Relative Validity and Reproducibility of a Food Frequency Questionnaire for Assessing Dietary Intakes in a Multi-Ethnic Asian Population Using 24-h Dietary Recalls and Biomarkers

Abstract
:1. Introduction
2. Materials and Methods
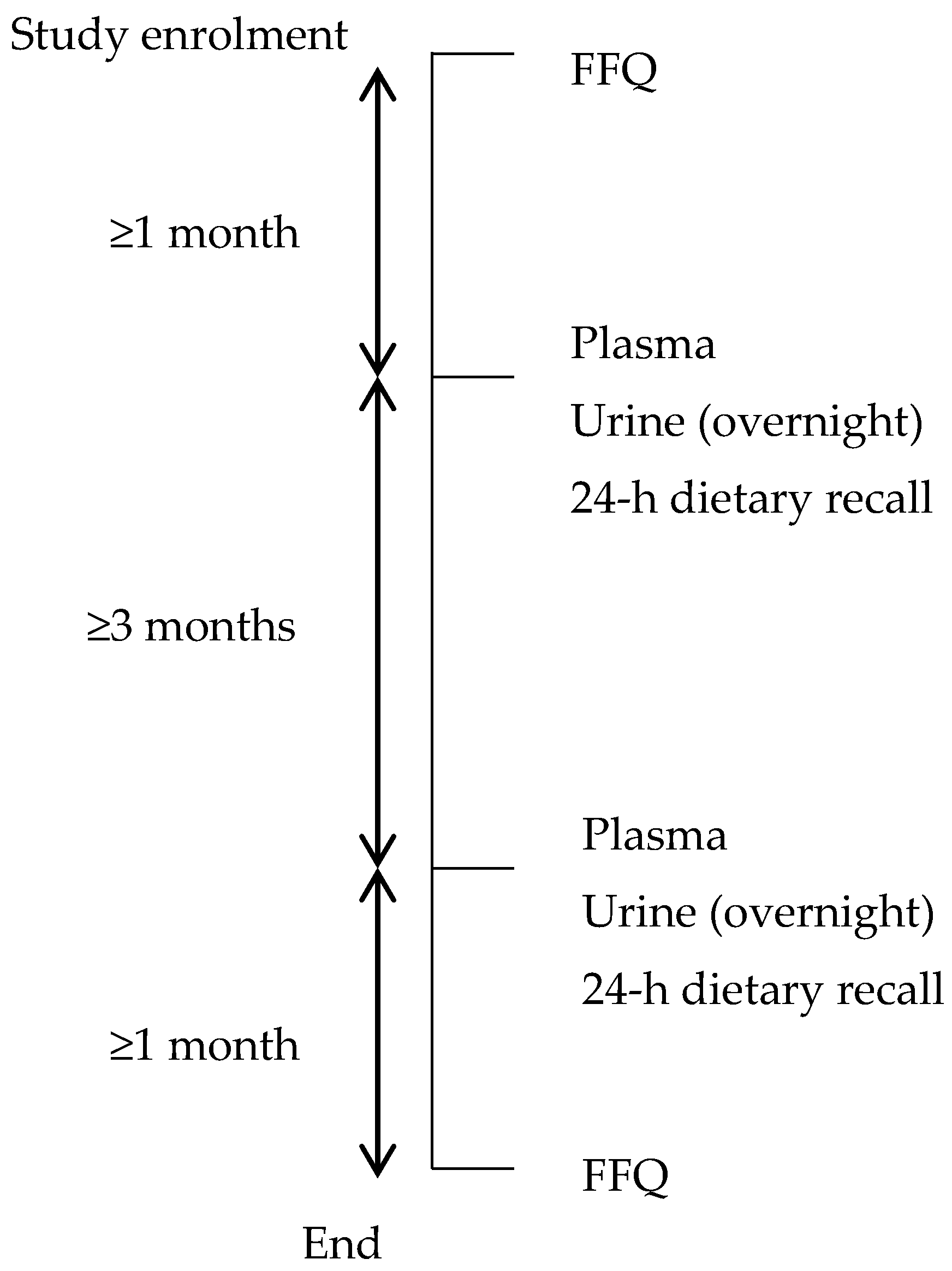
2.1. Participants and Study Design
2.2. Food Frequency Questionnaire
2.3. 24-h Dietary Recall
2.4. Biological Samples
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organisation. Global Status Report on Noncommunicable Diseases 2014; World Health Organisation: Geneva, Switzerland, 2014. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Baker, P.; Friel, S. Food systems transformations, ultra-processed food markets and the nutrition transition in Asia. Global. Health 2016, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- McKay, J. Food industry and economic development in the Asia Pacific. Asia Pac. J. Clin. Nutr. 2007, 16 (Suppl. 1), 80–84. [Google Scholar] [PubMed]
- Department of Statistics Singapore. Singapore in Figures 2016; Department of Statistics Singapore: Singapore, 2016.
