B-Vitamin Intake and Biomarker Status in Relation to Cognitive Decline in Healthy Older Adults in a 4-Year Follow-Up Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
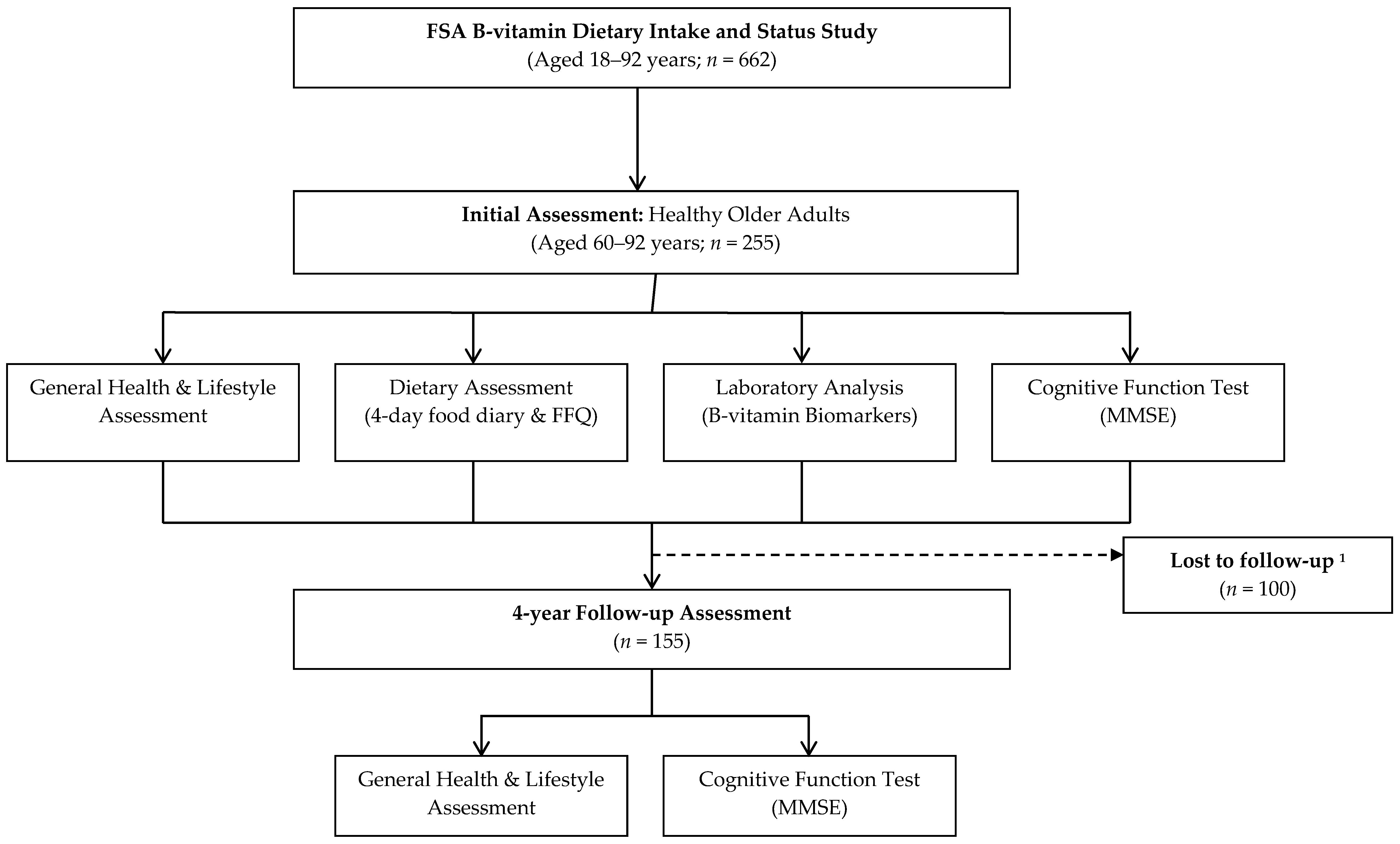
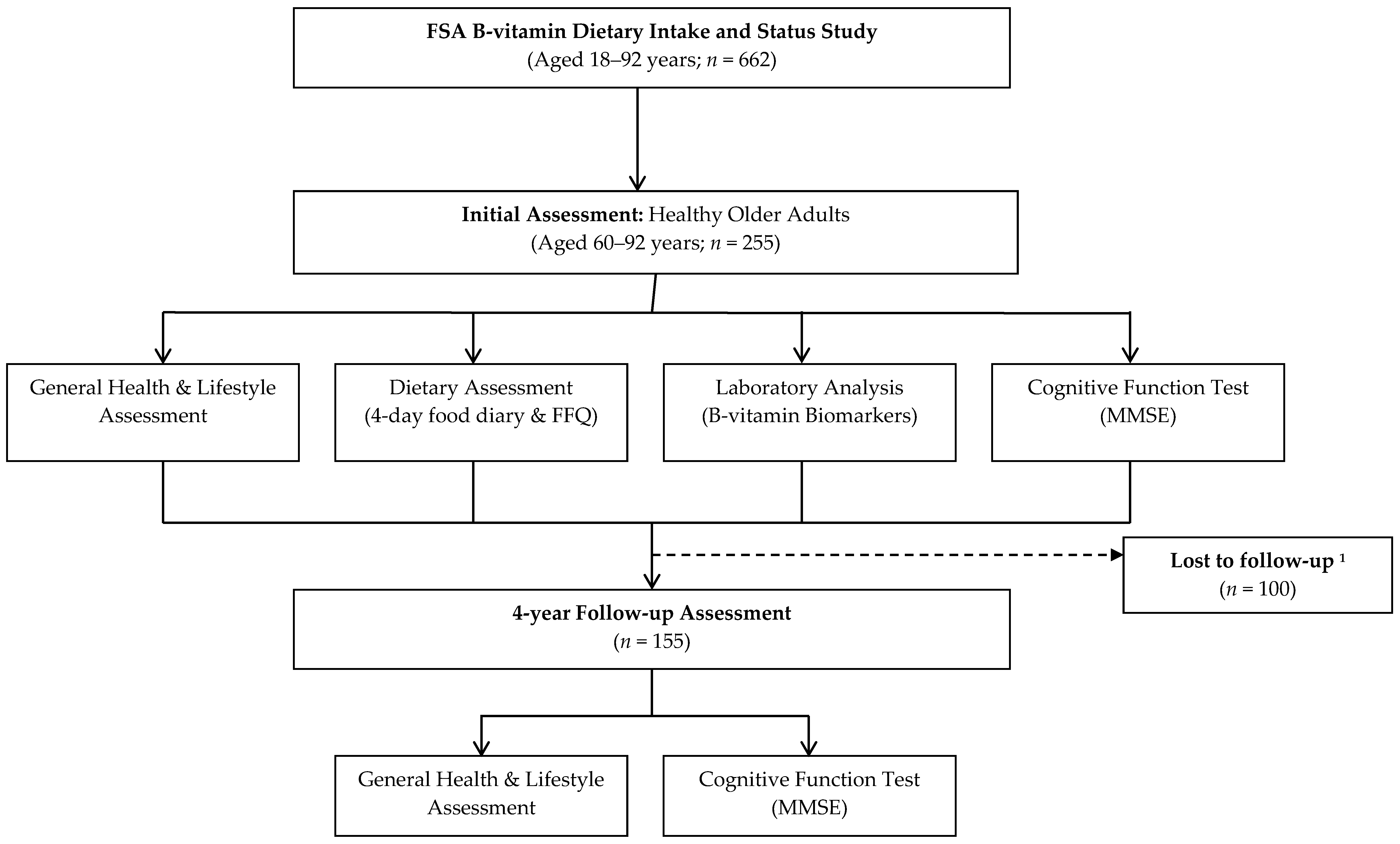
2.1. Participant Recruitment and Study Design
2.2. Cognitive Assessment
2.3. Dietary and Lifestyle Assessment
2.4. Laboratory Analysis
2.5. Statistical Analysis
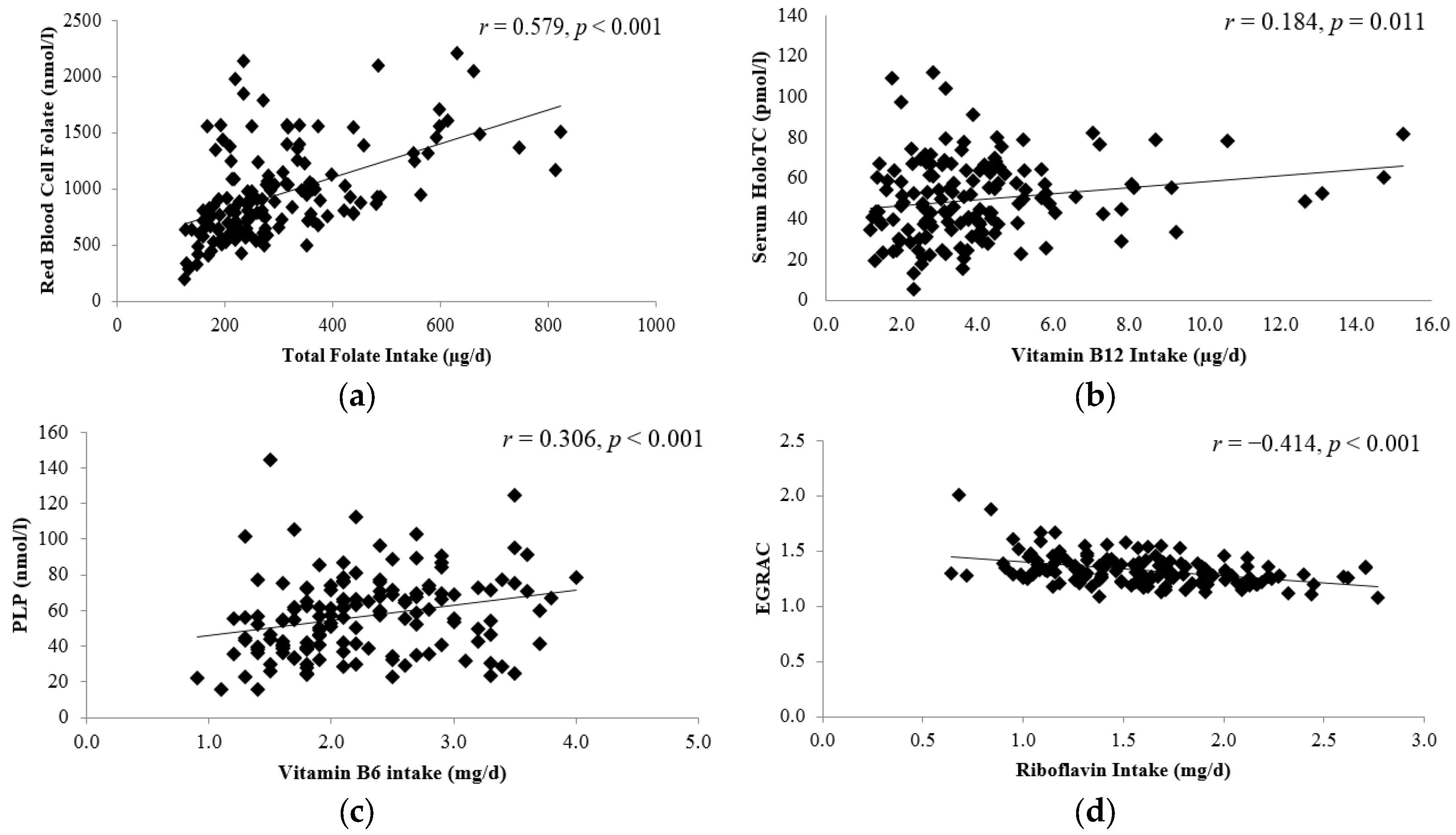
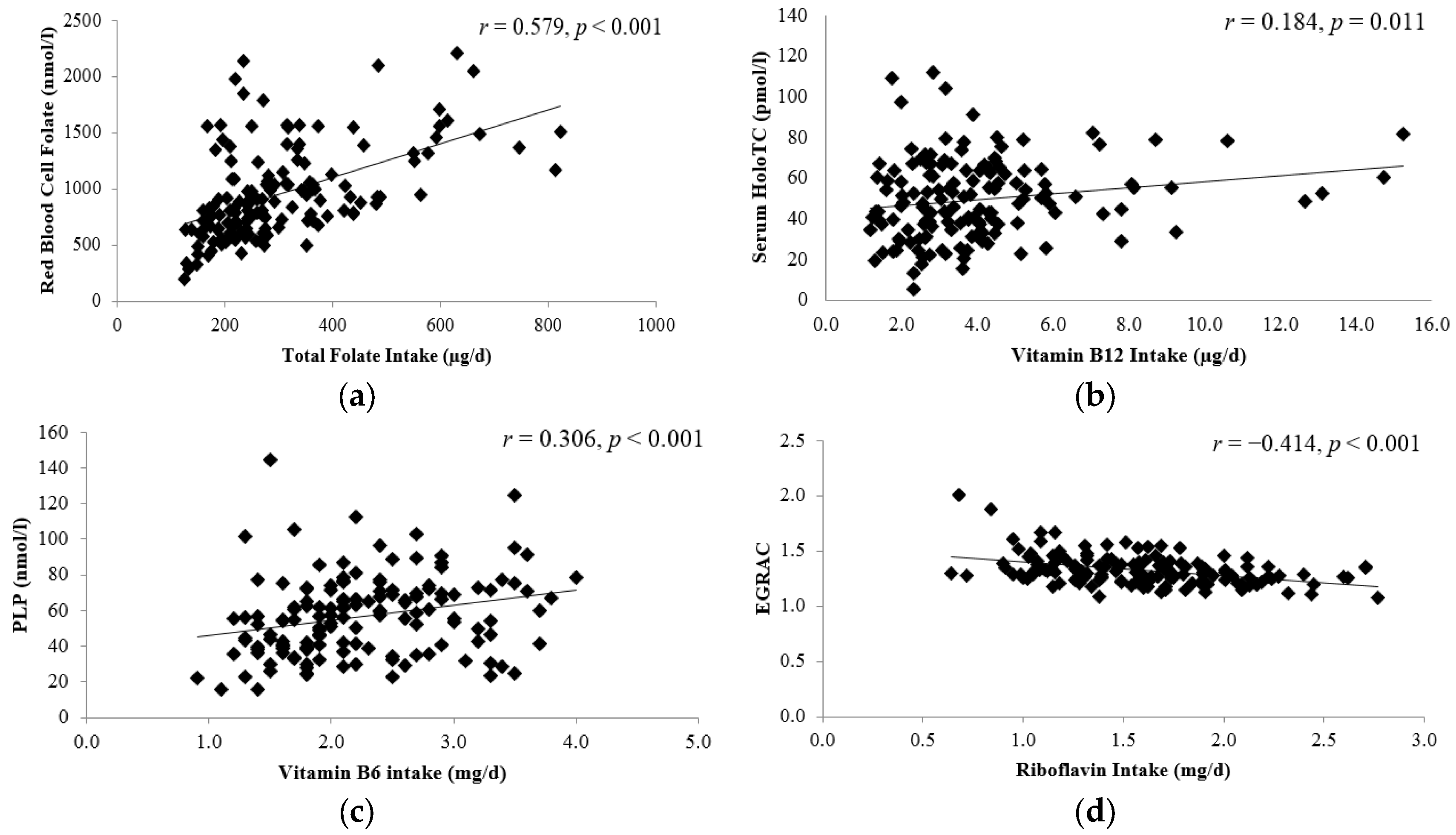
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MMSE | Mini-mental state examination |
| HoloTC | Holotranscobalamin—functional indicator of metabolically active fraction of vitamin B12 |
| MMA | methymalonic acid—an indicator of vitamin B12 status, a higher MMA status indicates a lower vitamin B12 status |
| PLP | Pyridoxal-5-phosphate—a measure of vitamin B6 status |
| EGRAC | Erythrocyte glutathione reductase activation coefficient—a functional indicator of riboflavin status, a higher ratio indicates a lower riboflavin status |
Appendix A

{kind=link}
{kind=link}
| Participants (n = 155) | Non-Participants (n = 100) | p-Value | |
|---|---|---|---|
| General Characteristics | |||
| Age (years) | 69.5 (7.3) | 72.2 (8.1) | 0.007 |
| Male n (%) | 60 (39) | 34 (34) | 0.530 |
| BMI (kg/m2) | 27.5 (4.2) | 27.3 (3.5) | 0.981 |
| Smokers n (%) | 6 (4) | 5 (5) | |
| Cognitive Function Score | |||
| MMSE Total Score | 29.1 (1.3) | 28.7 (1.4) | 0.093 |
| Orientation | 9.9 (0.3) | 9.8 (0.5) | 0.140 |
| Registration | 3.0 (0.1) | 3.0 (0.1) | 0.273 |
| Attention | 4.7 (0.7) | 4.6 (0.9) | 0.243 |
| Recall | 2.7 (0.6) | 2.6 (0.6) | 0.825 |
| Total Verbal | 20.0 (1.1) | 20.0 (1.2) | 0.263 |
| Language | 8.8 (0.5) | 8.6 (0.6) | 0.094 |
| B-vitamin Biomarker Status | |||
| Red blood cell folate (nmol/L) | 954 (410) | 851 (359) | 0.080 |
| Serum total vitamin B12 (pmol/L) | 282 (106) | 257 (127) | 0.013 |
| Serum HoloTC (pmol/L) | 50.8 (24.3) | 47.1 (28.8) | 0.381 |
| Serum MMA (µmol/L) | 0.24 (0.19) | 0.36 (0.56) | 0.035 |
| Vitamin B6 (Plasma PLP; nmol/L) | 58.4 (25.8) | 54.3 (22.9) | 0.314 |
| Riboflavin (EGRAC) | 1.33 (0.14) | 1.34 (0.15) | 0.387 |
| Plasma total homocysteine (µmol/L) | 12.0 (3.7) | 13.1 (4.4) | 0.117 |
| Gastric Function | |||
| Pepsinogen I (µg/L) | 126.8 (70.8) | 135.3 (78.2) | 0.515 |
| Pepsinogen Ratio2 | 8.4 (6.7) | 8.0 (6.6) | 0.713 |
References
