Serum Magnesium Levels in Preterm Infants Are Higher Than Adult Levels: A Systematic Literature Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
3. Results
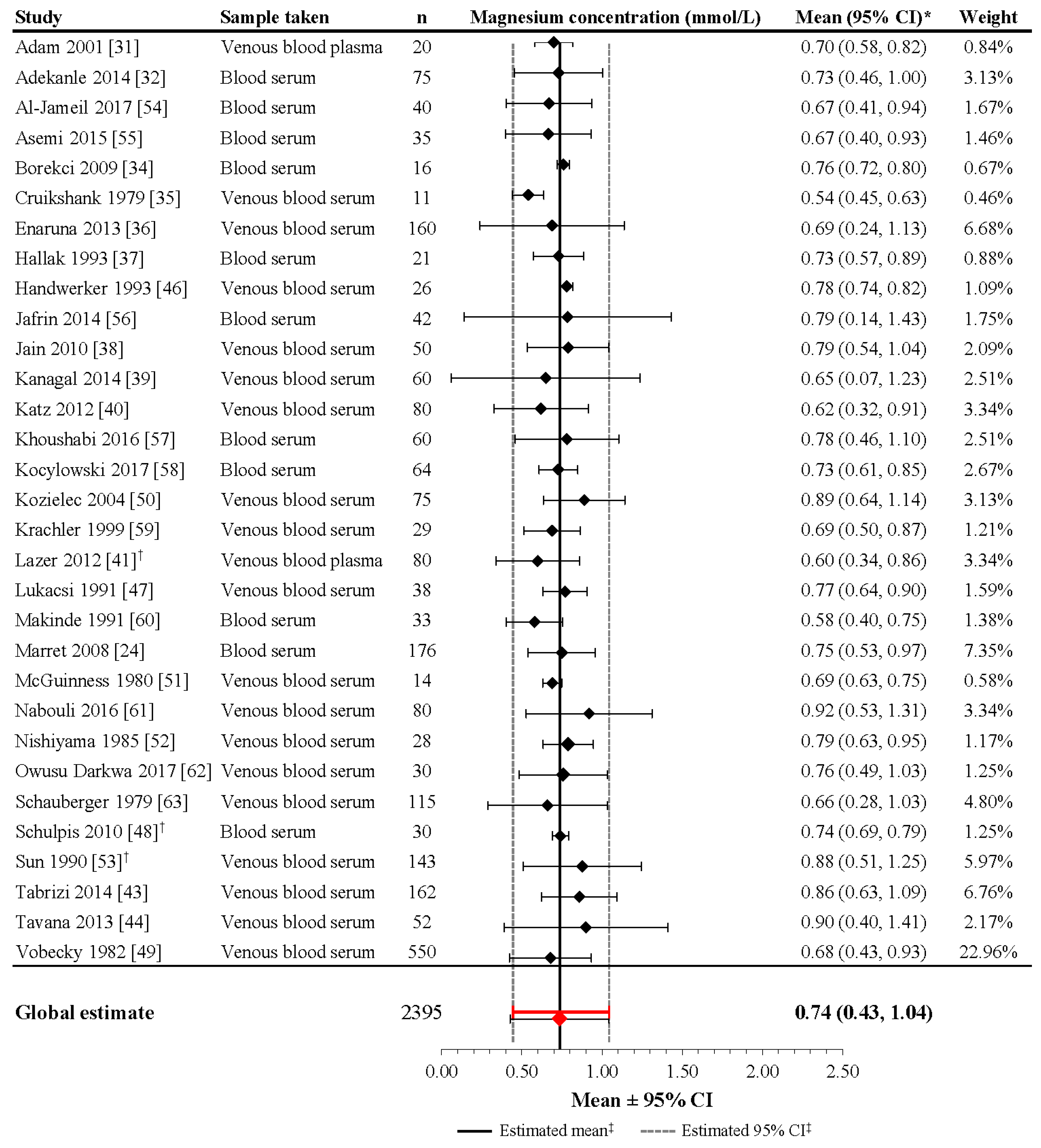
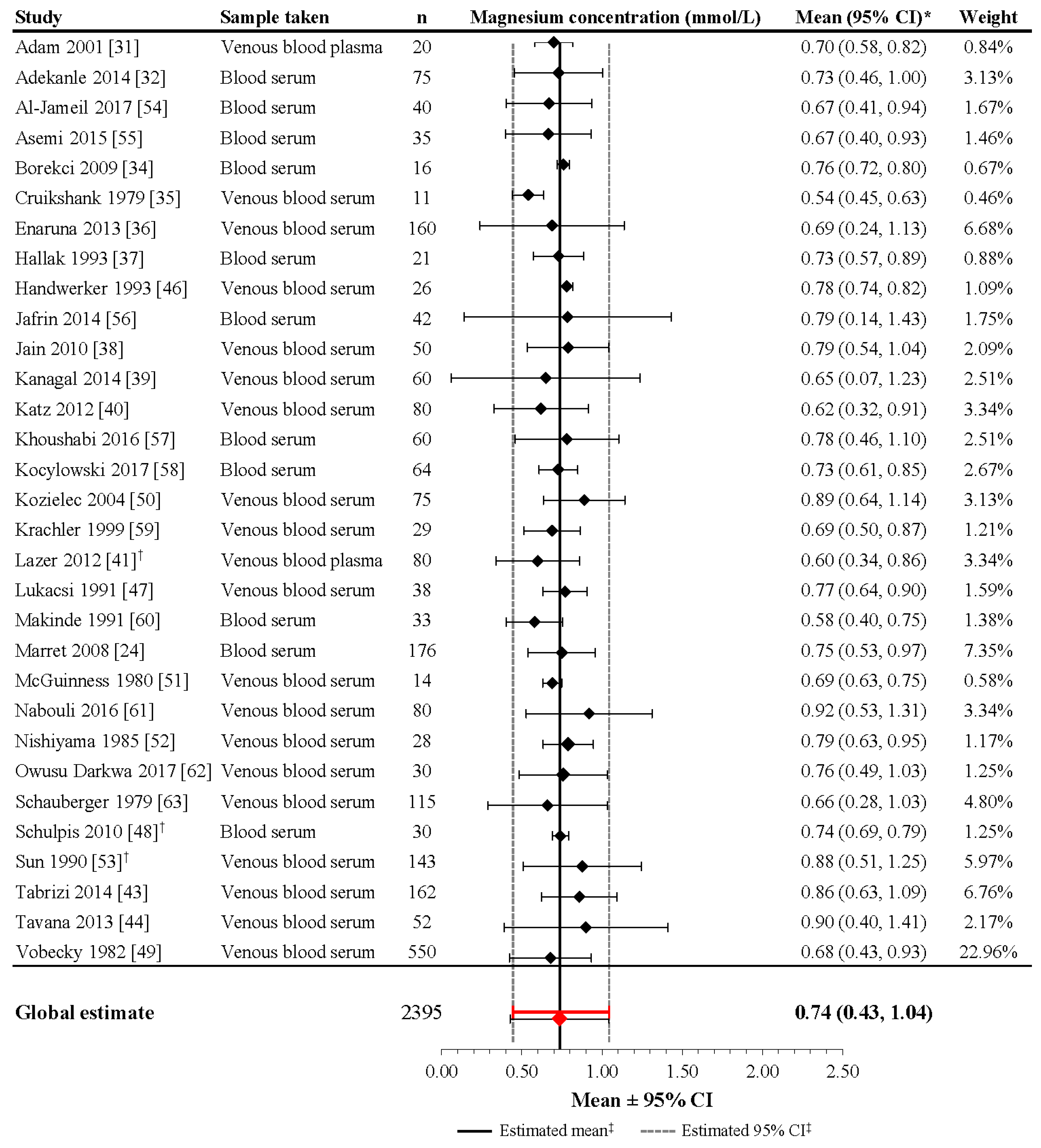
3.1. Maternal Magnesium Concentrations
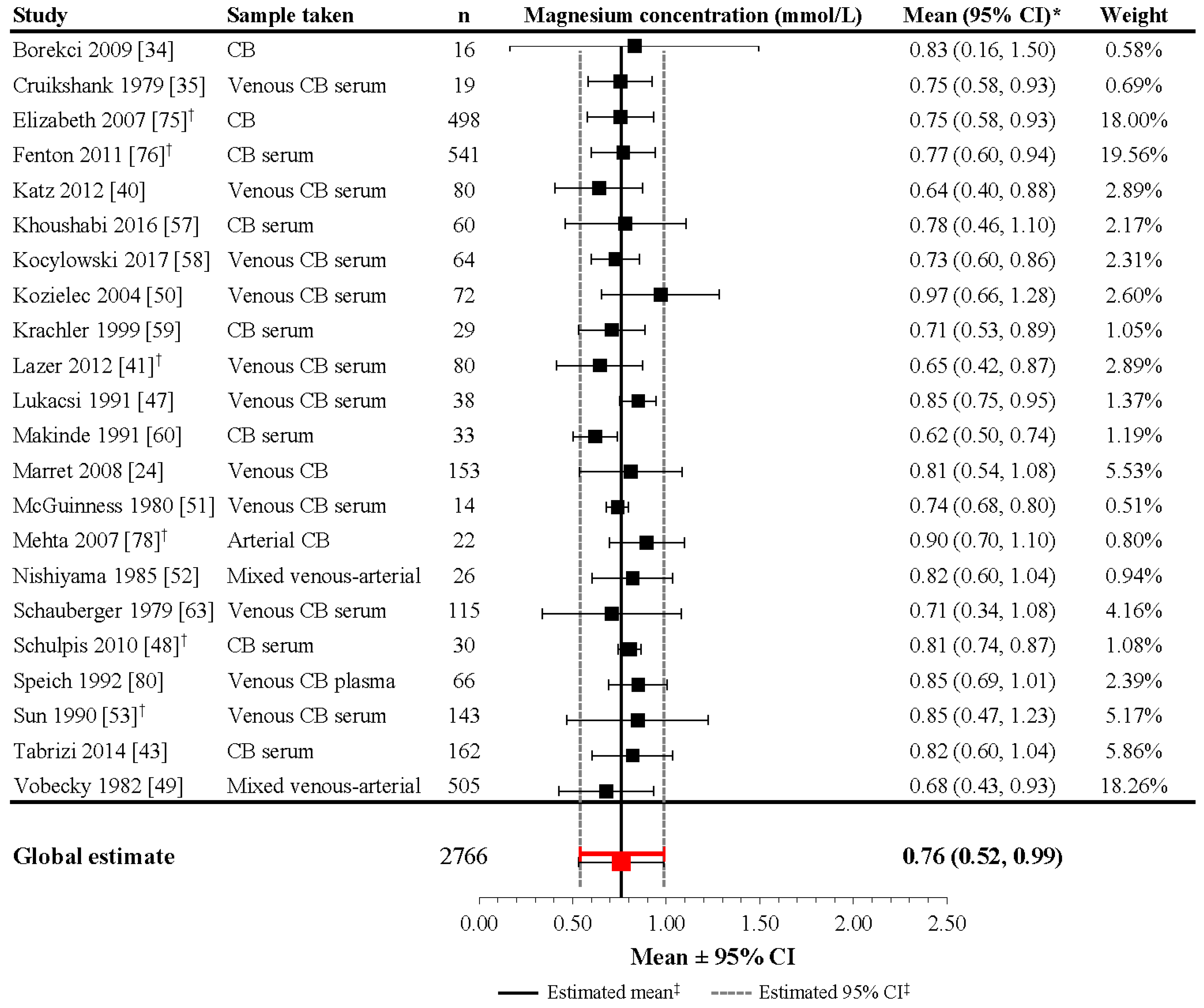
3.2. Magnesium Levels at Birth in Neonates without Magnesium Supplementation during Pregnancy
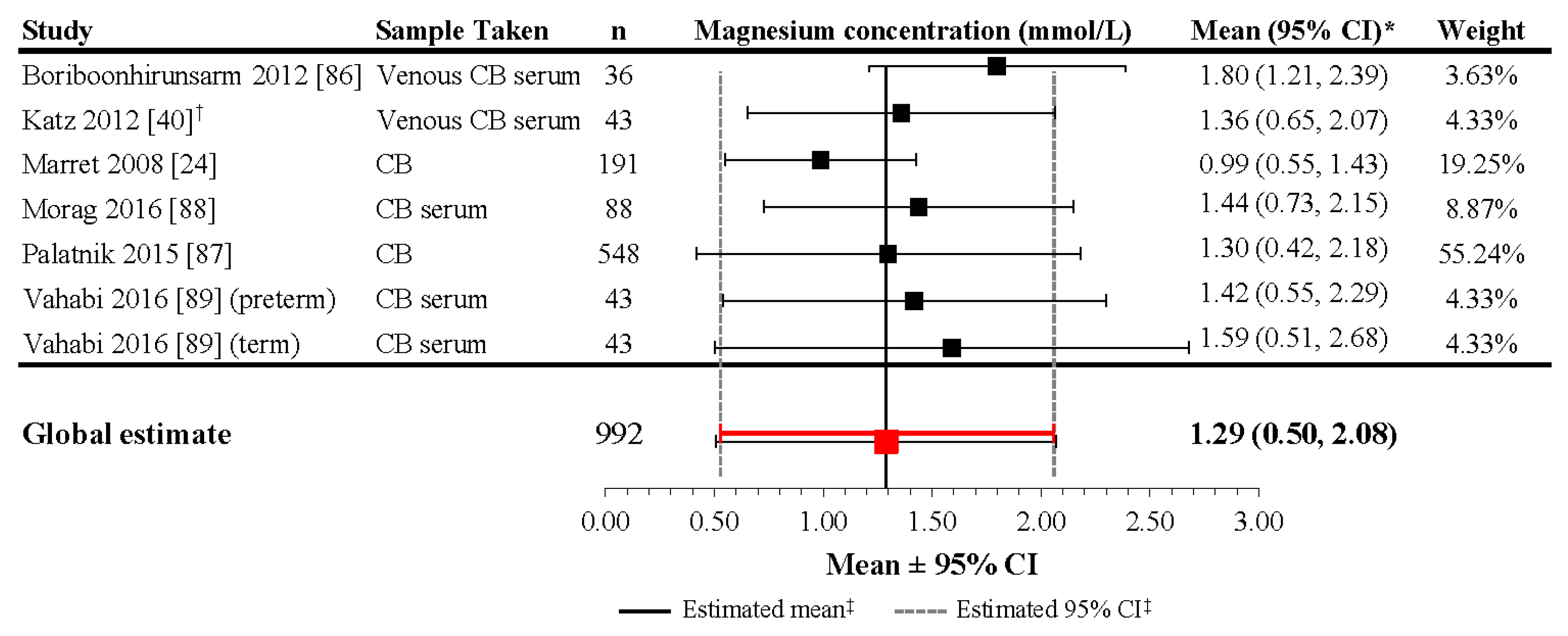
3.3. Magnesium Levels at Birth in Neonates with Magnesium Supplementation during Pregnancy
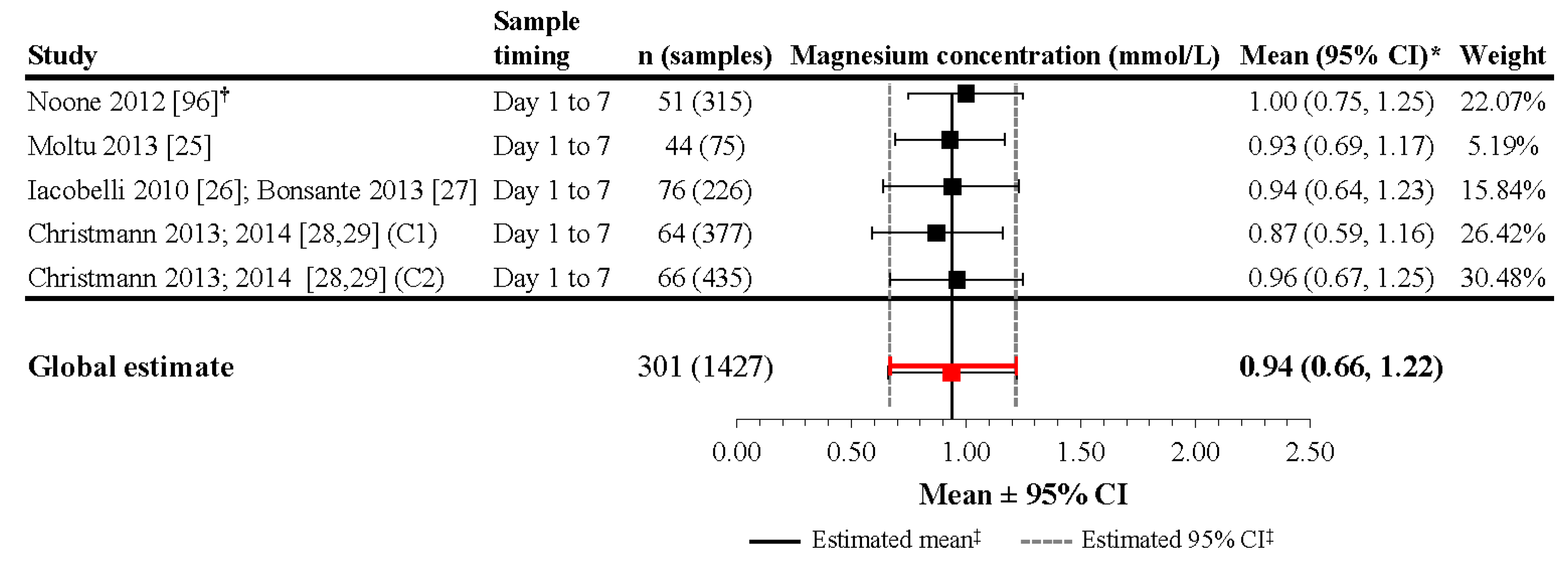
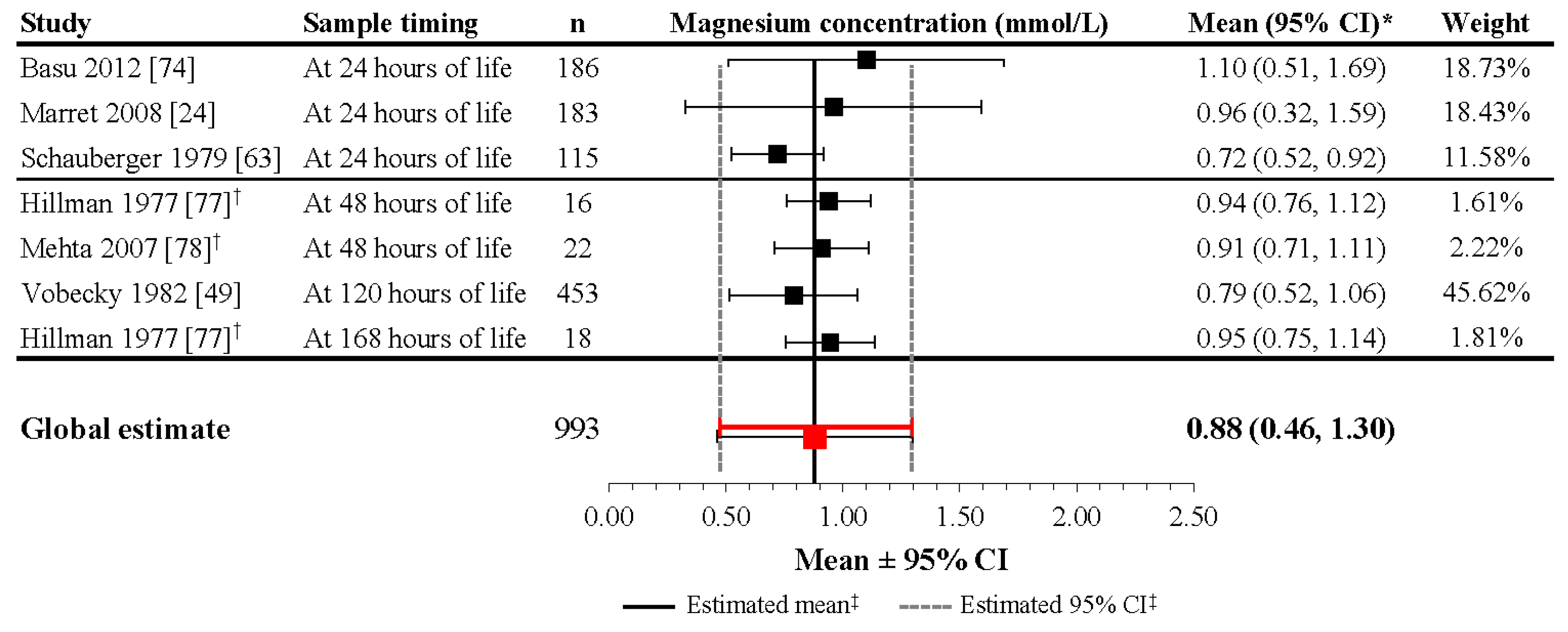
3.4. Magnesium Levels in Neonates during the First Days of Life
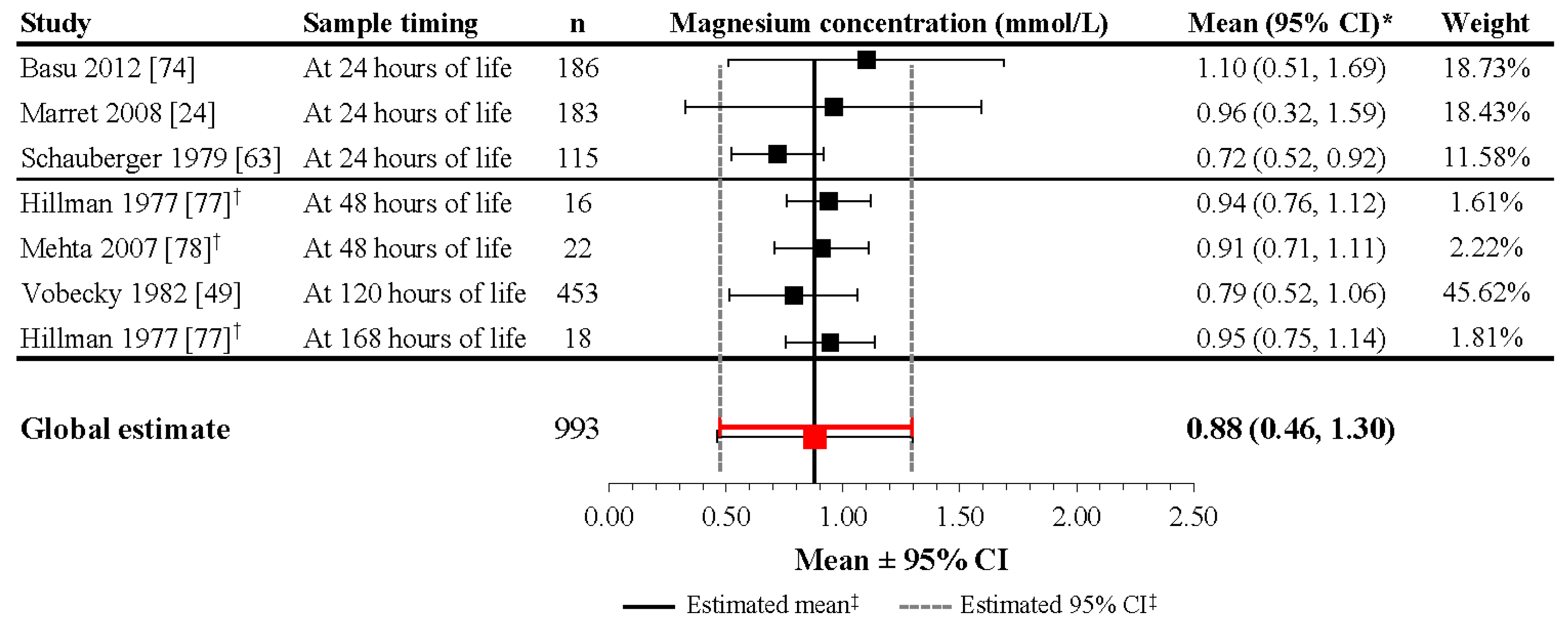
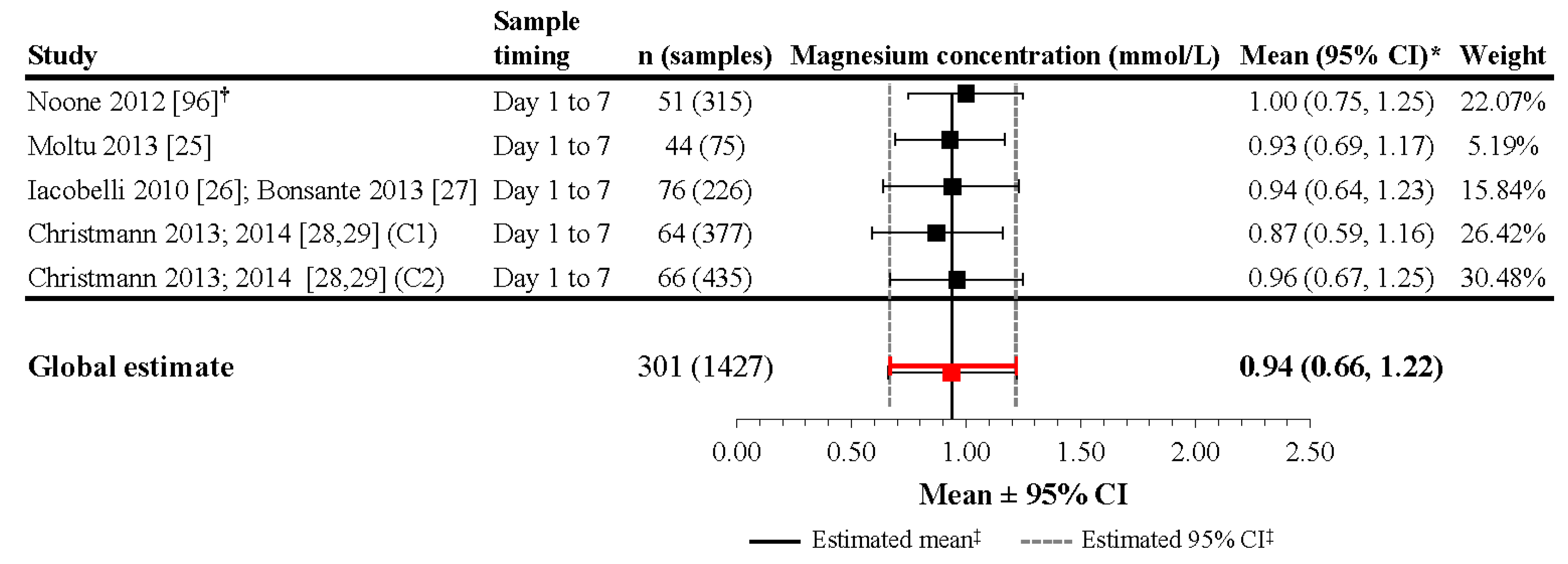
3.4.1. Infants without Prenatal Magnesium Supplementation
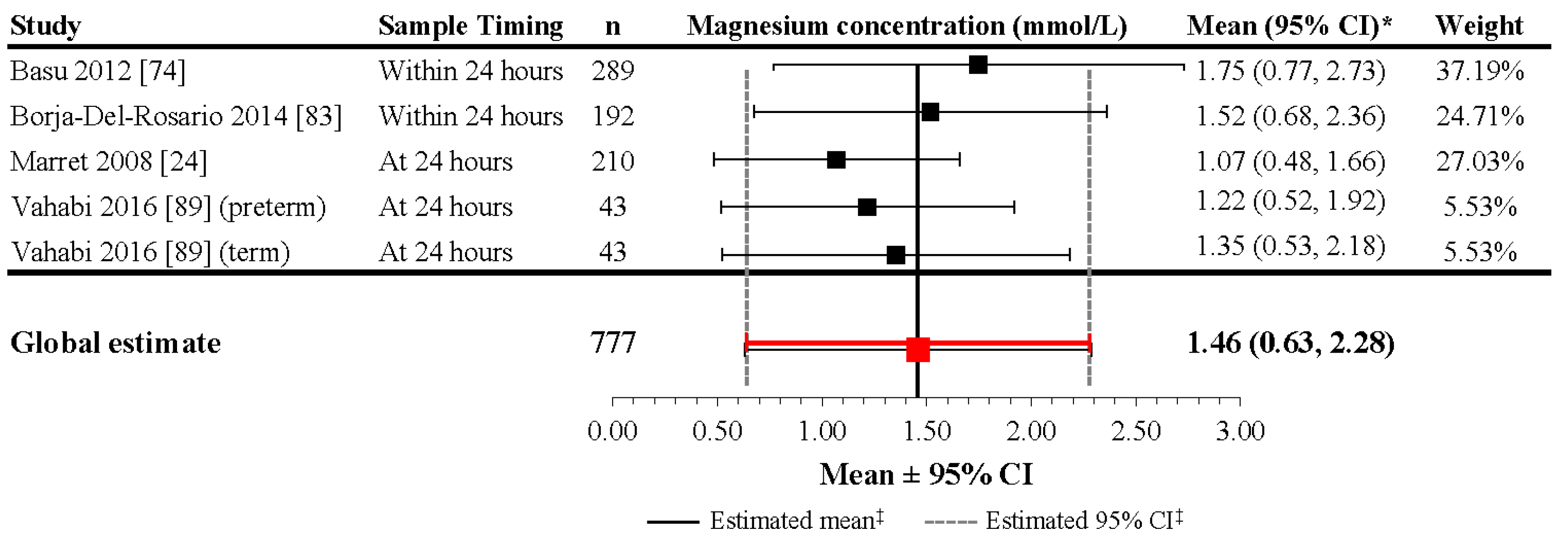
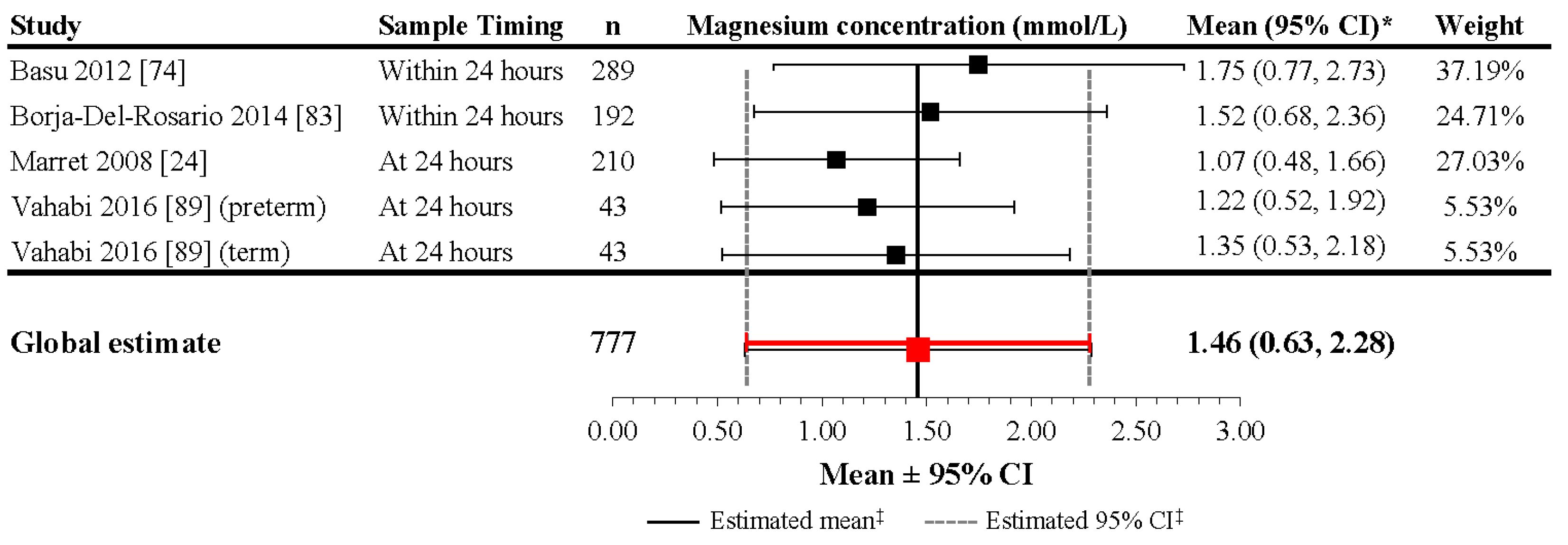
3.4.2. Infants with Prenatal Magnesium Supplementation
3.5. Factors Contributing to Magnesium Levels in Neonates during the First Days of Life
3.6. Benefits and Risks of Elevated Neonatal Serum Magnesium
3.6.1. Benefit: Neuroprotection
3.6.2. Risk: Adverse Outcomes
3.7. Implications for Postnatal Magnesium Supplementation in Preterm Infants
3.8. Limitations
4. Summary and Recommendations
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Elin, R.J. Assessment of magnesium status. Clin. Chem. 1987, 33, 1965–1970. [Google Scholar] [PubMed]
- Rubin, H. Central role for magnesium in coordinate control of metabolism and growth in animal cells. Proc. Natl. Acad. Sci. USA 1975, 72, 3551–3555. [Google Scholar] [CrossRef] [PubMed]
- Perraud, A.L.; Zhao, X.; Ryazanov, A.G.; Schmitz, C. The channel-kinase TRPM7 regulates phosphorylation of the translational factor eEF2 via eEF2-k. Cell. Signal. 2011, 23, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Rubin, H. Central roles of Mg2+ and MgATP2− in the regulation of protein synthesis and cell proliferation: Significance for neoplastic transformation. Adv. Cancer Res. 2005, 93, 1–58. [Google Scholar] [PubMed]
- Ko, Y.H.; Hong, S.; Pedersen, P.L. Chemical mechanism of ATP synthase. Magnesium plays a pivotal role in formation of the transition state where ATP is synthesized from ADP and inorganic phosphate. J. Biol. Chem. 1999, 274, 28853–28856. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, L.; Garfinkel, D. Magnesium regulation of the glycolytic pathway and the enzymes involved. Magnesium 1985, 4, 60–72. [Google Scholar] [PubMed]
- Hubbard, J.I.; Jones, S.F.; Landau, E.M. On the mechanism by which calcium and magnesium affect the release of transmitter by nerve impulses. J. Physiol. 1968, 196, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Iseri, L.T.; French, J.H. Magnesium: Nature’s physiologic calcium blocker. Am. Heart J. 1984, 108, 188–193. [Google Scholar] [CrossRef]
- Dorup, I.; Clausen, T. Correlation between magnesium and potassium contents in muscle: Role of Na(+)-K+ pump. Am. J. Physiol. 1993, 264, C457–C463. [Google Scholar] [PubMed]
- Shechter, M.; Kaplinsky, E.; Rabinowitz, B. The rationale of magnesium supplementation in acute myocardial infarction. A review of the literature. Arch. Intern. Med. 1992, 152, 2189–2196. [Google Scholar] [CrossRef] [PubMed]
- Rigo, J.; Mohamed, M.W.; De Curtis, M. Disorders of calcium, phosphorus and magnesium metabolism. In Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant, 9th ed.; Martin, R.J., Fanaroff, A.A., Walsh, M.C., Eds.; Elsevier: Philadelphia, PA, USA, 2011; Volume 2, pp. 1523–1556. [Google Scholar]
- Elin, R.J. Assessment of magnesium status for diagnosis and therapy. Magnes. Res. 2010, 23, S194–S198. [Google Scholar] [PubMed]
- Wu, A. Tietz Clinical Guide to Laboratory Tests, 4th ed.; Saunders: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Duncanson, G.O.; Worth, H.G. Determination of reference intervals for serum magnesium. Clin. Chem. 1990, 36, 756–758. [Google Scholar] [PubMed]
