Associations between Nut Consumption and Health Vary between Omnivores, Vegetarians, and Vegans

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Intake
2.3. Nut Intake
2.4. Lifestyle Questionnaire
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics and Nut Consumption among the Cohort
3.2. Predictors of Nut Consumption
3.3. Nut Consumption and Anthropometric Measures
3.4. History of Selected Chronic Diseases and Risk Factors for Chronic Disease by Nut Consumption
3.5. Nut Consumption and Nutrient Intake
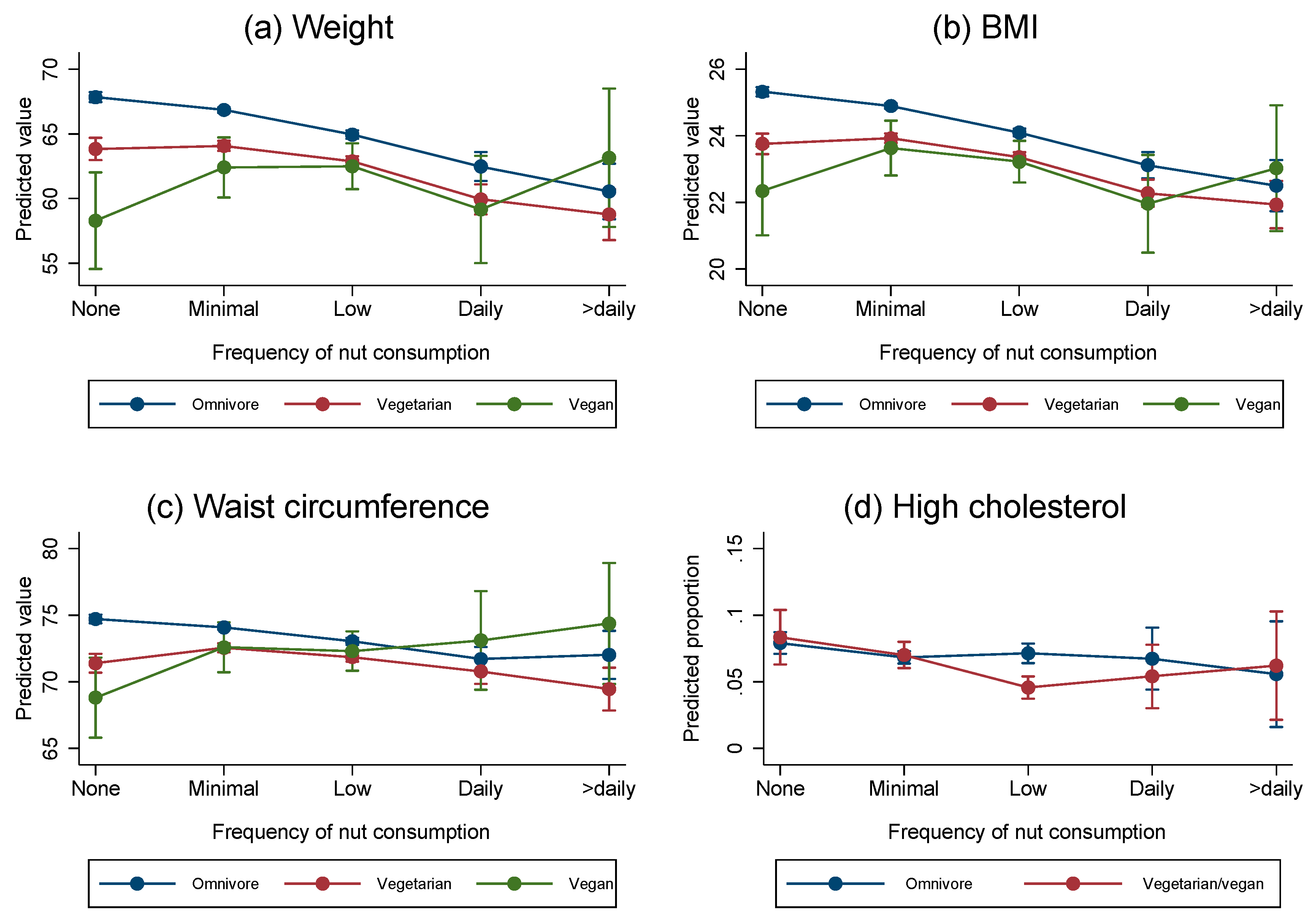
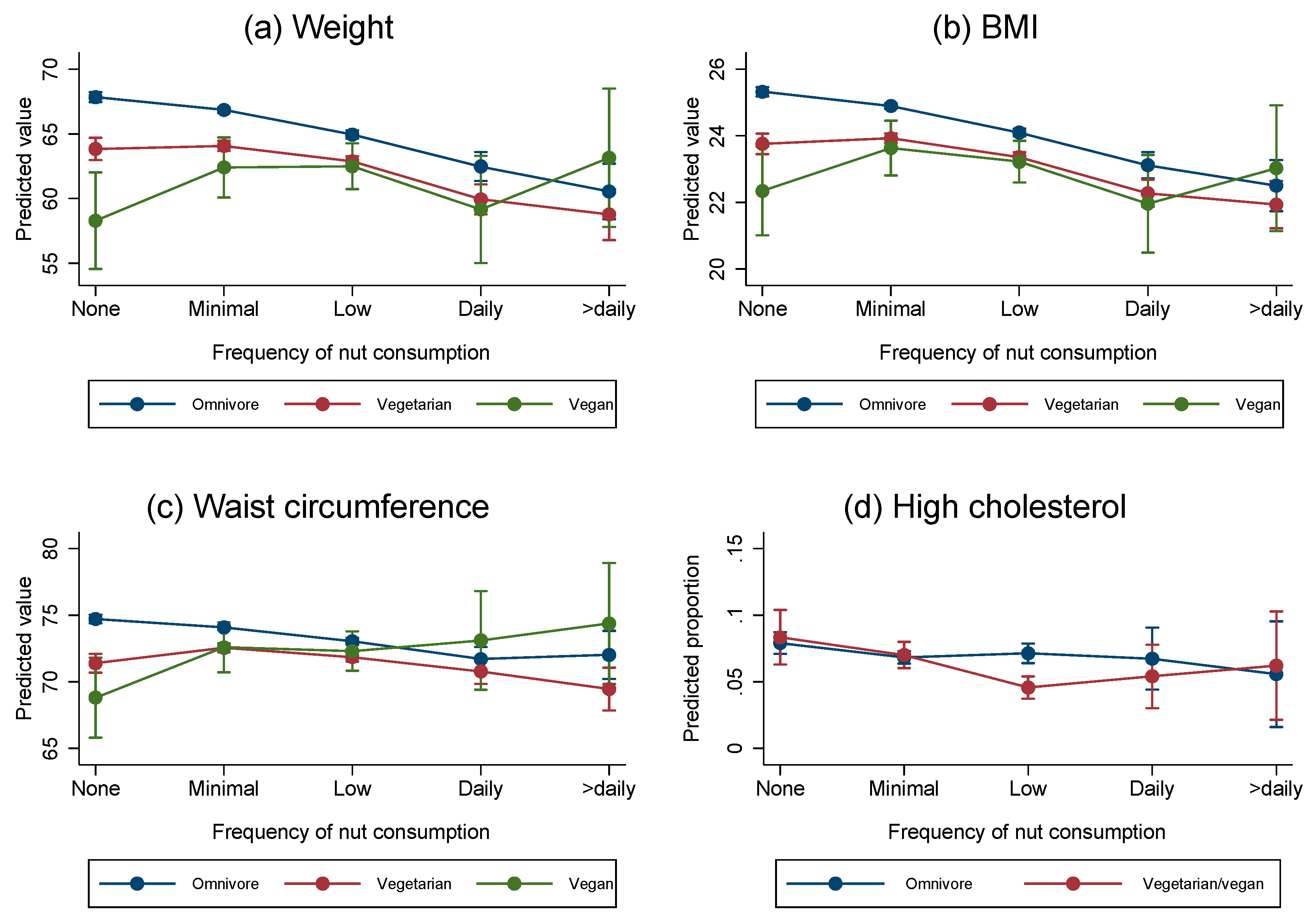
3.6. Effect Modification by Dietary Pattern
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alasalvar, C.; Bolling, B.W. Review of nut phytochemicals, fat-soluble bioactives, antioxidant components and health effects. Br. J. Nutr. 2015, 113, S68–S78. [Google Scholar] [CrossRef] [PubMed]
- Brufau, G.; Boatella, J.; Rafecas, M. Nuts: Source of energy and macronutrients. Br. J. Nutr. 2006, 96, S24–S28. [Google Scholar] [CrossRef] [PubMed]
- Ros, E. Health benefits of nut consumption. Nutrients 2010, 2, 652–682. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Han, J.; Hu, F.B.; Giovannucci, E.L.; Stampfer, M.J.; Willett, W.C.; Fuchs, C.S. Association of nut consumption with total and cause-specific mortality. N. Engl. J. Med. 2013, 369, 2001–2011. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Yang, J.; Marventano, S.; Micek, A.; Galvano, F.; Kales, S. Nut consumption and all-cause, cardiovascular, and cancer mortality risk: A systematic review and meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2015, 101, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Hshieh, T.T.; Petrone, A.B.; Gaziano, J.M.; Djousse, L. Nut consumption and risk of mortality in the Physicians’ Health Study. Am. J. Clin. Nutr. 2015, 101, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Zhang, Y.; Ding, Y.S.; Shan, Z.L.; Chen, S.J.; Yu, M.; Hu, F.B.; Liu, L.G. Nut consumption and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, A.J.; de Souza, R.J.; Meyre, D.; Anand, S.S.; Mente, A. A systematic review and meta-analysis of nut consumption and incident risk of CVD and all-cause mortality. Br. J. Nutr. 2016, 115, 212–225. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Penalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association Between Dietary Factors and Mortality From Heart Disease, Stroke, and Type 2 Diabetes in the United States. JAMA 2017, 317, 912–924. [Google Scholar] [CrossRef] [PubMed]
- Van den Brandt, P.A.; Schouten, L.J. Relationship of tree nut, peanut and peanut butter intake with total and cause-specific mortality: A cohort study and meta-analysis. Int. J. Epidemiol. 2015, 44, 1038–1049. [Google Scholar] [CrossRef] [PubMed]
- Guo, K.; Zhou, Z.; Jiang, Y.; Li, W.; Li, Y. Meta-analysis of prospective studies on the effects of nut consumption on hypertension and type 2 diabetes mellitus mamm. J. Diabetes 2015, 7, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Tang, H.; Zhao, W.; He, J. Nut intake and stroke risk: A dose-response meta-analysis of prospective cohort studies. Sci. Rep. 2016, 6, 30394. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.Q.; Tang, J.J.; Wu, H.; Xie, C.Y.; He, Z.Z. Consumption of nuts and legumes and risk of stroke: A meta-analysis of prospective cohort studies. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1262–1271. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Wang, Z.; Zhu, J.; Murad, A.L.; Prokop, L.J.; Murad, M.H. Nut consumption and risk of cancer and type 2 diabetes: A systematic review and meta-analysis. Nutr. Rev. 2015, 73, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.H.; Yu, H.B.; He, F.; Reilly, K.H.; Zliang, J.L.; Li, S.S.; Zhang, T.; Wang, B.Z.; Ding, Y.L.; Xi, B. Nut consumption in relation to cardiovascular disease risk and type 2 diabetes: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2014, 100, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Blakey, C.; Parnell, W. Patterns and predictors of nut consumption: Results from the 2008/09 New Zealand Adult Nutrition Survey. Br. J. Nutr. 2014, 112, 2028–2040. [Google Scholar] [CrossRef] [PubMed]
