Assessment of the Sustainability of the Mediterranean Diet Combined with Organic Food Consumption: An Individual Behaviour Approach

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.2.1. Socio-Demographic and Lifestyle Characteristics
2.2.2. Assessment and Treatment of Dietary Data
2.2.3. Assessment of the Cost of the Diet
2.3. Data Computation and Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Diet Quality and Dietary Diversity
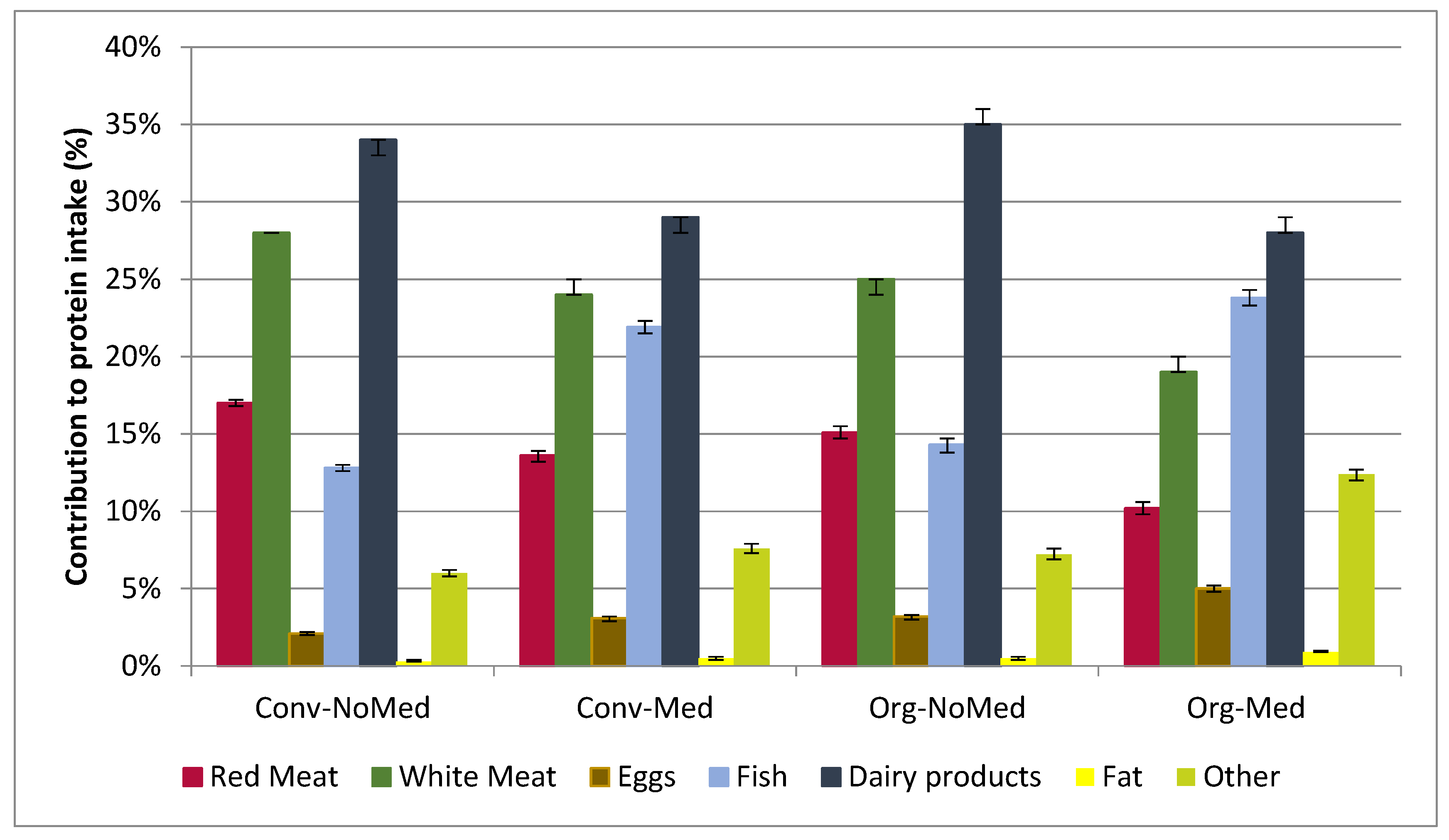
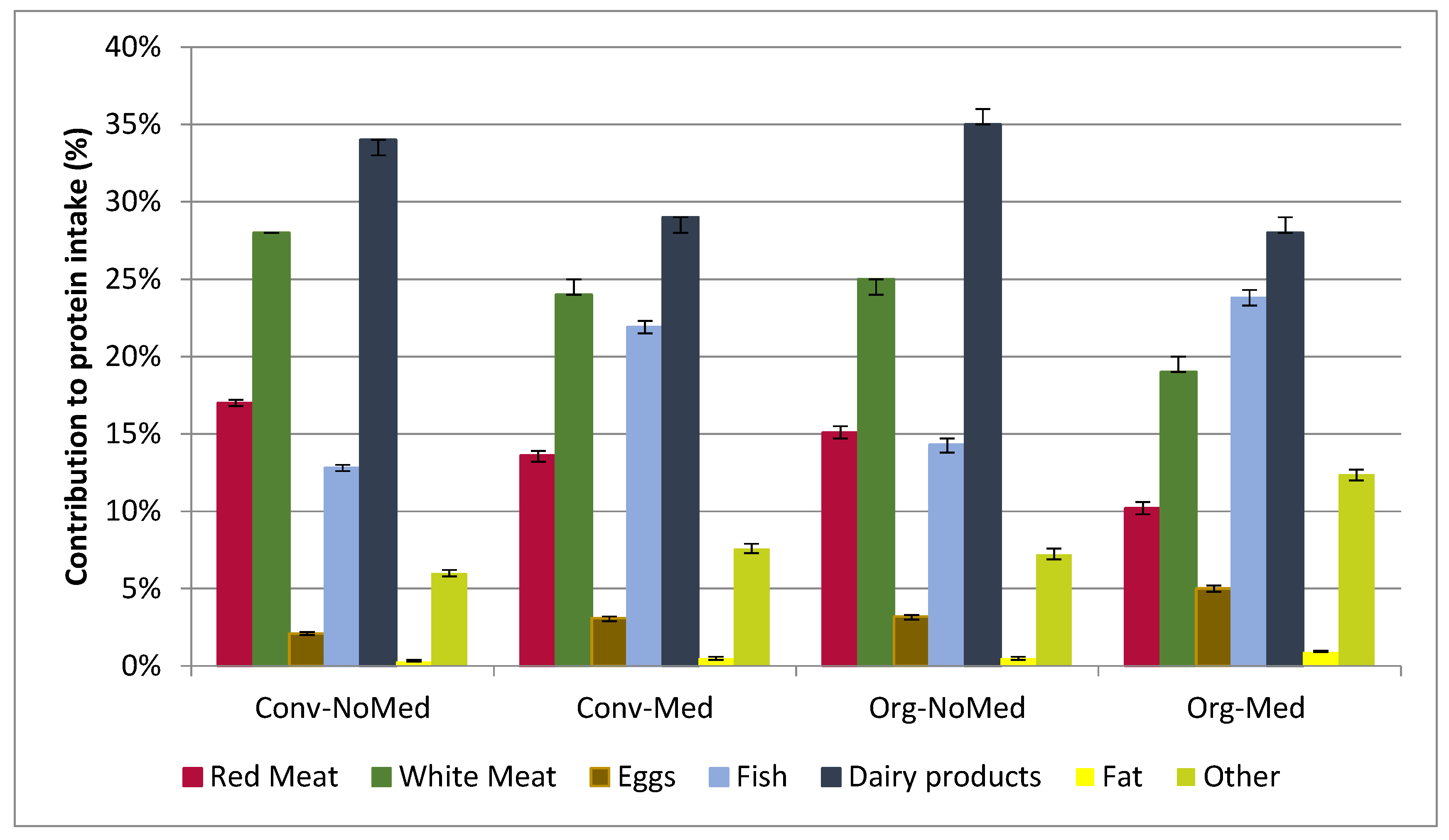
3.3. Plant and Animal Protein Source Intake as a Proxy for Environmental Impact
3.4. Economic Indicators
3.5. Diet-Related Sociocultural Indicators
4. Discussion
4.1. Nutritional Aspects
4.2. Economic Aspects
4.3. Environmental Aspects
4.4. Sociocultural Aspects
4.5. Limitations and Strengths
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Reganold, J.P.; Wachter, J.M. Organic agriculture in the twenty-first century. Nat. Plants 2016, 2, 15221. [Google Scholar] [CrossRef] [PubMed]
- Tilman, D.; Clark, M. Global diets link environmental sustainability and human health. Nature 2014, 515, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and evolution of the Western diet: Health implications for the 21st century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [PubMed]
- Tilman, D.; Clark, M. Food, Agriculture & the Environment: Can We Feed the World & Save the Earth? Daedalus 2015, 144, 8–23. [Google Scholar]
- Garnett, T. Food sustainability: Problems, perspectives and solutions. Proc. Nutr. Soc. 2013, 72, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Sustainable Diets and Biodiversity—Directions and Solutions for policy, Research and Action—i3004e.pdf. Available online: http://www.fao.org/docrep/016/i3004e/i3004e.pdf (accessed on 12 May 2016).
