The Diet and Haemodialysis Dyad: Three Eras, Four Open Questions and Four Paradoxes. A Narrative Review, Towards a Personalized, Patient-Centered Approach

 ,
,  ,
,
Abstract
:1. Diet and Dialysis: A Changing Picture
2. Dialysis and Diet: Different Enemies in Different Periods
2.1. The First Era: Potassium as the Killer
2.2. The Second Era: Phosphate as the Silent Killer
- -
- -
- -
2.3. The Third Era: Malnutrition as the Killer
3. Diet and Dialysis: Four Questions and Four Paradoxes
3.1. First Question: Are the “Magic Numbers” Still Valid?
- -
- Energy: 30–35 kcal/kg of dry body weight
- -
- Proteins: at least 1.2 g/kg of dry body weight
- -
- Phosphate: 800–1000 mg/day
- -
- Water: as little as possible
- -
- Sodium: not univocal; older guidelines recommend less than 100 mEq/day (5.8 g of NaCl)
- -
- Potassuim: 2 g/day
3.2. Second Question: Type of Dialysis Technique: Does It Matter?
- -
- On conventional thrice-weekly dialysis, dietary restrictions follow the need to maintain good metabolic balance (diet has to follow dialysis);
- -
- On intensive dialysis schedules, higher efficiency and/or frequency may make an unrestricted diet possible (dialysis liberalizes diet);
- -
3.3. Third Question: Processed or Unprocessed Food: What Are We Actually Eating?
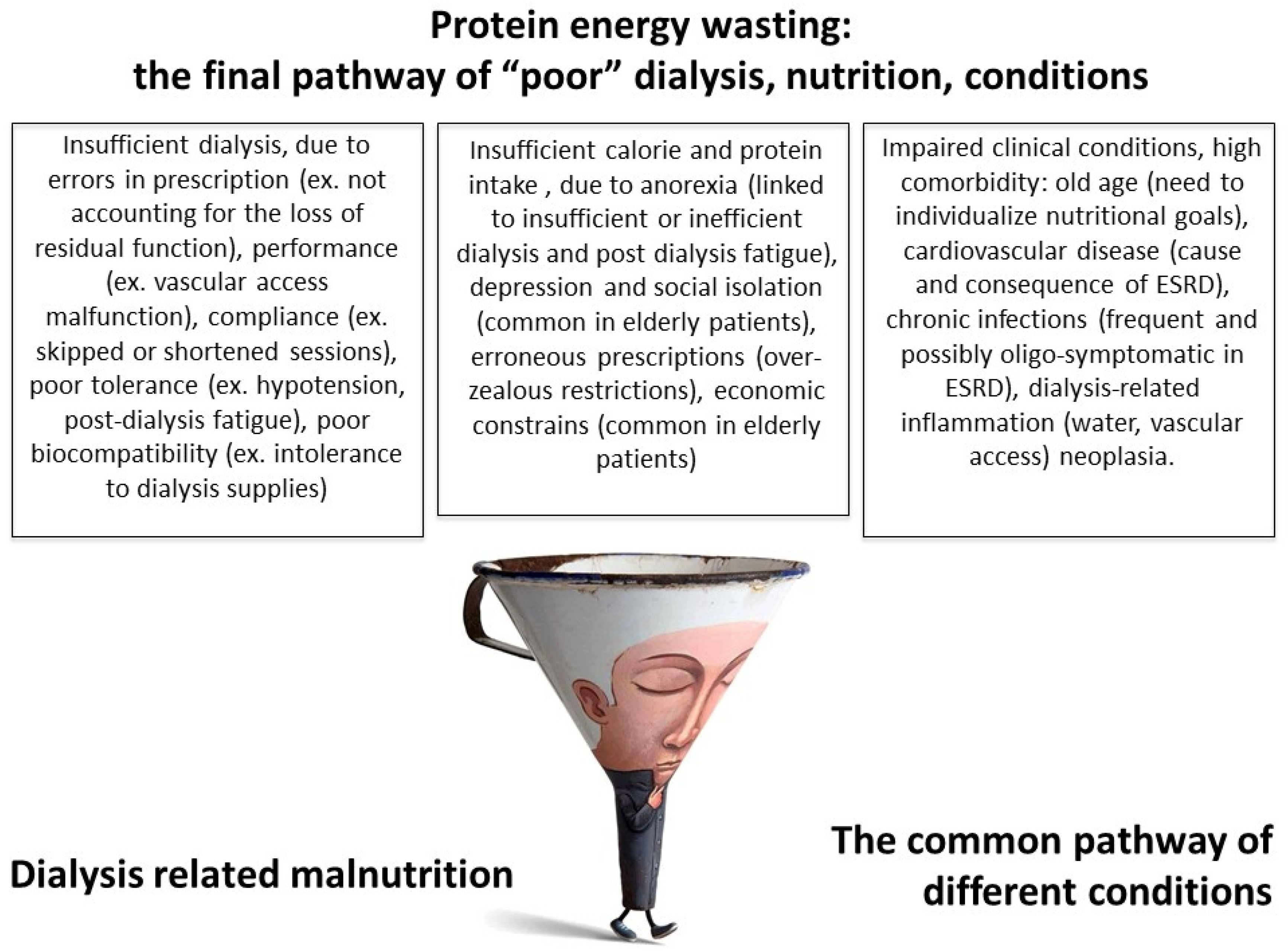
3.4. Fourth Question: How Should Malnutrition Be Seen?
- -
- Protein energy wasting due to “poor nutrition”, related to low nutrient intake, in turn linked to incomplete correction of metabolic balance, insufficient dialysis, non biocompatible membranes, poorly controlled hypertension, combined with an overly restricted diet. This form of malnutrition generally responds to nutritional intervention, after optimization of the dialysis schedule.
- -
- Protein energy wasting as a result of poor clinical conditions: the prototype is the MIA syndrome, mentioned above. This type of malnutrition is less responsive to nutritional interventions and its prognosis is linked to the patient’s life expectancy (Figure 1).
4. Diet and Dialysis: Four Paradoxes
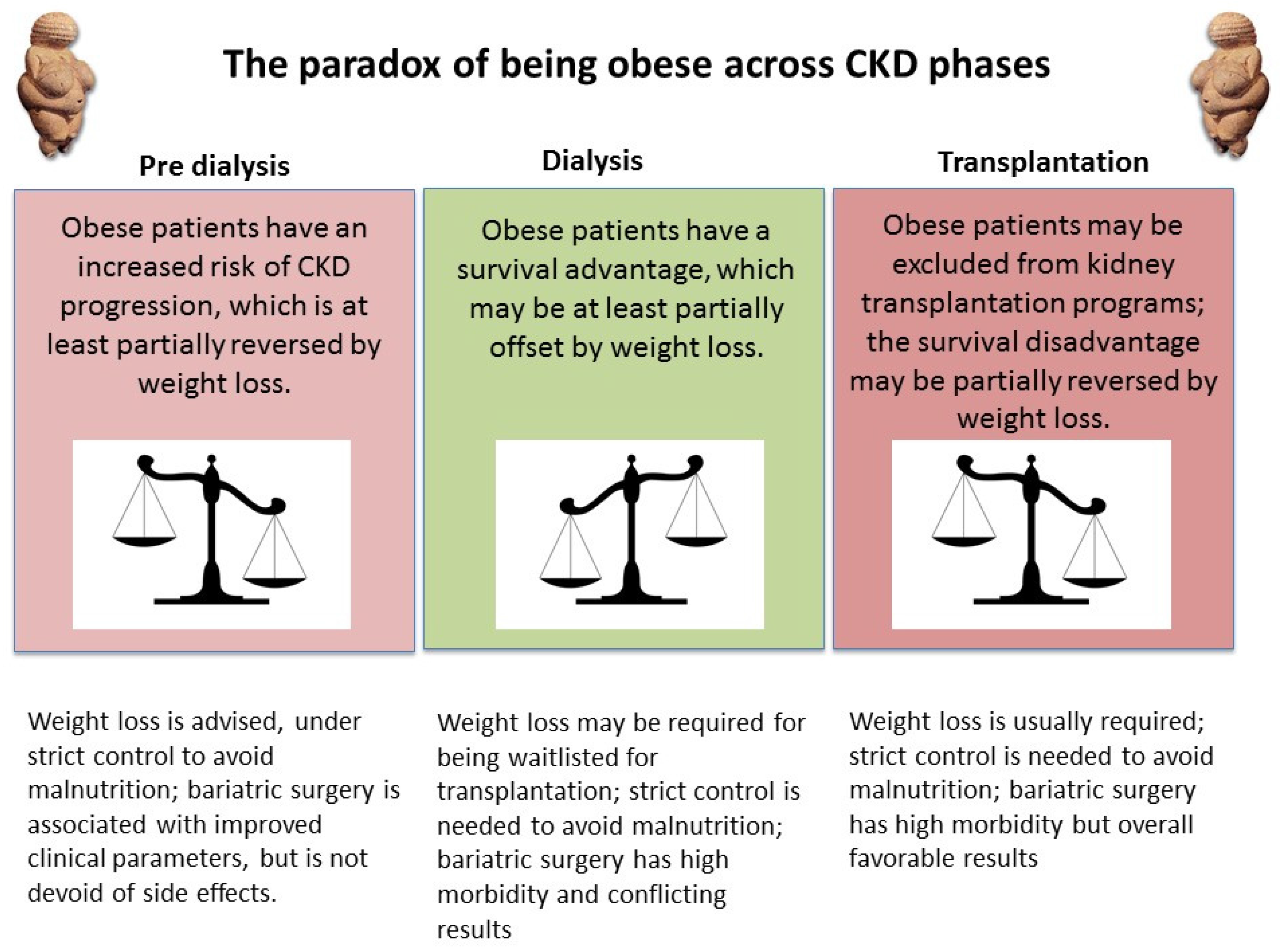
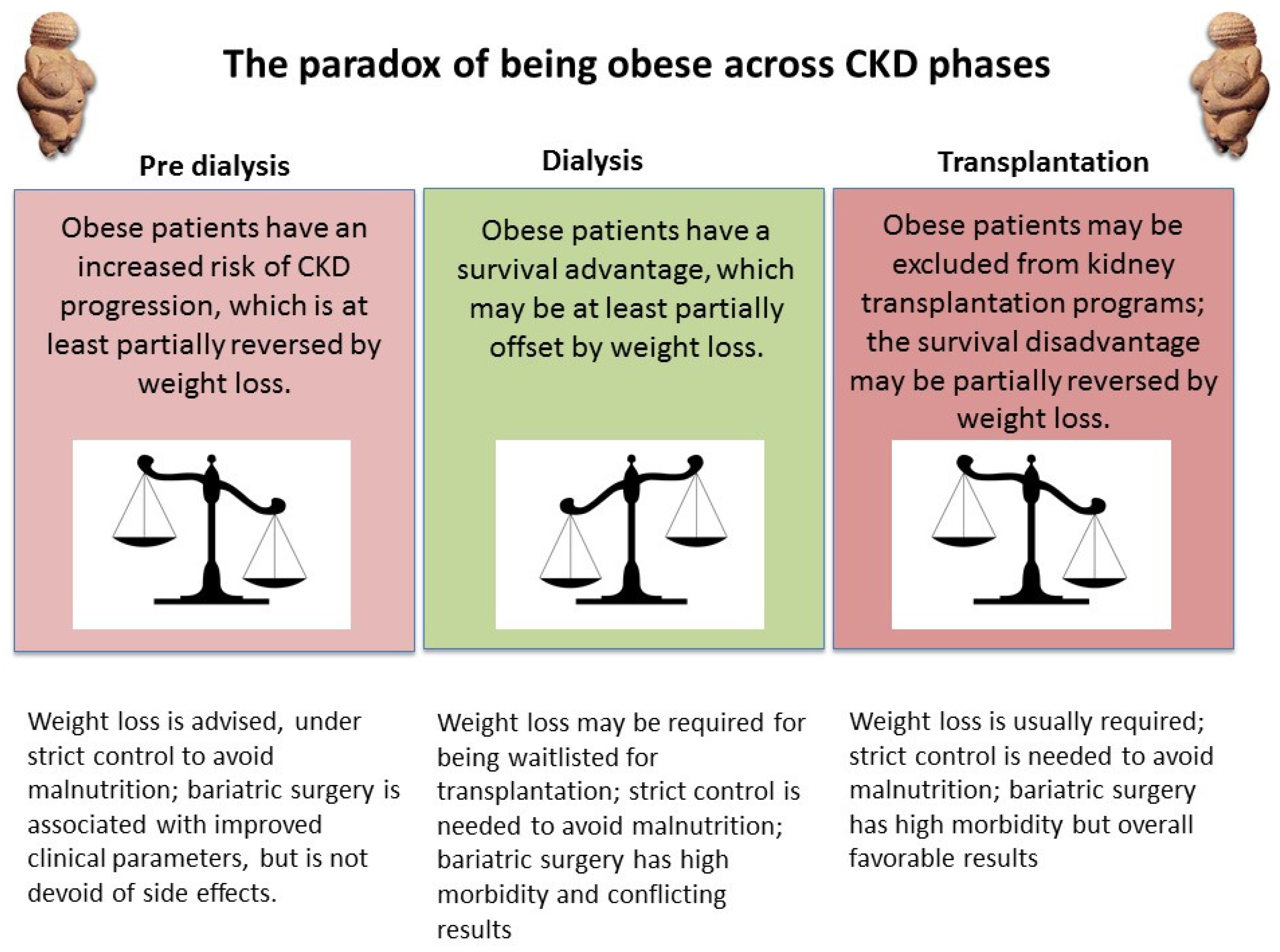
4.1. First Paradox: Energy Intake and Obesity
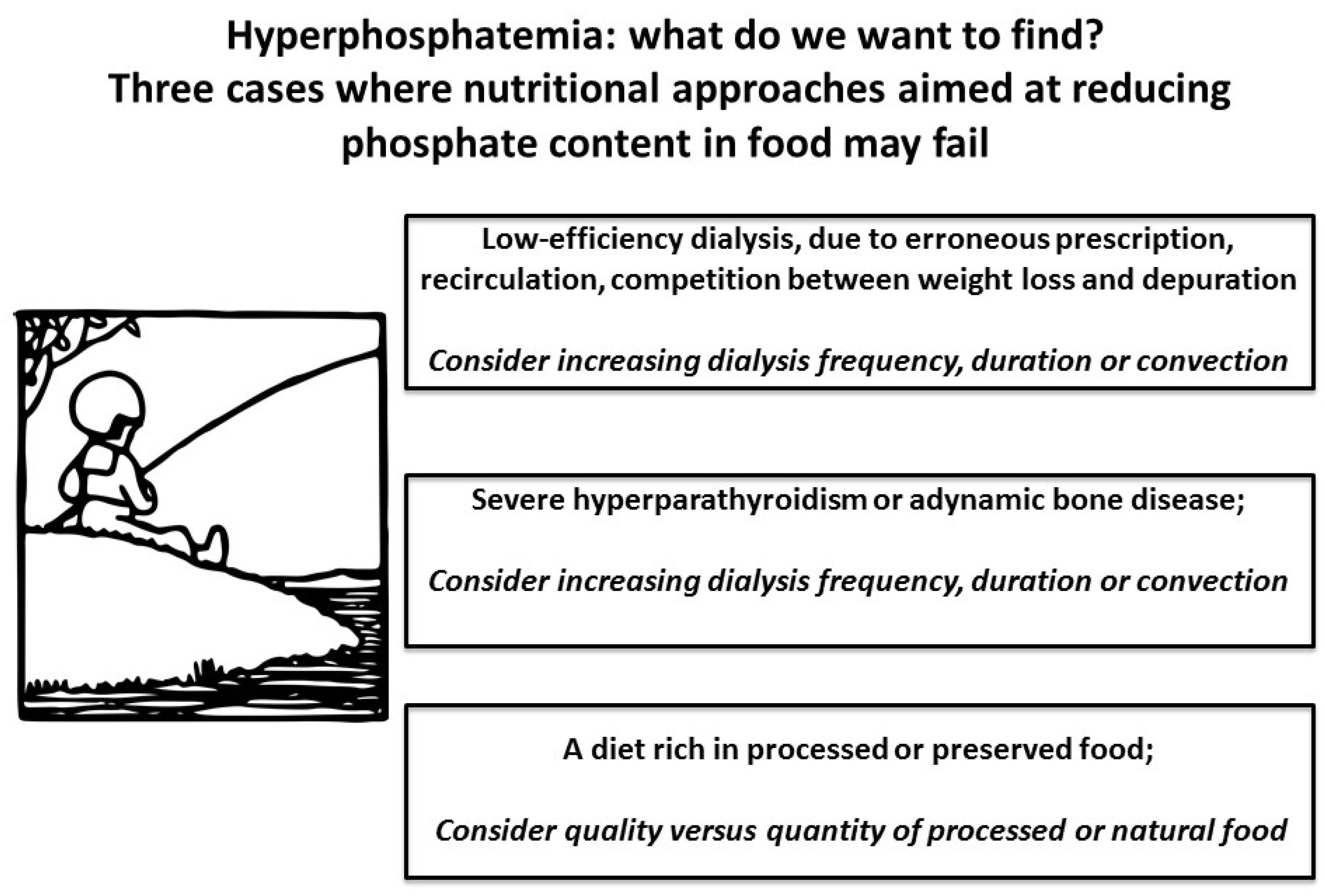
4.2. Second Paradox: Phosphate, Acidosis and Protein Intake
- -
- -
- Not all phosphate is created equal: plant organic phosphate is less absorbable than phosphate in animal protein. Added inorganic phosphate, found in food preservatives, is devoid of nutritional benefit and is more easily absorbed; information on added phosphate is however often lacking from packaging [102,103,104,105,106].
