Relationships among Different Water-Soluble Choline Compounds Differ between Human Preterm and Donor Milk

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Biochemical Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate OBV, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin and Choline; National Academies Press (US): Washington, DC, USA, 1998. [Google Scholar]
- Bernhard, W.; Full, A.; Arand, J.; Maas, C.; Poets, C.F.; Franz, A.R. Choline supply of preterm infants: Assessment of dietary intake and pathophysiological considerations. Eur. J. Nutr. 2013, 52, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.M.; da Costa, K.A.; Galanko, J.; Sha, W.; Stephenson, B.; Vick, J.; Zeisel, S.H. Choline intake and genetic polymorphisms influence choline metabolite concentrations in human breast milk and plasma. Am. J. Clin. Nutr. 2010, 92, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S.H.; Char, D.; Sheard, N.F. Choline, phosphatidylcholine and sphingomyelin in human and bovine milk and infant formulas. J. Nutr. 1986, 116, 50–58. [Google Scholar] [PubMed]
- Ilcol, Y.O.; Ozbek, R.; Hamurtekin, E.; Ulus, I.H. Choline status in newborns, infants, children, breast-feeding women, breast-fed infants and human breast milk. J. Nutr. Biochem. 2005, 16, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Holmes-McNary, M.Q.; Cheng, W.L.; Mar, M.H.; Fussell, S.; Zeisel, S.H. Choline and choline esters in human and rat milk and in infant formulas. Am. J. Clin. Nutr. 1996, 64, 572–576. [Google Scholar] [PubMed]
- Zeisel, S.H. Choline: Critical role during fetal development and dietary requirements in adults. Annu. Rev. Nutr. 2006, 26, 229–250. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.L.; Holmes-McNary, M.Q.; Mar, M.H.; Lien, E.L.; Zeisel, S.H. Bioavailability of choline and choline esters from milk in rat pups. J. Nutr. Biochem. 1996, 7, 457–464. [Google Scholar] [CrossRef]
- Lewis, E.D.; Jacobs, R.L.; Field, C.J. Should the forms of dietary choline also be considered when estimating dietary intake and the implications for health? Lipid Technol. 2015, 27, 227–230. [Google Scholar] [CrossRef]
- Landers, S.; Hartmann, B.T. Donor human milk banking and the emergence of milk sharing. Pediatr. Clin. N. Am. 2013, 60, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Soberanes Garcia, L.S. Water–Soluble Choline Compounds in Human Milk: Their Variation and Impact of Storage and Diet. Master's Thesis, University of British Columbia, Vancouver, BC, Canada, 2015. [Google Scholar]
- Maas, C.; Franz, A.R.; Shunova, A.; Mathes, M.; Bleeker, C.; Poets, C.F.; Schleicher, E.; Bernhard, W. Choline and polyunsaturated fatty acids in preterm infants’ maternal milk. Eur. J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Moukarzel, S. The Complexity of Understanding Human Milk Components and Infant Brain Development. Available online: https://open.library.ubc.ca/cIRcle/collections/24/items/1.0228326 (accessed on 12 March 2017).
- Lucas, A.; Gibbs, J.A.; Lyster, R.L.; Baum, J.D. Creamatocrit: Simple clinical technique for estimating fat concentration and energy value of human milk. BMJ 1978, 1, 1018–1020. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.B.; Kruger, N.J. The Bradford method for protein quantitation. Methods Mol. Biol. 1988, 3, 25–32. [Google Scholar] [PubMed]
- Preacher, K.J. Calculation for the Test of the Difference between Two Independent Correlation Coefficients. Available online: http://quantpsy.org (accessed on 13 June 2016).