- World Health Organization. Preterm Birth; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Colantonio, D.A.; Kyriakopoulou, L.; Chan, M.K.; Daly, C.H.; Brinc, D.; Venner, A.A.; Pasic, M.D.; Armbruster, D.; Adeli, K. Closing the gaps in pediatric laboratory reference intervals: A CALIPER database of 40 biochemical markers in a healthy and multiethnic population of children. Clin. Chem. 2012, 58, 854–868. [Google Scholar] [CrossRef] [PubMed]
- Mimouni, F.B.; Mandel, D.; Lubetzky, R.; Senterre, T. Calcium, phosphorus, magnesium and vitamin D requirements of the preterm infant. World Rev. Nutr. Diet. 2014, 110, 140–151. [Google Scholar] [PubMed]
- Ziegler, E.E.; O’Donnell, A.M.; Nelson, S.E.; Fomon, S.J. Body composition of the reference fetus. Growth 1976, 40, 329–341. [Google Scholar] [PubMed]
- Vafaei, H.; Dalili, M.; Hashemi, S.A. Serum concentration of calcium, magnesium and zinc in normotensive versus preeclampsia pregnant women: A descriptive study in women of Kerman province of Iran. Iran. J. Reprod. Med. 2015, 13, 23–26. [Google Scholar] [PubMed]
- Sherwani, S.; Hasnain, N.; Qadir, U. Magnesium status in maternal and cord blood. J. Pak. Med. Assoc. 1998, 48, 32–34. [Google Scholar] [PubMed]
- Sherwin, C.M.; Balch, A.; Campbell, S.C.; Fredrickson, J.; Clark, E.A.; Varner, M.; Stockmann, C.; Korgenski, E.K.; Bonkowsky, J.L.; Spigarelli, M.G. Maternal magnesium sulphate exposure predicts neonatal magnesium blood concentrations. Basic Clin. Pharmacol. Toxicol. 2014, 114, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Ephraim, R.K.; Osakunor, D.N.; Denkyira, S.W.; Eshun, H.; Amoah, S.; Anto, E.O. Serum calcium and magnesium levels in women presenting with pre-eclampsia and pregnancy-induced hypertension: A case-control study in the Cape Coast metropolis, Ghana. BMC Pregnancy Childbirth 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marret, S.; Marpeau, L.; Follet-Bouhamed, C.; Cambonie, G.; Astruc, D.; Delaporte, B.; Bruel, H.; Guillois, B.; Pinquier, D.; Zupan-Simunek, V.; et al. Effect of magnesium sulphate on mortality and neurologic morbidity of the very-preterm newborn (of less than 33 weeks) with two-year neurological outcome: Results of the prospective PREMAG trial. Gynecol. Obstet. Fertil. 2008, 36, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Moltu, S.J.; Strommen, K.; Blakstad, E.W.; Almaas, A.N.; Westerberg, A.C.; Braekke, K.; Ronnestad, A.; Nakstad, B.; Berg, J.P.; Veierod, M.B.; et al. Enhanced feeding in very-low-birth-weight infants may cause electrolyte disturbances and septicemia--a randomized, controlled trial. Clin. Nutr. 2013, 32, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Iacobelli, S.; Bonsante, F.; Gouyon, J.B. Fluid and electrolyte intake during the first week of life in preterm infants receiving parenteral nutrition according current guidelines. Minerva Pediatr. 2010, 62, 203–204. [Google Scholar] [PubMed]
- Bonsante, F.; Iacobelli, S.; Latorre, G.; Rigo, J.; De Felice, C.; Robillard, P.Y.; Gouyon, J.B. Initial amino acid intake influences phosphorus and calcium homeostasis in preterm infants—It is time to change the composition of the early parenteral nutrition. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Christmann, V.; Visser, R.; Engelkes, M.; de Grauw, A.M.; van Goudoever, J.B.; van Heijst, A.F. The enigma to achieve normal postnatal growth in preterm infants—Using parenteral or enteral nutrition? Acta Paediatr. 2013, 102, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Christmann, V.; de Grauw, A.M.; Visser, R.; Matthijsse, R.P.; van Goudoever, J.B.; van Heijst, A.F. Early postnatal calcium and phosphorus metabolism in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Kurzel, R.B. Serum magnesium levels in pregnancy and preterm labor. Am. J. Perinatol. 1991, 8, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Adam, B.; Malatyalioglu, E.; Alvur, M.; Talu, C. Magnesium, zinc and iron levels in pre-eclampsia. J. Matern. Fetal Med. 2001, 10, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Adekanle, D.; Adeyemo, O.; Adeniyi, A.; Okere, R.; Jimoh, A.; Adebara, I.; Bakare, A.; Atiba, A.; Adelekan, A.; Olofinbiyi, B. Serum magnesium levels in healthy pregnant and pre-eclamptic patients—A cross-section study. Open J. Obstet. Gynecol. 2014, 4, 561–568. [Google Scholar] [CrossRef]