- Dernini, S.; Berry, E.M. Mediterranean Diet: From a healthy diet to a sustainable dietary pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Germani, A.; Vitiello, V.; Giusti, A.M.; Pinto, A.; Donini, L.M.; del Balzo, V. Environmental and economic sustainability of the Mediterranean Diet. Int. J. Food Sci. Nutr. 2014, 65, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Sáez-Almendros, S.; Obrador, B.; Bach-Faig, A.; Serra-Majem, L. Environmental footprints of Mediterranean versus Western dietary patterns: Beyond the health benefits of the Mediterranean diet. Environ. Health 2013, 12, 118. [Google Scholar] [CrossRef] [PubMed]
- León-Muñoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to the Mediterranean Diet Pattern Has Declined in Spanish Adults. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Vareiro, D.; Bach-Faig, A.; Quintana, B.R.; Bertomeu, I.; Buckland, G.; de Almeida, M.D.; Serra-Majem, L. Availability of Mediterranean and non-Mediterranean foods during the last four decades: Comparison of several geographical areas. Public Health Nutr. 2009, 12, 1667–1675. [Google Scholar] [CrossRef] [PubMed]
- Strassner, C.; Cavoski, I.; Di Cagno, R.; Kahl, J.; Kesse-Guyot, E.; Lairon, D.; Lampkin, N.; Løes, A.K.; Matt, D.; Niggli, U.; et al. How the Organic Food System Supports Sustainable Diets and Translates These into Practice. Front. Nutr. 2015, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Baudry, J.; Méjean, C.; Allès, B.; Péneau, S.; Touvier, M.; Hercberg, S.; Lairon, D.; Galan, P.; Kesse-Guyot, E. Contribution of Organic Food to the Diet in a Large Sample of French Adults (the NutriNet-Santé Cohort Study). Nutrients 2015, 7, 8615–8632. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Castetbon, K.; Czernichow, S.; Malon, A.; Mejean, C.; Kesse, E.; Touvier, M.; Galan, P. The Nutrinet-Santé Study: A web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health 2010, 10, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjorstrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Victora, C.G. Reliability and validity of the International Physical Activity Questionnaire (IPAQ). Med. Sci. Sports Exerc. 2004, 36, 556. [Google Scholar] [CrossRef] [PubMed]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Castetbon, K.; Touvier, M.; Hercberg, S.; Galan, P. Relative Validity and Reproducibility of a Food Frequency Questionnaire Designed for French Adults. Ann. Nutr. Metab. 2010, 57, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Nutrinet-Santé, E. Table de Composition des ALiments de l’Étude Nutrinet-Santé; Economica: Paris, France, 2013. [Google Scholar]
- Verger, E.O.; Mariotti, F.; Holmes, B.A.; Paineau, D.; Huneau, J.-F. Evaluation of a Diet Quality Index Based on the Probability of Adequate Nutrient Intake (PANDiet) Using National French and US Dietary Surveys. PLoS ONE 2012, 7, e42155. [Google Scholar] [CrossRef] [PubMed]
- Chauliac, M.; Razanamahefa, L.; Choma, C.; Boudot, J.; Houssin, D. National health and nutrition program: Challenges of a global action plan. Rev. Prat. 2009, 59, 10–12. [Google Scholar] [PubMed]
- Arimond, M.; Wiesmann, D.; Becquey, E.; Carriquiry, A.; Daniels, M.C.; Deitchler, M.; Fanou-Fogny, N.; Joseph, M.L.; Kennedy, G.; Martin-Prevel, Y.; et al. Simple Food Group Diversity Indicators Predict Micronutrient Adequacy of Women’s Diets in 5 Diverse, Resource-Poor Settings. J. Nutr. 2010, 140, S2059–S2069. [Google Scholar] [CrossRef] [PubMed]
- Consumer Panels—Kantar Worldpanel. Available online: http://www.kantarworldpanel.com/global/Sectors (accessed on 3 June 2016).