- Health Promotion Board; Strategic Planning Division. Report of the National Nutrition Survey; Health Promotion Board: Singapore, 2010.
- Deurenberg-Yap, M.; Li, T.; Tan, W.L.; van Staveren, W.A.; Deurenberg, P. Validation of a semiquantitative food frequency questionnaire for estimation of intakes of energy, fats and cholesterol among Singaporeans. Asia Pac. J. Clin. Nutr. 2000, 9, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Fatihah, F.; Ng, B.K.; Hazwanie, H.; Karim Norimah, A.; Shanita, S.N.; Ruzita, A.T.; Poh, B.K. Development and validation of a food frequency questionnaire for dietary intake assessment among multi-ethnic primary school-aged children. Singap. Med. J. 2015, 56, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Jayawardena, R.; Swaminathan, S.; Byrne, N.M.; Soares, M.J.; Katulanda, P.; Hills, A.P. Development of a food frequency questionnaire for Sri Lankan adults. Nutr. J. 2012, 11, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neelakantan, N.; Whitton, C.; Seah, S.; Koh, H.; Rebello, S.A.; Lim, J.Y.; Chen, S.; Chan, M.F.; Chew, L.; Van Dam, R.M. Development of a semi-quantitative food frequency questionnaire to assess the dietary intake of a multi-ethnic urban Asian population. Nutrients 2016, 8, 528. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- Health Promotion Board. Energy and Nutrient Composition of Food. Available online: https://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 1 August 2017).
- Lee, B.L.; Ong, C.N. Comprehensive high-performance liquid chromatographic method for the measurements of lipophilic antioxidants in human plasma. J. Chromatogr. A 2009, 1216, 3131–3137. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.-J.; Ho, W.E.; Xu, F.; Wen, T.; Ong, C.N. Exploratory investigation reveals parallel alteration of plasma fatty acids and eicosanoids in coronary artery disease patients. Prostaglandins Other Lipid Mediat. 2013, 106, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.L.; Rybak, M.E.; Pfeiffer, C. Phytoestrogen biomonitoring: An extractionless LC-MS/MS method for measuring urinary isoflavones and lignans by use of atmospheric pressure photoionization (APPI). Anal. Bioanal. Chem. 2012, 402, 1123–1136. [Google Scholar] [CrossRef] [PubMed]
- Snedecor, G.; Cochran, W. Statistical Methods, 8th ed.; Iowa State University Press: Ames, IA, USA, 1989. [Google Scholar]
- Wolk, A.; Vessby, B.; Ljung, H.; Barrefors, P. Evaluation of a biological marker of dairy fat intake. Am. J. Clin. Nutr. 1998, 68, 291–295. [Google Scholar] [PubMed]
