Effects of the Mediterranean Diet before and after Weight Loss on Eating Behavioral Traits in Men with Metabolic Syndrome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
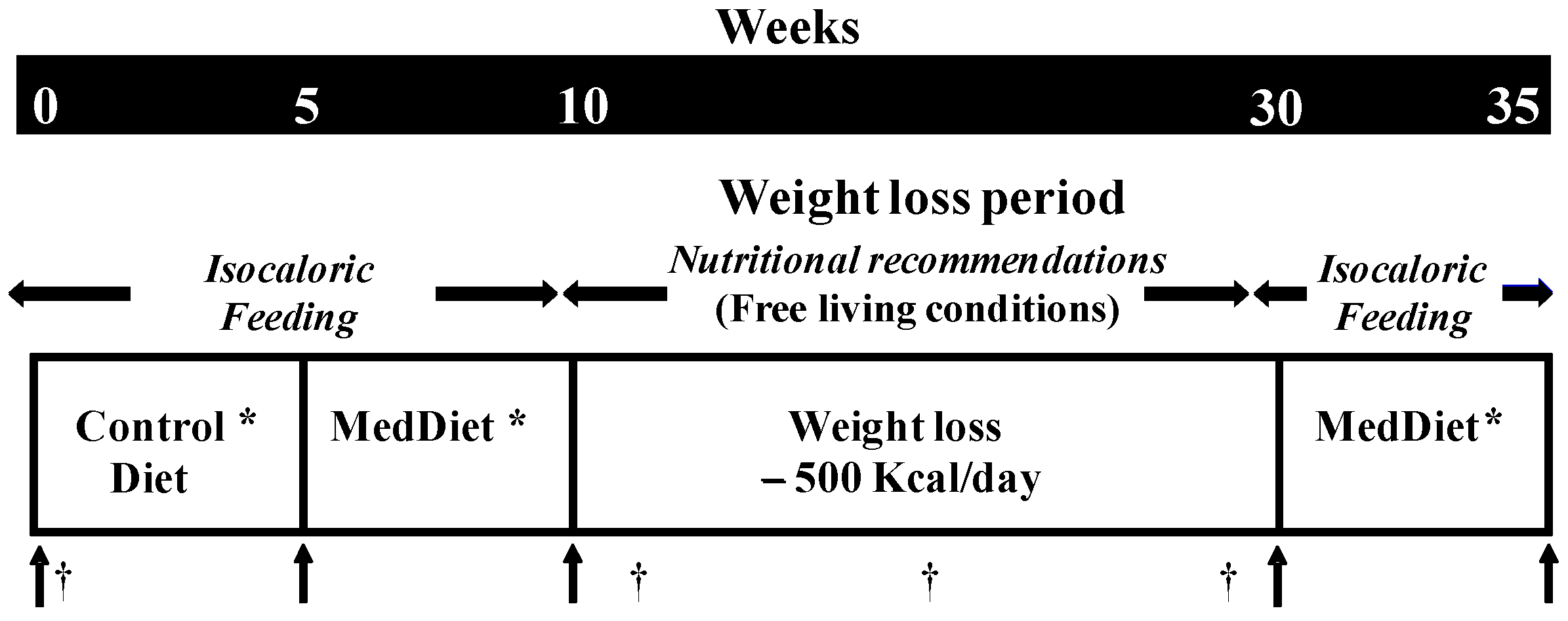
2.2. Study Design
2.3. Anthropometry Measurements
2.4. Eating Behaviors Measurements
2.5. Determination of Mediterranean Dietary Score (MedScore)
2.6. Statistical Analyses
3. Results
3.1. Weight Changes
3.2. Eating Behaviors
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Serra-Majem, L.; Roman, B.; Estruch, R. Scientific evidence of interventions using the Mediterranean diet: A systematic review. Nutr. Rev. 2006, 64, S27–S47. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.; Wareham, N.J.; Khaw, K.T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-mediterranean population: The epic-norfolk study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Guasch-Ferre, M.; Lee, C.H.; Estruch, R.; Clish, C.B.; Ros, E. Protective effects of the Mediterranean diet on type 2 diabetes and metabolic syndrome. J. Nutr. 2016, 146, 9205–9275. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Estruch, R.; Corella, D.; Fito, M.; Ros, E. Benefits of the Mediterranean diet: Insights from the predimed study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N.A. Comprehensive Meta-analysis on Evidence of Mediterranean Diet and Cardiovascular Disease: Are Individual Components Equal? Crit. Rev. Food Sci. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Meydani, M. A mediterranean-style diet and metabolic syndrome. Nutr. Rev. 2005, 63, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Polychronopoulos, E. The role of Mediterranean diet in the epidemiology of metabolic syndrome; converting epidemiology to clinical practice. Lipids Health Dis. 2005, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss: Meta-analysis of randomized controlled trials. Meta. Syndr. Relat. Disord. 2011, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Goudevenos, J.A.; Panagiotakos, D.B. Mediterranean diet and coronary heart disease: Is obesity a link?—A systematic review. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 536–551. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Fernandez-Ballart, J.; Ros, E.; Martinez-Gonzalez, M.A.; Fito, M.; Estruch, R.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: One-year results of the predimed randomized trial. Arch. Intern. Med. 2008, 168, 2449–2458. [Google Scholar] [CrossRef] [PubMed]