- Jenab, M.; Sabate, J.; Slimani, N.; Ferrari, P.; Mazuir, M.; Casagrande, C.; Deharveng, G.; Tyonneland, A.; Olsen, A.; Overvad, K.; et al. Consumption and portion sizes of tree nuts, peanuts and seeds in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohorts from 10 European countries. Br. J. Nutr. 2006, 96, S12–S23. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Keast, D.R.; Nicklas, T.A.; Fulgoni, V.L. Out-of-hand nut consumption is associated with improved nutrient intake and health risk markers in US children and adults: National Health and Nutrition Examination Survey 1999–2004. Nutr. Res. 2012, 32, 185–194. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L. Tree nut consumption is associated with better nutrient adequacy and diet quality in adults: National Health and Nutrition Examination Survey 2005–2010. Nutrients 2015, 7, 595–607. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Tree nut consumption improves nutrient intake and diet quality in US adults: An analysis of National Health and Nutrition Examination Survey (NHANES) 1999–2004. Asia Pac. J. Clin. Nutr. 2010, 19, 142–150. [Google Scholar] [PubMed]
- Fraser, G.E.; Sabate, J.; Beeson, W.L.; Strahan, T.M. A possible protective effect of nut consumption on risk of coronary heart disease. The Adventist Health Study. Arch. Intern. Med. 1992, 152, 1416–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabate, J.; Oda, K.; Ros, E. Nut consumption and blood lipid levels: A pooled analysis of 25 intervention trials. Arch. Intern. Med. 2010, 170, 821–827. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Keast, D.R.; Nicklas, T.A.; Fulgoni, V.L. Nut consumption is associated with decreased health risk factors for cardiovascular disease and metabolic syndrome in U.S. adults: NHANES 1999–2004. J. Am. Coll. Nutr. 2011, 30, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Parnell, W. Association of Nut Consumption with Cardiometabolic Risk Factors in the 2008/2009 New Zealand Adult Nutrition Survey. Nutrients 2015, 7, 7523–7542. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.A.; Howe, P.R.; Buckley, J.D.; Bryan, J.; Coates, A.M. Nut consumption for vascular health and cognitive function. Nutr. Res. Rev. 2014, 27, 131–158. [Google Scholar] [CrossRef] [PubMed]
- Blanco Mejia, S.; Kendall, C.W.; Viguiliouk, E.; Augustin, L.S.; Ha, V.; Cozma, A.I.; Mirrahimi, A.; Maroleanu, A.; Chiavaroli, L.; Leiter, L.A.; et al. Effect of tree nuts on metabolic syndrome criteria: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2014, 4, e004660. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Falk, M.C.; Feldman, R.; Lewis, K.; Mozaffarian, D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: Systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am. J. Clin. Nutr. 2015, 102, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Mohammadifard, N.; Salehi-Abarghouei, A.; Salas-Salvado, J.; Guasch-Ferre, M.; Humphries, K.; Sarrafzadegan, N. The effect of tree nut, peanut, and soy nut consumption on blood pressure: A systematic review and meta-analysis of randomized controlled clinical trials. Am. J. Clin. Nutr. 2015, 101, 966–982. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Sabate, J.; Gomez-Gracia, E.; Alonso, A.; Martinez, J.A.; Martinez-Gonzalez, M.A. Nut consumption and weight gain in a Mediterranean cohort: The SUN Study. Obesity 2007, 15, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Wedick, N.M.; Martinez-Gonzalez, M.A.; Li, T.Y.; Sampson, L.; Hu, F.B. Prospective study of nut consumption, long-term weight change, and obesity risk in women. Am. J. Clin. Nutr. 2009, 89, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.L.; Hu, F.B. Long-term associations of nut consumption with body weight and obesity. Am. J. Clin. Nutr. 2014, 100, 408S–411S. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Nut consumption, weight gain and obesity: Epidemiological evidence. Nutr. Metab. Cardiovasc. Dis. 2011, 21, S40–S45. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Dhillon, J.; Mattes, R.D. A review of the effects of nuts on appetite, food intake, metabolism, and body weight. Am. J. Clin. Nutr. 2014, 100, 412S–422S. [Google Scholar] [CrossRef] [PubMed]