- Apostol, A.; Apostol, R.; Ali, E.; Choi, A.; Ehsuni, N.; Hu, B.; Li, L.; Altura, B.T.; Altura, B.M. Cerebral spinal fluid and serum ionized magnesium and calcium levels in preeclamptic women during administration of magnesium sulfate. Fertil. Steril. 2010, 94, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Borekci, B.; Gulaboglu, M.; Gul, M. Iodine and magnesium levels in maternal and umbilical cord blood of preeclamptic and normal pregnant women. Biol. Trace Elem. Res. 2009, 129, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cruikshank, D.P.; Pitkin, R.M.; Reynolds, W.A.; Williams, G.A.; Hargis, G.K. Effects of magnesium sulfate treatment on perinatal calcium metabolism. I. Maternal and fetal responses. Am. J. Obstet. Gynecol. 1979, 134, 243–249. [Google Scholar] [CrossRef]
- Enaruna, N.O.; Ande, A.; Okpere, E.E. Clinical significance of low serum magnesium in pregnant women attending the University of Benin Teaching Hospital. Niger. J. Clin. Pract. 2013, 16, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Hallak, M.; Berry, S.M.; Madincea, F.; Romero, R.; Evans, M.I.; Cotton, D.B. Fetal serum and amniotic fluid magnesium concentrations with maternal treatment. Obstet. Gynecol. 1993, 81, 185–188. [Google Scholar] [PubMed]
- Jain, S.; Sharma, P.; Kulshreshtha, S.; Mohan, G.; Singh, S. The role of calcium, magnesium, and zinc in pre-eclampsia. Biol. Trace Elem. Res. 2010, 133, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Kanagal, D.V.; Rajesh, A.; Rao, K.; Devi, U.H.; Shetty, H.; Kumari, S.; Shetty, P.K. Levels of serum calcium and magnesium in pre-eclamptic and normal pregnancy: A study from coastal India. J. Clin. Diagn. Res. 2014, 8, Oc01–Oc04. [Google Scholar] [CrossRef] [PubMed]
- Katz, O.; Paz-Tal, O.; Lazer, T.; Aricha-Tamir, B.; Mazor, M.; Wiznitzer, A.; Sheiner, E. Severe pre-eclampsia is associated with abnormal trace elements concentrations in maternal and fetal blood. J. Matern. Fetal Neonatal Med. 2012, 25, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Lazer, T.; Paz-Tal, O.; Katz, O.; Aricha-Tamir, B.; Sheleg, Y.; Maman, R.; Silberstein, T.; Mazor, M.; Wiznitzer, A.; Sheiner, E. Trace elements’ concentrations in maternal and umbilical cord plasma at term gestation: A comparison between active labor and elective cesarean delivery. J. Matern. Fetal Neonatal Med. 2012, 25, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.L. Serum electrolytes in pregnancy, parturition, and puerperium. Obstet. Gynecol. 1957, 10, 51–55. [Google Scholar] [PubMed]
- Tabrizi, F.M.; Pakdel, F.G. Serum level of some minerals during three trimesters of pregnancy in Iranian women and their newborns: A longitudinal study. Indian J. Clin. Biochem. 2014, 29, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Tavana, Z.; Hosseinmirzaei, S. Comparison of maternal serum magnesium level in pre-eclampsia and normal pregnant women. Iran. Red Crescent Med. J. 2013, 15, e10394. [Google Scholar] [CrossRef] [PubMed]
- Uludag, E.U.; Gozukara, I.O.; Kucur, S.K.; Ulug, P.; Ozdegirmenci, O.; Erkaya, S. Maternal magnesium level effect on preterm labor treatment. J. Matern. Fetal Neonatal Med. 2014, 27, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Handwerker, S.M.; Altura, B.T.; Royo, B.; Altura, B.M. Ionized magnesium and calcium levels in umbilical cord serum of pregnant women with transient hypertension during labor. Am. J. Hypertens. 1993, 6, 542–545. [Google Scholar] [PubMed]
- Lukacsi, L.; Lintner, F.; Zsolnai, B.; Somogyi, J. Magnesium transport in human pregnancy (magnesium content of human gestation tissues and tissue fluids). Acta Chir. Hung. 1991, 32, 263–268. [Google Scholar] [PubMed]