- Chung, H.; Nettleton, J.A.; Lemaitre, R.N.; Barr, R.G.; Tsai, M.Y.; Tracy, R.P.; Siscovick, D.S. Frequency and Type of Seafood Consumed Influence Plasma (n-3) Fatty Acid Concentrations. J. Nutr. 2008, 138, 2422–2427. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B.; Willett, W.C. Interval estimates for correlation coefficients corrected for within-person variation: Implications for study design and hypothesis testing. Am. J. Epidemiol. 1988, 127, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, M.; Yuan, Z.; Lin, L.; Hu, B.; Wang, X.; Yang, Y.; Chen, X.; Jin, L.; Lu, M.; Ye, W. Reproducibility and relative validity of a food frequency questionnaire developed for adults in Taizhou, China. PLoS ONE 2012, 7, e48341. [Google Scholar] [CrossRef] [PubMed]
- Ibiebele, T.I.; Parekh, S.; Mallitt, K.-A.; Hughes, M.C.; O’Rourke, P.K.; Webb, P.M. Reproducibility of food and nutrient intake estimates using a semi-quantitative FFQ in Australian adults. Public Health Nutr. 2009, 12, 2359–2365. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Hong, X.; Wang, Z.; Yang, H.; Chen, X.; Zhou, H.; Wang, C.; Lai, Y.; Sun, L.; Xu, F. Reproducibility and validity of an FFQ developed for adults in Nanjing, China. Br. J. Nutr. 2016, 115, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, E.C.K.; Zainudin, S.B.; Loh, W.N.; Chua, C.L.; Fun, S.; Subramaniam, T.; Sum, C.F.; Lim, S.C. Fasting during Ramadan and associated changes in glycaemia, caloric intake and body composition with gender differences in Singapore. Ann. Acad. Med. Singap. 2015, 44, 202–206. [Google Scholar] [PubMed]
- Messina, M.; Nagata, C.; Wu, A.H. Estimated Asian Adult Soy Protein and Isoflavone Intakes. Nutr. Cancer 2006, 55, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-A.; Wen, W.; Xiang, Y.-B.; Barnes, S.; Liu, D.; Cai, Q.; Zheng, W.; Shu, X. Assessment of Dietary Isoflavone Intake among Middle-Aged Chinese Men. J. Nutr. 2007, 137, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Sobue, T.; Sasaki, S.; Kobayashi, M.; Arai, Y.; Uehara, M.; Adlercreutz, H.; Watanabe, S.; Takahashi, T.; Iitoi, Y.; et al. Validity and reproducibility of a self-administered food-frequency questionnaire to assess isoflavone intake in a Japanese population in comparison with dietary records and blood and urine isoflavones. J. Nutr. 2001, 131, 2741–2747. [Google Scholar] [PubMed]
- Setchell, K.; Cole, S. Variations in Isoflavone Levels in Soy Foods and Soy Protein Isolates and Issues Related to Isoflavone Databases and Food Labeling. J. Agric. Food Chem. 2003, 51, 4146–4155. [Google Scholar] [CrossRef] [PubMed]
- Jaceldo-Siegl, K.; Fraser, G.E.; Chan, J.; Franke, A.; Sabaté, J. Validation of soy protein estimates from a food-frequency questionnaire with repeated 24-h recalls and isoflavonoid excretion in overnight urine in a Western population with a wide range of soy intakes. Am. J. Clin. Nutr. 2008, 87, 1422–1427. [Google Scholar] [PubMed]