- -
- The role of animal-derived proteins in human nutrition has been reassessed in recent years, yet this critical analysis has not been fully extended to CKD and dialysis patients, for whom the equation “high quality protein = animal-derived protein = best protein” is still the basis for prescription, even if the interest on plant-based diets in all CKD stages is increasing [106,107,108,109,110,111,160,161,162].
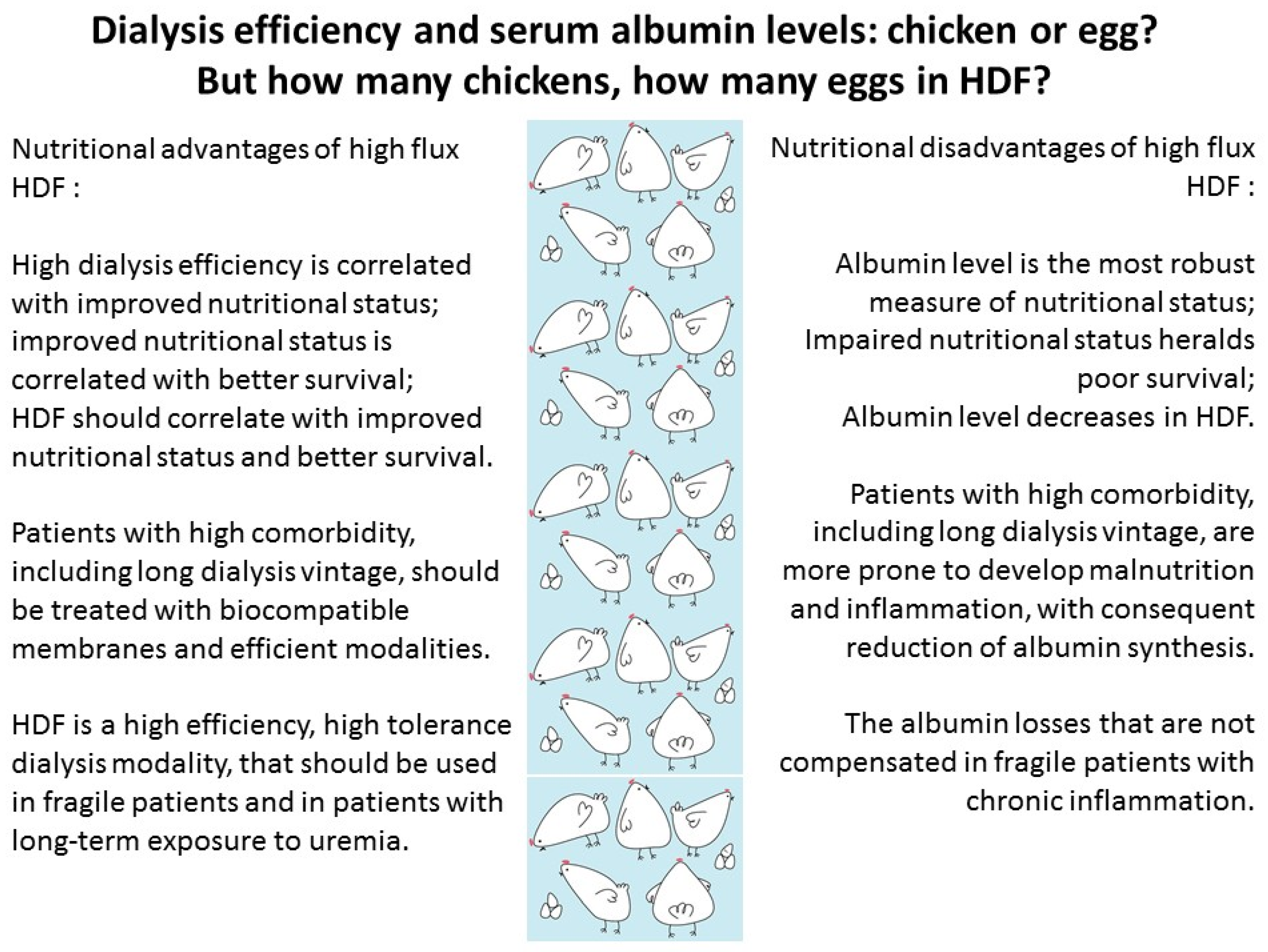
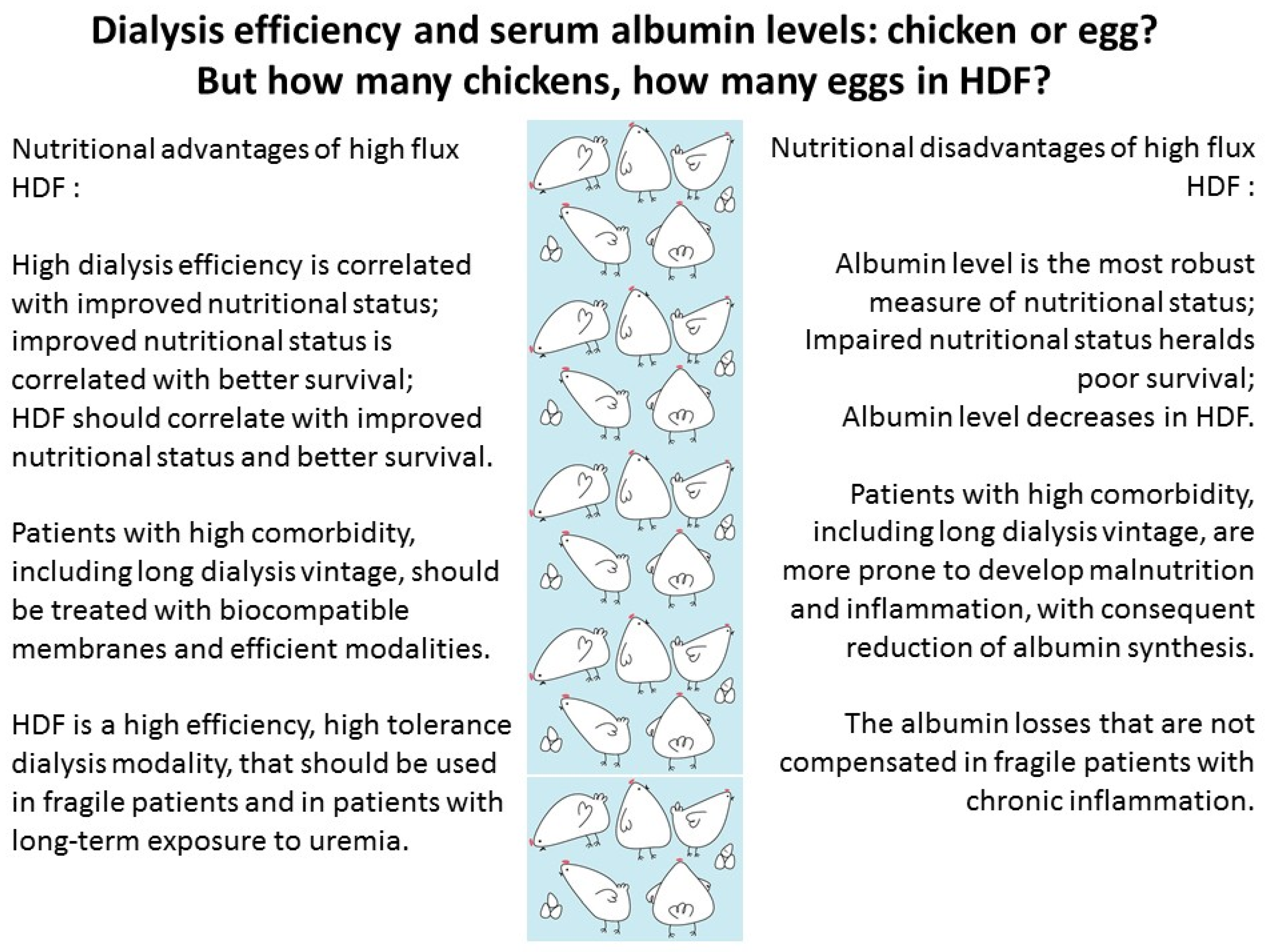
4.3. Third Paradox: High-Efficiency Dialysis and Serum Albumin Levels
- -
- On extracorporeal dialysis, albumin loss depends on the type of dialysis membranes used, dialysis, hematocrit, albumin and total protein level, blood and dialysate flows; due in part to the difficulty of sampling, few studies have assessed the intersession variability of albumin losses in individual patients, in stable conditions and in specific situations, such as inflammatory states;
- -
- No validated standardized method is available in clinical practice for dosing albumin levels at the low concentrations usually attained in the dialysate;
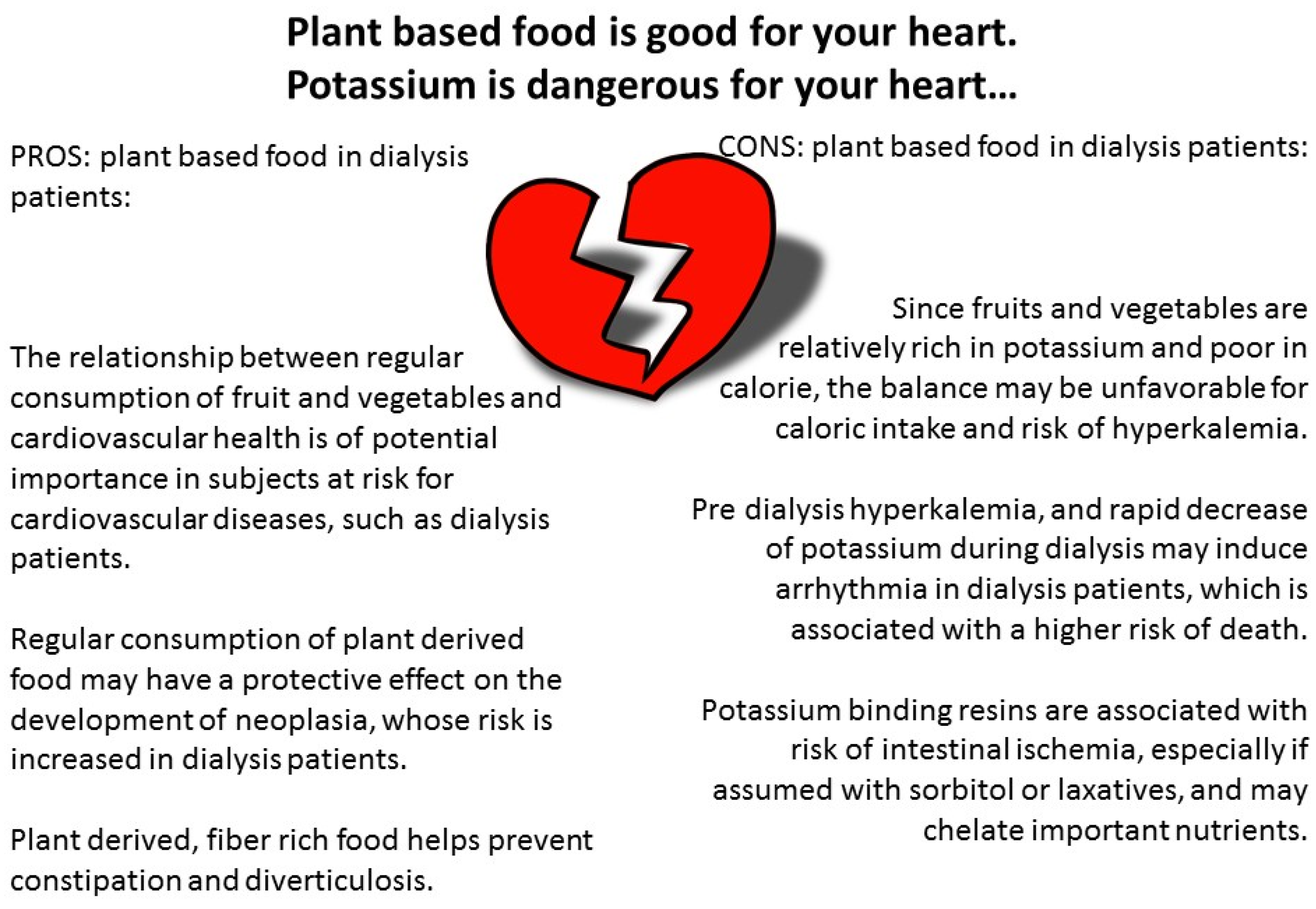
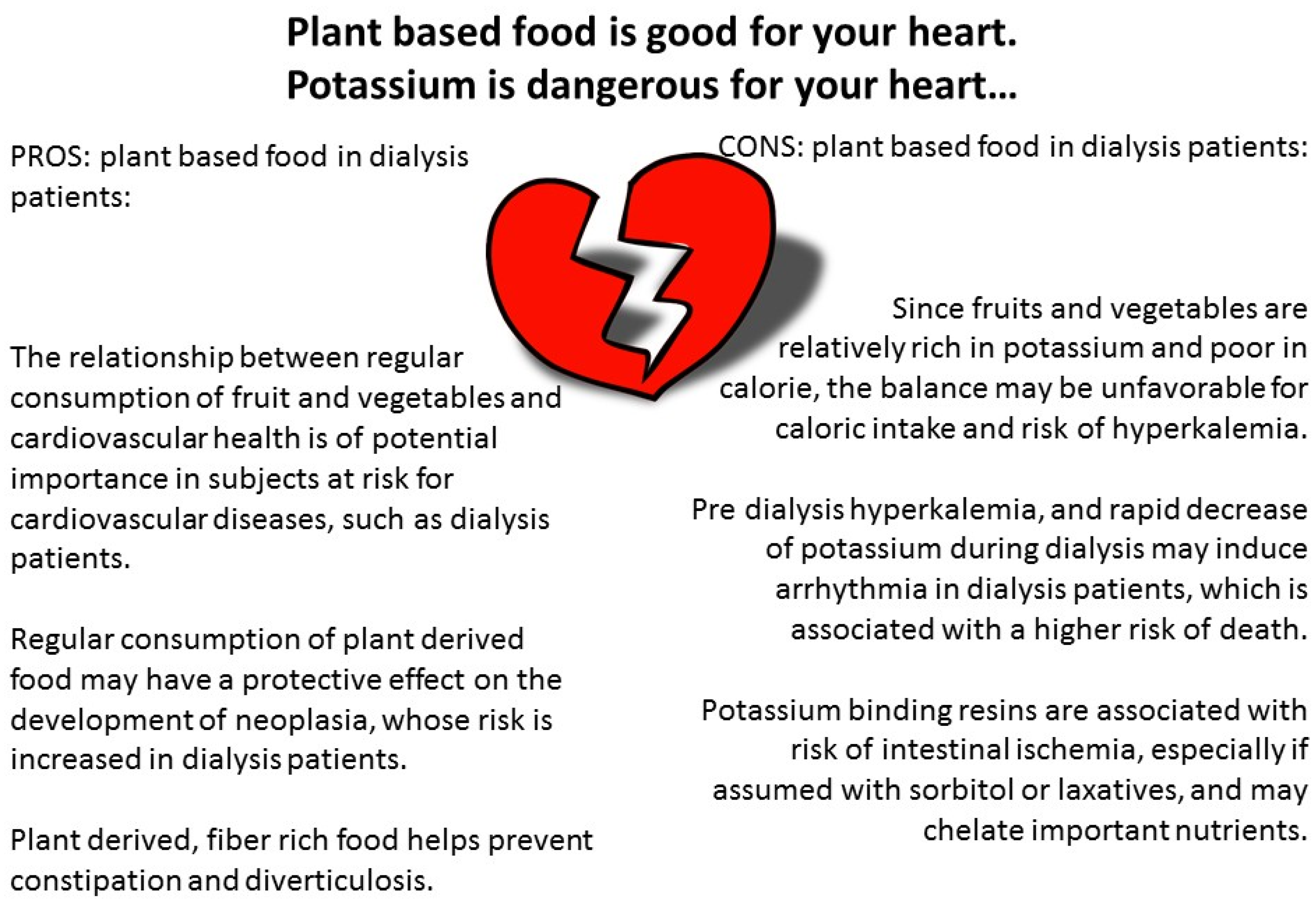
4.4. Fourth Paradox: Potassium and Vascular Health
5. What This Review Did Not Address
6. Conclusions and Suggestions for Future Research
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siddiqui, J.Y.; Fitz, A.E.; Lawton, R.L.; Kirkendall, W.M. Causes of death in patients receiving long-term hemodialysis. JAMA 1970, 212, 1350–1354. [Google Scholar] [CrossRef] [PubMed]
- Cloonan, C.C.; Gatrell, C.B.; Cushner, H.M. Emergencies in continuous dialysis patients: Diagnosis and management. Am. J. Emerg. Med. 1990, 8, 134–148. [Google Scholar] [CrossRef]
- Quintanilla, A.P.; Weffer, M.I. Hyperkalemia in the patient on chronic dialysis. Int. J. Artif. Organs 1987, 10, 17–19. [Google Scholar] [PubMed]
- Kopple, J.D.; Kalantar-Zadeh, K.; Mehrotra, R. Risks of chronic metabolic acidosis in patients with chronic kidney disease. Kidney Int. Suppl. 2005, 67, S21–S27. [Google Scholar] [CrossRef] [PubMed]
- Sanghavi, S.; Whiting, S.; Uribarri, J. Potassium balance in dialysis patients. Semin. Dial. 2013, 26, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, S.; Maggiore, Q. A low-nitrogen diet with proteins of high biological value for severe chronic uraemia. Lancet 1964, 1, 1000–1003. [Google Scholar]
- Berlyne, G.M.; Shaw, A.B.; Nilwarangkur, S. Dietary treatment of chronic renal failure. Experiences with a modified Giovannetti diet. Nephron 1965, 2, 129–147. [Google Scholar] [CrossRef] [PubMed]
- Silvererg, D.S.; Hunt, J.C. Dietary considerations in treating chronic renal failure. J. Am. Diet. Assoc. 1966, 49, 425–427. [Google Scholar] [PubMed]
- Mitch, W.E.; Abras, E.; Walser, M. Long-term effects of a new ketoacid-amino acid supplement in patients with chronic renal failure. Kidney Int. 1982, 22, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Laville, M.; Boissel, J.P.; Chifflet, R.; Labeeuw, M.; Zech, P.Y. Controlled low protein diets in chronic renal insufficiency: Meta-analysis. BMJ 1992, 304, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Mitch, W.E.; Remuzzi, G. Diets for patients with chronic kidney disease, should we reconsider? BMC Nephrol. 2016, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Kalantar-Zadeh, K. Back to the future, restricted protein intake for conservative management of CKD, triple goals of renoprotection, uremia mitigation, and nutritional health. Int. Urol. Nephrol. 2016, 48, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Tortorici, A.R.; Chen, J.L.; Kamgar, M.; Lau, W.L.; Moradi, H.; Rhee, C.M.; Streja, E.; Kovesdy, C.P. Dietary restrictions in dialysis patients, is there anything left to eat? Semin. Dial. 2015, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- St-Jules, D.E.; Goldfarb, D.S.; Sevick, M.A. Nutrient non-equivalence, does restricting high-potassium plant foods help to prevent hyperkalemia in hemodialysis patients? J. Ren. Nutr. 2016, 26, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Bakke, J.; Goodwin, L.; Okiyama, T. Sodium-restricted diets for dialysis patients. Hospitals 1966, 40, 76–81. [Google Scholar] [PubMed]
- Blumberg, A.; Nelp, W.B.; Hegstrom, R.M.; Scribner, B.H. Extracellular volume in patients with chronic renal disease treated for hypertension by sodium restriction. Lancet 1967, 2, 69–73. [Google Scholar] [CrossRef]
- Comity, C.M. Long-term dietary management of dialysis patients. II. Composition and planning of the diet and patient education. J. Am. Diet. Assoc. 1968, 53, 445–449. [Google Scholar] [PubMed]
- Rachoin, J.S.; Weisberg, L.S. How should dialysis fluid be individualized for the chronic hemodialysis patient? Potassium. Semin. Dial. 2008, 21, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Pani, A.; Floris, M.; Rosner, M.H.; Ronco, C. Hyperkalemia in hemodialysis patients. Semin. Dial. 2014, 27, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Regidor, D.L.; Mehrotra, R.; Jing, J.; McAllister, C.J.; Greenland, S.; Kopple, J.D.; Kalantar-Zadeh, K. Serum and dialysate potassium concentrations and survival in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2007, 2, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.; Weisberg, L.S. Hyperkalemia in dialysis patients. Semin. Dial. 2001, 14, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Biruete, A.; Jeong, J.H.; Barnes, J.L.; Wilund, K.R. Modified Nutritional Recommendations to Improve Dietary Patterns and Outcomes in Hemodialysis Patients. J. Ren. Nutr. 2017, 27, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.A.; Mehta, O. Phosphorus and potassium content of enhanced meat and poultry products, implications for patients who receive dialysis. Clin. J. Am. Soc. Nephrol. 2009, 4, 1370–1373. [Google Scholar]
- Curtis, C.J.; Niederman, S.A.; Kansagra, S.M. Availability of potassium on the nutrition facts panel of US packaged foods. JAMA Intern. Med. 2013, 173, 828–829. [Google Scholar] [CrossRef] [PubMed]
- Stover, J. Non-dietary causes of hyperkalemia. Nephrol. Nurs. J. 2006, 33, 221–222. [Google Scholar] [PubMed]
- Noori, N.; Kalantar-Zadeh, K.; Kovesdy, C.P.; Murali, S.B.; Bross, R.; Nissenson, A.R.; Kopple, J.D. Dietary potassium intake and mortality in long-term hemodialysis patients. Am. J. Kidney Dis. 2010, 56, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Burrowes, J.D.; Larive, B.; Cockram, D.B.; Dwyer, J.; Kusek, J.W.; McLeroy, S.; Poole, D.; Rocco, M.V.; Hemodialysis (HEMO) Study Group. Effects of dietary intake, appetite, and eating habits on dialysis and non-dialysis treatment days in hemodialysis patients, cross-sectional results from the HEMO study. J. Ren. Nutr. 2003, 13, 191–198. [Google Scholar] [CrossRef]
- Charney, D.I.; Walton, D.F.; Cheung, A.K. Atherosclerosis in chronic renal failure. Curr. Opin. Nephrol. Hypertens. 1993, 2, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Huysmans, K.; Lins, R.L.; Daelemans, R.; Zachée, P.; De Broe, M. Hypertension and accelerated atherosclerosis in endstage renal disease. J. Nephrol. 1998, 11, 185–195. [Google Scholar] [PubMed]
- Amann, K.; Tyralla, K.; Gross, M.L.; Eifert, T.; Adamczak, M.; Ritz, E. Special characteristics of atherosclerosis in chronic renal failure. Clin. Nephrol. 2003, 60, S13–S21. [Google Scholar] [PubMed]
- Shanahan, C.M. Mechanisms of vascular calcification in CKD-evidence for premature ageing? Nat. Rev. Nephrol. 2013, 9, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Mezza, E.; Anania, P.; Iadarola, A.M.; Vischi, M.; Torazza, M.C.; Fop, F.; Guarena, C.; Martina, G.; Messina, M.; et al. Patients on renal replacement therapy for 20 or more years, a clinical profile. Nephrol. Dial. Transplant. 2002, 17, 1440–1449. [Google Scholar] [CrossRef] [PubMed]
- Block, G.A.; Hulbert-Shearon, T.E.; Levin, N.W.; Port, F.K. Association of serum phosphorus and calcium × phosphate product with mortality risk in chronic hemodialysis patients, a national study. Am. J. Kidney Dis. 1998, 31, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Block, G.A.; Port, F.K. Re-evaluation of risks associated with hyperphosphatemia and hyperparathyroidism in dialysis patients, recommendations for a change in management. Am. J. Kidney Dis. 2000, 35, 1226–1237. [Google Scholar] [CrossRef]
- Ganesh, S.K.; Stack, A.G.; Levin, N.W.; Hulbert-Shearon, T.; Port, F.K. Association of elevated serum PO(4), Ca × PO(4) product, and parathyroid hormone with cardiac mortality risk in chronic hemodialysis patients. J. Am. Soc. Nephrol. 2001, 12, 2131–2138. [Google Scholar] [PubMed]
- Tentori, F.; Blayney, M.J.; Albert, J.M.; Gillespie, B.W.; Kerr, P.G.; Bommer, J.; Young, E.W.; Akizawa, T.; Akiba, T.; Pisoni, R.L.; et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH, the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2008, 52, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R. Phosphate is a vascular toxin. Pediatr. Nephrol. 2013, 28, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Rivara, M.B.; Ravel, V.; Kalantar-Zadeh, K.; Streja, E.; Lau, W.L.; Nissenson, A.R.; Kestenbaum, B.; de Boer, I.H.; Himmelfarb, J.; Mehrotra, R. Uncorrected and Albumin-Corrected Calcium, Phosphorus, and Mortality in Patients Undergoing Maintenance Dialysis. J. Am. Soc. Nephrol. 2015, 26, 1671–1681. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.A. Hyperphosphatemia in Dialysis Patients, Beyond Nonadherence to Diet and Binders. Am. J. Kidney Dis. 2016, 67, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Lynch, K.E.; Lynch, R.; Curhan, G.C.; Brunelli, S.M. Prescribed dietary phosphate restriction and survival among hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, A.M.; Fouque, D.; Toft, A.J. Dietary phosphate assessment in dialysis patients. J. Ren. Nutr. 2010, 20, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.A.; Mehta, O. Dietary phosphorus restriction in dialysis patients, potential impact of processed meat, poultry, and fish products as protein sources. Am. J. Kidney Dis. 2009, 54, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Cuppari, L.; Kamimura, M.A. Dialysis, Dietary phosphorus restriction, changing the paradigm? Nat. Rev. Nephrol. 2011, 7, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Horne, R.; Cozzolino, M.; Kalantar-Zadeh, K. Balancing nutrition and serum phosphorus in maintenance dialysis. Am. J. Kidney Dis. 2014, 64, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Gutekunst, L.; Mehrotra, R.; Kovesdy, C.P.; Bross, R.; Shinaberger, C.S.; Noori, N.; Hirschberg, R.; Benner, D.; Nissenson, A.R.; et al. Understanding sources of dietary phosphorus in the treatment of patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Shinaberger, C.S.; Greenland, S.; Kopple, J.D.; Van Wyck, D.; Mehrotra, R.; Kovesdy, C.P.; Kalantar-Zadeh, K. Is controlling phosphorus by decreasing dietary protein intake beneficial or harmful in persons with chronic kidney disease? Am. J. Clin. Nutr. 2008, 88, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, C.; Piccoli, G.B.; Cupisti, A. The “phosphorus pyramid”: A visual tool for dietary phosphate management in dialysis and CKD patients. BMC Nephrol. 2015, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Copland, M.; Komenda, P.; Weinhandl, E.D.; McCullough, P.A.; Morfin, J.A. Intensive Hemodialysis, Mineral and Bone Disorder, and Phosphate Binder Use. Am. J. Kidney Dis. 2016, 68, S24–S32. [Google Scholar] [CrossRef] [PubMed]