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the national institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Alzheimer’s Disease International. World Alzheimer Report 2015 the Global Impact of Dementia an Analysis of Prevalence, Incidence, Cost & Trends; Alzheimer’s Disease International (ADI): London, UK, 2015. [Google Scholar]
- Morris, M.S. The role of B vitamins in preventing and treating cognitive impairment and decline. Adv. Nutr. 2012, 3, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Smith, A.; Jobst, K.A.; Refsum, H.; Sutton, L.; Ueland, P.M. Folate, vitamin B12, and serum total homocysteine levels in confirmed Alzheimer disease. Arch. Neurol. 1998, 55, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Doets, E.L.; Ueland, P.M.; Tell, G.S.; Vollset, S.E.; Nygård, O.K.; van’t Veer, P.; de Groot, L.C.P.G.M.; Nurk, E.; Refsum, H.; Smith, A.D.; et al. Interactions between plasma concentrations of folate and markers of vitamin B12 status with cognitive performance in elderly people not exposed to folic acid fortification: The hordaland health study. Br. J. Nutr. 2014, 111, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Flicker, L.; Singh, U.; Hirani, V.; Almeida, O.P. Homocysteine, depression and cognitive function in older adults. J. Affect. Disord. 2013, 151, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Kado, D.M.; Karlamangla, A.S.; Huang, M.-H.; Troen, A.; Rowe, J.W.; Selhub, J.; Seeman, T.E. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high-functioning adults: Macarthur studies of successful aging. Am. J. Med. 2005, 118, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, D.; Peter, I.; Scott, T.M.; Parnell, L.D.; Lai, C.-Q.; Crott, J.W.; Ordovás, J.M.; Selhub, J.; Griffith, J.; Rosenberg, I.H.; et al. Status of vitamins B-12 and B-6 but not of folate, homocysteine, and the methylenetetrahydrofolate reductase C677T polymorphism are associated with impaired cognition and depression in adults. J. Nutr. 2012, 142, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- McCaddon, A.; Davies, G.; Hudson, P.; Tandy, S.; Cattell, H. Total serum homocysteine in senile dementia of Alzheimer type. Int. J. Geriatr. Psychiatry 1998, 13, 235–239. [Google Scholar] [CrossRef]
- Blasko, I.; Hinterberger, M.; Kemmler, G.; Jungwirth, S.; Krampla, W.; Leitha, T.; Heinz Tragl, K.; Fischer, P. Conversion from mild cognitive impairment to dementia: Influence of folic acid and vitamin B12 use in the vita cohort. J. Nutr. Health Aging 2012, 16, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Haan, M.N.; Miller, J.W.; Aiello, A.E.; Whitmer, R.A.; Jagust, W.J.; Mungas, D.M.; Allen, L.H.; Green, R. Homocysteine, B vitamins, and the incidence of dementia and cognitive impairment: Results from the sacramento area latino study on aging. Am. J. Clin. Nutr. 2007, 85, 511–517. [Google Scholar] [PubMed]