- Frankenfeld, C.L.; Patterson, R.E.; Horner, N.K.; Neuhouser, M.L.; Skor, H.E.; Kalhorn, T.F.; Howald, W.N.; Lampe, J.W. Validation of a soy food-frequency questionnaire and evaluation of correlates of plasma isoflavone concentrations in postmenopausal women. Am. J. Clin. Nutr. 2003, 77, 674–680. [Google Scholar] [PubMed]
- Fraser, G.E.; Jaceldo-Siegl, K.; Henning, S.M.; Fan, J.; Knutsen, S.F.; Haddad, E.H.; Sabaté, J.; Beeson, W.L.; Bennett, H. Biomarkers of Dietary Intake Are Correlated with Corresponding Measures from Repeated Dietary Recalls and Food-Frequency Questionnaires in the Adventist Health Study-2. J. Nutr. 2016, 146, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Maskarinec, G.; Singh, S.; Meng, L.; Franke, A.A. Dietary soy intake and urinary isoflavone excretion among women from a multiethnic population. Cancer Epidemiol. Biomarkers Prev. 1998, 7, 613–619. [Google Scholar] [PubMed]
- Sluik, D.; Geelen, A.; de Vries, J.H.M.; Eussen, S.J.P.M.; Brants, H.A.M.; Meijboom, S.; van Dongen, M.C.J.M.; Bueno-de-Mesquita, H.B.; Wijckmans-Duysens, N.E.G.; van’t Veer, P.; et al. A national FFQ for the Netherlands (the FFQ-NL 1.0): Validation of a comprehensive FFQ for adults. Br. J. Nutr. 2016, 116, 913–923. [Google Scholar] [CrossRef] [PubMed]
- Brevik, A.; Veierød, M.; Drevon, C.; Andersen, L. Evaluation of the odd fatty acids 15:0 and 17:0 in serum and adipose tissue as markers of intake of milk and dairy fat. Eur. J. Clin. Nutr. 2005, 59, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ma, J.; Campos, H.; Hu, F.B. Plasma and erythrocyte biomarkers of dairy fat intake and risk of ischemic heart disease. Am. J. Clin. Nutr. 2007, 86, 929–937. [Google Scholar] [PubMed]
- Resnicow, K.; Odom, E.; Wang, T.; Dudley, W.N.; Mitchell, D.; Vaughan, R.; Jackson, A.; Baranowski, T. Validation of three food frequency questionnaires and 24-h recalls with serum carotenoid levels in a sample of African-American adults. Am. J. Epidemiol. 2000, 152, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Marks, G.C.; Gaffney, P.; Williams, G.; Green, A. Validation of a food-frequency questionnaire assessment of carotenoid and vitamin E intake using weighed food records and plasma biomarkers: The method of triads model. Eur. J. Clin. Nutr. 2005, 59, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.H.; Huang, H.-Y.; Chen, K.-J.; Wu, Y.-R.; Chiu, J.P.; Li, Y.-H.; Chiu, B.C.-H.; Lin, C.-L.; Lin, M.-N. Relative validity and reproducibility of a quantitative FFQ for assessing nutrient intakes of vegetarians in Taiwan. Public Health Nutr. 2014, 17, 1459–1466. [Google Scholar] [CrossRef] [PubMed]