- Daugirdas, J.T.; Chertow, G.M.; Larive, B.; Pierratos, A.; Greene, T.; Ayus, J.C.; Kendrick, C.A.; James, S.H.; Miller, B.W.; Schulman, G.; et al. Effects of frequent hemodialysis on measures of CKD mineral and bone disorder. J. Am. Soc. Nephrol. 2012, 23, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Johansen, K.L.; Lew, N.; Lazarus, J.M.; Lowrie, E.G. Vintage, nutritional status, and survival in hemodialysis patients. Kidney Int. 2000, 57, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Avram, M.M.; Mittman, N.; Fein, P.A.; Agahiu, S.; Hartman, W.; Chattopadhyay, N.; Matza, B. Dialysis vintage, body composition, and survival in peritoneal dialysis patients. Adv. Perit. Dial. 2012, 28, 144–147. [Google Scholar] [PubMed]
- Chauhan, V.; Chauhan, C.G. Dialysis vintage could confound survival trends in ESRD patients. Am. J. Kidney Dis. 2014, 64, 156. [Google Scholar] [CrossRef] [PubMed]
- Drechsler, C.; Krane, V.; Grootendorst, D.C.; Ritz, E.; Winkler, K.; März, W.; Dekker, F.; Wanner, C.; German Diabetes and Dialysis Study Investigators. The association between parathyroid hormone and mortality in dialysis patients is modified by wasting. Nephrol. Dial. Transplant. 2009, 24, 3151–3157. [Google Scholar] [CrossRef] [PubMed]
- Frazão, J.M.; Martins, P. Adynamic bone disease, clinical and therapeutic implications. Curr. Opin. Nephrol. Hypertens. 2009, 18, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Dukkipati, R.; Kovesdy, C.P.; Colman, S.; Budoff, M.J.; Nissenson, A.R.; Sprague, S.M.; Kopple, J.D.; Kalantar-Zadeh, K. Association of relatively low serum parathyroid hormone with malnutrition-inflammation complex and survival in maintenance hemodialysis patients. J. Ren. Nutr. 2010, 20, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Jean, G.; Lataillade, D.; Genet, L.; Legrand, E.; Kuentz, F.; Moreau-Gaudry, X.; Fouque, D.; ARNOS study investigators. Association between very low PTH levels and poor survival rates in haemodialysis patients, results from the French ARNOS cohort. Nephron Clin. Pract. 2011, 118, c211–c216. [Google Scholar] [CrossRef] [PubMed]
- Lertdumrongluk, P.; Rhee, C.M.; Park, J.; Lau, W.L.; Moradi, H.; Jing, J.; Molnar, M.Z.; Brunelli, S.M.; Nissenson, A.R.; Kovesdy, C.P.; et al. Association of serum phosphorus concentration with mortality in elderly and nonelderly hemodialysis patients. J. Ren. Nutr. 2013, 23, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Zitt, E.; Lamina, C.; Sturm, G.; Knoll, F.; Lins, F.; Freistätter, O.; Kronenberg, F.; Lhotta, K.; Neyer, U. Interaction of time-varying albumin and phosphorus on mortality in incident dialysis patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 2650–2656. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Heimbürger, O.; Paultre, F.; Diczfalusy, U.; Wang, T.; Berglund, L.; Jogestrand, T. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999, 55, 1899–1911. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Stenvinkel, P.; Pillon, L.; Kopple, J.D. Inflammation and nutrition in renal insufficiency. Adv. Ren. Replace Ther. 2003, 10, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Okazaki, M.; Tsuchiya, K.; Kawaguchi, H.; Nitta, K. Geriatric Nutritional Risk Index Is a Simple Predictor of Mortality in Chronic Hemodialysis Patients. Blood Purif. 2015, 39, 281–287. [Google Scholar]
- Panichi, V.; Cupisti, A.; Rosati, A.; Di Giorgio, A.; Scatena, A.; Menconi, O.; Bozzoli, L.; Bottai, A. Geriatric nutritional risk index is a strong predictor of mortality in hemodialysis patients, data from the Riscavid cohort. J. Nephrol. 2014, 27, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.A.; Cordeiro, A.C.; Avesani, C.M.; Carrero, J.J.; Lindholm, B.; Amparo, F.C.; Amodeo, C.; Cuppari, L.; Kamimura, M.A. Sarcopenia in chronic kidney disease on conservative therapy, prevalence and association with mortality. Nephrol. Dial. Transplant. 2015, 30, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Fish, J.C.; Remmers, A.R., Jr.; Lindley, J.D.; Sarles, H.E. Albumin kinetics and nutritional rehabilitation in the unattended home-dialysis patient. N. Engl. J. Med. 1972, 287, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Blagg, C.R.; Scribner, B.H. Diet, drugs and dialysis in the management of chronic renal failure. Prog. Biochem. Pharmacol. 1972, 7, 452–497. [Google Scholar] [PubMed]
- Mackenzie, J.C. Nutrition and dialysis. World Rev. Nutr. Diet. 1971, 13, 194–276. [Google Scholar] [PubMed]
- Ginn, H.E. Nutritional aspects of chronic renal dialysis. South. Med. J. 1969, 62, 1471–1476. [Google Scholar] [CrossRef] [PubMed]
- Lowrie, E.G.; Lew, N.L. Death risk in hemodialysis patients, the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am. J. Kidney Dis 1990, 15, 458–482. [Google Scholar] [CrossRef]
- Kaminski, M.V., Jr.; Lowrie, E.G.; Rosenblatt, S.G.; Haase, T. Malnutrition is lethal, diagnosable, and treatable in ESRD patients. Transplant. Proc. 1991, 23, 1810–1815. [Google Scholar] [PubMed]
- Owen, W.F., Jr.; Lew, N.L.; Liu, Y.; Lowrie, E.G.; Lazarus, J.M. The urea reduction ratio and serum albumin concentration as predictors of mortality in patients undergoing hemodialysis. N. Engl. J. Med. 1993, 329, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Goldwasser, P.; Mittman, N.; Antignani, A.; Burrell, D.; Michel, M.A.; Collier, J.; Avram, M.M. Predictors of mortality in hemodialysis patients. J. Am. Soc. Nephrol. 1993, 9, 1613–1622. [Google Scholar]
- Avram, M.M.; Bonomini, L.V.; Sreedhara, R.; Mittman, N. Predictive value of nutritional markers (albumin, creatinine, cholesterol, and hematocrit) for patients on dialysis for up to 30 years. Am. J. Kidney Dis. 1996, 28, 910–917. [Google Scholar] [CrossRef]
- Maggiore, Q.; Nigrelli, S.; Ciccarelli, C.; Grimaldi, C.; Rossi, G.A.; Michelassi, C. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int. 1996, 50, 2103–2108. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003, 63, 793–808. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kilpatrick, R.D.; Kuwae, N.; Wu, D.Y. Reverse epidemiology, a spurious hypothesis or a hardcore reality? Blood Purif. 2005, 23, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Lowrie, E.G. Acute-phase inflammatory process contributes to malnutrition, anemia, and possibly other abnormalities in dialysis patients. Am. J. Kidney Dis. 1998, 32, S105–S112. [Google Scholar] [CrossRef]
- Stenvinkel, P. Inflammatory and atherosclerotic interactions in the depleted uremic patient. Blood Purif. 2001, 19, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Humphreys, M.H.; Block, G. Comparing outcome predictability of markers of malnutrition-inflammation complex syndrome in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1507–1519. [Google Scholar] [CrossRef] [PubMed]
- NKF. KDOQI—Clinical Practice Guidelines for Hemodialysis Adequacy. Am. J. Kidney Dis. 2006, 48, S2–S90. [Google Scholar]
- Beto, J.A.; Ramirez, W.E.; Bansal, V.K. Medical nutrition therapy in adults with chronic kidney disease, integrating evidence and consensus into practice for the generalist registered dietitian nutritionist. J. Acad. Nutr. Diet. 2014, 114, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Trudel, T.; McCune, A.; Donahue, K.; Zuberbuhler, L.; Farmer, A.; Mager, D. Variables influencing adoption of practice-based guidelines in Canadian renal dietetic practice. J. Ren. Nutr. 2010, 20, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Toigo, G.; Aparicio, M.; Attman, P.O.; Cano, N.; Cianciaruso, B.; Engel, B.; Fouque, D.; Heidland, A.; Teplan, V.; Wanner, C. Expert working group report on nutrition in adult patients with renal insufficiency (Part 2 of 2). Clin. Nutr. 2000, 19, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Vennegoor, M.; ter Wee, P.; Wanner, C.; Basci, A.; Canaud, B.; Haage, P.; Konner, K.; Kooman, J.; Martin-Malo, A.; et al. EBPG guideline on nutrition. Nephrol. Dial. Transplant. 2007, 22, ii45–ii87. [Google Scholar] [CrossRef] [PubMed]
- Combe, C.; McCullough, K.P.; Asano, Y.; Ginsberg, N.; Maroni, B.J.; Pifer, T.B. Kidney Disease Outcomes Quality Initiative (K/DOQI) and the Dialysis Outcomes and Practice Patterns Study (DOPPS), nutrition guidelines, indicators, and practices. Am. J. Kidney Dis 2004, 44, 39–46. [Google Scholar] [CrossRef]
- Hecking, E.; Bragg-Gresham, J.L.; Rayner, H.C.; Pisoni, R.L.; Andreucci, V.E.; Combe, C.; Greenwood, R.; McCullough, K.; Feldman, H.I.; Young, E.W.; et al. Haemodialysis prescription, adherence and nutritional indicators in five European countries, results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2004, 19, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; Hanson, C.S.; Craig, J.C.; Strippoli, G.F.; Ruospo, M.; Campbell, K.; Johnson, D.W.; Tong, A. Dietary and fluid restrictions in CKD: A thematic synthesis of patient views from qualitative studies. Am. J. Kidney Dis. 2015, 65, 559–573. [Google Scholar] [CrossRef] [PubMed]
- Galland, R.; Traeger, J. Short daily hemodialysis and nutritional status in patients with chronic renal failure. Semin. Dial. 2004, 17, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Spanner, E.; Suri, R.; Heidenheim, A.P.; Lindsay, R.M. The impact of quotidian hemodialysis on nutrition. Am. J. Kidney Dis. 2003, 42, 30–35. [Google Scholar] [CrossRef]
- Kjellstrand, C.; Buoncristiani, U.; Ting, G.; Traeger, J.; Piccoli, G.B.; Sibai-Galland, R.; Young, B.A.; Blagg, C.R. Survival with short-daily hemodialysis, association of time, site, and dose of dialysis. Hemodial. Int. 2010, 14, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Ipema, K.J.; Struijk, S.; van der Velden, A.; Westerhuis, R.; van der Schans, C.P.; Gaillard, C.A.J.M.; Krijnen, W.P.; Franssen, C.F.M. Nutritional Status in Nocturnal Hemodialysis Patients—A Systematic Review with Meta-Analysis. PLoS ONE 2016, 11, e0157621. [Google Scholar] [CrossRef] [PubMed]
- Demirci, C.; Ozkahya, M.; Demirci, M.S.; Asci, G.; Kose, T.; Colak, T.; Duman, S.; Toz, H.; Ergin, P.; Adam, S.M.; et al. Effects of three times weekly eight-hour nocturnal hemodialysis on volume and nutritional status. Am. J. Nephrol. 2013, 37, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Minelli, F.; Versino, E.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Rolfo, A.; Giuffrida, D.; Colombi, N.; Pani, A.; Todros, T. Pregnancy in dialysis patients in the new millennium: A systematic review and meta-regression analysis correlating dialysis schedules and pregnancy outcomes. Nephrol. Dial. Transplant. 2016, 31, 1915–1934. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.; Schatell, D. Intensive dialysis and pregnancy. Hemodial. Int. 2016, 20, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.H.; Hsu, C.W.; Hu, C.C.; Yen, T.H.; Huang, W.H. Association Between Hemodiafiltration and Hypoalbuminemia in Middle-Age Hemodialysis Patients. Medicine 2016, 95, e3334. [Google Scholar] [CrossRef] [PubMed]