- Schroder, H. Protective mechanisms of the Mediterranean diet in obesity and type 2 diabetes. J. Nutr. Biochem. 2007, 18, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J. The relationship between dietary energy density and energy intake. Physiol. Behav. 2009, 97, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Drapeau, V.; Blundell, J.E.; Therrien, F.; Lawton, C.; Richard, D.; Tremblay, A. Appetite sensations as a marker of overall intake. Br. J. Nutr. 2005, 93, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Drapeau, V.; King, N.; Hetherington, M.; Doucet, E.; Blundell, J.; Tremblay, A. Appetite sensations and satiety quotient: Predictors of energy intake and weight loss. Appetite 2007, 48, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, S.M.; Delargy, H.J.; Joanes, D.; Blundell, J.E. A satiety quotient: A formulation to assess the satiating effect of food. Appetite 1997, 29, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Lowe, M.R.; Levine, A.S. Eating motives and the controversy over dieting: Eating less than needed versus less than wanted. Obes. Res. 2005, 13, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.R.; Butryn, M.L. Hedonic hunger: A new dimension of appetite? Physiol. Behav. 2007, 91, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Richard, C.; Couture, P.; Desroches, S.; Charest, A.; Lamarche, B. Effect of the Mediterranean diet with and without weight loss on cardiovascular risk factors in men with the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.; Chumlea, W.; Bouchard, C. Standardization of anthropometric measurements. In The Airlie (va) Consensus Conference; Lohman, T., Roche, A., Martorel, R., Eds.; Human Kinetics Publishers: Champaign, IL, USA, 1988; pp. 39–80. [Google Scholar]
- Westenhoefer, J.; Stunkard, A.J.; Pudel, V. Validation of the flexible and rigid control dimensions of dietary restraint. Int. J. Eat. Disord. 1999, 26, 53–64. [Google Scholar] [CrossRef]
- Bond, M.J.; McDowell, A.J.; Wilkinson, J.Y. The measurement of dietary restraint, disinhibition and hunger: An examination of the factor structure of the three factor eating questionnaire (tfeq). Int. J. Obes. Relat. Metab. Disord. 2001, 25, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Goulet, J.; Lamarche, B.; Nadeau, G.; Lemieux, S. Effect of a nutritional intervention promoting the mediterranean food pattern on plasma lipids, lipoproteins and body weight in healthy French-Canadian women. Atherosclerosis 2003, 170, 115–124. [Google Scholar] [CrossRef]
- Munsch, S.; Biedert, E.; Keller, U. Evaluation of a lifestyle change programme for the treatment of obesity in general practice. Swiss Med. Wkly. 2003, 133, 148–154. [Google Scholar] [PubMed]
- Timko, C.A. Norms for the rigid and flexible control over eating scales in a United States population. Appetite 2007, 49, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Bédard, A.; Hudon, A.M.; Drapeau, V.; Corneau, L.; Dodin, S.; Lemieux, S. Gender differences in the appetite response to a satiating diet. J. Obes. 2015, 2015, 140139. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Wadden, T.A.; Swain, R.M.; Stunkard, A.J.; Platte, P.; Vogt, R.A. The eating inventory in obese women: Clinical correlates and relationship to weight loss. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Drapeau, V.; Hetherington, M.; Lemieux, S.; Provencher, V.; Tremblay, A. Psychobiological effects observed in obese men experiencing body weight loss plateau. Depress. Anxiety 2007, 24, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, S.; Rossell, N.; Drapeau, V.; Poulain, M.; Garnier, S.; Sanguignol, F.; Mauriege, P. Effect of weight reduction on quality of life and eating behaviors in obese women. Menopause 2007, 14, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Keranen, A.M.; Savolainen, M.J.; Reponen, A.H.; Kujari, M.L.; Lindeman, S.M.; Bloigu, R.S.; Laitinen, J.H. The effect of eating behavior on weight loss and maintenance during a lifestyle intervention. Prev. Med. 2009, 49, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Sarlio-Lahteenkorva, S.; Rissanen, A. Weight loss maintenance: Determinants of long-term success. Eat. Weight Disord. 1998, 3, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Fogelholm, M.; Kukkonen-Harjula, K.; Oja, P. Eating control and physical activity as determinants of short-term weight maintenance after a very-low-calorie diet among obese women. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraca, E.V.; Marques, M.M.; Rutter, H.; Oppert, J.M.; De Bourdeaudhuij, I.; Lakerveld, J.; Brug, J. Successful behavior change in obesity interventions in adults: A systematic review of self-regulation mediators. BMC Med. 2015, 13, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, A.J.; Blundell, J.E. The effects of a high-protein or high-carbohydrate meal on subjective motivation to eat and food preferences. Nut. Behav. 1986, 3, 133–144. [Google Scholar]


{kind=link}
| Variable | Control Diet | MedDiet |
|---|---|---|
| MedDiet score a | 20 | 37 |
| Key foods b | ||
| Whole grains products (servings/day) | 1.2 | 5.4 |
| Fruits and Vegetables (servings/day) | 6.6 | 16.1 |
| Legumes (servings/week) | 0.6 | 3.6 |
| Nuts (servings/day) | 0.5 c | 0.9 |
| Cheese and yogurt (servings/day) | 1.8 | 2.0 d |
| Fish (servings/week) | 1.0 | 8.8 |
| Poultry (servings/week) | 6.8 | 6.0 |
| Eggs (servings/week) | 2.6 | 2.2 |
| Sweets (servings/week) | 13.0 | 2.0 |
| Red meat (servings/week) | 13.1 | 1.2 |
| Red wine (servings/week) | 7.0 | 17.5 |
| Olive oil (ml/week) | 4.5 | 302.8 |
| Macronutrient composition/day | ||
| Proteins (g, (% of kcal)) | 106 (17) | 106 (17) |
| Lipids (g, (% of kcal)) | 95 (34) | 89 (32) |
| Carbohydrates (g, (% of kcal)) | 303 (48) | 313 (50) |
| Total fibers (g) | 20 | 42 |
| Energy density (kcal/g) | 1.35 | 0.93 |
| Variable | Mean ± SD a | Range |
|---|---|---|
| Age (years) | 50.8 ± 10.8 | 24–62 |
| Weight (kg) | 100.4 ± 19.7 | 80.8–155.9 |
| BMI (kg/m2) | 33.7 ± 5.5 | 26.9–50.4 |
| Waist circumference (cm) | 113.5 ± 12.2 | 98.7–145.7 |