- Mayer-Davis, E.J.; Vitolins, M.Z.; Carmichael, S.L.; Hemphill, S.; Tsaroucha, G.; Rushing, J.; Levin, S. Validity and reproducibility of a food frequency interview in a Multi-Cultural Epidemiology Study. Ann. Epidemiol. 1999, 9, 314–324. [Google Scholar] [CrossRef]
- Molag, M.L.; De Vries, J.H.M.; Ocké, M.C.; Dagnelie, P.C.; Van Den Brandt, P.A.; Jansen, M.C.J.F.; Van Staveren, W.A.; Van’t Veer, P. Design characteristics of food frequency questionnaires in relation to their validity. Am. J. Epidemiol. 2007, 166, 1468–1478. [Google Scholar] [CrossRef] [PubMed]
- Tjonneland, A.; Haraldsdómr, J.; Overvad, K.; Stripp, C.; Ewertz, M.; Jensen, O.M. Influence of individually estimated portion size data on the validity of a semiquantitative food frequency questionnaire. Int. J. Epidemiol. 1992, 21, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Thompson, F.E.; Kipnis, V.; Midthune, D.; Hurwitz, P.; Mcnutt, S. Comparative Validation of the Block, Willett, and National Cancer Institute The Eating at America’s Table Study. Am. J. Epidemiol. 2001, 154, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Giovannucci, E.L.; Ascherio, A.; Rimm, E.B.; Forman, M.R.; Sampson, L.; Willett, W.C. Associations of plasma carotenoid concentrations and dietary intake of specific carotenoids in samples of two prospective cohort studies using a new carotenoid database. Cancer Epidemiol. Biomakers Prev. 1998, 7, 283–290. [Google Scholar]
- Stryker, W.S.; Kaplan, L.A.; Stein, E.A.; Stampfer, M.J.; Sober, A.; Willett, W.C. The relation of diet, cigarette smoking, and alcohol consumption to plasma beta-carotene and alpha-tocopherol levels. Am. J. Epidemiol. 1988, 127, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Vioque, J.; Weinbrenner, T.; Asensio, L.; Castelló, A.; Young, I.S.; Fletcher, A. Plasma concentrations of carotenoids and vitamin C are better correlated with dietary intake in normal weight than overweight and obese elderly subjects. Br. J. Nutr. 2007, 97, 977–986. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total | Chinese | Malay | Indian | |
|---|---|---|---|---|---|
| n = 161 | n = 59 | n = 46 | n = 56 | p | |
| Age (years) | 44 ± 14 | 44 ± 16 | 43 ± 13 | 43 ± 14 | 0.9 |
| Sex (% male) | 50% | 51% | 50% | 50% | 0.995 |
| Housing type | 0.945 | ||||
| 1–3 room government flat | 39% | 39% | 37% | 39% | |
| 4–5 room government flat | 58% | 56% | 61% | 57% | |
| Private flat or landed property | 4% | 5% | 2% | 4% | |
| Monthly household income (S$) | 0.052 | ||||
| <2000 | 20% | 21% | 20% | 17% | |
| 2000–3999 | 32% | 25% | 43% | 30% | |