- Alper, C.M.; Mattes, R.D. Effects of chronic peanut consumption on energy balance and hedonics. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mateo, G.; Rojas-Rueda, D.; Basora, J.; Ros, E.; Salas-Salvadó, J. Nut intake and adiposity: Meta-analysis of clinical trials. Am. J. Clin. Nutr. 2013, 97, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Hollis, J.; Mattes, R. Effect of chronic consumption of almonds on body weight in healthy humans. Br. J. Nutr. 2007, 98, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Mattes, R.D.; Kris-Etherton, P.M.; Foster, G.D. Impact of peanuts and tree nuts on body weight and healthy weight loss in adults. J. Nutr. 2008, 138, S1741–S1745. [Google Scholar]
- Tey, S.L.; Brown, R.; Gray, A.; Chisholm, A.; Delahunty, C. Nuts improve diet quality compared to other energy-dense snacks while maintaining body weight. J. Nutr. Metab. 2011, 2011, 357350. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.E.; Burley, V.J.; Greenwood, D.C.; UK Women’s Cohort Study Steering Group. The UK Women’s Cohort Study: Comparison of vegetarians, fish-eaters and meat-eaters. Public Health Nutr. 2004, 7, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Spence, M.; Cade, J.; Burley, V.; Greenwood, D. Ability of the UK Women’s Cohort food frequency questionnaire to rank dietary intakes: A preliminary validation study. Proc. Nutr. Soc. 2002, 61, 117. [Google Scholar]
- Tey, S.; Brown, R.; Chisholm, A. Nuts and Heart Health. National Heart Foundation of New Zealand Evidence-Based Position Statement on the Relationship of Nuts to Heart Health; National Heart Foundation of New Zealand: Auckland, New Zealand, 2012.
- Cade, J.E.; Burley, V.J.; Alwan, N.A.; Hutchinson, J.; Hancock, N.; Morris, M.A.; Threapleton, D.E.; Greenwood, D.C. Cohort Profile: The UK Women’s Cohort Study (UKWCS). Int. J. Epidemiol. 2017, 46, e11. [Google Scholar] [CrossRef] [PubMed]
- Pawlak, R.; Colby, S.; Herring, J. Beliefs, benefits, barriers, attitude, intake and knowledge about peanuts and tree nuts among WIC participants in eastern North Carolina. Nutr. Res. Pract. 2009, 3, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Brennan, A.M.; Sweeney, L.L.; Liu, X.; Mantzoros, C.S. Walnut consumption increases satiation but has no effect on insulin resistance or the metabolic profile over a 4-day period. Obesity 2010, 18, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Mattes, R.D. Appetitive, dietary and health effects of almonds consumed with meals or as snacks: A randomized, controlled trial. Eur. J. Clin. Nutr. 2013, 67, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Alper, C.M.; Mattes, R.D. Peanut consumption improves indices of cardiovascular disease risk in healthy adults. J. Am. Coll. Nutr. 2003, 22, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Claesson, A.-L.; Holm, G.; Ernersson, Ã.; Lindström, T.; Nystrom, F.H. Two weeks of overfeeding with candy, but not peanuts, increases insulin levels and body weight. Scand. J. Clin. Lab. Investig. 2009, 69, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Coelho, S.B.; de Sales, R.L.; Iyer, S.S.; Bressan, J.; Costa, N.M.B.; Lokko, P.; Mattes, R. Effects of peanut oil load on energy expenditure, body composition, lipid profile, and appetite in lean and overweight adults. Nutrition 2006, 22, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Ellis, P.R.; Kendall, C.W.C.; Ren, Y.; Parker, C.; Pacy, J.F.; Waldron, K.W.; Jenkins, D.J.A. Role of cell walls in the bioaccessibility of lipids in almond seeds. Am. J. Clin. Nutr. 2004, 80, 604–613. [Google Scholar] [PubMed]
- Grundy, M.; Grassby, T.; Mandalari, G.; Waldron, K.; Butterworth, P.; Berry, S.; Ellis, P. Effect of mastication on lipid bioaccessibility of almonds in a randomized human study and its implications for digestion kinetics, metabolizable energy, and postprandial lipemia. Am. J. Clin. Nutr. 2015, 101, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novotny, J.A.; Gebauer, S.K.; Baer, D.J. Discrepancy between the Atwater factor predicted and empirically measured energy values of almonds in human diets. Am. J. Clin. Nutr. 2012, 96, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Mozaffarian, D. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Lovejoy, J.C. The influence of dietary fat on insulin resistance. Curr. Diabetes Rep. 2002, 2, 435–440. [Google Scholar] [CrossRef]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Parnell, W. Nut consumption is associated with better nutrient intakes: Results from the 2008/09 New Zealand Adult Nutrition Survey. Br. J. Nutr. 2016, 115, 105–112. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.; Blumberg, J.; Ingwersen, L.; Jenab, M.; Tucker, K.L. Tree nuts and peanuts as components of a healthy diet. J. Nutr. 2008, 138, S1736–S1740. [Google Scholar]