| MetS (%) | 100 | - |
| Cognitive restraint b | 7.3 ± 3.4 | 2–15 |
| Disinhibition b | 6.0 ± 2.5 | 2–11 |
| Susceptibility to hunger b | 3.3 ± 3.3 | 0–12 |
| Control Diet | MedDiet 1 before WL | Free-Living WL Phase | MedDiet after WL | p * | |
|---|---|---|---|---|---|
| Physical characteristics | |||||
| Body weight (kg) † | 99.5 ± 19.7 | 98.3 ± 19.6 | 90.4 ± 18.4 a,b | 89.4 ± 18.2 a,b | < 0.0001 |
| BMI (kg/m2) † | 33.4 ± 5.6 | 33.0 ± 5.5 | 30.3 ± 5.2 a,b | 29.9 ± 5.2 a,b | < 0.0001 |
| Waist circumference (cm) † | 110.7 ± 10.2 | 112.2 ± 12.2 | 105.2 ± 13.4 a,b | 104.3 ± 13.4 a,b | < 0.0001 |
| Eating behavioral traits (range score) 2 | |||||
| Cognitive restraint (0–21) † | 7.17 ± 4.35 | 7.23 ± 4.40 | 10.85 ± 4.23 a,b | 10.41 ± | < 0.0001 |
| Flexible restraint (0–7) † | 2.12 ± 1.36 | 2.44 ± 1.76 | 3.17 ± 2.12 | 3.18 ± 1.91 | 0.05 |
| Rigid restraint (0–7) | 1.79 ± 1.74 | 1.74 ± 1.56 | 3.04 ± 1.60 a,b | 3.43 ± 2.13 a,b | < 0.0001 |
| Strategic restraint (0–4) † | 0.38 ± 0.92 | 0.50 ± 0.79 | 1.06 ± 1.11 a | 0.74 ± 0.87 | 0.008 |
| Attitude to self-regulation (0–5) | 2.93 ± 1.39 | 2.79 ± 1.32 | 3.73 ± 0.80 a,b | 3.58 ± 1.43 a,b | 0.003 |
| Avoidance of fattening foods (0–4) | 1.67 ± 0.84 | 1.74 ± 1.10 | 2.29 ± 1.10 a | 2.32 ± 1.25 a | 0.004 |
| Disinhibition (0–16) | 6.28 ± 2.33 | 6.07 ± 2.31 | 5.07 ± 2.18 a,b | 5.04 ± 2.30 a,b | 0.0003 |
| Habitual (0–5) | 0.47 ± 0.62 | 0.56 ± 0.62 | 0.44 ± 0.63 | 0.47 ± 0.61 | 0.96 |
| Emotional (0–3) | 1.11 ± 1.29 | 1.00 ± 1.25 | 0.59 ± 1.12 | 0.61 ± 1.09 | 0.17 |
| Situational (0–5) | 3.00 ± 1.41 | 2.79 ± 1.23 | 2.06 ± 1.26 a,b | 2.06 ± 1.39 a,b | < 0.0001 |
| Susceptibility to hunger (0–14) † | 3.82 ± 3.67 | 3.74 ± 3.26 | 2.45 ± 2.74 b | 2.47 ± 2.67 b | 0.006 |
| Internal (0–6) † | 1.06 ± 1.57 | 0.84 ± 1.46 | 0.50 ± 1.25 a | 0.47 ± 1.02 | 0.03 |
| External (0–6) | 1.79 ± 1.76 | 1.89 ± 1.70 | 1.12 ± 1.41 b | 1.21 ± 1.36 | 0.01 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbonneau, É.; Royer, M.-M.; Richard, C.; Couture, P.; Desroches, S.; Lemieux, S.; Lamarche, B. Effects of the Mediterranean Diet before and after Weight Loss on Eating Behavioral Traits in Men with Metabolic Syndrome. Nutrients 2017, 9, 305. https://doi.org/10.3390/nu9030305
Carbonneau É, Royer M-M, Richard C, Couture P, Desroches S, Lemieux S, Lamarche B. Effects of the Mediterranean Diet before and after Weight Loss on Eating Behavioral Traits in Men with Metabolic Syndrome. Nutrients. 2017; 9(3):305. https://doi.org/10.3390/nu9030305
Chicago/Turabian StyleCarbonneau, Élise, Marie-Michelle Royer, Caroline Richard, Patrick Couture, Sophie Desroches, Simone Lemieux, and Benoît Lamarche. 2017. "Effects of the Mediterranean Diet before and after Weight Loss on Eating Behavioral Traits in Men with Metabolic Syndrome" Nutrients 9, no. 3: 305. https://doi.org/10.3390/nu9030305