- Wn, S. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar]
- Carlsson-Kanyama, A.; González, A.D. Potential contributions of food consumption patterns to climate change. Am. J. Clin. Nutr. 2009, 89, S1704–S1709. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [PubMed]
- Maillot, M.; Issa, C.; Vieux, F.; Lairon, D.; Darmon, N. The shortest way to reach nutritional goals is to adopt Mediterranean food choices: Evidence from computer-generated personalized diets. Am. J. Clin. Nutr. 2011, 94, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Peneau, S.; Mejean, C.; de Edelenyi, F.S.; Galan, P.; Hercberg, S.; Lairon, D. Profiles of Organic Food Consumers in a Large Sample of French Adults: Results from the Nutrinet-Santé Cohort Study. PLoS ONE 2013, 8, e76998. [Google Scholar] [CrossRef] [PubMed]
- Eisinger-Watzl, M.; Wittig, F.; Heuer, T.; Hoffmann, I. Customers Purchasing Organic Food—Do They Live Healthier? Results of the German National Nutrition Survey II. Eur. J. Nutr. Food Saf. 2015, 5, 59–71. [Google Scholar] [CrossRef]
- Schröder, H.; Marrugat, J.; Vila, J.; Covas, M.I.; Elosua, R. Adherence to the Traditional Mediterranean Diet Is Inversely Associated with Body Mass Index and Obesity in a Spanish Population. J. Nutr. 2004, 134, 3355–3361. [Google Scholar] [PubMed]
- De Lorenzo, A.; Noce, A.; Bigioni, M.; Calabrese, V.; Della Rocca, D.G.; Daniele, N.D.; Tozzo, C.; Renzo, L.D. The Effects of Italian Mediterranean Organic Diet (IMOD) on Health Status. Curr. Pharm. Des. 2010, 16, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Macdiarmid, J.I.; Kyle, J.; Horgan, G.W.; Loe, J.; Fyfe, C.; Johnstone, A.; McNeill, G. Sustainable diets for the future: Can we contribute to reducing greenhouse gas emissions by eating a healthy diet? Am. J. Clin. Nutr. 2012, 96, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Saulle, R.; Semyonov, L.; La Torre, G. Cost and Cost-Effectiveness of the Mediterranean Diet: Results of a Systematic Review. Nutrients 2013, 5, 4566–4586. [Google Scholar] [CrossRef] [PubMed]
- Organic Agriculture: Why Is Organic Food More Expensive Than Conventional Food? Available online: http://www.fao.org/organicag/oa-faq/oa-faq5/en/ (accessed on 3 June 2016).
- Niggli, U. Sustainability of organic food production: Challenges and innovations. Proc. Nutr. Soc. 2015, 74, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Chiffres de la Bio en France en 2014—Agence Française pour le Développement et la Promotion de l’Agriculture Biologique—Agence BIO. Available online: http://www.agencebio.org/la-bio-en-france (accessed on 6 June 2016).
- Sabaté, J.; Sranacharoenpong, K.; Harwatt, H.; Wien, M.; Soret, S. The environmental cost of protein food choices. Public Health Nutr. 2015, 18, 2067–2073. [Google Scholar] [CrossRef] [PubMed]
- Berners-Lee, M.; Hoolohan, C.; Cammack, H.; Hewitt, C.N. The relative greenhouse gas impacts of realistic dietary choices. Energy Policy 2012, 43, 184–190. [Google Scholar] [CrossRef]
- Scarborough, P.; Appleby, P.N.; Mizdrak, A.; Briggs, A.D.; Travis, R.C.; Bradbury, K.E.; Key, T.J. Dietary greenhouse gas emissions of meat-eaters, fish-eaters, vegetarians and vegans in the UK. Clim. Chang. 2014, 125, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Darmon, N.; Touazi, D.; Soler, L.G. Greenhouse gas emissions of self-selected individual diets in France: Changing the diet structure or consuming less? Ecol. Econ. 2012, 75, 91–101. [Google Scholar] [CrossRef]
- Tuomisto, H.L.; Hodge, I.D.; Riordan, P.; Macdonald, D.W. Does organic farming reduce environmental impacts?—A meta-analysis of European research. J. Environ. Manag. 2012, 112, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Michaelidou, N.; Hassan, L.M. The role of health consciousness, food safety concern and ethical identity on attitudes and intentions towards organic food. Int. J. Consum. Stud. 2008, 32, 163–170. [Google Scholar] [CrossRef]
- Auestad, N.; Fulgoni, V.L. What Current Literature Tells Us about Sustainable Diets: Emerging Research Linking Dietary Patterns, Environmental Sustainability, and Economics. Adv. Nutr. Int. Rev. J. 2015, 6, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Cinquante ans de Consommation Alimentaire: Une Croissance Modérée, mais de Profonds Changements. Available online: http://www.insee.fr/fr/ffc/ipweb/ip1568/IP1568.pdf (accessed on 27 July 2016).