- Fournier, A.; Birmelé, B.; François, M.; Prat, L.; Halimi, J.M. Factors associated with albumin loss in post-dilution hemodiafiltration and nutritional consequences. Int. J. Artif. Organs 2015, 38, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Orasan, R.A.; Patiu, I.M.; Anghel, D.; Bejan, C.; Iosub, L.; Totolici, C.; Pop, M.; Turcea, C.; Teodoru, C.; Orasan, O.H.; et al. Variation of clinical and laboratory features in chronic dialysis patients treated with high-flux hemodialysis after switching to online hemodiafiltration. Int. Urol. Nephrol. 2013, 45, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Cross, J.; Davenport, A. Does online hemodiafiltration lead to reduction in trace elements and vitamins? Hemodial. Int. 2011, 15, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Masakane, I. Choice of modality with the use of high-performance membrane and evaluation for clinical effects. Contrib. Nephrol. 2011, 173, 84–94. [Google Scholar] [PubMed]
- Vega, A.; Quiroga, B.; Abad, S.; Aragoncillo, I.; Arroyo, D.; Panizo, N.; López-Gómez, J.M. Albumin leakage in online hemodiafiltration, more convective transport, more losses? Ther. Apher. Dial. 2015, 19, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Guest, S. Hypoalbuminemia in peritoneal dialysis patients. Adv. Perit. Dial. 2013, 29, 55–60. [Google Scholar] [PubMed]
- Rippe, B.; Öberg, C.M. Albumin Turnover in Peritoneal and Hemodialysis. Semin. Dial. 2016, 29, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.; Sayre, S.S.; Leon, J.B.; Machekano, R.; Love, T.E.; Porter, D.; Marbury, M.; Sehgal, A.R. Effect of food additives on hyperphosphatemia among patients with end-stage renal disease, a randomized controlled trial. JAMA 2009, 301, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Sarathy, S.; Sullivan, C.; Leon, J.B.; Sehgal, A.R. Fast food, phosphorus-containing additives, and the renal diet. J. Ren. Nutr. 2008, 18, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; Kalantar-Zadeh, K. Management of natural and added dietary phosphorus burden in kidney disease. Semin. Nephrol. 2013, 33, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Shutto, Y.; Shimada, M.; Kitajima, M.; Yamabe, H.; Razzaque, M.S. Lack of awareness among future medical professionals about the risk of consuming hidden phosphate-containing processed food and drinks. PLoS ONE 2011, 6, e29105. [Google Scholar] [CrossRef] [PubMed]
- Benini, O.; D’Alessandro, C.; Gianfaldoni, D.; Cupisti, A. Extra-phosphate load from food additives in commonly eaten foods, a real and insidious danger for renal patients. J. Ren. Nutr. 2011, 21, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Ornish, D. Holy Cow! What’s good for you is good for our planet, comment on “Red Meat Consumption and Mortality”. Arch. Intern. Med. 2012, 172, 563–564. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Aragoncillo, I.; Arroyo, D.; Panizo, N.; López-Gómez, J.M. Red meat consumption and mortality, results from 2 prospective cohort studies. Arch. Intern. Med. 2012, 172, 555–563. [Google Scholar] [PubMed]
- Larsson, S.C.; Orsini, N. Red meat and processed meat consumption and all-cause mortality, a meta-analysis. Am. J. Epidemiol. 2014, 179, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Abete, I.; Romaguera, D.; Vieira, A.R.; Lopez de Munain, A.; Norat, T. Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality, a meta-analysis of cohort studies. Br. J. Nutr. 2014, 112, 762–775. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and processed meat consumption and mortality, dose-response meta-analysis of prospective cohort studies. Public Health Nutr. 2016, 19, 893–905. [Google Scholar] [CrossRef] [PubMed]
- Downer, M.K.; Martínez-González, M.A.; Gea, A.; Stampfer, M.; Warnberg, J.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Ros, E.; Fitó, M.; et al. Mercury exposure and risk of cardiovascular disease: A nested case-control study in the PREDIMED (PREvention with MEDiterranean Diet) study. BMC Cardiovasc. Disord. 2017, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Fish, mercury, selenium and cardiovascular risk, current evidence and unanswered questions. Int. J. Environ. Res. Public Health 2009, 6, 1894–1916. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Hemmelgarn, B.; Klarenbach, S.; Field, C.; Manns, B.; Thadhani, R.; Gill, J.; The Alberta Kidney Disease Network. Trace elements in hemodialysis patients, a systematic review and meta-analysis. BMC Med. 2009, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Rucker, D.; Thadhani, R.; Tonelli, M. Trace element status in hemodialysis patients. Semin. Dial. 2010, 23, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, L.; Green, S.R.; Radhakrishnan, H.; Kadavanu, T.M.; Ramachandrappa, A.; Tiwari, S.R.; Rajkumar, A.L.; Govindasamy, E. Trace Elements in Chronic Haemodialysis Patients and Healthy Individuals—A Comparative Study. J. Clin. Diagn. Res. 2016, 10, OC14–OC17. [Google Scholar] [PubMed]
- Caglar, K.; Hakim, R.M.; Ikizler, T.A. Approaches to the reversal of malnutrition, inflammation, and atherosclerosis in end-stage renal disease. Nutr. Rev. 2002, 60, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Ipema, K.J.; van der Schans, C.P.; Vonk, N.; de Vries, J.M.; Westerhuis, R.; Duym, E.; Franssen, C.F. A difference between day and night, protein intake improves after the transition from conventional to frequent nocturnal home hemodialysis. J. Ren. Nutr. 2012, 22, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Maduell, F.; Arias, M.; Durán, C.E.; Vera, M.; Fontseré, N.; Azqueta, M.; Rico, N.; Pérez, N.; Sentis, A.; Elena, M.; et al. Nocturnal, every-other-day, online haemodiafiltration: An effective therapeutic alternative. Nephrol. Dial. Transplant. 2012, 27, 1619–1631. [Google Scholar] [CrossRef] [PubMed]
- Rocco, M.V.; Lockridge, R.S., Jr.; Beck, G.J.; Eggers, P.W.; Gassman, J.J.; Greene, T.; Larive, B.; Chan, C.T.; Chertow, G.M.; Frequent Hemodialysis Network (FHN) Trial Group. The effects of frequent nocturnal home hemodialysis, the Frequent Hemodialysis Network Nocturnal Trial. Kidney Int. 2011, 80, 1080–1091. [Google Scholar] [CrossRef] [PubMed]
- Schorr, M.; Manns, B.J.; Culleton, B.; Walsh, M.; Klarenbach, S.; Tonelli, M.; Sauve, L.; Chin, R.; Barnieh, L.; Hemmelgarn, B.R.; et al. The effect of nocturnal and conventional hemodialysis on markers of nutritional status, results from a randomized trial. J. Ren. Nutr. 2011, 21, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R.M.; Daily/Nocturnal Dialysis Study Group. The London, Ontario, Daily/Nocturnal Hemodialysis Study. Semin. Dial. 2004, 17, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.W.; Chebrolu, S.B.; Ing, T.S.; Ting, G.; Blagg, C.R.; Twardowski, Z.J.; Woredekal, Y.; Delano, B.; Gandhi, V.C.; Kjellstrand, C.M.; et al. Early clinical, quality-of-life, and biochemical changes of “daily hemodialysis” (6 dialyses per week). Am. J. Kidney Dis. 2004, 43, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Pierratos, A. Daily (quotidian) nocturnal home hemodialysis, nine years later. Hemodial. Int. 2001, 8, 45–50. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Kümpers, P.; Eisenbach, G.M.; Haller, H.; Kielstein, J.T. Prospective evaluation of an in-centre conversion from conventional haemodialysis to an intensified nocturnal strategy. Nephrol. Dial. Transplant. 2009, 24, 2232–2240. [Google Scholar] [CrossRef] [PubMed]
- Brady, J.P.; Hasbargen, J.A. Correction of metabolic acidosis and its effect on albumin in chronic hemodialysis patients. Am. J. Kidney Dis. 1998, 31, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J.; Levin, N.W.; Delmez, J.; Depner, T.A.; Ornt, D.; Owen, W.; Yan, G. Association of acidosis and nutritional parameters in hemodialysis patients. Am. J. Kidney Dis. 1999, 34, 493–499. [Google Scholar] [CrossRef]
- Bergström, J. Metabolic acidosis and nutrition in dialysis patients. Blood Purif. 1995, 13, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Vashistha, T.; Kalantar-Zadeh, K.; Molnar, M.Z.; Torlén, K.; Mehrotra, R. Dialysis modality and correction of uremic metabolic acidosis, relationship with all-cause and cause-specific mortality. Clin. J. Am. Soc. Nephrol. 2013, 8, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.; Bonello, F.; Massara, C.; Salomone, M.; Maffei, S.; Iadarola, G.M.; Stramignoni, E.; Rosati, C.; Borca, M.; Belardi, P.; et al. Death in conditions of cachexia, the price for the dialysis treatment of the elderly? Kidney Int. Suppl. 1993, 41, S282–S286. [Google Scholar] [PubMed]
- Pecoits-Filho, R.; Lindholm, B.; Stenvinkel, P. The malnutrition, inflammation, and atherosclerosis (MIA) syndrome—The heart of the matter. Nephrol. Dial. Transplant. 2002, 17, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Quresh, A.R.; Alvestrand, A.; Divino-Filho, J.C.; Gutierrez, A.; Heimbürger, O.; Lindholm, B.; Bergström, J. Inflammation, malnutrition, and cardiac disease as predictors of mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2002, 13, S28–S36. [Google Scholar]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D. Relative contributions of nutrition and inflammation to clinical outcome in dialysis patients. Am. J. Kidney Dis. 2001, 38, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Doshi, M.; Streja, E.; Rhee, C.M.; Park, J.; Ravel, V.A.; Soohoo, M.; Moradi, H.; Lau, W.L.; Mehrotra, R.; Kuttykrishnan, S.; et al. Examining the robustness of the obesity paradox in maintenance hemodialysis patients, a marginal structural model analysis. Nephrol. Dial. Transplant. 2016, 31, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, S.; Yilmaz, R.; Akinci, D.; Arici, M.; Altun, B.; Erdem, Y.; Yasavul, U.; Turgan, C. U-shaped association of body mass index with inflammation and atherosclerosis in hemodialysis patients. J. Ren. Nutr. 2005, 15, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Kwan, B.C.; Murtaugh, M.A.; Beddhu, S. Associations of body size with metabolic syndrome and mortality in moderate chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2007, 2, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Beddhu, S. The body mass index paradox and an obesity, inflammation, and atherosclerosis syndrome in chronic kidney disease. Semin. Dial. 2004, 17, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.C.; Lin, H.Y.; Lim, L.M.; Chen, S.C.; Chang, J.M.; Hwang, S.J.; Tsai, J.C.; Hung, C.C.; Chen, H.C. Body mass index, mortality, and gender difference in advanced chronic kidney disease. PLoS ONE 2015, 10, e0126668. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Delos Santos, R.; Axelrod, D.; Schnitzler, M.A.; Brennan, D.C.; Tuttle-Newhall, J.E. Obesity and kidney transplant candidates, how big is too big for transplantation? Am. J. Nephrol. 2012, 36, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.T.; Danovitch, G.M.; Pham, P.C. Kidney transplantation in the obese transplant candidates, to transplant or not to transplant? Semin. Dial. 2013, 26, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Orlic, L.; Mikolasevic, I.; Jakopcic, I.; Grskovic, A.; Jelic Pranjic, I.; Racki, S.; Stimac, D. Body mass index, short- and long-term impact on kidney transplantation. Int. J. Clin. Pract. 2015, 69, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.M.; Hajjiri, Z.; Metwally, A.; Finn, P.W.; Perkins, D.L. Effect of the Obesity Epidemic on Kidney Transplantation, Obesity Is Independent of Diabetes as a Risk Factor for Adverse Renal Transplant Outcomes. PLoS ONE 2016, 11, e0165712. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, B.; Bridson, J.M.; Sharma, A.; Halawa, A. From chronic kidney disease to kidney transplantation: The impact of obesity and its treatment modalities. Transplant. Rev. 2016, 30, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Molnar, M.Z.; Streja, E.; Kovesdy, C.P.; Bunnapradist, S.; Sampaio, M.S.; Jing, J.; Krishnan, M.; Nissenson, A.R.; Danovitch, G.M.; Kalantar-Zadeh, K. Associations of body mass index and weight loss with mortality in transplant-waitlisted maintenance hemodialysis patients. Am. J. Transplant. 2011, 11, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Schold, J.D.; Srinivas, T.R.; Guerra, G.; Reed, A.I.; Johnson, R.J.; Weiner, I.D.; Oberbauer, R.; Harman, J.S.; Hemming, A.W.; Meier-Kriesche, H.U. A “weight-listing”paradox for candidates of renal transplantation? Am. J. Transplant. 2007, 7, 550–559. [Google Scholar] [CrossRef] [PubMed]