| 4000–5999 | 17% | 17% | 10% | 24% | |
| 6000–9999 | 20% | 15% | 28% | 17% | |
| ≥10,000 | 12% | 21% | 0% | 11% | |
| Highest educational attainment | 0.019 | ||||
| Primary or below | 11% | 15% | 11% | 7% | |
| Secondary | 11% | 8% | 11% | 14% | |
| Higher education inc. vocational | 53% | 44% | 71% | 46% | |
| University | 25% | 32% | 7% | 32% | |
| Carotenoid supplement user | 16% | 14% | 24% | 11% | 0.163 |
| Phytoestrogen supplement user | 15% | 14% | 24% | 9% | 0.1 |
| Biomarker concentrations | |||||
| Isoflavones (μg/gUCr) | 599 ± 868 | 757 ± 925 | 518 ± 1040 | 500 ± 601 | 0.036 |
| Total carotenoids (mg/L plasma) | 1.48 ± 0.43 | 1.66 ± 0.54 | 1.41 ± 0.34 | 1.35 ± 0.27 | 0.001 |
| Plasma EPA + DHA (% total FA) | 2.08 ± 0.98 | 2.33 ± 1.03 | 2.12 ± 1.09 | 1.78 ± 0.74 | 0.002 |
| Plasma PUFA (% total FA) | 56 ± 4 | 56 ± 4 | 55 ± 4 | 56 ± 5 | 0.2 |
| Plasma odd chain SFA (% total FA) | 0.16 ± 0.04 | 0.16 ± 0.04 | 0.14 ± 0.03 | 0.17 ± 0.04 | 0.005 |
| Food and nutrient intakes 1 | |||||
| Protein (%E) | 14 ± 2 | 16 ± 2 | 14 ± 2 | 13 ± 2 | <0.001 |
| Carbohydrate (%E) | 50 ± 6 | 46 ± 7 | 50 ± 5 | 53 ± 5 | <0.001 |
| Total fat (%E) | 35 ± 5 | 35 ± 5 | 36 ± 4 | 33 ± 5 | 0.02 |
| Saturated fat (%E) | 13 ± 3 | 13 ± 2 | 14 ± 2 | 13 ± 3 | 0.004 |
| Monounsaturated fat (%E) | 13 ± 3 | 14 ± 3 | 13 ± 2 | 13 ± 3 | 0.049 |
| Polyunsaturated fat (%E) | 6 ± 2 | 7 ± 2 | 6 ± 2 | 6 ± 2 | 0.2 |
| Sugar (g/1000 kcal) | 38 ± 10 | 35 ± 10 | 41 ± 10 | 40 ± 11 | 0.005 |
| Fibre (g/1000 kcal) | 9 ± 2 | 9 ± 2 | 8 ± 1 | 10 ± 2 | <0.001 |
| Vitamin A (RE, mcg/1000 kcal) | 358 ± 93 | 371 ± 108 | 347 ± 64 | 355 ± 94 | 0.7 |
| Vitamin C (mg/1000 kcal) | 51 ± 21 | 54 ± 24 | 48 ± 16 | 51 ± 21 | 0.7 |
| Calcium (mg/1000 kcal) | 305 ± 86 | 296 ± 76 | 288 ± 69 | 327 ± 103 | 0.07 |
| Iron (mg/1000 kcal) | 6.9 ± 1.2 | 7.1 ± 1.2 | 6.6 ± 1.2 | 7.0 ± 1.2 | 0.041 |
| Energy (kcal/day) | 2679 ± 1036 | 2609 ± 1006 | 2883 ± 1201 | 2586 ± 911 | 0.4 |
| Fruit (inc. 100% fruit juice) (g/day) | 161 ± 101 | 174 ± 114 | 143 ± 84 | 163 ± 100 | 0.4 |
| Vegetables (g/day) | 83 ± 54 | 101 ± 65 | 71 ± 41 | 74 ± 45 | 0.004 |
| Dairy fat (g/day) | 5 ± 5 | 4 ± 4 | 7 ± 6 | 6 ± 4 | 0.001 |
| Soy protein (g/day) | 3 ± 3 | 3 ± 2 | 3 ± 3 | 3 ± 3 | 0.1 |
| Fish/seafood (g/day) | 41 ± 31 | 47 ± 31 | 54 ± 34 | 25 ± 18 | <0.001 |
| Nutrient/Food | Total | Chinese | Malay | Indian |
|---|---|---|---|---|
| n = 161 | n = 59 | n = 46 | n = 56 | |
| Energy (kcal/day) | 0.78 (0.69, 0.85) | 0.83 (0.71, 0.90) | 0.72 (0.44, 0.85) | 0.80 (0.62, 0.89) |
| Protein (%E) | 0.78 (0.70, 0.84) | 0.73 (0.55, 0.84) | 0.62 (0.31, 0.79) | 0.62 (0.35, 0.78) |