- Schulpis, K.H.; Karakonstantakis, T.; Vlachos, G.D.; Mentis, A.F.; Karikas, G.A.; Afordakou, D.; Papastamataki, M.; Antsaklis, A.; Papassotiriou, I. Maternal-neonatal magnesium and zinc serum concentrations after vaginal delivery. Scand. J. Clin. Lab. Investig. 2010, 70, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Vobecky, J.S.; Vobecky, J.; Shapcott, D.; Demers, P.P.; Cloutier, D.; Blanchard, R.; Fisch, C. Biochemical indices of nutritional status in maternal, cord, and early neonatal blood. Am. J. Clin. Nutr. 1982, 36, 630–642. [Google Scholar] [PubMed]
- Kozielec, T.; Durska, G.; Karakiewicz, B.; Kedzierska, E. Analysis of blood and hair to investigate the magnesium status of neonates and their mothers. Magnes. Res. 2004, 17, 85–89. [Google Scholar] [PubMed]
- McGuinness, G.A.; Weinstein, M.M.; Cruikshank, D.P.; Pitkin, R.M. Effects of magnesium sulfate treatment on perinatal calcium metabolism. II. Neonatal responses. Obstet. Gynecol. 1980, 56, 595–600. [Google Scholar] [PubMed]
- Nishiyama, S.; Fujimoto, S.; Kodama, M.; Matsuda, I. The negative correlation between prolactin and ionic calcium in cord blood of full term infants. Endocrinol. Jpn. 1985, 32, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.D.; Shao, Y.F.; Zhang, P.L.; Li, D.Z.; Gu, L.Y.; Guo, Q.N. Evaluation of prenatal nutrition counseling: Maternal nutrition status and infant birthweight. Biomed. Environ. Sci. 1990, 3, 458–465. [Google Scholar] [PubMed]
- Al-Jameil, N.; Tabassum, H.; Ali, M.N.; Qadeer, M.A.; Khan, F.A.; Al-Rashed, M. Correlation between serum trace elements and risk of preeclampsia: A case controlled study in Riyadh, Saudi Arabia. Saudi J. Biol. Sci. 2017, 24, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Karamali, M.; Jamilian, M.; Foroozanfard, F.; Bahmani, F.; Heidarzadeh, Z.; Benisi-Kohansal, S.; Surkan, P.J.; Esmaillzadeh, A. Magnesium supplementation affects metabolic status and pregnancy outcomes in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2015, 102, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Jafrin, W.; Mia, A.R.; Chakraborty, P.K.; Hoque, M.R.; Paul, U.K.; Shaha, K.R.; Akhter, S.; Roy, A.S. An evaluation of serum magnesium status in pre-eclampsia compared to the normal pregnancy. Mymensingh Med. J. 2014, 23, 649–653. [Google Scholar] [PubMed]
- Khoushabi, F.; Shadan, M.R.; Miri, A.; Sharifi-Rad, J. Determination of maternal serum zinc, iron, calcium and magnesium during pregnancy in pregnant women and umbilical cord blood and their association with outcome of pregnancy. Mater. Sociomed. 2016, 28, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Kocylowski, R.; Lewicka, I.; Grzesiak, M.; Gaj, Z.; Oszukowski, P.; von Kaisenberg, C.; Suliburska, J. Evaluation of mineral concentrations in maternal serum before and after birth and in newborn cord blood postpartum-preliminary study. Biol. Trace Elem. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Krachler, M.; Rossipal, E.; Micetic-Turk, D. Trace element transfer from the mother to the newborn—Investigations on triplets of colostrum, maternal and umbilical cord sera. Eur. J. Clin. Nutr. 1999, 53, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Makinde, O.O.; Amole, F.; Ogunniyi, S.O. Serum copper, zinc and magnesium in maternal and cord blood at delivery. West Afr. J. Med. 1991, 10, 168–170. [Google Scholar] [PubMed]
- Nabouli, M.R.; Lassoued, L.; Bakri, Z.; Moghannem, M. Modification of total magnesium level in pregnant Saudi women developing gestational diabetes mellitus. Diabetes Metab. Syndr. 2016, 10, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Owusu Darkwa, E.; Antwi-Boasiako, C.; Djagbletey, R.; Owoo, C.; Obed, S.; Sottie, D. Serum magnesium and calcium in preeclampsia: A comparative study at the Korle-Bu Teaching Hospital, Ghana. Integr. Blood Press. Control 2017, 10, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Schauberger, C.W.; Pitkin, R.M. Maternal-perinatal calcium relationships. Obstet. Gynecol. 1979, 53, 74–76. [Google Scholar] [PubMed]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The case for an evidence-based reference interval for serum magnesium: The time has come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef] [PubMed]