- McClellan, W.M.; Plantinga, L.C. A public health perspective on CKD and obesity. Nephrol. Dial. Transplant. 2013, 28, iv37–iv42. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Zoccali, C.; Ikizler, T.A. Obesity in CKD—What should nephrologists know? J. Am. Soc. Nephrol. 2013, 24, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Hricik, D.E. Metabolic syndrome in kidney transplantation, management of risk factors. Clin. J. Am. Soc. Nephrol. 2011, 6, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Imam, T.H.; Fischer, H.; Jing, B.; Burchette, R.; Henry, S.; DeRose, S.F.; Coleman, K.J. Estimated GFR Before and After Bariatric Surgery in CKD. Am. J. Kidney Dis. 2017, 69, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Teta, D. Weight loss in obese patients with chronic kidney disease, who and how? J. Ren. Care 2010, 36, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Neel, J.V. Diabetes mellitus, a “thrifty” genotype rendered detrimental by “progress”? Am. J. Hum. Genet. 1962, 14, 353–362. [Google Scholar] [PubMed]
- Stefan, N.; Artunc, F.; Heyne, N.; Machann, J.; Schleicher, E.D.; Häring, H.U. Obesity and renal disease, not all fat is created equal and not all obesity is harmful to the kidneys. Nephrol. Dial. Transplant. 2016, 31, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Torino, C.; Tripepi, G.; Mallamaci, F. Assessment of obesity in chronic kidney disease, what is the best measure? Curr. Opin. Nephrol. Hypertens. 2012, 21, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Vigotti, F.N.; Teta, L.; Pia, A.; Mirasole, S.; Guzzo, G.; Giuffrida, D.; Capizzi, I.; Avagnina, P.; Ippolito, D.; Piccoli, G.B. Intensive weight loss combining flexible dialysis with a personalized, ad libitum, coach-assisted diet program. A “pilot” case series. Hemodial. Int. 2015, 19, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Young, G.A.; Parsons, F.M. Amino nitrogen loss during haemodialysis, its dietary significance and replacement. Clin. Sci. 1966, 31, 299–307. [Google Scholar] [PubMed]
- Kurella, M.; Covinsky, K.E.; Collins, A.J.; Chertow, G.M. Octogenarians and nonagenarians starting dialysis in the United States. Ann. Intern. Med. 2007, 146, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Seckinger, J.; Dschietzig, W.; Leimenstoll, G.; Rob, P.M.; Kuhlmann, M.K.; Pommer, W.; Fraass, U.; Ritz, E.; Schwenger, V. Morbidity, mortality and quality of life in the ageing haemodialysis population, results from the ELDERLY study. Clin. Kidney J. 2016, 9, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Chauveau, P.; Combe, C.; Fouque, D.; Aparicio, M. Vegetarianism, advantages and drawbacks in patients with chronic kidney diseases. J. Ren. Nutr. 2013, 23, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Long, Q.; Shao, C.; Fan, H.; Yuan, L.; Huang, B.; Gu, Y.; Lin, S.; Hao, C.; Chen, J. Effect of short-term low-protein diet supplemented with keto acids on hyperphosphatemia in maintenance hemodialysis patients. Blood Purif. 2011, 31, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Qian, J.; Sun, W.; Lin, A.; Cao, L.; Wang, Q.; Ni, Z.; Wan, Y.; Linholm, B.; Axelsson, J.; Yao, Q. Better preservation of residual renal function in peritoneal dialysis patients treated with a low-protein diet supplemented with keto acids, a prospective, randomized trial. Nephrol. Dial. Transplant. 2009, 24, 2551–2558. [Google Scholar] [CrossRef] [PubMed]
- Fissell, R.B.; Karaboyas, A.; Bieber, B.A.; Sen, A.; Li, Y.; Lopes, A.A.; Akiba, T.; Bommer, J.; Ethier, J.; Jadoul, M.; et al. Phosphate binder pill burden, patient-reported non-adherence, and mineral bone disorder markers: Findings from the DOPPS. Hemodial. Int. 2016, 20, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, K.; Braunhofer, P.; Newsome, B.; Lubeck, D.; Wang, S.; Deuson, J.; Claxton, A.J. The economic impact of improving phosphate binder therapy adherence and attainment of guideline phosphorus goals in hemodialysis patients, a Medicare cost-offset model. Adv. Ther. 2014, 31, 1272–1286. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Alfieri, T.; Ramakrishnan, K.; Braunhofer, P.; Newsome, B.A. Serum phosphorus levels and pill burden are inversely associated with adherence in patients on hemodialysis. Nephrol. Dial. Transplant. 2014, 29, 2092–2099. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.W.; Teitelbaum, I.; Misra, M.; de Leon, E.M.; Adzize, T.; Mehrotra, R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- St-Jules, D.E.; Woolf, K.; Pompeii, M.L.; Sevick, M.A. Exploring Problems in Following the Hemodialysis Diet and Their Relation to Energy and Nutrient Intakes: The BalanceWise Study. J. Ren. Nutr. 2016, 26, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R.M.; Spanner, E.; Heidenheim, R.P.; LeFebvre, J.M.; Hodsman, A.; Baird, J.; Allison, M.E. Which comes first, Kt/V or PCR—Chicken or egg? Kidney Int. Suppl. 1992, 38, S32–S36. [Google Scholar] [PubMed]
- Lindsay, R.M.; Bergström, J. Membrane biocompatibility and nutrition in maintenance haemodialysis patients. Nephrol. Dial. Transplant. 1994, 9, 150–155. [Google Scholar] [PubMed]
- Kloppenburg, W.D.; Stegeman, C.A.; Hovinga, T.K.; Vastenburg, G.; Vos, P.; de Jong, P.E.; Huisman, R.M. Effect of prescribing a high protein diet and increasing the dose of dialysis on nutrition in stable chronic haemodialysis patients, a randomized, controlled trial. Nephrol. Dial. Transplant. 2004, 19, 1212–1223. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Altieri, P.; Andrulli, S.; Bolasco, P.; Sau, G.; Pedrini, L.A.; Basile, C.; David, S.; Feriani, M.; Montagna, G.; et al. Hemofiltration and hemodiafiltration reduce intradialytic hypotension in ESRD. J. Am. Soc. Nephrol. 2010, 21, 1798–1807. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, K.; Minakuchi, J. Clinical benefits of predilution on-line hemodiafiltration. Blood Purif. 2013, 35, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Masakane, I. How to prescribe hemodialysis or hemodiafiltration in order to ameliorate dialysis-related symptoms and complications. Contrib. Nephrol. 2011, 168, 53–63. [Google Scholar] [PubMed]
- Locatelli, F.; Martin-Malo, A.; Hannedouche, T.; Loureiro, A.; Papadimitriou, M.; Wizemann, V.; Jacobson, S.H.; Czekalski, S.; Ronco, C.; Vanholder, R.; et al. Effect of membrane permeability on survival of hemodialysis patients. J. Am. Soc. Nephrol. 2009, 20, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Nubé, M.J.; Peters, S.A.; Blankestijn, P.J.; Canaud, B.; Davenport, A.; Grooteman, M.P.; Asci, G.; Locatelli, F.; Maduell, F.; HDF Pooling Project investigators. Mortality reduction by post-dilution online-haemodiafiltration: A cause-specific analysis. Nephrol. Dial. Transplant. 2016. [Google Scholar] [CrossRef]
- Blankestijn, P.J. Haemodiafiltration, becoming the new standard? Nephrol. Dial. Transplant. 2013, 28, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Mostovaya, I.M.; Grooteman, M.P.; Basile, C.; Davenport, A.; de Roij van Zuijdewijn, C.L.; Wanner, C.; Nubé, M.J.; Blankestijn, P.J. High convection volume in online post-dilution haemodiafiltration, relevance, safety and costs. Clin. Kidney J. 2015, 8, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Canaud, B.; Bragg-Gresham, J.L.; Marshall, M.R.; Desmeules, S.; Gillespie, B.W.; Depner, T.; Klassen, P.; Port, F.K. Mortality risk for patients receiving hemodiafiltration versus hemodialysis, European results from the DOPPS. Kidney Int. 2006, 69, 2087–2093. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, K.; Minakuchi, J. Albumin loss under the use of the high-performance membrane. Contrib. Nephrol. 2011, 173, 76–83. [Google Scholar] [PubMed]
- Kirschbaum, B. The decline in serum albumin after conversion to high flux, high efficiency dialysis. Artif. Organs 1994, 18, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Mineshima, M. Optimal Design of Dialyzers. Contrib. Nephrol. 2017, 189, 204–209. [Google Scholar] [PubMed]
- Ikizler, T.A. Using and interpreting serum albumin and prealbumin as nutritional markers in patients on chronic dialysis. Semin. Dial. 2014, 27, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Mittman, N.; Avram, M.M.; Oo, K.K.; Chattopadhyay, J. Serum prealbumin predicts survival in hemodialysis and peritoneal dialysis, 10 years of prospective observation. Am. J. Kidney Dis. 2001, 38, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Sreedhara, R.; Avram, M.M.; Blanco, M.; Batish, R.; Avram, M.M.; Mittman, N. Prealbumin is the best nutritional predictor of survival in hemodialysis and peritoneal dialysis. Am. J. Kidney Dis. 1996, 28, 937–942. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Martin-Calvo, N. Mediterranean diet and life expectancy, beyond olive oil, fruits, and vegetables. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.; Wareham, N.J.; Khaw, K.T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-Mediterranean population, the EPIC-Norfolk study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, T.; Ninomiya, T.; Wang, A.; Neal, B.; Jun, M.; Wong, M.G.; Jardine, M.; Hillis, G.S.; Perkovic, V. Effects of the Mediterranean Diet on Cardiovascular Outcomes—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0159252. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. The Mediterranean diet and mortality—Olive oil and beyond. N. Engl. J. Med. 2003, 348, 2595–2596. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; PREDIMED Study Investigators. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Flint, A.J.; Qi, Q.; van Dam, R.M.; Sampson, L.A.; Rimm, E.B.; Holmes, M.D.; Willett, W.C.; Hu, F.B.; Sun, Q. Association between dietary whole grain intake and risk of mortality, two large prospective studies in US men and women. JAMA Intern. Med. 2015, 175, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.; Bauman, A.; Gale, J.; Banks, E.; Kritharides, L.; Ding, D. Fruit and vegetable consumption and all-cause mortality, evidence from a large Australian cohort study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Stefler, D.; Pikhart, H.; Kubinova, R.; Pajak, A.; Stepaniak, U.; Malyutina, S.; Simonova, G.; Peasey, A.; Marmot, M.G.; Bobak, M. Fruit and vegetable consumption and mortality in Eastern Europe, Longitudinal results from the Health, Alcohol and Psychosocial Factors in Eastern Europe study. Eur. J. Prev. Cardiol. 2016, 23, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, O.M.; Muntner, P.; Rizk, D.V.; McClellan, W.M.; Warnock, D.G.; Newby, P.K.; Judd, S.E. Dietary patterns and risk of death and progression to ESRD in individuals with CKD: A cohort study. Am. J. Kidney Dis. 2014, 64, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Bakris, G.L.; Pitt, B.; Weir, M.R.; Freeman, M.W.; Mayo, M.R.; Garza, D.; Stasiv, Y.; Zawadzki, R.; Berman, L.; Bushinsky, D.A. AMETHYST-DN Investigators. Effect of Patiromer on Serum Potassium Level in Patients WITH Hyperkalemia and Diabetic Kidney Disease: The AMETHYST-DN Randomized Clinical Trial. JAMA 2015, 314, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Kosiborod, M.; Rasmussen, H.S.; Lavin, P.; Qunibi, W.Y.; Spinowitz, B.; Packham, D.; Roger, S.D.; Yang, A.; Lerma, E.; Singh, B. Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia: The HARMONIZE randomized clinical trial. JAMA 2014, 312, 2223–2233. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Updates in hyperkalemia: Outcomes and therapeutic strategies. Rev. Endocr. Metab. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Meaney, C.J.; Beccari, M.V.; Yang, Y.; Zhao, J. Systematic Review and Meta-Analysis of Patiromer and Sodium Zirconium Cyclosilicate: A New Armamentarium for the Treatment of Hyperkalemia. Pharmacotherapy 2017. [Google Scholar] [CrossRef] [PubMed]