- Średnicka-Tober, D.; Barański, M.; Seal, C.; Sanderson, R.; Benbrook, C.; Steinshamn, H.; Gromadzka-Ostrowska, J.; Rembiałkowska, E.; Skwarło-Sońta, K.; Eyre, M.; et al. Composition differences between organic and conventional meat: A systematic literature review and meta-analysis. Br. J. Nutr. 2016, 115, 994–1011. [Google Scholar] [CrossRef] [PubMed]
- Barański, M.; Średnicka-Tober, D.; Volakakis, N.; Seal, C.; Sanderson, R.; Stewart, G.B.; Benbrook, C.; Biavati, B.; Markellou, E.; Giotis, C.; et al. Higher antioxidant and lower cadmium concentrations and lower incidence of pesticide residues in organically grown crops: A systematic literature review and meta-analyses. Br. J. Nutr. 2014, 112, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Średnicka-Tober, D.; Barański, M.; Seal, C.J.; Sanderson, R.; Benbrook, C.; Steinshamn, H.; Gromadzka-Ostrowska, J.; Rembiałkowska, E.; Skwarło-Sońta, K.; Eyre, M.; et al. Higher PUFA and n-3 PUFA, conjugated linoleic acid, α-tocopherol and iron, but lower iodine and selenium concentrations in organic milk: A systematic literature review and meta- and redundancy analyses. Br. J. Nutr. 2016, 115, 1043–1060. [Google Scholar] [CrossRef] [PubMed]
- Assessing Sustainable Diets within the Sustainability of Food Systems—A-i4806e.pdf. Available online: http://www.fao.org/3/a-i4806e.pdf (accessed on 3 June 2016).

{kind=link}
| Name of the Score | Objective | Methods/Calculation | Score Components | Scale Range |
|---|---|---|---|---|
| Diet Quality Index Based on the Probability of Adequate Nutrient Intake PANDiet [21] | Reflects the adequacy between nutrient intakes and French recommendations for 24 nutrients | PANDiet is the average of two sub-scores. The adequacy sub-score is the average of the probability of adequacy * (between 0 and 1), multiplied by 100 for nutrients for which the usual intake should be above a reference value. The moderation sub-score is the average of the probability of adequacy * (between 0 and 1) for nutrients for which the usual intake should not exceed a reference value and penalty values. | Adequacy score: protein, total carbohydrate, total fat, poly-unsaturated fatty acids, fibre, vitamins A, B1, B2, B3, B6, B9, B12, C, D, E, calcium, magnesium, zinc, phosphorus, potassium and iron. Moderation score: protein, total fat, saturated fatty acids, carbohydrate, cholesterol, and sodium Penalty: retinol, niacin, vitamin B6, C, D, E, folate, calcium, magnesium, zinc, phosphorus and iron | 0 to 100 |
| mPNNS-GS [22] | Reflects the level of adherence to the French food-based recommendation defined by the PNNS (Programme National Nutrition Santé) | mPNNS-GS is the sum of components. We did not use the physical activity component. | Fruit and vegetables (0–2), starchy foods (0–1), whole-grain (0–1), dairy products (0–1), meat (0–1), seafood (0–1), added fat (0–1), sweets (−0.5–1), water and soda (0–1), alcohol (0–1), salt (−0.5–1.5), penalty if energy intake >105% of calculated energy needs | 0 to 13.5 |