| Total fat (%E) | 0.70 (0.59, 0.78) | 0.73 (0.54, 0.84) | 0.70 (0.45, 0.83) | 0.65 (0.40, 0.79) |
| Saturated fat (%E) | 0.77 (0.69, 0.83) | 0.68 (0.46, 0.81) | 0.78 (0.60, 0.88) | 0.80 (0.65, 0.88) |
| Monounsaturated fat (%E) | 0.69 (0.58, 0.78) | 0.71 (0.51, 0.82) | 0.72 (0.49, 0.84) | 0.66 (0.42, 0.80) |
| Polyunsaturated fat (%E) | 0.77 (0.68, 0.83) | 0.73 (0.55, 0.84) | 0.81 (0.65, 0.89) | 0.77 (0.61, 0.86) |
| Carbohydrate (%E) | 0.74 (0.65, 0.81) | 0.66 (0.43, 0.80) | 0.76 (0.56, 0.87) | 0.68 (0.46, 0.81) |
| Sugar (g/1000 kcal) | 0.70 (0.59, 0.78) | 0.74 (0.57, 0.85) | 0.65 (0.37, 0.81) | 0.62 (0.36, 0.78) |
| Fiber (g/1000 kcal) | 0.85 (0.79, 0.89) | 0.82 (0.71, 0.90) | 0.72 (0.50, 0.85) | 0.87 (0.79, 0.93) |
| Vitamin A (mcg/1000 kcal) | 0.67 (0.55, 0.76) | 0.79 (0.65, 0.88) | 0.35 (−0.16, 0.63) | 0.64 (0.38, 0.79) |
| Vitamin C (mg/1000 kcal) | 0.66 (0.53, 0.75) | 0.76 (0.59, 0.86) | 0.37 (−0.12, 0.64) | 0.69 (0.47, 0.82) |
| Calcium (mg/1000 kcal) | 0.75 (0.66, 0.82) | 0.77 (0.62, 0.86) | 0.64 (0.36, 0.80) | 0.78 (0.62, 0.87) |
| Iron (mg/1000 kcal) | 0.75 (0.66, 0.82) | 0.70 (0.50, 0.82) | 0.74 (0.52, 0.85) | 0.79 (0.65, 0.88) |
| Fruit (inc 100% fruit juice) (g/day) | 0.62 (0.47, 0.72) | 0.86 (0.77, 0.92) | 0.22 (−0.43, 0.57) | 0.52 (0.18, 0.72) |
| Vegetables (g/day) | 0.62 (0.48, 0.72) | 0.51 (0.19, 0.71) | 0.64 (0.35, 0.80) | 0.68 (0.46, 0.81) |
| Dairy fat (g/day) | 0.83 (0.76, 0.87) | 0.85 (0.75, 0.91) | 0.74 (0.52, 0.85) | 0.85 (0.74, 0.91) |
| Soy protein (g/day) | 0.71 (0.61, 0.79) | 0.70 (0.49, 0.82) | 0.79 (0.62, 0.88) | 0.64 (0.38, 0.79) |
| Fish/seafood (g/day) | 0.80 (0.73, 0.86) | 0.87 (0.77, 0.92) | 0.66 (0.40, 0.81) | 0.77 (0.60, 0.86) |
| Nutrient | FFQ1 | FFQ2 | ||||
|---|---|---|---|---|---|---|
| Crude | Adjusted 1 | Deatt. 2 | Crude | Adjusted 1 | Deatt. 2 | |
| Protein (%E) | 0.39 | 0.33 | 0.53 * | 0.36 | 0.28 | 0.45 * |
| Total fat (%E) | 0.30 | 0.26 | 0.35 * | 0.33 | 0.30 | 0.39 * |
| Saturated fat (%E) | 0.35 | 0.33 | 0.48 * | 0.27 | 0.26 | 0.38 * |
| Monounsaturated fat (%E) | 0.28 | 0.24 | 0.39 * | 0.23 | 0.20 | 0.32 * |
| Polyunsaturated fat (%E) | 0.04 | 0.04 | 0.09 | 0.16 | 0.15 | 0.31 |
| Carbohydrate (%E) | 0.28 | 0.19 | 0.25 * | 0.25 | 0.15 | 0.20 |
| Sugar (g/1000 kcal) | 0.33 | 0.31 | 0.39 * | 0.32 | 0.30 | 0.39 * |
| Fiber (g/1000 kcal) | 0.47 | 0.41 | 0.49 * | 0.51 | 0.47 | 0.56 * |
| Vitamin A (mcg/1000 kcal) | 0.11 | 0.21 | 0.40 * | 0.10 | 0.17 | 0.32 * |
| Vitamin C (mg/1000 kcal) | 0.36 | 0.37 | 0.50 * | 0.31 | 0.32 | 0.43 * |
| Calcium (mg/1000 kcal) | 0.40 | 0.38 | 0.68 * | 0.34 | 0.32 | 0.57 * |
| Iron (mg/1000 kcal) | 0.36 | 0.33 | 0.50 * | 0.43 | 0.41 | 0.64 * |
| Energy (kcal/day) | 0.15 | 0.03 | 0.04 | 0.11 | 0.02 | 0.02 |