- Bardicef, M.; Bardicef, O.; Sorokin, Y.; Altura, B.M.; Altura, B.T.; Cotton, D.B.; Resnick, L.M. Extracellular and intracellular magnesium depletion in pregnancy and gestational diabetes. Am. J. Obstet. Gynecol. 1995, 172, 1009–1013. [Google Scholar] [CrossRef]
- Goker Tasdemir, U.; Tasdemir, N.; Kilic, S.; Abali, R.; Celik, C.; Gulerman, H.C. Alterations of ionized and total magnesium levels in pregnant women with gestational diabetes mellitus. Gynecol. Obstet. Investig. 2015, 79, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.V.; Hocher, B.; Verkaart, S.; van Zeeland, F.; Pfab, T.; Slowinski, T.; Chen, Y.P.; Schlingmann, K.P.; Schaller, A.; Gallati, S.; et al. Loss of insulin-induced activation of TRPM6 magnesium channels results in impaired glucose tolerance during pregnancy. Proc. Natl. Acad. Sci. USA 2012, 109, 11324–11329. [Google Scholar] [CrossRef] [PubMed]
- Mitrovic-Jovanovic, A.; Dragojevic-Dikic, S.; Zamurovic, M.; Nikolic, B.; Gojnic, M.; Rakic, S.; Jovanovic, T. Comparison of electrolytic status (Na+, K+, Ca2+, Mg2+) in preterm and term deliveries. Clin. Exp. Obstet. Gynecol. 2012, 39, 479–482. [Google Scholar] [PubMed]
- Standley, C.A.; Whitty, J.E.; Mason, B.A.; Cotton, D.B. Serum ionized magnesium levels in normal and preeclamptic gestation. Obstet. Gynecol. 1997, 89, 24–27. [Google Scholar] [CrossRef]
- Makrides, M.; Crowther, C.A. Magnesium supplementation in pregnancy. Cochrane Database Syst. Rev. 2001. [Google Scholar] [CrossRef]
- Abbassi-Ghanavati, M.; Alexander, J.M.; McIntire, D.D.; Savani, R.C.; Leveno, K.J. Neonatal effects of magnesium sulfate given to the mother. Am. J. Perinatol. 2012, 29, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W.; Crowther, C.A.; Middleton, P.; Marret, S.; Rouse, D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Doyle, L.W.; Crowther, C.A.; Middleton, P.; Marret, S. Antenatal magnesium sulfate and neurologic outcome in preterm infants. Obstet. Gynecol. 2009, 113, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.K.; Chickajajur, V.; Lopez, V.; Bhutada, A.; Pagala, M.; Rastogi, S. Immediate clinical outcomes in preterm neonates receiving antenatal magnesium for neuroprotection. J. Perinat. Med. 2012, 40, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, K.E.; Krishnan, V.; Zachariah, P. Auxologic, biochemical and clinical (ABC) profile of low birth weight babies- a 2-year prospective study. J. Trop. Pediatr. 2007, 53, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Lyon, A.W.; Rose, M.S. Cord blood calcium, phosphate, magnesium, and alkaline phosphatase gestational age-specific reference intervals for preterm infants. BMC Pediatr. 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Hillman, L.S.; Rojanasathit, S.; Slatopolsky, E.; Haddad, J.G. Serial measurements of serum calcium, magnesium, parathyroid hormone, calcitonin, and 25-hydroxy-vitamin D in premature and term infants during the first week of life. Pediatr. Res. 1977, 11, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Petrova, A. Ionized magnesium and gestational age. Indian J. Pediatr. 2007, 74, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Rudnicki, M.; Frolich, A.; Fischer-Rasmussen, W. Magnesium supplement in pregnancy-induced hypertension: Effects on maternal and neonatal magnesium and calcium homeostasis. Miner. Electrolyte Metab. 1991, 17, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Speich, M.; Murat, A.; Auget, J.L.; Bousquet, B.; Arnaud, P. Magnesium, total calcium, phosphorus, copper, and zinc in plasma and erythrocytes of venous cord blood from infants of diabetic mothers: Comparison with a reference group by logistic discriminant analysis. Clin. Chem. 1992, 38, 2002–2007. [Google Scholar] [PubMed]