| Literature-based adherence score of Mediterranean diet [8] | Assesses the adherence to the Mediterranean diet regardless of the sample | For each food group, three levels of consumption are considered (predefined portion) and 0, 1, or 2 points were given depending on the daily consumption and the component | Fruits, vegetables, legumes, fish, starches, meat, dairy products, alcohol and olive oil | 0 to 18 |
| Dietary diversity score [23] | Evaluates the number of food groups consumed per day | The score is the sum of individual food groups consumed on average per day, among 21 food groups. A minimum portion size is required for each food group to be included in the score: 40 g for vegetables or fruits, 15 g for grains, legumes, cheese and 30 g for other foods. | Grains, cereals, legumes, tubers, vitamin A-rich vegetables, dark green leafy vegetables, vitamin C-rich vegetables, soybeans and soy products, other vegetables, vitamin A-rich fruits, vitamin C-rich fruits, others fruits, organ meat, meat, eggs, seafood, fish, insects, dairy products, cheeses and fat | 0 to 21 |
| N (%) | Conv–NoMed | Conv–Med | Org–NoMed | Org–Med | p * |
|---|---|---|---|---|---|
| N = 14,266 (62%) | N = 3498 (15%) | N = 2532 (11%) | N = 2570 (12%) | ||
| Mediterranean diet score (/18) | 7.55 (7.52–7.57) | 11.81 (11.75–11.86) | 8.39 (8.33–8.46) | 12.31 (12.25–12.38) | <0.0001 |
| Contribution (in % of weight) of organic food to the diet | 15.5 (15.3–15.8) | 22.4 (21.9–22.9) | 68.2 (67.6–68.7) | 74.6 (74.0–75.1) | <0.0001 |
| Age (years) | 52.9 (52.7–53.2) | 57.0 (56.6–57.5) | 53.8 (53.2–54.3) | 54.6 (54.1–55.2) | <0.0001 |
| Male (%) | 27.07 | 31.45 | 21.80 | 22.45 | <0.0001 |
| Educational level (%) | |||||
| <High school diploma | 22.89 | 22.38 | 20.62 | 17.55 | <0.0001 |
| High school | 15.37 | 14.89 | 13.55 | 14.55 | |
| Post-secondary graduate | 61.75 | 62.72 | 65.84 | 67.90 | |
| Monthly income per household unit (%) | |||||
| Refuse to declare | 12.15 | 12.29 | 11.89 | 11.67 | <0.0001 |
| <1200 euros | 11.21 | 9.35 | 9.12 | 10.86 | |
| 1200–1800 euros | 22.21 | 19.13 | 22.24 | 21.13 | |
| 1800–2700 euros | 25.33 | 25.44 | 26.78 | 26.50 | |
| >2700 euros | 29.09 | 33.79 | 29.98 | 29.84 | |
| Location (%) | |||||
| Rural Community | 21.61 | 19.70 | 25.24 | 24.82 | <0.0001 |
| Urban unit: population <20,000 inhabitants | 15.51 | 14.47 | 16.23 | 14.82 | |
| Urban unit: population between 20,000 and 200,000 inhabitants | 18.16 | 17.38 | 17.77 | 18.44 | |
| Urban unit: population >200,000 inhabitants | 44.73 | 48.46 | 40.76 | 41.91 | |
| Type of diet (%) | |||||
| Vegetarian diet | 0.67 | 2.23 | 2.05 | 6.85 | <0.0001 |
| Vegan diet | 0.21 | 0.77 | 1.22 | 4.75 | <0.0001 |
| Smoking status (%) | |||||
| Former smoker | 39.25 | 44.54 | 40.09 | 41.56 | <0.0001 |
| Occasional smoker | 3.38 | 2.92 | 3.59 | 2.96 | |
| Current smoker | 8.44 | 5.75 | 6.60 | 4.94 | |
| Never smoker | 48.93 | 46.80 | 49.72 | 50.54 | |
| Alcohol intake (%) | |||||
| No or low drinker | 5.05 | 4.69 | 5.96 | 7.12 | <0.0001 |
| Moderate drinker (<20 g/day for women and <30 g/day for men) | 84.33 | 89.42 | 84.99 | 88.29 | |
| High drinker | 10.62 | 5.89 | 9.04 | 4.59 | |
| Physical activity (%) | |||||