| Biomarker and FFQ Measurement | FFQ1 | FFQ2 | ||||
|---|---|---|---|---|---|---|
| Crude | Adjusted 1 | Deatt. 2 | Crude | Adjusted 1 | Deatt. 2 | |
| Isoflavones (μg/gUCr) | ||||||
| Soy protein (g/day) 3 | 0.21 | 0.20 | 0.27 * | 0.31 | 0.32 | 0.46 * |
| Total carotenoids (mg/L plasma) | ||||||
| Fruit (inc 100% fruit juice) (g/day) 4 | 0.12 | 0.14 | 0.15 | 0.29 | 0.30 | 0.31 * |
| Vegetables (g/day) 4 | 0.25 | 0.18 | 0.19 * | 0.20 | 0.21 | 0.22 * |
| Total fruit and vegetables (g/day) 4 | 0.20 | 0.19 | 0.20 * | 0.31 | 0.33 | 0.34 * |
| Plasma EPA + DHA (% total FA) | ||||||
| Fish/seafood (g/day) | 0.47 | 0.48 | 0.51 * | 0.34 | 0.35 | 0.36 * |
| Plasma polyunsaturated FA (% total FA) | ||||||
| Polyunsaturated fat (%E) | 0.12 | 0.14 | 0.15 | 0.14 | 0.12 | 0.12 |
| Plasma odd chain saturated FA (% total FA) | ||||||
| Dairy fat (g/day) | 0.11 | 0.14 | 0.15 | 0.18 | 0.24 | 0.25 * |
| Biomarker and FFQ Measurement | Chinese | Malay | Indian |
|---|---|---|---|
| n = 59 | n = 46 | n = 56 | |
| Isoflavones (μg/gUCr) | |||
| Soy protein (g/day) 1 | 0.31 | 0.58 * | 0.64 * |
| Total carotenoids (mg/L plasma) | |||
| Fruit (inc 100% fruit juice) (g/day) 2 | 0.41 * | 0.13 | 0.11 |
| Vegetables (g/day) 2 | 0.29 * | 0.28 | −0.15 |
| Total fruit and vegetables (g/day)2 | 0.43 * | 0.22 | 0.04 |
| Plasma EPA + DHA (% total FA) | |||
| Fish and seafood (g/day) | 0.35 * | 0.49 * | 0.28 * |
| Plasma polyunsaturated FA (% total FA) | |||
| Polyunsaturated fat (%E) | 0.08 | 0.02 | 0.24 |
| Plasma odd chain saturated FA (% total FA) | |||
| Dairy fat (g/day) | 0.36 * | 0.13 | 0.37 * |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whitton, C.; Ho, J.C.Y.; Tay, Z.; Rebello, S.A.; Lu, Y.; Ong, C.N.; Van Dam, R.M. Relative Validity and Reproducibility of a Food Frequency Questionnaire for Assessing Dietary Intakes in a Multi-Ethnic Asian Population Using 24-h Dietary Recalls and Biomarkers. Nutrients 2017, 9, 1059. https://doi.org/10.3390/nu9101059
Whitton C, Ho JCY, Tay Z, Rebello SA, Lu Y, Ong CN, Van Dam RM. Relative Validity and Reproducibility of a Food Frequency Questionnaire for Assessing Dietary Intakes in a Multi-Ethnic Asian Population Using 24-h Dietary Recalls and Biomarkers. Nutrients. 2017; 9(10):1059. https://doi.org/10.3390/nu9101059
Chicago/Turabian StyleWhitton, Clare, Jolene Chien Yee Ho, Zoey Tay, Salome A. Rebello, Yonghai Lu, Choon Nam Ong, and Rob M. Van Dam. 2017. "Relative Validity and Reproducibility of a Food Frequency Questionnaire for Assessing Dietary Intakes in a Multi-Ethnic Asian Population Using 24-h Dietary Recalls and Biomarkers" Nutrients 9, no. 10: 1059. https://doi.org/10.3390/nu9101059