- Caudill, M.A. Pre- and postnatal health: Evidence of increased choline needs. J. Am. Diet. Assoc. 2010, 110, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.T.; Dyer, R.A.; King, D.J.; Richardson, K.J.; Innis, S. Early second trimester maternal plasma choline and betaine are related to measures of early cognitive development in term infants. PLoS ONE 2012, 7, e43448. [Google Scholar] [CrossRef] [PubMed]
- Ueland, P. Choline and betaine in health and disease. J. Inherit. Metab. Dis. 2011, 34, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C.; Mato, J.M. S-adenosylmethionine in liver health, injury, and cancer. Physiol. Rev. 2012, 92, 1515–1542. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W.; Raith, M.; Kunze, R.; Koch, V.; Heni, M.; Maas, C.; Abele, H.; Poets, C.F.; Franz, A.R. Choline concentrations are lower in postnatal plasma of preterm infants than in cord plasma. Eur. J. Nutr. 2015, 54, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.K.; Pomfret, E.A.; Zeisel, S.H. Uptake of choline by rat mammary-gland epithelial cells. Biochem. J. 1988, 254, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.K.; Blusztajn, J.K.; Pomfret, E.A.; Zeisel, S.H. Rat and human mammary tissue can synthesize choline moiety via the methylation of phosphatidylethanolamine. Biochem. J. 1988, 256, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Romano, K.A.; Vivas, E.I.; Amador-Noguez, D.; Rey, F.E. Intestinal microbiota composition modulates choline bioavailability from diet and accumulation of the proatherogenic metabolite trimethylamine-N-oxide. mBio 2015, 6, e02481. [Google Scholar] [CrossRef] [PubMed]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Detopoulou, P.; Panagiotakos, D.B.; Antonopoulou, S.; Pitsavos, C.; Stefanadis, C. Dietary choline and betaine intakes in relation to concentrations of inflammatory markers in healthy adults: The ATTICA study. Am. J. Clin. Nutr. 2008, 87, 424–430. [Google Scholar] [PubMed]
