lane, H.; Alexander, R.; Estabrooks, P.A. Effects of a behavioral and health literacy intervention to reduce sugar-sweetened beverages: A randomized-controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Stote, K.S.; Radecki, S.V.; Moshfegh, A.J.; Ingwersen, L.A.; Baer, D.J. The number of 24 h dietary recalls using the US Department of Agriculture’s automated multiple-pass method required to estimate nutrient intake in overweight and obese adults. Public Health Nutr. 2011, 14, 1736–1742. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.; You, W.; Connell, C.; Smith-Ray, R.L.; Allen, K.; Tucker, K.L.; Davy, B.M.; Estabrooks, P. Health literacy is associated with healthy eating index scores and sugar-sweetened beverage intake: Findings from the rural Lower Mississippi Delta. J. Am. Diet. Assoc. 2011, 111, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 3rd ed.; Academic Press: Cambridge, MA, USA, 2013; pp. 5–46. [Google Scholar]
- National Cancer Instititue’s Register of Validated Short Dietary Assessment Instruments. Available online: https://epi.grants.cancer.gov/diet/shortreg/ (accessed on 8 December 2016).
- KrisEtherton, P.; Eissenstat, B.; Jaax, S.; Srinath, U.; Scott, L.; Rader, J.; Pearson, T. Validation for MEDFICTS, a Dietary Assessment Instrument for Evaluating Adherence to Total and Saturated Fat Recommendations of the National Cholesterol Education Program Step 1 and Step 2 Diets. J. Am. Diet. Assoc. 2001, 101, 81–86. [Google Scholar] [CrossRef]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a food frequency questionnaire for use in Italian adults living in Sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Birgisdottir, B.E.; Kiely, M.; Martinez, J.A.; Thorsdottir, I. Validity of a food frequency questionnaire to assess intake of seafood in adults in three European countries. Food Control 2008, 19, 648–653. [Google Scholar] [CrossRef]
- Andersen, L.; Johansson, L.; Solvoll, K. Usefulness of a short food frequency questionnaire for screening of low intake of fruit and vegetable and for intake of fat. Eur. J. Public Health 2002, 12, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Kuhnle, G.G. Nutritional biomarkers for objective dietary assessment. J. Sci. Food Agric. 2012, 92, 1145–1149. [Google Scholar] [CrossRef] [PubMed]
- Halliday, T.M.; Davy, B.M.; Clark, A.G.; Baugh, M.E.; Hedrick, V.E.; Marinik, E.L.; Flack, K.D.; Savla, J.; Winett, S.; Winett, R.A. Dietary intake modification in response to a participation in a resistance training program for sedentary older adults with prediabetes: Findings from the Resist Diabetes study. Eat. Behav. 2014, 15, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Kristal, A.R.; Beresford, S.A.; Lazovich, D. Assessing change in diet-intervention research. Am. J. Clin. Nutr. 1994, 59, 185S–189S. [Google Scholar] [PubMed]