- Griel, A.E.; Eissenstat, B.; Juturu, V.; Hsieh, G.; Kris-Etherton, P.M. Improved diet quality with peanut consumption. J. Am. Coll. Nutr. 2004, 23, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Jaceldo-Siegl, K.; Joan, S.; Rajaram, S.; Fraser, G.E. Long-term almond supplementation without advice on food replacement induces favourable nutrient modifications to the habitual diets of free-living individuals. Br. J. Nutr. 2004, 92, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Aranceta, J.; Rodrigo, C.P.; Naska, A.; Vadillo, V.R.; Trichopoulou, A. Nut consumption in Spain and other countries. Br. J. Nutr. 2006, 96, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.A.; Howe, P.R.; Buckley, J.D.; Wright, G.C.; Bryan, J.; Coates, A.M. Lower energy intake following consumption of Hi-oleic and regular peanuts compared with iso-energetic consumption of potato crisps. Appetite 2014, 82, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Hu, F.B.; Ros, E.; Sabate, J. The role of tree nuts and peanuts in the prevention of coronary heart disease: Multiple potential mechanisms. J. Nutr. 2008, 138, S1746–S1751. [Google Scholar]
- Luu, H.N.; Blot, W.J.; Xiang, Y.B.; Cai, H.; Hargreaves, M.K.; Li, H.; Yang, G.; Signorello, L.; Gao, Y.T.; Zheng, W.; et al. Prospective evaluation of the association of nut/peanut consumption with total and cause-specific mortality. JAMA Intern. Med. 2015, 175, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Nouran, M.G.; Kimiagar, M.; Abadi, A.; Mirzazadeh, M.; Harrison, G. Peanut consumption and cardiovascular risk. Public Health Nutr. 2010, 13, 1581–1586. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.J. Nutrition concerns and health effects of vegetarian diets. Nutr. Clin. Pract. 2010, 25, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Messina, V.; Melina, V.; Mangels, A.R. A new food guide for North American vegetarians. J. Am. Diet. Assoc. 2003, 103, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Kaaks, R.; Riboli, E. Validation and calibration of dietary intake measurements in the EPIC project: Methodological considerations. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, S15–S25. [Google Scholar] [CrossRef] [PubMed]
- White, E.; Kushi, L.H.; Pepe, M.S. The effect of exposure variance and exposure measurement error on study sample size: Implications for the design of epidemiologic studies. J. Clin. Epidemiol. 1994, 47, 873–880. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Variable | All Participants * (n = 34,831) | Non-Nut Consumers (n = 5631) | Nut Consumers (n = 29,200) |
|---|---|---|---|
| Age (years) a | 52.2 (9.3) | 55.5 (9.6) | 51.6 (9.1) |
| Height (cm) a | 163.7 (6.8) | 163.1 (6.8) | 163.8 (6.7) |
| Weight (kg) a | 65.6 (11.9) | 67.4 (13.2) | 65.3 (11.6) |
| BMI (kg/m2) a | 24.5 (4.3) | 25.3 (4.7) | 24.3 (4.1) |
| Waist circumference (cm) a | 73.6 (9.3) | 75.0 (10.3) | 73.3 (9.0) |
| Physical activity b | |||
| None | 42.2 (13,934) | 52.9 (2769) | 40.2 (11,165) |
| <75 min/week | 20.0 (6606) | 14.1 (738) | 21.1 (5868) |
| 75 min/week or more | 37.7 (12,448) | 33.0 (1725) | 38.6 (10,723) |
| Ethnicity b | |||
| White | 96.0 (33,432) | 95.9 (5400) | 96.0 (28,032) |
| Asia | 0.5 (188) | 0.1 (8) | 0.6 (180) |
| Black | 0.1 (50) | 0.1 (6) | 0.2 (44) |
| Other | 3.3 (1161) | 3.9 (217) | 3.2 (944) |
| Employment b | |||
| Professional | 24.7 (8590) | 18.2 (1024) | 25.9 (7566) |
| Managerial, technical, admin | 28.7 (9994) | 23.9 (1346) | 29.6 (8648) |
| Clerical/Skilled | 41.2 (14,338) | 49.0 (2760) | 39.7 (11,578) |
| Manual | 1.0 (344) | 1.6 (89) | 0.9 (255) |
| Other/missing/no job | 4.5 (1565) | 7.3 (412) | 4.0 (1153) |
| Highest educational achievement b | |||
| No qualifications | 16.8 (5347) | 30.2 (1507) | 14.3 (3840) |
| O-level (16 years) | 31.2 (9940) | 33.8 (1688) | 30.7 (8252) |
| A-level (18 years) | 24.7 (7859) | 20.2 (1009) | 25.5 (6850) |
| Degree | 27.4 (8718) | 15.9 (794) | 29.5 (7924) |
| Dietary pattern b | |||
| Omnivore | 72.1 (25,116) | 83.1 (4679) | 70.0 (20,437) |