- Stigson, L.; Kjellmer, I. Serum levels of magnesium at birth related to complications of immaturity. Acta Paediatr. 1997, 86, 991–994. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Bone metabolism in the fetus and neonate. Pediatr. Nephrol. 2014, 29, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Borja-Del-Rosario, P.; Basu, S.K.; Haberman, S.; Bhutada, A.; Rastogi, S. Neonatal serum magnesium concentrations are determined by total maternal dose of magnesium sulfate administered for neuroprotection. J. Perinat. Med. 2014, 42, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Handwerker, S.M.; Altura, B.T.; Royo, B.; Altura, B.M. Ionized serum magnesium levels in umbilical cord blood of normal pregnant women at delivery: Relationship to calcium, demographics, and birthweight. Am. J. Perinatol. 1993, 10, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J.; Smith, L.G., Jr.; Burns, P.A. Effects of long-term maternal intravenous magnesium sulfate therapy on neonatal calcium metabolism and bone mineral content. Gynecol. Obstet. Investig. 1997, 43, 236–241. [Google Scholar] [CrossRef]
- Boriboonhirunsarn, D.; Lertbunnaphong, T.; Suwanwanich, M. Correlation of magnesium levels in cord blood and maternal serum among pre-eclamptic pregnant women treated with magnesium sulfate. J. Obstet. Gynaecol. Res. 2012, 38, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Palatnik, A.; Rouse, D.J.; Stamilio, D.M.; McPherson, J.A.; Grobman, W.A. Association between cerebral palsy or death and umbilical cord blood magnesium concentration. Am. J. Perinatol. 2015, 32, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Morag, I.; Yakubovich, D.; Stern, O.; Siman-Tov, M.; Schushan-Eisen, I.; Strauss, T.; Simchen, M. Short-term morbidities and neurodevelopmental outcomes in preterm infants exposed to magnesium sulphate treatment. J. Paediatr. Child Health 2016, 52, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Vahabi, S.; Zaman, M.; Farzan, B. Analysis of serum calcium, magnesium, and parathyroid hormone in neonates delivered following preeclampsia treatment. Cell. Mol. Biol. 2016, 62, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.; Schleyerbach, U.; Schaub, J. Magnesium balance studies in premature and term infants. Eur. J. Nutr. 2000, 39, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Guignard, J.P.; John, E.G. Renal function in the tiny, premature infant. Clin. Perinatol. 1986, 13, 377–401. [Google Scholar] [PubMed]
- Bueva, A.; Guignard, J.P. Renal function in preterm neonates. Pediatr. Res. 1994, 36, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Ariceta, G.; Rodriguez-Soriano, J.; Vallo, A. Renal magnesium handling in infants and children. Acta Paediatr. 1996, 85, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Pacifici, G.M. Clinical pharmacology of ibuprofen and indomethacin in preterm infants with patent ductus arteriosus. Curr. Pediatr. Rev. 2014, 10, 216–237. [Google Scholar] [PubMed]
- Allegaert, K.; Vanhole, C.; de Hoon, J.; Guignard, J.P.; Tibboel, D.; Devlieger, H.; Van Overmeire, B. Nonselective cyclo-oxygenase inhibitors and glomerular filtration rate in preterm neonates. Pediatr. Nephrol. 2005, 20, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Noone, D.; Kieran, E.; Molloy, E.J. Serum magnesium in the first week of life in extremely low birth weight infants. Neonatology 2012, 101, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Iacobelli, S.; Bonsante, F.; Vintejoux, A.; Gouyon, J.B. Standardized parenteral nutrition in preterm infants: Early impact on fluid and electrolyte balance. Neonatology 2010, 98, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Marret, S.; Marpeau, L.; Benichou, J. Benefit of magnesium sulfate given before very preterm birth to protect infant brain. Pediatrics 2008, 121, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Bain, E.; Middleton, P.; Crowther, C.A. Different magnesium sulphate regimens for neuroprotection of the fetus for women at risk of preterm birth. Cochrane Database Syst. Rev. 2012, 2. [Google Scholar] [CrossRef]