- Guyatt, G.; Walter, S.; Norman, G. Measuring change over time: Assessing the usefulness of evaluative instruments. J. Chronic Dis. 1987, 40, 171–178. [Google Scholar] [CrossRef]
- Monsen, E.R. Research: Successful Approaches, 2nd ed.; American Dietetic Association: Chicago, IL, USA, 2003. [Google Scholar]
- US Census Bureau (2010) American FactFinder Fact Sheet: Lee County, Giles County, Pulaski County, Washington County, Grayson County, Wise County, VA, USA. Available online: http://factfinder2.census.gov (accessed on 1 March 2014).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Validity Sample (n = 273) n (%) | Sensitivity Sample (n = 162) n (%) |
|---|---|---|
| Sex | ||
| Male | 46 (17) | 29 (18) |
| Female | 227 (83) | 133 (82) |
| Mean Age (years) ± SD | 42.0 ± 13.4 | 43.3 ± 13.3 |
| Race/Ethnicity | ||
| White | 256 (94) | 153 (94.5) |
| African American | 12 (4) | 7 (4.5) |
| Other | 5 (2) | 2 (1) |
| Mean BMI (kg/m2) ± SD | 33.1 ± 9.1 | 33.3 ± 9.2 |
| BMI Categories | ||
| Underweight (≤18.4) | 4 (2) | 2 (1) |
| Normal weight (18.5–24.9) | 54 (20) | 30 (18.5) |
| Overweight (25–29.9) | 61 (22) | 35 (21.5) |
| Obese (≥30) | 154 (56) | 95 (59) |
| Education Level | ||
| <High school | 29 (10.5) | 17 (10.5) |
| High school graduate | 56 (20.5) | 35 (21.5) |
| ≥Some college | 188 (69) | 110 (68) |
| Annual Household Income ($) | ||
| Mean income ± SD | 23,782 ± 17,306 | 24,907 ± 18,466 |
| ≤14,999 | 113 (41.5) | 68 (42) |
| 15,000–34,999 | 88 (32) | 44 (27) |
| 35,000–54,999 | 37 (13.5) | 22 (14) |
| ≥55,000 | 35 (13) | 28 (17) |
| Beverage Category | Health Literacy Level | IMM-BEVQ-1 a | Dietary Recall a | Mean Difference b |
|---|---|---|---|---|
| Water fl oz | Total (n = 273) | 21.3 (18.7) | 24.1 (25.6) | 2.8 (21.6) * |
| Low (n = 85) | 20.6 (19.5) | 23.2 (24.9) | 2.6 (23.8) | |
| Adequate (n = 188) | 21.6 (18.3) | 24.5 (26.0) | 2.9 (20.7) | |
| 100% Fruit Juice fl oz | Total | 2.9 (4.5) | 0.7 (1.9) | 2.3 (4.6) *** |
| Low | 3.5 (5.7) | 0.5 (1.5) | 3.0 (5.6) *** | |
| Adequate | 2.7 (3.9) | 0.8 (2.0) | 1.9 (4.0) *** | |
| Sweetened Juice Drinks fl oz | Total | 3.7 (8.9) | 1.0 (2.5) | 2.6 (9.1) *** |
| Low | 4.9 (10.1) | 0.9 (2.4) | 4.0 (10.4) ** | |
| Adequate | 3.1 (8.3) | 1.1 (2.6) | 2.0 (8.4) ** | |
| Whole Milk fl oz | Total | 3.3 (9.0) | 0.5 (1.8) | 2.8 (8.5) *** |
| Low | 4.7 (11.4) | 0.4 (1.1) | 4.3 (11.2) ** | |
| Adequate | 2.7 (7.7) | 0.6 (2.0) | 2.1 (6.9) *** | |
| Reduced Fat Milk fl oz | Total | 2.6 (5.1) | 1.1 (2.9) | 1.5 (4.7) *** |
| Low | 2.3 (4.6) | 1.1 (2.3) | 1.2 (4.5) * | |
| Adequate | 2.7 (5.3) | 1.1 (3.1) | 1.6 (4.8) *** | |
| Fat-Free Milk fl oz | Total | 1.6 (4.5) | 0.9 (3.1) | 0.7 (3.9) ** |
| Low | 0.5 (1.7) | 0.3 (1.5) | 0.2 (1.9) | |