- Buoncristiani, U.; Quintaliani, G.; Cozzari, M.; Giombini, L.; Ragaiolo, M. Daily dialysis, long-term clinical metabolic results. Kidney Int. Suppl. 1988, 24, S137–S140. [Google Scholar] [PubMed]
- Raj, D.S.; Charra, B.; Pierratos, A.; Work, J. In search of ideal hemodialysis, is prolonged frequent dialysis the answer? Am. J. Kidney Dis. 1999, 34, 597–610. [Google Scholar] [CrossRef]
- Weinhandl, E.D.; Gilbertson, D.T.; Collins, A.J. Mortality, Hospitalization, and Technique Failure in Daily Home Hemodialysis and Matched Peritoneal Dialysis Patients: A Matched Cohort Study. Am. J. Kidney Dis. 2016, 67, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Woods, J.D.; Port, F.K.; Stannard, D.; Blagg, C.R.; Held, P.J. Comparison of mortality with home hemodialysis and center hemodialysis: A national study. Kidney Int. 1996, 49, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Arkouche, W.; Traeger, J.; Delawari, E.; Sibaï-Galland, R.; Abdullah, E.; Galland, R.; Leitienne, P.; Fouque, D.; Laville, M. Twenty-five years of experience with out-center hemodialysis. Kidney Int. 1999, 56, 2269–2275. [Google Scholar] [CrossRef] [PubMed]
- Ting, G.O.; Kjellstrand, C.; Freitas, T.; Carrie, B.J.; Zarghamee, S. Long-term study of high-comorbidity ESRD patients converted from conventional to short daily hemodialysis. Am. J. Kidney Dis. 2003, 42, 1020–1035. [Google Scholar] [CrossRef] [PubMed]
- Puñal, J.; Lema, L.V.; Sanhez-Guisande, D.; Ruano-Ravina, A. Clinical effectiveness and quality of life of conventional haemodialysis versus short daily haemodialysis, a systematic review. Nephrol. Dial. Transplant. 2008, 23, 2634–2646. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Ferraresi, M.; Consiglio, V.; Scognamiglio, S.; Deagostini, M.C.; Randone, O.; Vigotti, F.N.; Calderale, P.M. Why home hemodialysis? A systematic “marketing” analysis. J. Nephrol. 2012, 25, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, T.; Kotanko, P.; Goffin, E.; Kooman, J.P.; van der Sande, F.M.; Chan, C.T. Can intensive hemodialysis prevent loss of functionality in the elderly ESRD patient? Semin. Dial. 2011, 24, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Mezza, E.; Quaglia, M.; Bermond, F.; Bechis, F.; Burdese, M.; Gai, M.; Pacitti, A.; Jeantet, A.; Segoloni, G.P.; Piccoli, G. Flexibility as an implementation strategy for a daily dialysis program. J. Nephrol. 2003, 16, 365–372. [Google Scholar] [PubMed]
- Takahashi, S. Future home hemodialysis—Advantages of the NxStage System One. Contrib. Nephrol. 2012, 177, 117–126. [Google Scholar] [PubMed]
- Buoncristiani, U.; Giombini, L.; Cozzari, M.; Carobi, C.; Quintaliani, G.; Brugnano, R. Daily recycled bicarbonate dialysis with polyacrylonitrile. Trans. Am. Soc. Artif. Intern. Organs 1983, 29, 669–672. [Google Scholar] [PubMed]
- Lockridge, R.S., Jr.; Pipkin, M. Short and long nightly hemodialysis in the United States. Hemodial. Int. 2008, 12, S48–S50. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Barta, V.; Thakkar, I.; Sakhiya, V.; Miller, I. Pregnancy outcomes in women on hemodialysis, a national survey. Clin. Kidney J. 2017. [Google Scholar] [CrossRef]
- Vilar, E.; Fry, A.C.; Wellsted, D.; Tattersall, J.E.; Greenwood, R.N.; Farrington, K. Long-term outcomes in online hemodiafiltration and high-flux hemodialysis, a comparative analysis. Clin. J. Am. Soc. Nephrol. 2009, 4, 1944–1953. [Google Scholar] [CrossRef] [PubMed]
- Panichi, V.; Rizza, G.M.; Paoletti, S.; Bigazzi, R.; Aloisi, M.; Barsotti, G.; Rindi, P.; Donati, G.; Antonelli, A.; Panicucci, E.; et al. Chronic inflammation and mortality in haemodialysis, effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol. Dial. Transplant. 2008, 23, 2337–2343. [Google Scholar] [CrossRef] [PubMed]
- Siriopol, D.; Canaud, B.; Stuard, S.; Mircescu, G.; Nistor, I.; Covic, A. New insights into the effect of haemodiafiltration on mortality, the Romanian experience. Nephrol Dial. Transplant. 2015, 30, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macià, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A.; et al. High-efficiency postdilution online haemodiafiltration reduces all-cause mortality in haemodialysis patients. J. Am. Soc. Nephrol. 2013, 24, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Grooteman, M.P.; van den Dorpel, M.A.; Bots, M.L.; Penne, E.L.; van der Weerd, N.C.; Mazairac, A.H.; den Hoedt, C.H.; van der Tweel, I.; Lévesque, R.; Nubé, M.J.; et al. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J. Am. Soc. Nephrol. 2012, 23, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Nistor, I.; Palmer, S.C.; Craig, J.C.; Saglimbene, V.; Vecchio, M.; Covic, A.; Strippoli, G.F. Haemodiafiltration, haemofiltration and haemodialysis for end-stage kidney disease. Cochrane Database Syst. Rev. 2015, 5, CD006258. [Google Scholar]
- Lornoy, W.; Becaus, I.; Billiouw, J.M.; Sierens, L.; Van Malderen, P.; D’Haenens, P. On-line haemodiafiltration, Remarkable removal of beta2-microglobulin—Long-term clinical observations. Nephrol. Dial. Transplant. 2000, 15, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, J. Clearance of beta-2-microglobulin and middle molecules in haemodiafiltration. Contrib. Nephrol. 2007, 158, 201–209. [Google Scholar] [PubMed]
- Borrelli, S.; Minutolo, R.; de Nicola, L.; De Simone, E.; De Simone, W.; Zito, B.; Guastaferro, P.; Nigro, F.; Iulianiello, G.; Credentino, O.; et al. Effect of hemodiafiltration with endogenous reinfusion on overt idiopathic chronic inflammation in maintenance hemodialysis patients, a multicenter longitudinal study. Hemodial. Int. 2014, 18, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Winchester, J.F.; Salsberg, J.A.; Levin, N.W. Beta-2 microglobulin in ESRD, an in-depth review. Adv. Ren. Replace Ther. 2003, 10, 279–309. [Google Scholar] [CrossRef] [PubMed]
- Canaud, B. Effect of online hemodiafiltration on morbidity and mortality of chronic kidney disease patients. Contrib. Nephrol. 2007, 158, 216–224. [Google Scholar] [PubMed]
- Akizawa, T.; Koiwa, F. Clinical Expectation of Online Hemodiafiltration: A Japanese Perspective. Blood Purif. 2015, 40, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Masakane, I.; Esashi, S.; Igarashi, H. Biocompatibility of predilution on-line hemodiafiltration. Blood Purif. 2013, 35, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Rosansky, S.J.; Clark, W.F.; Eggers, P.; Glassock, R.J. Initiation of dialysis at higher GFRs: Is the apparent rising tide of early dialysis harmful or helpful? Kidney Int. 2009, 76, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Johnson, D.W.; Kesselhut, J.; IDEAL Study. A randomized, controlled trial of early versus late initiation of dialysis. N. Engl. J. Med. 2010, 363, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Nesrallah, G.E.; Mustafa, R.A.; Clark, W.F.; Bass, A.; Barnieh, L.; Hemmelgarn, B.R.; Klarenbach, S.; Quinn, R.R.; Hiremath, S.; Canadian Society of Nephrology. Canadian Society of Nephrology 2014 clinical practice guideline for timing the initiation of chronic dialysis. CMAJ 2014, 186, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Crews, D.C.; Scialla, J.J.; Boulware, L.E.; Navaneethan, S.D.; Nally, J.V., Jr.; Liu, X.; Arrigain, S.; Schold, J.D.; Ephraim, P.L.; DEcIDE Network Patient Outcomes in End Stage Renal Disease Study Investigators. Comparative effectiveness of early versus conventional timing of dialysis initiation in advanced CKD. Am. J. Kidney Dis. 2014, 63, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Streja, E.; Rhee, C.M.; Ravel, V.; Amin, A.N.; Cupisti, A.; Chen, J.; Mathew, A.T.; Kovesdy, C.P.; Mehrotra, R.; et al. Incremental Hemodialysis, Residual Kidney Function, and Mortality Risk in Incident Dialysis Patients: A Cohort Study. Am. J. Kidney Dis. 2016, 68, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.T.; Fishbane, S.; Obi, Y.; Kalantar-Zadeh, K. Preservation of residual kidney function in hemodialysis patients, reviving an old concept. Kidney Int. 2016, 90, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Borràs Sans, M.; Chacón Camacho, A.; Cerdá Vilaplana, C.; Usón Nuño, A.; Fernández, E. Incremental peritoneal dialysis, clinical outcomes and residual kidney function preservation. Nefrologia 2016, 36, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Golper, T.A. Incremental Hemodialysis: How I Do It. Semin. Dial. 2016, 29, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.; Obi, Y.; Rhee, C.M.; Chen, J.L.; Shah, G.; Lau, W.L.; Kovesdy, C.P.; Mehrotra, R.; Kalantar-Zadeh, K. Treatment frequency and mortality among incident hemodialysis patients in the United States comparing incremental with standard and more frequent dialysis. Kidney Int. 2016, 90, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Caria, S.; Cupisti, A.; Sau, G.; Bolasco, P. The incremental treatment of ESRD, a low-protein diet combined with weekly hemodialysis may be beneficial for selected patients. BMC Nephrol. 2014, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Bolasco, P.; Cupisti, A.; Locatelli, F.; Caria, S.; Kalantar-Zadeh, K. Dietary Management of Incremental Transition to Dialysis Therapy, Once-Weekly Hemodialysis Combined With Low-Protein Diet. J. Ren. Nutr. 2016, 26, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Eriguchi, R.; Ou, S.M.; Rhee, C.M.; Kalantar-Zadeh, K. What Is Known and Unknown about Twice-Weekly Hemodialysis. Blood Purif. 2015, 40, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A. Will incremental hemodialysis preserve residual function and improve patient survival? Semin. Dial. 2015, 28, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Unruh, M.; Zager, P.G.; Kovesdy, C.P.; Bargman, J.M.; Chen, J.; Sankarasubbaiyan, S.; Shah, G.; Golper, T.; Sherman, R.A.; et al. Twice-weekly and incremental hemodialysis treatment for initiation of kidney replacement therapy. Am. J. Kidney Dis. 2014, 64, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Casino, F.G. Let us give twice-weekly hemodialysis a chance, revisiting the taboo. Nephrol. Dial. Transplant. 2014, 29, 1618–1620. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A. Is Hemodialysis Patient Survival Dependent upon Small Solute Clearance (Kt/V)? If So How Can Kt/V be Adjusted to Prevent under Dialysis in Vulnerable Groups? Semin. Dial. 2017. [Google Scholar] [CrossRef] [PubMed]