| Vegetarian | 26.6 (9280) | 16.1 (905) | 28.7 (8375) |
| Vegan | 1.3 (435) | 0.8 (47) | 1.3 (388) |
| Energy intake (kJ/day) a | 9817 (2986) | 9029 (2954) | 9969 (2986) |
| Alcohol | |||
| consume any alcohol b | 89.6 (29,848) | 80.4 (4302) | 91.3 (25,546) |
| g/day among alcohol consumers c | 6.7 (11.8) | 4.1 (10.1) | 7.0 (12.1) |
| Smoking status b | |||
| Never smoked | 57.9 (19,535) | 58.8 (3186) | 57.7 (16,349) |
| Current smoker | 11.1 (3739) | 12.1 (657) | 10.9 (3082) |
| Former smoker | 31.1 (10,486) | 29.1 (1580) | 31.4 (8906) |
| Menopausal status b | |||
| Premenopausal | 47.6 (15,859) | 33.0 (1768) | 50.4 (14,091) |
| Postmenopausal | 52.4 (17,462) | 67.0 (3586) | 49.6 (13,876) |
| Current HRT use (%) b | 23.2 (7539) | 23.1 (1195) | 23.2 (6344) |
| Current OCP use (%) b | 3.9 (1294) | 3.2 (166) | 4.1 (1128) |
| Age of menarche (year) a | 12.8 (1.6) | 12.8 (1.7) | 12.8 (1.6) |
| Parity b | |||
| no children | 13.6 (4258) | 13.3 (667) | 13.7 (3591) |
| 1–2 children | 65.9 (17,775) | 55.6 (2790) | 57.2 (14,985) |
| 3–4 children | 27.1 (8449) | 27.9 (1399) | 26.9 (7050) |
| ≥5 children | 2.3 (724) | 3.2 (162) | 2.2 (562) |
| Demographic Variable | Total Nut Consumption | Unadjusted OR † | Unadjusted p-Value | Adjusted OR †,‡ | Adjusted p-Value ‡ | ||||
|---|---|---|---|---|---|---|---|---|---|
| No Nuts (n = 5631) | <Once per Week (n = 17,992) | 2–6 Times per Week (n = 9887) | Daily (n = 995) | >Daily (n = 326) | |||||
| Age (years) OR per 5 years 1 | 55.5 (55.3, 55.8) | 51.8 (51.7, 52.0) | 51.0 (50.8, 51.2) | 53.3 (52.7, 53.9) | 54.1 (53.1, 55.2) | <0.001 | <0.001 | ||
| OR for 50 vs. 40 | 0.84 (0.83, 0.85) | 0.95 (0.93, 0.97) | |||||||
| OR for 60 vs. 40 | 0.65 (0.63, 0.67) | 0.88 (0.84, 0.92) | |||||||
| OR for 70 vs. 40 | 0.45 (0.42, 0.48) | 0.79 (0.73, 0.86) | |||||||
| Physical activity 2 | |||||||||
| None | 52.9 (2769) | 42.5 (7262) | 36.4 (3436) | 36.6 (348) | 38.8 (119) | 1.00 a | <0.001 | 1.00 a | <0.001 |
| <75 min/week | 14.1 (738) | 20.8 (3543) | 21.8 (2054) | 21.7 (206) | 21.2 (65) | 1.54 (1.45, 1.62) b | 1.31 (1.24, 1.40) b | ||
| 75 min/week or more | 33.0 (1725) | 36.7 (6264) | 41.8 (3940) | 41.7 (396) | 40.1 (123) | 1.47 (1.41, 1.54) b | 1.29 (1.23, 1.36) b | ||
| Employment 2 | <0.001 | <0.001 | |||||||
| Professional | 18.2 (1024) | 24.3 (4370) | 28.3 (2794) | 32.5 (323) | 24.2 (79) | 1.00 a | 1.00 a | ||
| Managerial, technical, admin | 23.9 (1346) | 28.5 (5133) | 31.7 (3138) | 29.0 (289) | 27.0 (88) | 0.90 (0.85, 0.95) b | 1.12 (1.05, 1.19) b | ||
| Clerical/Skilled | 49.0 (2760) | 42.1 (7580) | 35.6 (3514) | 34.4 (342) | 43.6 (142) | 0.63 (0.60, 0.66) c | 1.01 (0.94, 1.08) a | ||
| Manual | 1.6 (89) | 1.0 (183) | 0.7 (67) | 0.2 (2) | 0.9 (3) | 0.42 (0.35, 0.52) d | 0.87 (0.68, 1.10) a,b | ||
| other/missing/no job | 7.3 (412) | 4.0 (726) | 3.8 (374) | 3.9 (39) | 14 (4.3%) | 0.51 (0.46, 0.56) d | 0.91 (0.80, 1.04) a | ||
| Highest educational achievement (%) 2 | <0.001 | <0.001 | |||||||
| no qualifications | 30.2 (1507) | 16.1 (2656) | 11.0 (1008) | 13.0 (120) | 18.4 (56) | 1.00 a | 1.00 a | ||
| O-level (16 years) | 33.8 (1688) | 32.8 (5404) | 27.5 (2529) | 25.4 (234) | 28.0 (85) | 1.66 (1.55, 1.77) b | 1.41 (1.31, 1.52) b | ||
| A-level (18 years) | 20.2 (1009) | 24.9 (4092) | 26.7 (2456) | 24.5 (226) | 25.0 (76) | 2.24 (2.09, 2.39) c | 1.87 (1.73, 2.03) c | ||
| Degree | 15.9 (794) | 26.2 (4302) | 34.8 (3194) | 37.0 (341) | 28.6 (87) | 2.98 (2.78, 3.18) d | 2.26 (2.07, 2.46) d | ||
| Dietary status 2 | <0.001 | <0.001 | |||||||
| Omnivore | 83.1 (4679) | 77.4 (13,931) | 59.3 (5861) | 50.9 (506) | 42.6 (139) | 1.00 a | 1.00 a | ||
| Vegetarian | 16.1 (905) | 21.9 (3932) | 38.7 (3823) | 45.7 (455) | 50.6 (165) | 2.51 (2.40, 2.63) b | 2.23 (2.12, 2.35) b | ||
| Vegan | 0.8 (47) | 0.7 (12) | 2.1 (203) | 3.4 (34) | 6.8 (22) | 4.06 (3.36, 4.89) c | 3.76 (3.05, 4.64) c | ||
| Energy intake (kJ/day) 1 | 9029 (8952, 9107) | 9474 (9434, 9514) | 10,565 (10,505, 10,642) | 11,819 (11,610, 12,028) | 13,596 (13,170, 14,022) | <0.001 | |||
| OR for 4 MJ vs. 10 MJ | 0.31 (0.29, 0.32) | ||||||||
| OR for 6 MJ vs. 10 MJ | 0.49 (0.47, 0.50) | ||||||||
| OR for 8 MJ vs. 10 MJ | 0.71 (0.70, 0.72) | ||||||||
| OR for 12 MJ vs. 10 MJ | 1.36 (1.34, 1.38) | ||||||||
| OR for 14 MJ vs. 10 MJ | 1.80 (1.75, 1.85) | ||||||||