| Adequate | 2.1 (5.3) | 1.1 (3.5) | 1.0 (4.5) ** | |
| Regular Soft Drinks fl oz | Total | 14.8 (17.9) | 12.2 (15.6) | 2.6 (13.4) ** |
| Low | 16.5 (18.5) | 12.9 (16.4) | 3.6 (15.8) * | |
| Adequate | 14.0 (17.6) | 11.8 (15.2) | 2.1 (12.1) * | |
| Artificially Sweetened Drinks fl oz | Total | 6.4 (13.6) | 4.1 (11.0) | 2.3 (8.5) *** |
| Low | 6.6 (14.2) | 4.4 (10.8) | 2.2 (7.4) ** | |
| Adequate | 6.3 (13.3) | 3.9 (11.1) | 2.4 (9.0) *** | |
| Sweet Tea fl oz | Total | 9.0 (13.9) | 5.7 (11.7) | 3.3 (12.7) *** |
| Low | 8.5 (14.6) | 3.7 (7.5) | 4.9 (14.5) ** | |
| Adequate | 9.2 (13.6) | 6.6 (13.0) | 2.6 (11.8) ** | |
| Sweetened Coffee fl oz | Total | 8.9 (12.5) | 7.0 (17.1) | 1.8 (14.1) * |
| Low | 6.6 (11.1) | 4.4 (8.4) | 2.2 (10.2) | |
| Adequate | 9.9 (13.0) | 8.3 (19.8) | 1.7 (15.5) | |
| Black Coffee/Tea fl oz | Total | 2.7 (8.8) | 4.1 (11.1) | 1.3 (11.2) |
| Low | 2.6 (8.1) | 5.4 (13.5) | 2.9 (12.2) * | |
| Adequate | 2.8 (9.2) | 3.4 (9.9) | 0.6 (10.6) | |
| Beer fl oz | Total | 1.3 (5.2) | 0.9 (4.8) | 0.4 (4.5) |
| Low | 1.8 (7.5) | 1.4 (6.7) | 0.4 (6.4) | |
| Adequate | 1.0 (3.7) | 0.7 (3.6) | 0.3 (3.4) | |
| Liquor fl oz | Total | 0.1 (0.6) | 0.1 (1.3) | 0.0 (1.3) |
| Low | 0.1 (0.5) | 0.0 (0.0) | 0.1 (0.5) | |
| Adequate | 0.1 (0.6) | 0.2 (1.6) | 0.0 (1.6) | |
| Wine fl oz | Total | 0.2 (0.7) | 0.1 (0.6) | 0.1 (0.8) * |
| Low | 0.1 (0.5) | 0.1 (0.4) | 0.1 (0.6) | |
| Adequate | 0.3 (0.8) | 0.1 (0.6) | 0.1 (0.9) * | |
| Energy Drinks fl oz | Total | 2.3 (6.3) | 1.3 (4.0) | 1.0 (6.4) * |
| Low | 3.8 (9.5) | 0.8 (3.0) | 3.0 (9.3) ** | |
| Adequate | 1.6 (3.9) | 1.5 (4.3) | 0.1 (4.2) | |
| Total Sugar-Sweetened Beverages fl oz | Total | 38.2 (28.8) | 27.6 (23.4) | 10.6 (27.4) *** |
| Low | 39.9 (34.6) | 23.6 (19.6) | 16.3 (32.5) *** | |
| Adequate | 37.5 (25.9) | 29.5 (24.7) | 8.0 (24.5) *** | |
| Total Sugar-Sweetened Beverage kcal | Total | 440 (351) | 316 (254) | 124 (317) *** |
| Low | 477 (421) | 281 (242) | 196 (395) *** | |
| Adequate | 422 (314) | 331 (259) | 91 (269) *** | |
| Total Beverage fl oz | Total | 80.3 (39.9) | 64.3 (31.4) | 16.0 (41.2) *** |
| Low | 81.9 (47.9) | 60.8 (31.8) | 21.2 (49.7) *** | |
| Adequate | 79.5 (35.9) | 65.9 (31.2) | 13.6 (36.6) *** | |
| Total Beverage kcal | Total | 659 (478) | 391 (279) | 268 (460) *** |
| Low | 723 (586) | 344 (252) | 380 (567) *** | |
| Adequate | 630 (420) | 412 (288) | 217 (395) *** |
| Beverage Category | Health Literacy Level | IMM-BEVQ-1 a | IMM-BEVQ-2 a | Mean Difference between IMM 1 and 2 b | Mean Difference between Dietary Recall 1 and 2 c | Mean Difference between IMM Change and Recall Change d |
|---|---|---|---|---|---|---|
| Water fl oz | Total (n = 162) | 21.2 (18.7) | 26.4 (19.0) | 5.2 (20.5) ** | 5.5 (26.6) ** | 0.4 (29.9) |
| Low (n = 58) | 20.4 (18.0) | 26.3 (20.5) | 5.9 (23.0) | 7.0 (30.4) | 1.0 (39.3) | |