- Doll, E.; Wilkes, J.; Cook, L.J.; Korgenski, E.K.; Faix, R.G.; Yoder, B.A.; Srivastava, R.; Sherwin, C.M.; Spigarelli, M.G.; Clark, E.A.; et al. Neonatal magnesium levels correlate with motor outcomes in premature infants: A long-term retrospective cohort study. Front. Pediatr. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.A.; Charoo, B.A.; Bhat, J.I.; Ahmad, S.M.; Ali, S.W.; Mufti, M.U. Magnesium sulfate in severe perinatal asphyxia: A randomized, placebo-controlled trial. Pediatrics 2009, 123, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Ichiba, H.; Tamai, H.; Negishi, H.; Ueda, T.; Kim, T.J.; Sumida, Y.; Takahashi, Y.; Fujinaga, H.; Minami, H. Randomized controlled trial of magnesium sulfate infusion for severe birth asphyxia. Pediatr. Int. 2002, 44, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Mannan, M.A.; Yeasmin, F.; Shaha, C.K.; Rahman, M.H.; Shahidullah, M. Short-term outcome of magnesium sulfate infusion in perinatal asphyxia. Mymensingh Med. J. 2013, 22, 727–735. [Google Scholar] [PubMed]
- Fridman, E.; Linder, N. Magnesium and bronchopulmonary dysplasia. Harefuah 2013, 152, 158–161. [Google Scholar] [PubMed]
- Guerrero-Romero, F.; Rodriguez-Moran, M.; Hernandez-Ronquillo, G.; Gomez-Diaz, R.; Pizano-Zarate, M.L.; Wacher, N.H.; Mondragon-Gonzalez, R.; Simental-Mendia, L.E. Low serum magnesium levels and its association with high blood pressure in children. J. Pediatr. 2016, 168. [Google Scholar] [CrossRef] [PubMed]
- De Jesus, L.C.; Sood, B.G.; Shankaran, S.; Kendrick, D.; Das, A.; Bell, E.F.; Stoll, B.J.; Laptook, A.R.; Walsh, M.C.; Carlo, W.A.; et al. Antenatal magnesium sulfate exposure and acute cardiorespiratory events in preterm infants. Am. J. Obstet. Gynecol. 2015, 212. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, R.; Dambrosia, J.; Pryde, P.G.; Lee, K.S.; Gianopoulos, J.G.; Besinger, R.E.; Tomich, P.G. Association between the use of antenatal magnesium sulfate in preterm labor and adverse health outcomes in infants. Am. J. Obstet. Gynecol. 2002, 186, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Shimada, E.; Ogawa, M.; Matsuda, Y.; Mitani, M.; Matsui, H. Umbilical artery pH may be a possible confounder for neonatal adverse outcomes in preterm infants exposed to antenatal magnesium. J. Matern. Fetal Neonatal Med. 2013, 26, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, M.B.; Penn, A.A.; Thomas, L.J.; El-Sayed, Y.Y.; Caughey, A.B.; Lyell, D.J. Neonatal medical admission in a term and late-preterm cohort exposed to magnesium sulfate. Am. J. Obstet. Gynecol. 2011, 204. [Google Scholar] [CrossRef] [PubMed]
- Weisz, D.E.; Shivananda, S.; Asztalos, E.; Yee, W.; Synnes, A.; Lee, S.K.; Shah, P.S. Intrapartum magnesium sulfate and need for intensive delivery room resuscitation. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F59–F65. [Google Scholar] [CrossRef] [PubMed]
- Katayama, Y.; Minami, H.; Enomoto, M.; Takano, T.; Hayashi, S.; Lee, Y.K. Antenatal magnesium sulfate and the postnatal response of the ductus arteriosus to indomethacin in extremely preterm neonates. J. Perinatol. 2011, 31, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Walentik, C.; Mantych, G.J.; Sadiq, H.F.; Keenan, W.J.; Noguchi, A. Iatrogenic acute hypermagnesemia after total parenteral nutrition infusion mimicking septic shock syndrome: Two case reports. Pediatrics 2003, 112 Pt 1, e70–e72. [Google Scholar] [CrossRef] [PubMed]
- Huey, C.G.; Chan, K.M.; Wong, E.T.; Nelson, J.M.; Durand, M. Los Angeles County-University of Southern California Medical Center clinical pathology case conference: Extreme hypermagnesemia in a neonate. Clin. Chem. 1995, 41, 615–618. [Google Scholar] [PubMed]
- Hyun, H.S.; Choi, H.S.; Kim, J.K.; Ahn, S.Y.; Yoo, H.S.; Kim, E.S.; Chang, Y.S.; Park, W.S. Idiopathic severe hypermagnesemia in an extremely low birth weight infant on the first day of life. Korean J. Pediatr. 2011, 54, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration FDA Drug Safety Communication: FDA Recommends against Prolonged Use of Magnesium Sulfate to Stop Pre-Term Labor Due to Bone Changes in Exposed Babies. Available online: http://www.fda.gov/Drugs/DrugSafety/ucm353333.htm (accessed on 3 October 2017).
- Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.; Petersen, C.; Sacks, G.; Seres, D.; Guenter, P. Safe practices for parenteral nutrition. JPEN J. Parenter. Enteral Nutr. 2004, 28, S39–S70. [Google Scholar] [CrossRef] [PubMed]
- Canada, T.; Crill, C.M.; Guenter, P.; American Society of Parenteral and Enteral Nutrition. A.S.P.E.N. Parenteral Nutrition Handbook, 1st ed.; American Society for Parenteral and Enteral Nutrition: Silver Spring, MD, USA, 2009. [Google Scholar]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De, C.M.; Darmaun, D.; Decsi, T.; Domellof, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Canadian Paediatric Society. Nutrient needs and feeding of premature infants. Nutrition Committee. CMAJ 1995, 152, 1765–1785. [Google Scholar]
- Edmond, K.; Bahl, R. Optimal Feeding of LBW Infants 2006; World Health Organization (WHO): Geneva, Switzerland, 2006. [Google Scholar]
- Working Group of Pediatrics—Chinese Society of Parenteral and Enteral Nutrition; Working Group of Neonatology—Chinese Society of Pediatrics; Working Group of Neonatal Surgery—Chinese Society of Pediatric Surgery. CSPEN guidelines for nutrition support in neonates. Asia Pac. J. Clin. Nutr. 2013, 22, 655–663. [Google Scholar]
- Chawla, D.; Thukral, A.; Agarwal, R.; Deorari, A.K.; Paul, V.K. Parenteral nutrition. Indian J. Pediatr. 2008, 75, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 41 (Suppl. S2), S1–S87. [Google Scholar] [PubMed]
- Greene, H.L.; Hambidge, K.M.; Schanler, R.; Tsang, R.C. Guidelines for the use of vitamins, trace elements, calcium, magnesium, and phosphorus in infants and children receiving total parenteral nutrition: Report of the Subcommittee on Pediatric Parenteral Nutrient Requirements from the Committee on Clinical Practice Issues of the American Society for Clinical Nutrition. Am. J. Clin. Nutr. 1988, 48, 1324–1342. [Google Scholar] [PubMed]
- Klein, C.J. Nutrient requirements for preterm infant formulas. J. Nutr. 2002, 132, 1395s–1577s. [Google Scholar] [PubMed]
- Rigo, J.; Marlowe, M.L.; Bonnot, D.; Senterre, T.; Lapillonne, A.; Kermorvant-Duchemin, E.; Hascoet, J.M.; Desandes, R.; Malfilatre, G.; Pladys, P.; et al. Benefits of a new pediatric triple-chamber bag for parenteral nutrition in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 210–217. [Google Scholar] [CrossRef] [PubMed]
- A.S.P.E.N. Pediatric/Neonatal Parenteral Nutrition: The In’s and Out’s for the Non-Pediatric Clinician; American Society for Parenteral & Enteral Nutrition: Silver Spring, MD, USA, 2013. [Google Scholar]
- Tsang, R.C.; Tsang, R.C. Nutrition of the Preterm Infant: Scientific Basis and Practical Guidelines; Digital Educational Publishing, Incorporated: Cincinnati, OH, USA, 2005. [Google Scholar]
- Numeta G13%E to Be Suspended and New Risk Minimisation Measures to Be Introduced for NUMETA G16%E [Press Release]; European Medicines Agency: London, UK, 2013.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population (n) | Sampling Method | Maternal Magnesium Level, Mean ± SD, mmol/L | Neonatal Magnesium Level, Mean ± SD, mmol/L | Correlation |
|---|---|---|---|---|---|
| No magnesium supplementation | |||||
| Kozielec 2004 [50] | Term infants (38–41 weeks (72)) and mothers (75) derived from population of mothers (83) and neonates | At delivery, 2 mL maternal venous blood and 5 mL cord blood | 0.89 ± 0.13 | 0.97 ± 0.16 | r = 0.52 p = 0.000006 |
| Marret 2008 [24] | Preterm infants (23–32 weeks (92)) and mothers (92) | At delivery; mothers blood serum and venous cord blood | 0.78 ± 0.11 | 0.83 ± 0.13 | r = 0.36 p = 0.0004 |
| Schulpis 2010 [48] | Term infants and mothers - Vaginal delivery (16) - Scheduled cesarean delivery (14) | Mothers at the beginning of delivery; cord blood within 3–4 min of delivery | 0.81 ± 0.09 0.81 ± 0.04 | 0.81 ± 0.04 0.80 ± 0.02 | r = not provided p > 0.05 r = not provided p > 0.05 |
| Vobecky 1982 [49] | Mothers (550) and healthy term infants (505) | Maternal venous blood obtained during delivery; mixed venous-arterial cord blood at delivery | 0.68 ± 0.13 | 0.69 ± 0.13 | r = 0.64 p < 0.01 |
| Magnesium supplementation | |||||
| Borja-Del-Rosario 2014 [83] | Preterm infants 24–32 weeks (192) and their mothers | Maternal serum within 6 h before delivery; neonatal serum 24 h post-delivery | 2.30 ± 0.51 | 1.52 ± 0.43 | r = 0.10 p = 0.15 |
| Marret 2008 [24] | Preterm infants (23–32 weeks (119)) and mothers (119) | At delivery; mothers blood serum and venous cord blood | 0.77 ± 0.129 | 1.0 ± 0.193 | r = 0.23 p = 0.012 |
| Rudnicki 1991 [79] | Women (12) with pregnancy-induced hypertension and their infants (gestational age, 37–39 weeks) | Mothers prior to delivery; arterial blood from cord | 0.74 (0.71, 0.81) 1 | 0.80 (0.70, 0.91) 1 | r = 0.77 p < 0.02 |
| Schanler 1997 [85] | Women in preterm labor (16) and their infants (22); mean gestational age, 31.7 ± 2.6 weeks | At delivery; peripheral venous blood from mothers and infants | Not provided (figure only) | Not provided (figure only) | r = 0.61 p = 0.004 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigo, J.; Pieltain, C.; Christmann, V.; Bonsante, F.; Moltu, S.J.; Iacobelli, S.; Marret, S. Serum Magnesium Levels in Preterm Infants Are Higher Than Adult Levels: A Systematic Literature Review and Meta-Analysis. Nutrients 2017, 9, 1125. https://doi.org/10.3390/nu9101125
Rigo J, Pieltain C, Christmann V, Bonsante F, Moltu SJ, Iacobelli S, Marret S. Serum Magnesium Levels in Preterm Infants Are Higher Than Adult Levels: A Systematic Literature Review and Meta-Analysis. Nutrients. 2017; 9(10):1125. https://doi.org/10.3390/nu9101125
Chicago/Turabian StyleRigo, Jacques, Catherine Pieltain, Viola Christmann, Francesco Bonsante, Sissel J. Moltu, Silvia Iacobelli, and Stéphane Marret. 2017. "Serum Magnesium Levels in Preterm Infants Are Higher Than Adult Levels: A Systematic Literature Review and Meta-Analysis" Nutrients 9, no. 10: 1125. https://doi.org/10.3390/nu9101125