- Hooshmand, B.; Solomon, A.; Kareholt, I.; Rusanen, M.; Hanninen, T.; Leiviska, J.; Winblad, B.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Associations between serum homocysteine, holotranscobalamin, folate and cognition in the elderly: A longitudinal study. J. Intern. Med. 2012, 271, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Zylberstein, D.E.; Lissner, L.; Björkelund, C.; Mehlig, K.; Thelle, D.S.; Gustafson, D.; Östling, S.; Waern, M.; Guo, X.; Skoog, I. Midlife homocysteine and late-life dementia in women. A prospective population study. Neurobiol. Aging 2011, 32, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Birks, J.; Nexo, E.; Ueland, P.M.; Schneede, J.; Scott, J.; Molloy, A.; Evans, J.G. Low vitamin B-12 status and risk of cognitive decline in older adults. Am. J. Clin. Nutr. 2007, 86, 1384–1391. [Google Scholar] [PubMed]
- Morris, M.S.; Selhub, J.; Jacques, P.F. Vitamin B-12 and folate status in relation to decline in scores on the mini-mental state examination in the framingham heart study. J. Am. Geriatr. Soc. 2012, 60, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Riggs, K.M.; Spiro, A.; Tucker, K.; Rush, D. Relations of vitamin B-12, vitamin B-6, folate, and homocysteine to cognitive performance in the normative aging study. Am. J. Clin. Nutr. 1996, 63, 306–314. [Google Scholar] [PubMed]
- Durga, J.; van Boxtel, M.P.J.; Schouten, E.G.; Kok, F.J.; Jolles, J.; Katan, M.B.; Verhoef, P. Effect of 3-year folic acid supplementation on cognitive function in older adults in the facit trial: A randomised, double blind, controlled trial. Lancet 2007, 369, 208–216. [Google Scholar] [CrossRef]
- Deijen, J.B.; Beek, E.J.; Orlebeke, J.F.; Berg, H. Vitamin B-6 supplementation in elderly men: Effects on mood, memory, performance and mental effort. Psychopharmacology 1992, 109, 489–496. [Google Scholar] [CrossRef] [PubMed]
- De Jager, C.A.; Oulhaj, A.; Jacoby, R.; Refsum, H.; Smith, A.D. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2012, 27, 592–600. [Google Scholar] [CrossRef] [PubMed]