- Sachan, D.S.; Hongu, N.; Johnsen, M. Decreasing oxidative stress with choline and carnitine in women. J. Am. Coll. Nutr. 2005, 24, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Menon, R. Oxidative Stress Damage as a Detrimental Factor in Preterm Birth Pathology. Front. Immunol. 2014, 5, 567. [Google Scholar] [CrossRef] [PubMed]
- Cappelletti, M.; Della Bella, S.; Ferrazzi, E.; Mavilio, D.; Divanovic, S. Inflammation and preterm birth. J. Leukoc. Biol. 2016, 99, 67–78. [Google Scholar] [CrossRef] [PubMed]
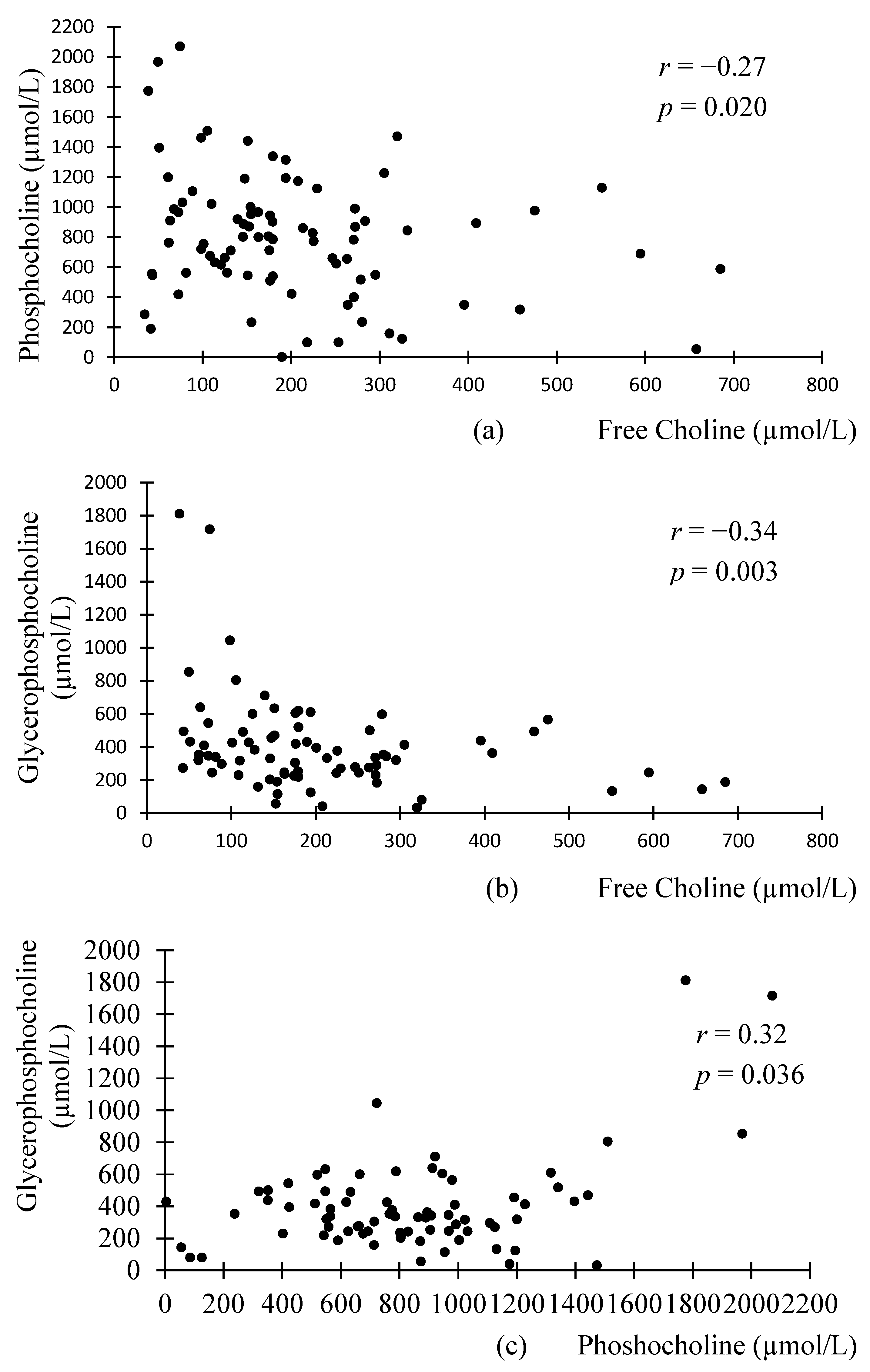

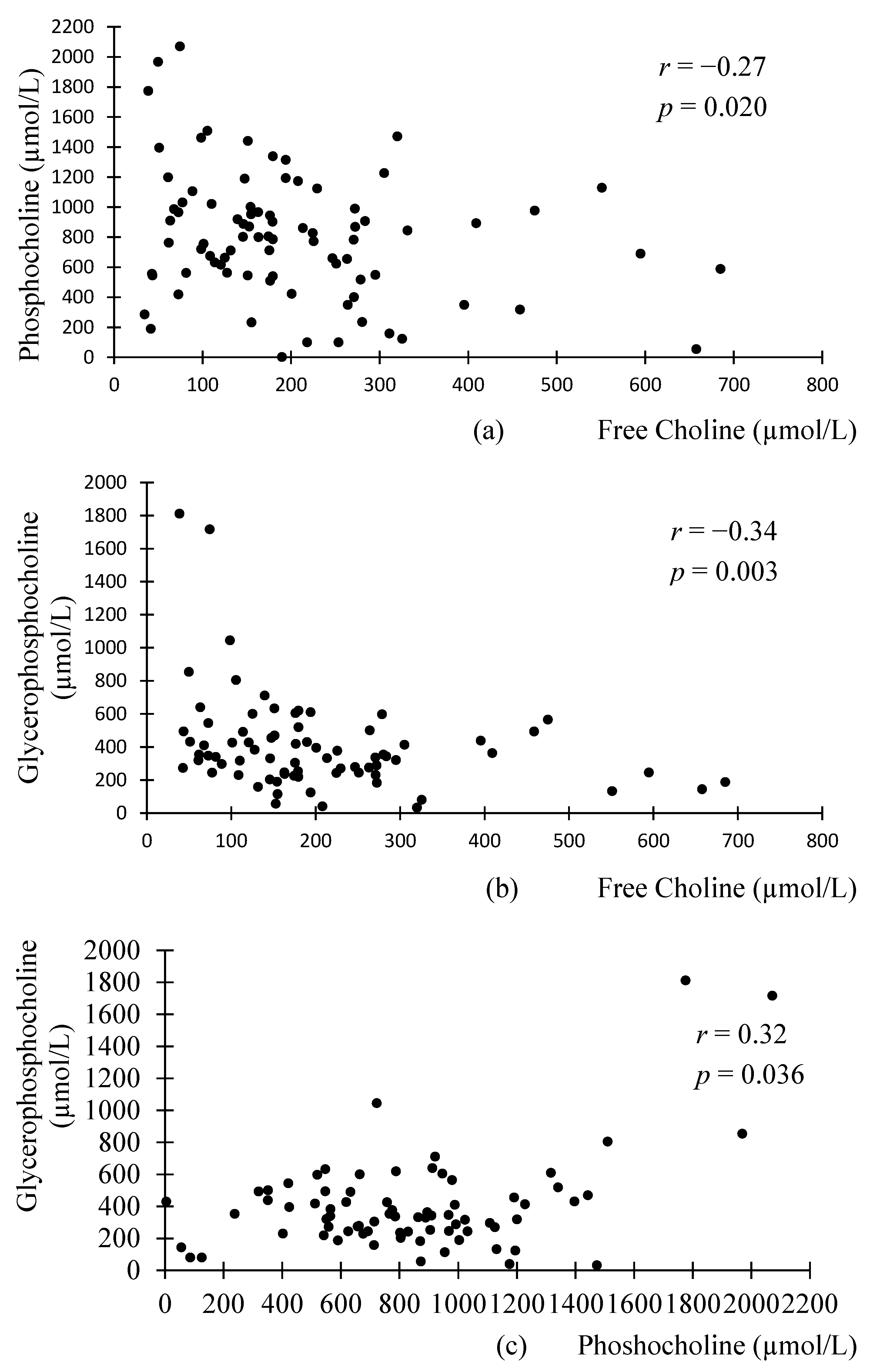{kind=link}
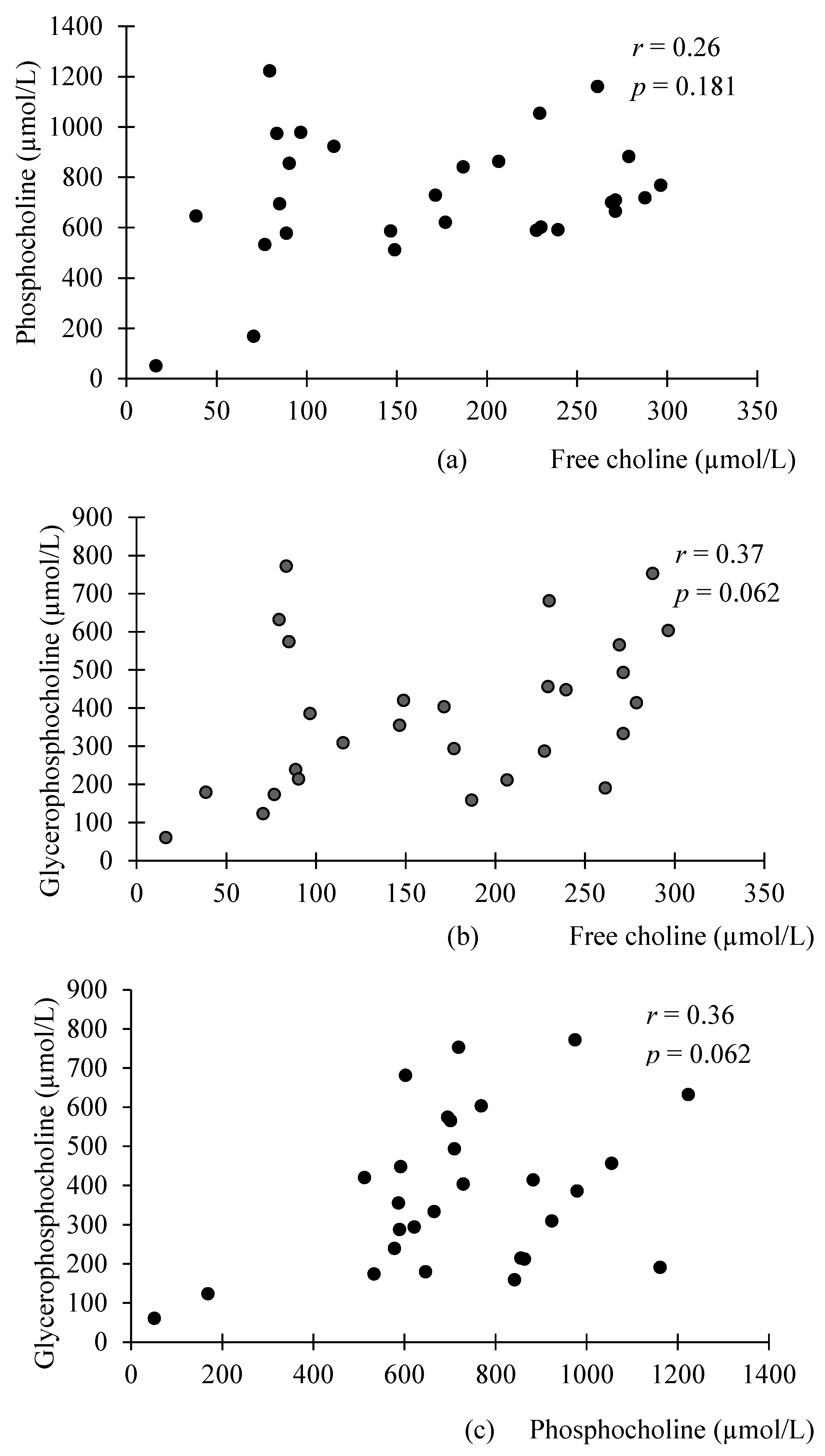
{kind=link}
| µmol/L | Preterm Milk n = 75 | Term Donor Milk n = 30 | p-Value |
|---|---|---|---|
| Phosphocholine | 0.068 1 | ||
| Mean ± SD | 859 ± 385 | 722 ± 255 | |
| Median | 805 | 705 | |
| Range | 3.4–2070 | 50.8–1223 | |
| Glycerophoshocholine | 0.928 2 | ||
| Mean ± SD | 404 ± 294 | 383 ± 195 | |
| Median | 343 | 370 | |
| Range | 33.5–1813 | 60.5–772 | |
| Free choline | 0.569 2 | ||
| Mean ± SD | 203 ± 139 | 170 ± 86.5 | |