| OR for 16 MJ vs. 10 MJ | 2.34 (2.25, 2.43) | ||||||||
| Smoking status 2 | |||||||||
| Never smoked | 58.8 (3186) | 57.9 (10,132) | 57.2 (5482) | 57.3 (545) | 61.5 (190) | 1.00 a | <0.001 | 1.00 a | <0.001 |
| Current smoker | 12.1 (657) | 11.0 (1928) | 10.8 (1034) | 9.8 (93) | 8.7 (27) | 0.94 (0.88, 1.00) a | 0.98 (0.91, 1.05) a | ||
| Former smoker | 29.1 (1580) | 31.0 (5430) | 32.0 (3071) | 32.9 (313) | 29.8 (92) | 1.07 (1.02, 1.12) b | 1.07 (1.02, 1.12) b | ||
| Anthropometry Variable | Total Nut Consumption | p for Linear Trend Unadjusted † | p for Linear Trend Adjusted †,‡ | p for Linear trend Further Adjusted for Energy Intake †,‡ | |||||
|---|---|---|---|---|---|---|---|---|---|
| All Participants (n = 34,831) | No Nuts (n = 5631) | <Once per Week (n = 17,992) | 2–6 Times per Week (n = 9887) | Daily (n = 995) | >Daily (n = 326) | ||||
| Weight (kg) | 65.6 (65.5, 65.7) | 67.4 (67.1, 67.8) | 66.2 (66.0, 66.4) | 64.0 (63.8, 64.3) | 61.7 (63.8, 64.3) | 60.6 (59.5, 61.7) | <0.001 § | <0.001 § | <0.001 § |
| BMI (kg/m2) | 24.5 (24.4, 24.5) | 25.3 (25.2, 25.4) | 24.7 (24.7, 24.8) | 23.7 (23.6, 23.9) | 22.8 (22.6, 23.1) | 22.5 (22.2, 22.9) | <0.001 § | <0.001 § | <0.001 § |
| Waist circumference (cm) | 73.6 (73.5, 73.7) | 75.0 (74.7, 75.3) | 73.8 (73.6, 74.0) | 72.5 (72.3, 72.7) | 72.2 (71.6, 72.8) | 72.1 (71.1, 73.2) | <0.001 § | <0.001 | <0.001 § |
| Disease/Risk Factor Variable | Total Nut Consumption | p for Linear Trend † | ||||
|---|---|---|---|---|---|---|
| No Nuts (n = 5631) | <Once per Week (n = 17,992) | 2–6 Times per Week (n = 9887) | Daily (n = 995) | >Daily (n = 326) | ||
| High Blood Pressure | ||||||
| Cases | 1190 | 2945 | 1329 | 144 | 44 | |
| Unadjusted | 1.00 | 0.70 (0.65, 0.75) | 0.55 (0.51, 0.60) | 0.60 (0.5, 0.73) | 0.54 (0.40, 0.76) | <0.001 |
| Adjusted for age only | 1.00 | 0.86 (0.80, 0.93) | 0.71 (0.65, 0.78) | 0.68 (0.56, 0.83) | 0.57 (0.41, 0.80) | <0.001 |
| Adjusted ‡ | 1.00 | 0.85 (0.78, 0.93) | 0.75 (0.67, 0.83) | 0.72 (0.58, 0.90) | 0.69 (0.48, 0.98) | <0.001 |
| Further adjusted for BMI | 1.00 | 0.86 (0.78, 0.93) | 0.82 (0.74, 0.91) | 0.90 (0.72, 1.12) | 0.92 (0.63, 1.34) | 0.010 |
| High cholesterol | ||||||
| Cases | 547 | 1261 | 564 | 58 | 20 | |
| Unadjusted ‡ | 1.00 | 0.66 (0.60, 0.74) | 0.53 (0.47, 0.60) | 0.54 (0.41, 0.72) | 0.57 (0.36, 0.90) | <0.001 |
| Adjusted for age only | 1.00 | 0.87 (0.78, 0.97) | 0.73 (0.64, 0.83) | 0.63 (0.47, 0.83) | 0.62 (0.38, 0.99) | <0.001 |
| Adjusted ‡ | 1.00 | 0.84 (0.74, 0.95) | 0.75 (0.65, 0.87) | 0.70 (0.51, 0.96) | 0.67 (0.40, 1.14) | <0.001 |
| Further adjusted for BMI | 1.00 | 0.85 (0.75, 0.96) | 0.78 (0.67, 0.91) | 0.78 (0.57, 1.08) | 0.76 (0.44, 1.32) | 0.004 |
| Heart Attack | ||||||
| Cases | 151 | 212 | 101 | 17 | 2 | |
| Unadjusted | 1.00 | 0.41 (0.33, 0.51) | 0.35 (0.27, 0.46) | 0.59 (0.36, 0.99) | 0.21 (0.05, 0.86) | <0.001 |
| Adjusted for age only | 1.00 | 0.59 (0.47, 0.73) | 0.55 (0.42, 0.72) | 0.73 (0.44, 1.22) | 0.23 (0.06, 0.94) | <0.001 |
| Adjusted ‡ | 1.00 | 0.56 (0.44, 0.72) | 0.51 (0.37, 0.69) | 0.70 (0.38, 1.26) | 0.28 (0.07, 1.15) | <0.001 |
| Further adjusted for BMI | 1.00 | 0.56 (0.44, 0.72) | 0.55 (0.40, 0.75) | 0.82 (0.45, 1.49) | 0.36 (0.09, 1.51) | 0.011 |
| Angina | ||||||
| Cases | 206 | 314 | 144 | 20 | 9 | |
| Unadjusted | 1.00 | 0.44 (0.37, 0.53) | 0.37 (0.30, 0.46) | 0.51 (0.32, 0.81) | 0.70 (0.25, 1.37) | <0.001 |
| Adjusted for age only | 1.00 | 0.65 (0.54, 0.79) | 0.60 (0.48, 0.74) | 0.63 (0.39, 1.01) | 0.78 (0.39, 1.55) | <0.001 |
| Adjusted ‡ | 1.00 | 0.64 (0.51, 0.79) | 0.63 (0.48, 0.82) | 0.64 (0.36, 1.12) | 0.85 (0.38, 1.88) | 0.016 |
| Further adjusted for BMI | 1.00 | 0.65 (0.52, 0.82) | 0.67 (0.51, 0.88) | 0.74 (0.41, 1.30) | 0.95 (0.40, 2.22) | 0.092 § |
| Stroke | ||||||
| Cases | 79 | 109 | 51 | 10 | 4 | |
| Unadjusted | 1.00 | 0.41 (0.30, 0.54) | 0.34 (0.24, 0.49) | 0.67 (0.35, 1.30) | 0.82 (0.30, 2.25) | <0.001 |
| Adjusted for age only | 1.00 | 0.55 (0.41, 0.74) | 0.51 (0.35, 0.73) | 0.79 (0.41, 1.54) | 0.89 (0.32, 2.48) | 0.023 |
| Adjusted ‡ | 1.00 | 0.62 (0.44, 0.87) | 0.54 (0.36, 0.83) | 0.89 (0.42, 1.91) | 1.31 (0.46, 3.71) | 0.115 § |
| Further adjusted for BMI | 1.00 | 0.61 (0.43, 0.86) | 0.56 (0.36, 0.86) | 0.94 (0.44, 2.02) | 1.48 (0.52, 4.21) | 0.201 § |
| Diabetes | ||||||
| Cases | 197 | 297 | 119 | 12 | 5 | |