- McMahon, J.A.; Green, T.J.; Skeaff, C.M.; Knight, R.G.; Mann, J.I.; Williams, S.M. A controlled trial of homocysteine lowering and cognitive performance. N. Engl. J. Med. 2006, 354, 2764–2772. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Flicker, L.; Alfonso, H.; Thomas, J.; Clarnette, R.; Martins, R.; Almeida, O.P. Vitamins B12, B6, and folic acid for cognition in older men. Neurology 2010, 75, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- Van der Zwaluw, N.L.; Dhonukshe-Rutten, R.A.M.; van Wijngaarden, J.P.; Brouwer-Brolsma, E.M.; van de Rest, O.; In ’t Veld, P.H.; Enneman, A.W.; van Dijk, S.C.; Ham, A.C.; Swart, K.M.A.; et al. Results of 2-year vitamin B treatment on cognitive performance: Secondary data from an RCT. Neurology 2014, 83, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Kasturiratne, A.; Simmonds, M. Effect of folic acid, with or without other B vitamins, on cognitive decline: Meta-analysis of randomized trials. Am. J. Med. 2010, 123, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Almeida, O.P. Effect of homocysteine lowering treatment on cognitive function: A systematic review and meta-analysis of randomized controlled trials. J. Alzheimers Dis. 2012, 29, 133–149. [Google Scholar] [PubMed]
- McGarel, C.; Pentieva, K.; Strain, J.J.; McNulty, H. Emerging roles for folate and related B-vitamins in brain health across the lifecycle. Proc. Nutr. Soc. 2015, 74, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: A randomized controlled trial. PLoS ONE 2010, 5, e12244. [Google Scholar] [CrossRef] [PubMed]
- Douaud, G.; Refsum, H.; de Jager, C.A.; Jacoby, R.; Nichols, T.E.; Smith, S.M.; Smith, A.D. Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc. Natl. Acad. Sci. USA 2013, 110, 9523–9528. [Google Scholar] [CrossRef] [PubMed]
- Hoey, L.; McNulty, H.; Askin, N.; Dunne, A.; Ward, M.; Pentieva, K.; Strain, J.; Molloy, A.M.; Flynn, C.A.; Scott, J.M. Effect of a voluntary food fortification policy on folate, related B vitamin status, and homocysteine in healthy adults. Am. J. Clin. Nutr. 2007, 86, 1405–1413. [Google Scholar] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Food Standards Agency. Food Portion Sizes, 3rd ed.Mills, A., Patel, S., Crawley, H., Eds.; Stationery Office Books: London, UK, 2002.
- Leino, A. Fully automated measurement of total homocysteine in plasma and serum on the Abbott iMx analyzer. Clin. Chem. 1999, 45, 569–570. [Google Scholar] [PubMed]
- Molloy, A.M.; Scott, J.M. Microbiological assay for serum, plasma, and red cell folate using cryopreserved, microtiter plate method. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1997; Volume 281, pp. 43–53. [Google Scholar]