- Jhamb, M.; McNulty, M.L.; Ingalsbe, G.; Childers, J.W.; Schell, J.; Conroy, M.B.; Forman, D.E.; Hergenroeder, A.; Dew, M.A. Knowledge, barriers and facilitators of exercise in dialysis patients, a qualitative study of patients, staff and neprologists. BMC Nephrol. 2016, 17, 192. [Google Scholar] [CrossRef] [PubMed]
- Martin-Alemañy, G.; Valdez-Ortiz, R.; Olvera-Soto, G.; Gomez-Guerrero, I.; Aguire-Esquivel, G.; Cantu-Quintanilla, G.; Lopez-Alvarenga, J.C.; Miranda-Alatriste, P.; Espinosa-Cuevas, A. The effects of resistance exercise and oral nutritional supplementation during hemodialysis on indicators of nutritional status and quality of life. Nephrol. Dial. Transplant. 2016, 31, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Magnard, J.; Deschamps, T.; Cornu, C.; Paris, A.; Hristea, D. Effects of a six-month intradialytic physical ACTIvity program and adequate NUTritional support on protein-energy wasting, physical functioning and quality of life in chronic hemodialysis patients, ACTINUT study protocol for a randomised controlled trial. BMC Nephrol. 2013, 14, 259. [Google Scholar] [CrossRef] [PubMed]
- Hristea, D.; Deschamps, T.; Paris, A.; Lefrançois, G.; Collet, V.; Savoiu, C.; Ozenne, S.; Coupel, S.; Testa, A.; Magnard, J. Combining intra-dialytic exercise and nutritional supplementation in malnourished older haemodialysis patients, Towards better quality of life and autonomy. Nephrology 2016, 21, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.N.; Daly, R.M.; Fraser, S.F.; Haines, T.; Barnard, R.; Ockerby, C.; Kent, B. The impact of an exercise physiologist coordinated resistance exercise program on the physical function of people receiving hemodialysis: A stepped wedge randomised control study. BMC Nephrol. 2013, 14, 204. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.N.; Fraser, S.; Barnard, R.; Haines, T.; Ockerby, C.; Street, M.; Wang, W.C.; Daly, R. Effects of an intradialytic resistance training programme on physical function: A prospective stepped-wedge randomized controlled trial. Nephrol. Dial. Transplant. 2016, 31, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.; Green, S.; Fiatarone Singh, M.; Barnard, R.; Cheema, B.S. Development, feasibility, and efficacy of a customized exercise device to deliver intradialytic resistance training in patients with end stage renal disease, Non-randomized controlled crossover trial. Hemodial. Int. 2016, 20, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Capitanini, A.; Lange, S.; D’Alessandro, C.; Salotti, E.; Tavolaro, A.; Baronti, M.E.; Giannese, D.; Cupisti, A. Dialysis exercise team, the way to sustain exercise programs in hemodialysis patients. Kidney Blood Press Res. 2014, 39, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; D’Alessandro, C.; Fumagalli, G.; Vigo, V.; Meola, M.; Cianchi, C.; Egidi, M.F. Nutrition and physical activity in CKD patients. Kidney Blood Press Res. 2014, 39, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Ikizler, T.A. New insights into the role of anabolic interventions in dialysis patients with protein energy wasting. Curr. Opin. Nephrol. Hypertens. 2009, 18, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, I.G.; Price, D.E.; Howlett, T.A.; Harris, K.P.; Feehally, J.; Walls, J. Erythropoietin and sexual dysfunction. Nephrol. Dial. Transplant. 1997, 12, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Collister, D.; Komenda, P.; Hiebert, B.; Gunasekara, R.; Xu, Y.; Eng, F.; Lerner, B.; Macdonald, K.; Rigatto, C.; Tangri, N. The Effect of Erythropoietin-Stimulating Agents on Health-Related Quality of Life in Anemia of Chronic Kidney Disease: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2016, 164, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Yan, W.; Li, J. An update for the controversies and hypotheses of regulating nonthyroidal illness syndrome in chronic kidney diseases. Clin. Exp. Nephrol. 2014, 18, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. Gonadal dysfunction in chronic kidney disease. Rev. Endocr. Metab. Disord. 2016. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Mulligan, K.; Schambelan, M. Anabolic effects of nandrolone decanoate in patients receiving dialysis: A randomized controlled trial. JAMA 1999, 281, 1275–1281. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Painter, P.L.; Sakkas, G.K.; Gordon, P.; Doyle, J.; Shubert, T. Effects of resistance exercise training and nandrolone decanoate on body composition and muscle function among patients who receive hemodialysis: A randomized, controlled trial. J. Am. Soc. Nephrol. 2006, 17, 2307–2314. [Google Scholar] [CrossRef] [PubMed]
- Supasyndh, O.; Satirapoj, B.; Aramwit, P.; Viroonudomphol, D.; Chaiprasert, A.; Thanachatwej, V.; Vanichakarn, S.; Kopple, J.D. Effect of oral anabolic steroid on muscle strength and muscle growth in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Carrero, J.J.; von Walden, F.; Ikizler, T.A.; Nader, G.A. Muscle wasting in end-stage renal disease promulgates premature death, established, emerging and potential novel treatment strategies. Nephrol. Dial. Transplant. 2016, 31, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Mehls, O.; Tönshoff, B.; Blum, W.F.; Heinrich, U.; Seidel, C. Growth hormone and insulin-like growth factor I in chronic renal failure—Pathophysiology and rationale for growth hormone treatment. Acta Paediatr. Scand. Suppl. 1990, 370, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Blake, P.G. Growth hormone and malnutrition in dialysis patients. Perit. Dial. Int. 1995, 15, 210–216. [Google Scholar] [PubMed]
- Ikizler, T.A.; Wingard, R.L.; Hakim, R.M. Interventions to treat malnutrition in dialysis patients, the role of the dose of dialysis, intradialytic parenteral nutrition, and growth hormone. Am. J. Kidney Dis. 1995, 26, 256–265. [Google Scholar] [CrossRef]
- Iglesias, P.; Díez, J.J.; Fernández-Reyes, M.J.; Aguilera, A.; Burgués, S.; Martínez-Ara, J.; Miguel, J.L.; Gómez-Pan, A.; Selgas, R. Recombinant human growth hormone therapy in malnourished dialysis patients: A randomized controlled study. Am. J. Kidney Dis. 1998, 32, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, F.; Filho, J.C.; Lindgren, B.F. Growth hormone treatment in hemodialysis patients—A randomized, double-blind, placebo-controlled study. Scand. J. Urol. Nephrol. 2004, 38, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Cheung, A.K.; Christiansen, J.S.; Djurhuus, C.B.; El Nahas, M.; Feldt-Rasmussen, B.; Lange, M.; Mitch, W.E.; Wanner, C.; Wiedemann, J.; et al. OPPORTUNITY: A randomized clinical trial of growth hormone on outcome in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Cheung, A.K.; Christiansen, J.S.; Djurhuus, C.B.; El Nahas, M.; Feldt-Rasmussen, B.; Mitch, W.E.; Wanner, C.; Göthberg, M.; Ikizler, T.A. OPPORTUNITY: A large-scale randomized clinical trial of growth hormone in hemodialysis patients. Nephrol. Dial. Transplant. 2011, 26, 4095–4103. [Google Scholar] [CrossRef] [PubMed]
- Garagarza, C.A.; Valente, A.T.; Oliveira, T.S.; Caetano, C.G. Effect of personalized nutritional counseling in maintenance hemodialysis patients. Hemodial. Int. 2015, 19, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lim, H.; Choue, R. A Better Diet Quality is Attributable to Adequate Energy Intake in Hemodialysis Patients. Clin. Nutr. Res. 2015, 4, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Karavetian, M.; de Vries, N.; Rizk, R.; Elzein, H. Dietary educational interventions for management of hyperphosphatemia in hemodialysis patients, a systematic review and meta-analysis. Nutr. Rev. 2014, 72, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Leo, A.; Viola, A.; Carlomagno, G.; Monteburini, T.; Cenerelli, S.; Santarelli, S.; Boggi, R.; Miggiano, G.; Vulpio, C.; et al. Dietary intake of macronutrients and fiber in Mediterranean patients on chronic hemodialysis. J. Nephrol. 2013, 26, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Khoueiry, G.; Waked, A.; Goldman, M.; El-Charabaty, E.; Dunne, E.; Smith, M.; Kleiner, M.; Lafferty, J.; Kalantar-Zadeh, K.; El-Sayegh, S. Dietary intake in hemodialysis patients does not reflect a heart healthy diet. J. Ren. Nutr. 2011, 21, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Bross, R.; Shapiro, B.B.; Morrison, G.; Kopple, J.D. Dietary energy requirements in relatively healthy maintenance hemodialysis patients estimated from long-term metabolic studies. Am. J. Clin. Nutr. 2016, 103, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Kato, A.; Ishida, J.; Endo, Y.; Takita, T.; Furuhashi, M.; Maruyama, Y.; Odamaki, M. Association of abdominal visceral adiposity and thigh sarcopenia with changes of arteriosclerosis in haemodialysis patients. Nephrol. Dial. Transplant. 2011, 26, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Honda, H.; Qureshi, A.R.; Axelsson, J.; Heimburger, O.; Suliman, M.E.; Barany, P.; Stenvinkel, P.; Lindholm, B. Obese sarcopenia in patients with end-stage renal disease is associated with inflammation and increased mortality. Am. J. Clin. Nutr. 2007, 86, 633–638. [Google Scholar] [PubMed]
- Kistler, B.M.; Fitschen, P.J.; Ikizler, T.A.; Wilund, K.R. Rethinking the restriction on nutrition during hemodialysis treatment. J. Ren. Nutr. 2015, 25, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Ikizler, T.A. Let them eat during dialysis, an overlooked opportunity to improve outcomes in maintenance hemodialysis patients. J. Ren. Nutr. 2013, 23, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Kistler, B.; Benner, D.; Burgess, M.; Stasios, M.; Kalantar-Zadeh, K.; Wilund, K.R. To eat or not to eat-international experiences with eating during hemodialysis treatment. J. Ren. Nutr. 2014, 24, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Karupaiah, T.; Sahathevan, S.; Sadu Singh, B.K.; Khor, B.H.; Salhab, N.; Karavetian, M.; Cupisti, A.; Fiaccadori, E. Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Beddhu, S.; Filipowicz, R.; Chen, X.; Neilson, J.L.; Wei, G.; Huang, Y.; Greene, T. Supervised oral protein supplementation during dialysis in patients with elevated C-reactive protein levels, a two phase, longitudinal, single center, open labeled study. BMC Nephrol. 2015, 16, 87. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Koyama, H.; Kondo, K.; Fujii, H.; Hirayama, Y.; Tabata, T.; Okamura, M.; Yamakawa, T.; Okada, S.; Hirata, S.; et al. Effects of nutritional supplementation on fatigue, and autonomic and immune dysfunction in patients with end-stage renal disease: A randomized, double-blind, placebo-controlled, multicenter trial. PLoS ONE 2015, 10, e0119578. [Google Scholar] [CrossRef] [PubMed]