| Missing data | 11.26 | 10.38 | 9.44 | 8.91 | <0.0001 |
| Low (<30 min/day) | 21.77 | 14.35 | 17.81 | 12.76 | |
| Medium (30–60 min/day) | 36.59 | 37.54 | 37.01 | 38.05 | |
| High (>60 min/day) | 30.38 | 37.74 | 35.74 | 40.27 | |
| Conv–NoMed | Conv–Med | Org–NoMed | Org–Med | |||||
|---|---|---|---|---|---|---|---|---|
| N = 14,266 (62%) | N = 3498 (15%) | N = 2532 (11%) | N = 2570 (12%) | |||||
| PANDiet * (/100) | 63.71 a | (63.57–63.84) | 69.02 b | (68.75–69.29) | 64.72 c | (64.41–65.03) | 71.40 d | (71.09–71.71) |
| mPNNS-GS * (/13.5) | 8.19 a | (8.17–8.22) | 9.30 b | (9.24–9.35) | 8.45 c | (8.39–8.51) | 9.29 b | (9.23–9.36) |
| Dietary diversity score * (/21) | 8.73 a | (8.70–8.76) | 10.39 b | (10.33–10.45) | 9.24 c | (9.16–9.30) | 10.67 b | (10.59–10.74) |
| Energy density † (kcal/100 g) | 86.99 a | (86.61–87.36) | 84.00 b | (83.29–84.72) | 82.95 b,c | (82.11–83.79) | 82.38 c | (81.54–83.21) |
| Total energy intake † (kcal/day) | 2020 a | (2010–2031) | 2270 b | (2249–2290) | 1966 c | (1942–1990) | 2233 b | (2209–2256) |
| Total protein intake ‡ (g/day) | 94.37 a | (94.05–94.69) | 88.22 b | (87.60–88.83) | 88.90 b | (88.18–89.61) | 79.00 c | (78.29–79.72) |
| Protein intake *,§ (%) | 19.61 a | (19.54–19.67) | 18.17 b | (18.05–18.29) | 18.27 b | (18.13–18.41) | 16.43 c | (16.29–16.57) |
| Animal Protein intake ‡ (g/day) | 69.20 a | (68.84–69.57) | 55.32 b | (54.61–56.03) | 60.29 c | (59.46–61.11) | 39.01 d | (38.18–39.83) |
| Plant Protein intake ‡ (g/day) | 25.17 a | (25.03–25.31) | 32.89 b | (32.62–33.16) | 28.61 c | (28.29–28.92) | 40.00 d | (39.68–40.31) |
| Plant/Animal protein intake ratio ‡ | 0.44 a | (0.28–0.60) | 0.66 a | (0.35–0.98) | 0.57 a | (0.20–0.93) | 1.38 b | (1.01–1.74) |
| Body mass index (BMI) * (kg/m2) | 24.89 a | (24.81–24.96) | 24.11 b | (23.96–24.26) | 24.09 b | (23.92–24.27) | 22.90 c | (22.72–23.08) |
| Conv–NoMed | Conv–Med | Org–NoMed | Org–Med | |||||
|---|---|---|---|---|---|---|---|---|
| N = 14,266 (62%) | N = 3498 (15%) | N = 2532 (11%) | N = 2570 (12%) | |||||
| Cost of the diet * (€/day) | 8.59 a | (8.55–8.63) | 9.11 b | (9.03–9.19) | 10.90 c | (10.81–10.98) | 11.43 d | (11.34–11.52) |
| Total organic energy intake † (kcal/day) | 311 a | (304–318) | 526 b | (513–539) | 1186 c | (1171–1202) | 1566 d | (1551–1582) |
| Cost of the intake for 100 organic calories †,‡ (€) | 0.58 a | (0.56–0.59) | 0.56 a | (0.54–0.58) | 0.58 a | (0.55–0.60) | 0.55 a | (0.53–0.58) |
| Cost of the intake for 100 conventional calories †,§ (€) | 0.37 a | (0.36–0.37) | 0.39 b | (0.38–0.40) | 0.45 c | (0.44–0.45) | 0.54 d | (0.53–0.55) |
| Portion of the total budget allocated to food || (%) | 19.3 a | (19.1–19.5) | 22.0 b | (21.7–22.3) | 23.4 c | (23.0–23.7) | 26.4 d | (26.0–26.8) |
| Purchase Motivations | Conv–NoMed | Conv–Med | Org–NoMed | Org–Med | ||||
|---|---|---|---|---|---|---|---|---|
| N = 14,266 (62%) | N = 3498 (15%) | N = 2532 (11%) | N = 2570 (12%) | |||||
| Seasonality | ||||||||
| Marginal factor (%) | 5.2 a | (4.6–5.9) | 3.6 b | (2.8–4.4) | 1.3 c | (0.8–1.9) | 1.2 c | (0.7–1.8) |