- Kelleher, B.P.; Broin, S.D. Microbiological assay for vitamin B12 performed in 96-well microtitre plates. J. Clin. Pathol. 1991, 44, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J.; Pentieva, K.D.; Matthews, N.; Macdonald, A. A simple, sensitive and reproducible assay for pyridoxal 5′-phosphate and 4-pyridoxic acid in human plasma. Clin. Chim. Acta 1999, 280, 101–111. [Google Scholar] [CrossRef]
- Powers, H.J.; Bates, C.J.; Prentice, A.M.; Lamb, W.H.; Jepson, M.; Bowman, H. The relative effectiveness of iron and iron with riboflavin in correcting a microcytic anaemia in men and children in rural Gambia. Hum. Nutr. Clin. Nutr. 1983, 37, 413–425. [Google Scholar] [PubMed]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.; den Heijer, M.; Kluijtmans, L.A.; van den Heuvel, L.P.; et al. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nat. Genet. 1995, 10, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Park, H.L.; O’Connell, J.E.; Thomson, R.G. A systematic review of cognitive decline in the general elderly population. Int. J. Geriatr. Psychiatry 2003, 18, 1121–1134. [Google Scholar] [CrossRef] [PubMed]
- Britain, G. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom: Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy; Reports of Health and Social Subjects; Stationery Office Books: London, UK, 1991. [Google Scholar]
- Tucker, K.L.; Qiao, N.; Scott, T.; Rosenberg, I.; Spiro, A. High homocysteine and low B vitamins predict cognitive decline in aging men: The veterans affairs normative aging study. Am. J. Clin. Nutr. 2005, 82, 627–635. [Google Scholar] [PubMed]
- Bryan, J.; Calvaresi, E.; Hughes, D. Short-term folate, vitamin B-12 or vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J. Nutr. 2002, 132, 1345–1356. [Google Scholar] [PubMed]
- Kim, H.; Kim, G.; Jang, W.; Kim, S.Y.; Chang, N. Association between intake of B vitamins and cognitive function in elderly Koreans with cognitive impairment. Nutr. J. 2014, 13, 118. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Tang, M.; Miller, J.; Green, R.; Mayeux, R. Relation of higher folate intake to lower risk of Alzheimer disease in the elderly. Arch. Neurol. 2007, 64, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.W.; Green, R.; Mungas, D.M.; Reed, B.R.; Jagust, W.J. Homocysteine, vitamin B6, and vascular disease in ad patients. Neurology 2002, 58, 1471–1475. [Google Scholar] [CrossRef] [PubMed]