| Unadjusted | 1.00 | 0.44 (0.37, 0.53) | 0.32 (0.25, 0.40) | 0.32 (0.18, 0.57) | 0.40 (0.16, 0.99) | <0.001 |
| Adjusted for age only | 1.00 | 0.54 (0.45, 0.66) | 0.41 (0.32, 0.52) | 0.35 (0.20, 0.65) | 0.44 (0.18, 1.07) | <0.001 |
| Adjusted ‡ | 1.00 | 0.58 (0.47, 0.72) | 0.46 (0.35, 0.60) | 0.57 (0.31, 1.04) | 0.54 (0.20, 1.50) | <0.001 |
| Further adjusted for BMI | 1.00 | 0.61 (0.48, 0.76) | 0.54 (0.40, 0.72) | 0.79 (0.43, 1.44) | 0.89 (0.32, 2.46) | 0.008 |
| Gallstones | ||||||
| Cases | 440 | 931 | 391 | 48 | 13 | |
| Unadjusted | 1.00 | 0.61 (0.54, 0.69) | 0.46 (0.40, 0.53) | 0.56 (0.41, 0.76) | 0.46 (0.26, 0.80) | <0.001 |
| Adjusted for age only | 1.00 | 0.73 (0.65, 0.83) | 0.58 (0.50, 0.66) | 0.59 (0.43, 0.81) | 0.49 (0.28, 0.86) | <0.001 |
| Adjusted ‡ | 1.00 | 0.77 (0.67, 0.88) | 0.64 (0.55, 0.76) | 0.73 (0.52, 1.03) | 0.46 (0.24, 0.92) | <0.001 |
| Further adjusted for BMI | 1.00 | 0.78 (0.68, 0.90) | 0.70 (0.59, 0.83) | 0.85 (0.60, 1.22) | 0.63 (0.32, 1.25) | 0.002 |
| Polyps | ||||||
| Cases | 85 | 172 | 93 | 4 | 4 | |
| Unadjusted | 1.00 | 0.60 (0.46, 0.77) | 0.58 (0.43, 0.78) | 0.25 (0.09, 0.67) | 0.76 (0.28, 2.07) | 0.001 |
| Adjusted for age only | 1.00 | 0.78 (0.60, 1.02) | 0.80 (0.59, 1.09) | 0.29 (0.10, 0.78) | 0.62 (0.19, 1.97) | 0.028 |
| Adjusted ‡ | 1.00 | 0.80 (0.58, 1.09) | 0.83 (0.58, 1.19) | 0.31 (0.10, 0.99) | 0.85 (0.26, 2.79) | 0.119 |
| Further adjusted for BMI | 1.00 | 0.81 (l.59, 1.11) | 0.85 (0.59, 1.24) | 0.34 (0.11, 1.09) | 1.01 (0.31, 3.33) | 0.206 |
| Cancer | ||||||
| Cases | 463 | 1175 | 671 | 72 | 20 | |
| Unadjusted | 1.00 | 0.74 (0.66, 0.83) | 0.77 (0.68, 0.87) | 0.81 (0.63, 1.05) | 0.68 (0.43, 1.09) | 0.003 |
| Adjusted for age only | 1.00 | 0.89 (0.80, 1.00) | 0.98 (0.86, 1.11) | 0.91 (0.70, 1.19) | 0.66 (0.40, 1.07) | 0.632 § |
| Adjusted ‡ | 1.00 | 1.01 (0.88, 1.15) | 1.13 (0.97, 1.31) | 0.95 (0.70, 1.29) | 0.78 (0.46, 1.34) | 0.366 |
| Further adjusted for BMI | 1.00 | 1.01 (0.88, 1.16) | 1.15 (0.98, 1.33) | 0.94 (0.68, 1.28) | 0.84 (0.49, 1.44) | 0.267 |
| Nutrient | Total Nut Consumption | p for Linear Trend Unadjusted †,‡ | p for Linear Trend Adjusted †,‡ | p for Linear Trend Further Adjusted for Energy Intake †,‡ | |||||
|---|---|---|---|---|---|---|---|---|---|
| All Participants (n = 34,831) | No Nuts (n = 5631) | <Once per Week (n = 17,992) | 2–6 Times per Week (n = 9887) | Daily (n = 995) | >Daily (n = 326) | ||||
| Total energy (kJ) | 9817 (9786, 9849) | 9029 (8952, 9107) | 9474 (9434, 9514) | 10,565 (10,504, 10,624) | 11,819 (11,610, 12,028) | 13,596 (13,169, 14,023) | <0.001 § | <0.001§ | |
| Total fat (g) | 84.7 (84.4, 85.0) | 73.3 (72.5, 74.1) | 80.3 (79.9, 80.8) | 94.4 (93.8, 95.1) | 112.3 (110.0, 114.6) | 142.7 (137.2, 148.2) | <0.001 § | <0.001 § | |
| %TE | 32.4 (32.4, 32.5) | 30.5 (30.3, 30.6) | 32.0 (31.9, 32.1) | 33.7 (33.6, 33.8) | 35.9 (35.5, 36.2) | 39.5 (38.8, 40.3) | <0.001 § | <0.001 § | |
| Saturated fat (g) | 29.3 (29.2, 29.4) | 26.5 (26.1, 26.8) | 28.5 (28.3, 28.7) | 31.7 (31.4, 31.9) | 33.8 (32.8, 34.7) | 37.4 (35.6, 39.2) | <0.001 § | <0.001 § | |
| %TE | 11.1 (11.1, 11.1) | 10.9 (10.8, 11.0) | 11.2 (11.2, 11.2) | 11.2 (11.1, 11.2) | 10.6 (10.4, 10.8) | 10.3 (9.9, 10.6) | 0.938 § | <0.001 § | |
| Monounsaturated fat (g) | 27.7 (27.6, 27.8) | 23.4 (23.1, 23.6) | 26.0 (25.9, 26.1) | 31.2 (31.0, 31.4) | 39.0 (38.2, 39.7) | 52.9 (50.7, 55.2) | <0.001 § | <0.001 § | |
| %TE | 10.5 (10.5, 10.6) | 9.7 (9.6, 9.7) | 10.3 (10.3, 10.3) | 11.1 (11.1, 11.2) | 12.5 (12.3, 12.6) | 14.7 (14.3, 15.1) | <0.001 § | <0.001 § | |
| Polyunsaturated fat (g) | 16.3 (16.2, 16.4) | 13.4 (13.2, 13.6) | 15.0 (14.9, 15.1) | 18.8 (18.6, 18.9) | 25.0 (24.5, 25.5) | 36.2 (34.6, 37.8) | <0.001 § | <0.001 § | |
| %TE | 6.2 (6.2, 6.2) | 5.6 (5.5, 5.6) | 6.0 (6.0, 6.0) | 6.7 (6.7, 6.8) | 8.1 (8.0, 8.2) | 10.1 (9.8, 10.4) | <0.001 § | <0.001 § | |
| Protein (g) | 89.3 (89.0, 89.6) | 87.5 (86.8, 88.2) | 87.7 (87.3, 88.1) | 91.5 (91.0, 92.1) | 98.1 (96.2, 100.0) | 110.1 (106.4, 113.9) | <0.001 § | <0.001 § | |
| %TE | 15.1 (15.0, 15.1) | 16.1 (16.0, 16.2) | 15.3 (15.2, 15.3) | 14.3 (14.3, 14.4) | 13.8 (13.7, 13.9) | 13.5 (13.3, 13.8) | <0.001 § | <0.001 § | |
| Carbohydrate (g) | 313 (312, 314) | 297 (294, 300) | 303 (302, 305) | 322 (330, 335) | 365 (358, 372) | 394 (379, 409) | <0.001 § | <0.001 § | |