| Adequate (n = 104) | 21.6 (19.2) | 26.4 (18.3) | 4.7 (19.2) * | 4.6 (24.3) | 0.0 (23.5) | |
| 100% Fruit Juice fl oz | Total | 3.2 (5.0) | 2.7 (6.6) | 0.5 (7.1) | 0.0 (2.7) | 0.5 (7.5) |
| Low | 4.3 (6.5) | 3.5 (9.6) | 0.8 (11.2) | 0.1 (1.6) | 0.6 (11.2) | |
| Adequate | 2.6 (3.9) | 2.2 (4.2) | 0.4 (3.4) | 0.1 (3.1) | 0.5 (4.4) | |
| Sweetened Juice Drinks fl oz | Total | 3.9 (9.4) | 2.2 (7.8) | 1.8 (11.5) | 0.0 (4.6) | 1.7 (11.2) * |
| Low | 6.1 (11.8) | 3.4 (11.1) | 2.7 (16.4) | 0.1 (5.0) | 2.6 (15.3) | |
| Adequate | 2.8 (7.6) | 1.5 (4.9) | 1.3 (7.5) | 0.0 (4.5) | 1.2 (8.0) | |
| Whole Milk fl oz | Total | 3.0 (8.6) | 1.9 (5.4) | 1.1 (7.8) | 0.3 (2.2) | 0.8 (7.4) |
| Low | 3.7 (9.7) | 3.1 (7.2) | 0.6 (10.1) | 0.0 (1.7) | 0.7 (10.0) | |
| Adequate | 2.7 (8.0) | 1.3 (3.9) | 1.4 (6.2) * | 0.5 (2.4) * | 0.9 (5.5) | |
| Reduced Fat Milk fl oz | Total | 2.5 (4.9) | 2.3 (5.0) | 0.2 (5.4) | 0.3 (3.4) | 0.0 (6.2) |
| Low | 3.0 (5.4) | 3.8 (7.0) | 0.7 (8.1) | 0.2 (3.3) | 0.7 (8.8) | |
| Adequate | 2.2 (4.7) | 1.5 (3.2) | 0.7 (3.0) * | 0.3 (3.5) | 0.4 (4.1) | |
| Fat-Free Milk fl oz | Total | 1.6 (4.2) | 2.8 (9.0) | 1.2 (8.5) | 0.2 (5.6) | 1.0 (10.3) |
| Low | 0.5 (1.6) | 2.2 (8.5) | 1.6 (8.6) | 0.1 (1.6) | 1.7 (8.4) | |
| Adequate | 2.2 (5.1) | 3.2 (9.3) | 1.0 (8.5) | 0.3 (6.9) | 0.7 (11.2) | |
| Regular Soft Drinks fl oz | Total | 14.3 (17. 2) | 6.8 (12.7) | 7.5 (16.0) *** | 4.8 (12.7) *** | 2.8 (15.3) * |
| Low | 15.8 (18.4) | 5.5 (10.3) | 10.3 (16.8) *** | 5.9 (14.6) ** | 4.8 (14.8) * | |
| Adequate | 13.5 (16.5) | 7.6 (13.8) | 6.0 (15.5) *** | 4.2 (11.6) *** | 1.7 (15.5) | |
| Artificially Sweetened Drinks fl oz | Total | 6.3 (13.5) | 7.1 (12.8) | 0.8 (13.4) | 0.2 (11.8) | 0.5 (14.4) |
| Low | 7.6 (14.9) | 6.6 (13.5) | 1.0 (2.0) | 0.3 (10.7) | 0.4 (11.8) | |
| Adequate | 5.7 (12.6) | 7.5 (12.5) | 1.8 (12.4) | 0.5 (12.4) | 1.0 (15.6) | |
| Sweet Tea fl oz | Total | 9.1 (14.8) | 4.1 (9.5) | 5.1 (14.2) *** | 1.1 (10.0) ** | 4.0 (14.9) ** |
| Low | 8.3 (15.2) | 3.4 (9.6) | 4.9 (16.6) * | 0.5 (9.3) | 5.5 (15.5) * | |
| Adequate | 9.6 (14.7) | 4.5 (9.4) | 5.1 (12.8) *** | 2.0 (10.2) | 3.1 (14.6) * | |
| Sweetened Coffee fl oz | Total | 9.5 (14.1) | 6.5 (10.8) | 3.0 (11.3) ** | 4.3 (18.1) | 1.3 (18.8) |
| Low | 6.3 (12.1) | 5.7 (9.7) | 0.7 (12.6) | 1.6 (9.2) | 0.7 (15.1) | |
| Adequate | 11.2 (14.8) | 6.9 (11.4) | 4.3 (10.4) *** | 5.8 (21.4) ** | 1.6 (20.5) | |
| Black Coffee/Tea fl oz | Total | 3.2 (9.5) | 3.8 (9.1) | 0.6 (11.5) | 1.4 (14.4) | 0.9 (17.0) |
| Low | 3.0 (9.2) | 4.6 (11.3) | 1.5 (12.7) | 0.9 (13.4) | 2.5 (17.6) | |
| Adequate | 3.3 (9.7) | 3.4 (7.6) | 0.1 (10.8) | 2.8 (14.8) | 2.8 (16.5) | |
| Beer fl oz | Total | 1.6 (6.7) | 1.7 (6.8) | 0.1 (6.7) | 0.1 (6.3) | 0.2 (6.1) |
| Low | 2.1 (8.9) | 2.8 (9.9) | 0.7 (10.2) | 0.7 (9.4) | 0.0 (8.7) | |