| Medium factor (%) | 13.8 a | (12.8–14.8) | 11.3 b | (10.0–12.7) | 5.4 c | (4.3–6.4) | 4.2 c | (3.3–5.0) |
| Major factor (%) | 81.0 a | (79.8–82.1) | 85.1 b | (83.6–86.6) | 93.3 c | (92.2–94.5) | 94.6 c | (93.6–95.6) |
| Product origin | ||||||||
| Marginal factor (%) | 7.9 a | (7.1–8.7) | 6.0 b | (5.0–7.0) | 1.5 c | (1.0–2.1) | 0.9 c | (0.5–1.3) |
| Medium factor (%) | 24.0 a | (22.8–25.3) | 21.2 b | (19.5–23) | 7.4 c | (6.3–8.6) | 9.0 c | (7.7–10.2) |
| Major factor (%) | 68.1 a | (66.7–69.5) | 72.7 b | (70.9–74.6) | 91.0 c | (89.8–92.3) | 90.2 c | (88.8–91.5) |
| Production methods | ||||||||
| Marginal factor (%) | 22.2 a | (20.9–23.4) | 13.8 b | (12.4–15.2) | 1.1 c | (0.6–1.5) | 0.2 d | (0.0–0.4) |
| Medium factor (%) | 39.9 a | (38.4–41.3) | 34.1 b | (32.2–36.1) | 7.9 c | (6.8–9.1) | 4.0 d | (3.2–4.7) |
| Major factor (%) | 38.0 a | (36.5–39.4) | 52.1 b | (49.9–54.2) | 91.0 c | (89.8–92.2) | 95.8 d | (95.0–96.6) |
| Ethical production | ||||||||
| Marginal factor (%) | 23.8 a | (22.4–25.1) | 15.7 b | (14.2–17.2) | 3.1 c | (2.4–3.9) | 2.2 d | (1.6–2.8) |
| Medium factor (%) | 42.5 a | (41–43.9) | 39.9 b | (37.9–42.0) | 18.3 c | (16.5–20.0) | 13. d | (11.9–14.9) |
| Major factor (%) | 33.8 a | (32.4–35.1) | 44.3 b | (42.3–46.4) | 78.6 c | (76.8–80.5) | 84.4 d | (82.8–86.0) |
| Direct contact with producers | ||||||||
| Marginal factor (%) | 27.0 a | (25.6–28.3) | 24.0 b | (22.2–25.8) | 13.4 c | (12.0–14.9) | 12.5 c | (11.1–13.9) |
| Medium factor (%) | 34.8 a | (33.5–36.2) | 33.6 b | (31.7–35.6) | 29.6 c | (27.6–31.7) | 29.1 c | (27.0–31.2) |
| Major factor (%) | 38.2 a | (36.8–39.6) | 42.4 b | (40.3–44.4) | 56.9 c | (54.6–59.2) | 58.4 c | (56.1–60.7) |
| Regional product | ||||||||
| Marginal factor (%) | 25.0 a | (23.7–26.3) | 22.5 b | (20.7–24.2) | 13.3 c | (11.9–14.8) | 14.0 c | (12.5–15.5) |
| Medium factor (%) | 34.9 a | (33.5–36.2) | 33.7 b | (31.7–35.6) | 28.4 c | (26.3–30.4) | 28.6 c | (26.5–30.6) |
| Major factor (%) | 40.1 a | (38.7–41.5) | 43.9 b | (41.8–45.9) | 58.3 c | (56.0–60.6) | 57.4 c | (55.1–59.7) |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seconda, L.; Baudry, J.; Allès, B.; Hamza, O.; Boizot-Szantai, C.; Soler, L.-G.; Galan, P.; Hercberg, S.; Lairon, D.; Kesse-Guyot, E. Assessment of the Sustainability of the Mediterranean Diet Combined with Organic Food Consumption: An Individual Behaviour Approach. Nutrients 2017, 9, 61. https://doi.org/10.3390/nu9010061
Seconda L, Baudry J, Allès B, Hamza O, Boizot-Szantai C, Soler L-G, Galan P, Hercberg S, Lairon D, Kesse-Guyot E. Assessment of the Sustainability of the Mediterranean Diet Combined with Organic Food Consumption: An Individual Behaviour Approach. Nutrients. 2017; 9(1):61. https://doi.org/10.3390/nu9010061
Chicago/Turabian StyleSeconda, Louise, Julia Baudry, Benjamin Allès, Oualid Hamza, Christine Boizot-Szantai, Louis-Georges Soler, Pilar Galan, Serge Hercberg, Denis Lairon, and Emmanuelle Kesse-Guyot. 2017. "Assessment of the Sustainability of the Mediterranean Diet Combined with Organic Food Consumption: An Individual Behaviour Approach" Nutrients 9, no. 1: 61. https://doi.org/10.3390/nu9010061