| %TE | 52.6 (52.6, 52.7) | 54.2 (54.0, 54.4) | 52.7 (52.6, 52.8) | 51.9 (51.8, 52.1) | 51.0 (50.6, 51.4) | 48.2 (47.3, 49.1) | <0.001 § | <0.001 § | |
| Sugar (g) | 149 (148, 149) | 142 (140, 144) | 143 (142, 144) | 157 (156, 159) | 180 (176, 185) | 199 (189, 208) | <0.001 § | <0.001 § | |
| %TE | 25.2 (25.2, 25.3) | 26.2 (26.0, 26.4) | 25.1 (25.1, 25.2) | 24.8 (24.7, 24.9) | 25.5 (25.1, 25.9) | 24.3 (23.5, 25.0) | <0.001 § | <0.001 § | |
| Fibre (g) | 25.6 (25.5, 25.7) | 23.6 (23.3, 23.9) | 24.3 (24.1, 24.4) | 28.0 (27.8, 28.2) | 33.1 (32.3, 33.8) | 39.5 (37.7, 41.3) | <0.001 § | <0.001 § | 0.002 § |
| Vitamin A (μg) | 1243 (1236, 1249) | 1175 (1158, 1192) | 1219 (1210, 1227) | 1303 (1291, 1314) | 1390 (1349, 1431) | 1477 (1382, 1572) | <0.001 § | <0.001 § | 0.340 § |
| Thiamin (mg) | 3.13 (3.10, 3.15) | 2.79 (2.72, 2.85) | 2.94 (2.90, 2.97) | 3.54 (3.48, 3.59) | 3.94 (3.76, 4.13) | 4.65 (4.28, 5.03) | <0.001 § | <0.001 § | <0.001 |
| Riboflavin (mg) | 2.52 (2.51, 2.53) | 2.48 (2.46, 2.50) | 2.47 (2.46, 2.48) | 2.58 (2.56, 2.60) | 2.75 (2.69, 2.81) | 2.94 (2.81, 3.06) | <0.001 § | <0.001 § | <0.001 § |
| Vitamin B6 (mg) | 2.82 (2.81, 2.83) | 2.77 (2.74, 2.79) | 2.75 (2.74, 2.76) | 2.92 (2.90, 2.94) | 3.19 (3.13, 3.25) | 3.62 (3.48, 3.75) | <0.001 § | <0.001 § | <0.001 § |
| Vitamin B12 (μg) | 5.69 (5.66, 5.72) | 5.93 (5.85, 6.01) | 5.80 (5.75, 5.84) | 5.44 (5.37, 5.50) | 5.21 (4.99, 5.43) | 4.76 (4.38, 5.15) | <0.001 § | <0.001 § | <0.001 § |
| Folate (μg) | 402 (401, 403) | 384 (381, 388) | 388 (386, 389) | 426 (423, 429) | 476 (466, 485) | 550 (527, 573) | <0.001 § | <0.001 § | <0.001 § |
| Vitamin C (mg) | 171 (170, 172) | 160 (158, 163) | 164 (163, 165) | 185 (184, 187) | 206 (200, 212) | 230 (213, 246) | <0.001 § | <0.001 § | 0.664 § |
| Vitamin E (mg) | 9.71 (9.66, 9.75) | 8.19 (8.09, 8.29) | 9.01 (8.96, 9.07) | 11.09 (11.01, 11.18) | 14.14 (13.84, 14.44) | 18.74 (17.97, 19.52) | <0.001 § | <0.001 § | <0.001 § |
| Calcium (mg) | 1137 (1133, 1141) | 1099 (1089, 1109) | 1114 (1109, 1120) | 1182 (1174, 1190) | 1252 (1225, 1279) | 1367 (1313, 1421) | <0.001 § | <0.001 § | <0.001 § |
| Iron (mg) | 18.8 (18.8, 18.9) | 17.8 (17.5, 18.0) | 18.2 (18.1, 18.3) | 20.0 (19.9, 20.2) | 22.7 (22.1, 23.2) | 25.7 (24.6, 26.9) | <0.001 § | <0.001 § | <0.001 |
| Zinc (mg) | 11.5 (11.4, 11.5) | 11.0 (10.9, 11.1) | 11.2 (11.1, 11.2) | 11.9 (11.9, 12.0) | 13.3 (13.1, 13.6) | 15.6 (15.1, 16.2) | <0.001 § | <0.001 § | <0.001 § |
| Anthropometry/Risk Factor Variable | Linear Trend * | Quadratic Trend after Accounting for Linear Trend * | All Trends Combined * | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Omnivores | Vegetarians | Vegans | p-Value for between Group Difference | Omnivores | Vegetarians | Vegans | p-Value for between Group Difference | p-Value for between Group Difference | |
| Weight (kg) | −1.30 (−1.48, −1.12) | −0.73 (−1.01, −0.46) | 0.87 (−0.29, 2.04) | <0.001 | −0.28 (−0.46, −0.09) | −0.53 (−0.79, −0.27) | −1.08 (−2.20, 0.05) | 0.133 | <0.001 |
| BMI (kg/m2) | −0.54 (−0.60, −0.47) | −0.30 (−0.39, −0.20) | 0.07 (−0.34, 0.49) | <0.001 | −0.09 (−0.16, −0.03) | −0.21 (−0.31, −0.12) | −0.39 (−0.79, 0.01) | 0.050 | <0.001 |
| Waist circumference (cm) | −0.69 (−0.83, −0.54) | −0.13 (−0.36, 0.09) | 0.96 (0.01, 1.92) | <0.001 | −0.04 (−0.19, 0.11) | −0.50 (−0.72, −0.29) | −0.68 (−1.60, 0.24) | 0.002 | <0.001 |
| High cholesterol † | 0.96 (0.91, 1.02) | 0.81 (0.73, 0.90) | 0.004 | 1.02 (0.96, 1.09) | 1.06 (0.96, 1.16) | 0.507 | 0.005 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, R.C.; Gray, A.R.; Tey, S.L.; Chisholm, A.; Burley, V.; Greenwood, D.C.; Cade, J. Associations between Nut Consumption and Health Vary between Omnivores, Vegetarians, and Vegans. Nutrients 2017, 9, 1219. https://doi.org/10.3390/nu9111219
Brown RC, Gray AR, Tey SL, Chisholm A, Burley V, Greenwood DC, Cade J. Associations between Nut Consumption and Health Vary between Omnivores, Vegetarians, and Vegans. Nutrients. 2017; 9(11):1219. https://doi.org/10.3390/nu9111219
Chicago/Turabian StyleBrown, Rachel C., Andrew R. Gray, Siew Ling Tey, Alexandra Chisholm, Victoria Burley, Darren C. Greenwood, and Janet Cade. 2017. "Associations between Nut Consumption and Health Vary between Omnivores, Vegetarians, and Vegans" Nutrients 9, no. 11: 1219. https://doi.org/10.3390/nu9111219