| Adequate | 1.4 (4.9) | 1.1 (3.9) | 0.3 (3.2) | 0.5 (3.6) | 0.2 (3.9) | |
| Liquor fl oz | Total | 0.1 (0.5) | 0.1 (0.4) | 0.0 (0.3) | 0.0 (0.1) | 0.0 (0.3) |
| Low | 0.1 (0.6) | 0.1 (0.5) | 0.0 (0.4) | 0.0 (0.0) | 0.0 (0.4) | |
| Adequate | 0.1 (0.4) | 0.1 (0.4) | 0.0 (0.2) | 0.0 (0.1) | 0.0 (0.3) | |
| Wine fl oz | Total | 0.2 (0.7) | 0.2 (0.8) | 0.0 (0.7) | 0.1 (0.9) | 0.0 (1.0) |
| Low | 0.2 (0.5) | 0.1 (0.8) | 0.1 (0.8) | 0.1 (1.2) | 0.1 (0.7) | |
| Adequate | 0.3 (0.8) | 0.2 (0.8) | 0.1 (0.7) | 0.2 (0.7)* | 0.1 (1.1) | |
| Energy Drinks fl oz | Total | 1.8 (3.7) | 1.1 (5.1) | 0.6 (5.9) | 0.4 (3.9) | 0.4 (5.3) |
| Low | 2.3 (4.1) | 0.9 (2.1) | 1.4 (3.3) ** | 0.4 (3.5) | 1.4 (3.4) ** | |
| Adequate | 1.5 (3.4) | 1.3 (6.3) | 0.2 (6.9) | 0.4 (4.2) | 0.2 (6.1) | |
| Total Sugar Sweetened Beverages fl oz | Total | 38.4 (30.8) | 20.3 (23.6) | 18.1 (31.8) *** | 10.8 (23.7) *** | 7.2 (33.8) ** |
| Low | 38.5 (37.0) | 18.2 (23.9) | 20.3 (40.0) *** | 7.3 (19.4) ** | 13.0 (36.4) ** | |
| Adequate | 38.4 (26.9) | 21.5 (23.5) | 16.9 (26.2) *** | 12.7 (25.6) *** | 4.0 (32.0) | |
| Total Sugar-Sweetened Beverages kcal | Total | 438 (369) | 227 (286) | 212 (382) *** | 118 (249) *** | 92 (377) * |
| Low | 462 (446) | 208 (299) | 254 (478) *** | 91 (236) ** | 163 (427) ** | |
| Adequate | 426 (319) | 239 (279) | 187 (316) *** | 134 (256) *** | 52 (341) | |
| Total Beverage fl oz | Total | 80.8 (43.3) | 69.0 (40.4) | 11.8 (45.5) ** | 4.3 (30.9) | 7.6 (53.5) |
| Low | 82.0 (54.1) | 70.3 (52.1) | 11.7 (62.0) | 1.1 (34.1) | 10.6 (70.0) | |
| Adequate | 80.1 (36.2) | 68.2 (32.2) | 11.9 (33.2) *** | 6.0 (29.0) * | 6.0 (41.8) | |
| Total Beverage kcal | Total | 655 (510) | 422 (487) | 234 (506) *** | 131 (280) *** | 102 (506) * |
| Low | 715 (623) | 474 (652) | 243 (677) ** | 89 (258) * | 154 (649) | |
| Adequate | 621 (435) | 393 (365) | 228 (383) *** | 154 (291) *** | 74 (407) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hooper, L.P.; Myers, E.A.; Zoellner, J.M.; Davy, B.M.; Hedrick, V.E. The Impact of Health Literacy Status on the Comparative Validity and Sensitivity of an Interactive Multimedia Beverage Intake Questionnaire. Nutrients 2017, 9, 5. https://doi.org/10.3390/nu9010005
Hooper LP, Myers EA, Zoellner JM, Davy BM, Hedrick VE. The Impact of Health Literacy Status on the Comparative Validity and Sensitivity of an Interactive Multimedia Beverage Intake Questionnaire. Nutrients. 2017; 9(1):5. https://doi.org/10.3390/nu9010005
Chicago/Turabian StyleHooper, Lucy P., Emily A. Myers, Jamie M. Zoellner, Brenda M. Davy, and Valisa E. Hedrick. 2017. "The Impact of Health Literacy Status on the Comparative Validity and Sensitivity of an Interactive Multimedia Beverage Intake Questionnaire" Nutrients 9, no. 1: 5. https://doi.org/10.3390/nu9010005