- Agnew-Blais, J.C.; Wassertheil-Smoller, S.; Kang, J.H.; Hogan, P.E.; Coker, L.H.; Snetselaar, L.G.; Smoller, J.W. Folate, vitamin B6 and vitamin B12 intake and mild cognitive impairment and probable dementia in the women’s health initiative memory study. J. Acad. Nutr. Diet. 2015, 115, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.; Wengreen, H.J.; Munger, R.G.; Corcoran, C.D.; The Cache County Investigators. Dietary folate, vitamin B-12, vitamin B-6 and incident Alzheimer’s disease: The cache county memory, health, and aging study. J. Nutr. Health Aging 2009, 13, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Vercambre, M.-N.; Boutron-Ruault, M.-C.; Ritchie, K.; Clavel-Chapelon, F.; Berr, C. Long-term association of food and nutrient intakes with cognitive and functional decline: A 13-year follow-up study of elderly french women. Br. J. Nutr. 2009, 102, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Seshadri, S.; Beiser, A.; Selhub, J.; Jacques, P.F.; Rosenberg, I.H.; D’Agostino, R.B.; Wilson, P.W.F.; Wolf, P.A. Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease. N. Engl. J. Med. 2002, 346, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.J.; de Groot, L.C.; Joosten, L.W.; Bloo, R.J.; Clarke, R.; Ueland, P.M.; Schneede, J.; Blom, H.J.; Hoefnagels, W.H.; van Staveren, W.A. Effect of oral vitamin B-12 with or without folic acid on cognitive function in older people with mild vitamin B-12 deficiency: A randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 84, 361–370. [Google Scholar] [PubMed]
- Mooijaart, S.P.; Gussekloo, J.; Frölich, M.; Jolles, J.; Stott, D.J.; Westendorp, R.G.; de Craen, A.J. Homocysteine, vitamin B-12, and folic acid and the risk of cognitive decline in old age: The leiden 85-plus study. Am. J. Clin. Nutr. 2005, 82, 866–871. [Google Scholar] [PubMed]
- Kalmijn, S.; Launer, L.J.; Lindemans, J.; Bots, M.L.; Hofman, A.; Breteler, M.M.B. Total homocysteine and cognitive decline in a community-based sample of elderly subjects: The rotterdam study. Am. J. Epidemiol. 1999, 150, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Ravaglia, G.; Forti, P.; Maioli, F.; Vettori, C.; Grossi, G.; Mario Bargossi, A.; Caldarera, M.; Franceschi, C.; Facchini, A.; Mariani, E.; et al. Elevated plasma homocysteine levels in centenarians are not associated with cognitive impairment. Mech. Ageing Dev. 2001, 121, 251–261. [Google Scholar] [CrossRef]
- Guilarte, T.R. Vitamin B6 and cognitive development: Recent research findings from human and animal studies. Nutr. Rev. 1993, 51, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Wei, I.-L.; Huang, Y.-H.; Wang, G.-S. Vitamin B6 deficiency decreases the glucose utilization in cognitive brain structures of rats. J. Nutr. Biochem. 1999, 10, 525–531. [Google Scholar] [CrossRef]