| Median | 176 | 174 | |
| Range | 38.4–685 | 16.3–297 | |
| Total WSC compounds | 0.322 2 | ||
| Mean ± SD | 1460 ± 543 | 1275 ± 414 | |
| Median | 1365 | 1293 | |
| Range | 531.3–3863 | 127.6–1934 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moukarzel, S.; Soberanes, L.; Dyer, R.A.; Albersheim, S.; Elango, R.; Innis, S.M. Relationships among Different Water-Soluble Choline Compounds Differ between Human Preterm and Donor Milk. Nutrients 2017, 9, 369. https://doi.org/10.3390/nu9040369
Moukarzel S, Soberanes L, Dyer RA, Albersheim S, Elango R, Innis SM. Relationships among Different Water-Soluble Choline Compounds Differ between Human Preterm and Donor Milk. Nutrients. 2017; 9(4):369. https://doi.org/10.3390/nu9040369
Chicago/Turabian StyleMoukarzel, Sara, Lynda Soberanes, Roger A. Dyer, Susan Albersheim, Rajavel Elango, and Sheila M. Innis. 2017. "Relationships among Different Water-Soluble Choline Compounds Differ between Human Preterm and Donor Milk" Nutrients 9, no. 4: 369. https://doi.org/10.3390/nu9040369