- Tomayko, E.J.; Kistler, B.M.; Fitschen, P.J.; Wilund, K.R. Intradialytic protein supplementation reduces inflammation and improves physical function in maintenance hemodialysis patients. J. Ren. Nutr. 2015, 25, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Maduro, I.P.; Nonino, C.B.; Sakamoto, L.M.; Meirelles, M.G.; Cardeal Da Costa, J.A.; Marchini, J.S. Red meat snacks for chronic hemodialysis patients, effect on inflammatory activity (a pilot study). Ren. Fail. 2013, 35, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Siefker, K.; DiSilvestro, R.A. Safety and antioxidant effects of a modest soy protein intervention in hemodialysis patients. J. Med. Food 2006, 9, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Ferng, S.H.; Yang, C.S.; Peng, S.J.; Lee, H.R.; Chen, J.R. Variable effects of soy protein on plasma lipids in hyperlipidemic and normolipidemic hemodialysis patients. Am. J. Kidney Dis. 2005, 46, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Kapoian, T.; Johnson, D.S. Nutrition, vitamin D, and health outcomes in hemodialysis, time for a feeding frenzy? Curr. Opin. Nephrol. Hypertens. 2015, 24, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Pupim, L.B.; Majchrzak, K.M.; Flakoll, P.J.; Ikizler, T.A. Intradialytic oral nutrition improves protein homeostasis in chronic hemodialysis patients with deranged nutritional status. J. Am. Soc. Nephrol. 2006, 17, 3149–3157. [Google Scholar] [CrossRef] [PubMed]
- Lacson, E., Jr.; Wang, W.; Zebrowski, B.; Wingard, R.; Hakim, R.M. Outcomes associated with intradialytic oral nutritional supplements in patients undergoing maintenance hemodialysis: A quality improvement report. Am. J. Kidney Dis. 2012, 60, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Tighiouart, H.; Ladik, V.; Meyer, K.B.; Zager, P.G.; Johnson, D.S. Oral intradialytic nutritional supplement use and mortality in hemodialysis patients. Am. J. Kidney Dis. 2014, 63, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Dukkipati, R.; Kalantar-Zadeh, K.; Kopple, J.D. Is there a role for intradialytic parenteral nutrition? A review of the evidence. Am. J. Kidney Dis. 2010, 55, 352–364. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Li, Y.J.; Xu, R.; Ikizler, T.A.; Wang, H.Y. Ketoacid Supplementation Partially Improves Metabolic Parameters in Patients on Peritoneal Dialysis. Perit. Dial. Int. 2015, 35, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Serna-Thomé, M.G.; Padilla-Rosciano, A.E.; Suchil-Bernal, L. Practical aspects of intradialytic nutritional support. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Nongnuch, A.; Assanatham, M.; Panorchan, K.; Davenport, A. Strategies for preserving residual renal function in peritoneal dialysis patients. Clin. Kidney J. 2015, 8, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, M.K.; Levin, A.; Tejani, A.M. Systematic review of evidence for the use of intradialytic parenteral nutrition in malnourished hemodialysis patients. J. Ren. Nutr. 2010, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Marsen, T.A.; Beer, J.; Mann, H.; German IDPN-Trial Group. Intradialytic parenteral nutrition in maintenance hemodialysis patients suffering from protein-energy wasting. Results of a multicenter, open, prospective, randomized trial. Clin. Nutr. 2017, 36, 107–117. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period * | The Main “Enemy” | The Risks | Dietary Indications | Notes |
|---|---|---|---|---|
| First era | Potassium | Hyperkalemia can be deadly | Restrictions on fruit and vegetables | Can be mitigated by high dialysis efficiency and acidosis control |
| Second era | Phosphate | Vascular calcification, vascular ageing | Restrictions on cheese, milk and derivates | May contrast with the indications of high-protein intake |
| Third era | Malnutrition | Risk of death is higher in malnourished patients | Increased protein and calorie intake | May be impossible to conciliate with previous restrictions |
| The Questions | Pros | Cons | Comments |
|---|---|---|---|
| Are the nutritional requirements usually cited (calories: 30–35 kcal/kg; proteins > 1.2 g/kg) still relevant? | International standard followed for more than 40 years | The requirements were assessed in a different dialysis population, and may not be relevant to the present one; they do not consider the changes in the indications given to the overall population | There is a need for a re-assessment of the requirements of elderly dialysis patients |
| Are the present standards of “adequate nutrition” applicable to intensive dialysis schedules, and to haemodiafiltration? | Simple markers such as albumin level make it possible to compare results, and are robust enough to maintain a constant predictive value | Sensibility may be lower in non conventional dialysis techniques, and can be affected by albumin losses in haemodiafiltration | None of the proposed evaluations of malnutrition is clearly superior or self-standing; results of studies depend in part on the definition-diagnoses chosen |
| Processed and preserved food may be significantly different from untreated food. What are we eating? | Nutritional approaches have to be simple and basing them on quantity and quality may not be feasible | Processed foods may be rich in rapidly absorbable phosphate and potassium | Not acknowledging the importance of additives in processed and preserved foods can lead to unnecessary restrictions |
| Is malnutrition a single disease or the result of several diseases? | The clinical signs of malnutrition are universal and do not depend on pathogenesis | If malnutrition is not linked to poor intake but to poor clinical conditions, itwill not respond to therapy | Differentiation may allow setting attainable goals according to the individualpatient’s comorbidity |
| The paradoxes | The “logic” (overall population or general data in the dialysis population) | The finding (in the dialysis population or in specific dialysis populations) | Comments |
| Obesity and survival | Obesity is associated with lower survival in the overall population | Obesity is associated with higher survival in dialysis patients; losing weight is associated with higher mortality on dialysis | Obesity is often a contraindication for kidney transplantation |
| High protein intake and phosphate control | A high protein diet is indicated after dialysis start | Reduction of phosphate intake is not compatible with a high-protein diet | Plant derived phosphate may be less well absorbed; acidosis induced by catabolism is often a missing element in hyperphosphatemia |
| Albumin level, Kt/V and survival | Low serum albumin and low dialysis efficiency are associated with reduced survival | In haemodiafiltration, high efficiency is coupled with significant albumin losses | Albumin losses are incompletely quantified; nutrition is probably more important than high efficiency in elderly or fragile sarcopenic patients |
| Potassium and vascular health | Since dialysis patients are at risk for hyperkalemia, potassium is often restricted | Banning plant derived food to avoid hyperkalemia limits consumption of “vascular healthy” food in a high-risk population | Hyperkalemia is still a rare, but possible cause of death |
| The Field of Intervention | Intervention | Pros | Cons |
|---|---|---|---|
| Dialysis optimization | Increasing efficiency and tolerance by increasing frequency (daily or more frequent dialysis) [200,201,202,203,204,205,206,207,208,209,210,211,212,213] | Improvement in nutritional status in most of prospective studies (see also pregnancy on dialysis) | May be difficult to organize; possibly higher risk of vascular access problems |
| Increasing efficiency and probably also tolerance by switching to convective dialysis modalities (such as high flow haemodiafiltration) [214,215,216,217,218,219,220,221,222,223,224,225,226] | Efficiency is associated with nutritional status at least in “standard patients” | Losses may be significant in elderly, malnourished patients. No demonstration of nutritional advantages | |
| Decreasing losses, and preserving renal function (incremental dialysis, tailored dialysis) [227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242] | Residual diuresis and residual renal function are two of the most powerful predictors of survival; “dialysis shock” may be a cause of early death after dialysis start | Experience is still limited and there is still no agreed standard | |
| Physical exercise | Physical exercise is theoretically a powerful means of improving clinical conditions and nutritional status in patients with a chronic disease [243,244,245,246,247,248,249,250,251,252] | The best results have been reported in observational studies; biases linked to self-selection limit the generalization of results. | Barriers are evident in the elderly population, in which inactivity is often the result of the same comprehensive physical failure that causes malnutrition |
| Metabolic interventions * | Anemia correction [253,254] | ESA improved quality of life, fertility and sex life, issues associated with nutritional status | The association between lack of response to ESAs, inflammation, malnutrition and atherosclerosis is part of the MIA syndrome |
| Thyroid hormones [255] | The euthyroid sick syndrome or “low T3 syndrome” is typical of malnutrition/starvation | Correction of the metabolic deficit can worsen the clinical picture | |
| Androgen steroids [256,257,258,259] | Recently reconsidered therapeutic options include nandrolone decanoate and oxymetholone, which display good effects on sarcopenia | Side effects may be relevant; this treatment could be considered in males with testicular failure and severe sarcopenia | |
| Recombinant growth hormone [260,261,262,263,264,265,266,267] | Recombinant growth hormone is routinely used in children on dialysis. In adults, growth hormone is often low, and the effect on severe malnutrition has been favorable | High costs and side effects limit its use | |
| Nutritional interventions | Increasing the quantity/quality of food [268,269,270,271,272,273,274,275,276,277,278] | The best tool for improving nutritional status, eating during dialysis may be an important way to improve the nutritional status of dialysis patients | If malnutrition is linked to inflammation and atherosclerosis, it is difficult to increase the quantity or quality of food |
| Nutritional supplements (oral) [279,280,281,282,283,284,285,286,287,288,289,290,291,292] | Can be of use especially for limited periods of time; specific supplements for dialysis patients (poor in phosphate) are also available | Can decrease appetite for “normal” food; may be less tasty after a longer period | |
| Intravenous or enteral supplements [293,294,295] | Can help reverse acute malnutrition, especially in the case of failure of the two previous interventions | May further reduce food intake; and create a need for a high quantity of fluids; metabolic derangements are frequent in the long term |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccoli, G.B.; Moio, M.R.; Fois, A.; Sofronie, A.; Gendrot, L.; Cabiddu, G.; D’Alessandro, C.; Cupisti, A. The Diet and Haemodialysis Dyad: Three Eras, Four Open Questions and Four Paradoxes. A Narrative Review, Towards a Personalized, Patient-Centered Approach. Nutrients 2017, 9, 372. https://doi.org/10.3390/nu9040372
Piccoli GB, Moio MR, Fois A, Sofronie A, Gendrot L, Cabiddu G, D’Alessandro C, Cupisti A. The Diet and Haemodialysis Dyad: Three Eras, Four Open Questions and Four Paradoxes. A Narrative Review, Towards a Personalized, Patient-Centered Approach. Nutrients. 2017; 9(4):372. https://doi.org/10.3390/nu9040372
Chicago/Turabian StylePiccoli, Giorgina Barbara, Maria Rita Moio, Antioco Fois, Andreea Sofronie, Lurlinys Gendrot, Gianfranca Cabiddu, Claudia D’Alessandro, and Adamasco Cupisti. 2017. "The Diet and Haemodialysis Dyad: Three Eras, Four Open Questions and Four Paradoxes. A Narrative Review, Towards a Personalized, Patient-Centered Approach" Nutrients 9, no. 4: 372. https://doi.org/10.3390/nu9040372