- Karlsson, I. Neurotransmitter changes in aging and dementia. Nord. J. Psychiatry 1993, 47, 41–44. [Google Scholar] [CrossRef]
- Kannan, K.; Jain, S.K. Effect of vitamin B6 on oxygen radicals, mitochondrial membrane potential, and lipid peroxidation in H2O2-treated U937 monocytes. Free Radic. Biol. Med. 2004, 36, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Lai, C.-Q.; Mattei, J.; Ordovas, J.M.; Tucker, K.L. Association of vitamin B-6 status with inflammation, oxidative stress, and chronic inflammatory conditions: The boston puerto rican health study. Am. J. Clin. Nutr. 2010, 91, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Suever, B.L.; Prakash, R.S.; Colcombe, S.J.; McAuley, E.; Kramer, A.F. Greater intake of vitamins B6 and B12 spares gray matter in healthy elderly: A voxel-based morphometry study. Brain Res. 2008, 1199, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Viitanen, M.; Guo, Z.; Winblad, B.; Fratiglioni, L. Blood pressure reduction, cardiovascular diseases, and cognitive decline in the mini-mental state examination in a community population of normal very old people: A three-year follow-up. J. Clin. Epidemiol. 1998, 51, 385–391. [Google Scholar] [CrossRef]
- Lindeboom, J.; Weinstein, H. Neuropsychology of cognitive ageing, minimal cognitive impairment, Alzheimer’s disease, and vascular cognitive impairment. Eur. J. Pharmacol. 2004, 490, 83–86. [Google Scholar] [CrossRef] [PubMed]
| Participants | Reference Range | |
|---|---|---|
| Age (years) | 69.5 (7.3) | |
| Male n (%) | 60 (39) | |
| BMI (kg/m2) | 27.5 (4.2) | 20–25 |
| Smokers n (%) | 6 (4) | |
| 3rd Level Education n (%) | 48 (31) | |
| Depression n (%) * | 11 (7) | |
| Cognitive Function (MMSE) | 29.1 (1.3) | ≤25 |
| B-Vitamin Dietary Intakes † | ||
| Energy (MJ/day) | 7.621 (1.789) | 9.71 (M); 7.96 (F) |
| Total Folate (µg/day) | 303 (141) | 200 |
| Vitamin B12 (µg/day) | 4.0 (2.4) | 1.5 |
| Vitamin B6 (mg/day) | 2.3 (0.7) | 1.4 (M); 1.2 (F) |
| Riboflavin (mg/day) | 1.6 (0.4) | 1.3 (M); 1.1 (F) |
| Fortified Food Consumer n (%) ‡ | 116 (75) | |
| B-Vitamin Biomarker Status § | ||
| Red Blood Cell Folate (nmol/L) | 954 (410) | 340–2270 |
| Serum total B12 (pmol/L) | 282 (106) | 111–740 |
| Serum HoloTC (pmol/L) | 50.8 (24.3) | 40–200 |
| Serum MMA (µmol/L) | 0.24 (0.19 | ≤0.36 |
| Vitamin B6 (Plasma PLP; nmol/L) | 58.4 (25.8) | 20–121 |
| Riboflavin (EGRAC) | 1.33 (0.14) | ≤1.3 |
| Plasma total homocysteine (µmol/L) | 12.0 (3.7) | <10 |
| Initial Assessment | Follow-Up Assessment | p-Value | |
|---|---|---|---|
| Age | 69.5 (7.2) | 73.4 (7.1) | <0.001 |
| Cognitive Function Score | |||
| MMSE Total Score | 29.1 (1.3) | 27.5 (2.4) | <0.001 |
| Orientation | 9.9 (0.3) | 9.8 (0.7) | 0.014 |
| Registration | 3.0 (0.1) | 3.0 (0.1) | 0.565 |
| Attention | 4.7 (0.7) | 4.4 (1.1) | 0.004 |
| Recall | 2.7 (0.6) | 1.8 (1.0) | <0.001 |
| Total Verbal | 20.3 (1.1) | 19.0 (2.0) | <0.001 |
| Language | 8.8 (0.5) | 8.5 (0.8) | <0.001 |
| Impaired Cognition n (%) * | 0 (0) | 19 (12) |
| Range | Odds Ratio | 95% CI | p-Value | |
|---|---|---|---|---|
| Age | 1.11 | (1.05–1.16) | <0.001 | |
| Female Gender | 0.69 | (0.34–1.41) | 0.310 | |
| BMI | 1.04 | (0.95–1.13) | 0.410 | |
| Smoking | 2.82 | (0.55–14.56) | 0.216 | |
| MTHFR TT genotype | 1.82 | (0.56–5.93) | 0.318 | |
| Secondary level education | 1.37 | (0.62–3.03) | 0.434 | |
| Depression | 0.40 | (0.08–2.18) | 0.293 | |
| B-Vitamin Biomarker Status | ||||
| Low folate status (RBC Folate) * | (191–719 nmol/L) | 1.81 | (0.83–3.91) | 0.134 |
| Low vitamin B12 (serum total B12) * | (118–231 pmol/L) | 1.14 | (0.52–2.49) | 0.750 |
| Low vitamin B6 (PLP) * | (15.4–42.9 nmol/L) | 3.49 | (1.60–7.62) | 0.002 |
| Low riboflavin status (EGRAC) † | ≥1.3 | 1.01 | (0.48–2.15) | 0.972 |
| High homocysteine | (12.6–25.4 µmol/L) | 1.50 | (0.58–3.85) | 0.402 |
| B-Vitamin Dietary Intake ‡ | ||||
| Low Folate intake | (124–166 µg/day) | 2.55 | (0.78–8.41) | 0.123 |
| Low vitamin B12 intake | (1.2–1.8 µg/day) | 1.04 | (0.29–3.78) | 0.949 |
| Low vitamin B6 intake | (0.9–1.4 mg/day) | 4.08 | (1.24–13.50) | 0.021 |
| Low riboflavin intake | 0.6–1.0 mg/day) | 0.41 | (0.13–1.32) | 0.136 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, C.F.; Ward, M.; Tracey, F.; Hoey, L.; Molloy, A.M.; Pentieva, K.; McNulty, H. B-Vitamin Intake and Biomarker Status in Relation to Cognitive Decline in Healthy Older Adults in a 4-Year Follow-Up Study. Nutrients 2017, 9, 53. https://doi.org/10.3390/nu9010053
Hughes CF, Ward M, Tracey F, Hoey L, Molloy AM, Pentieva K, McNulty H. B-Vitamin Intake and Biomarker Status in Relation to Cognitive Decline in Healthy Older Adults in a 4-Year Follow-Up Study. Nutrients. 2017; 9(1):53. https://doi.org/10.3390/nu9010053
Chicago/Turabian StyleHughes, Catherine F., Mary Ward, Fergal Tracey, Leane Hoey, Anne M. Molloy, Kristina Pentieva, and Helene McNulty. 2017. "B-Vitamin Intake and Biomarker Status in Relation to Cognitive Decline in Healthy Older Adults in a 4-Year Follow-Up Study" Nutrients 9, no. 1: 53. https://doi.org/10.3390/nu9010053