Know Your Noodles! Assessing Variations in Sodium Content of Instant Noodles across Countries

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Categorisation
2.2. Data Analysis
3. Results
3.1. Labelling
3.2. Range and Levels of Sodium Per 100 g
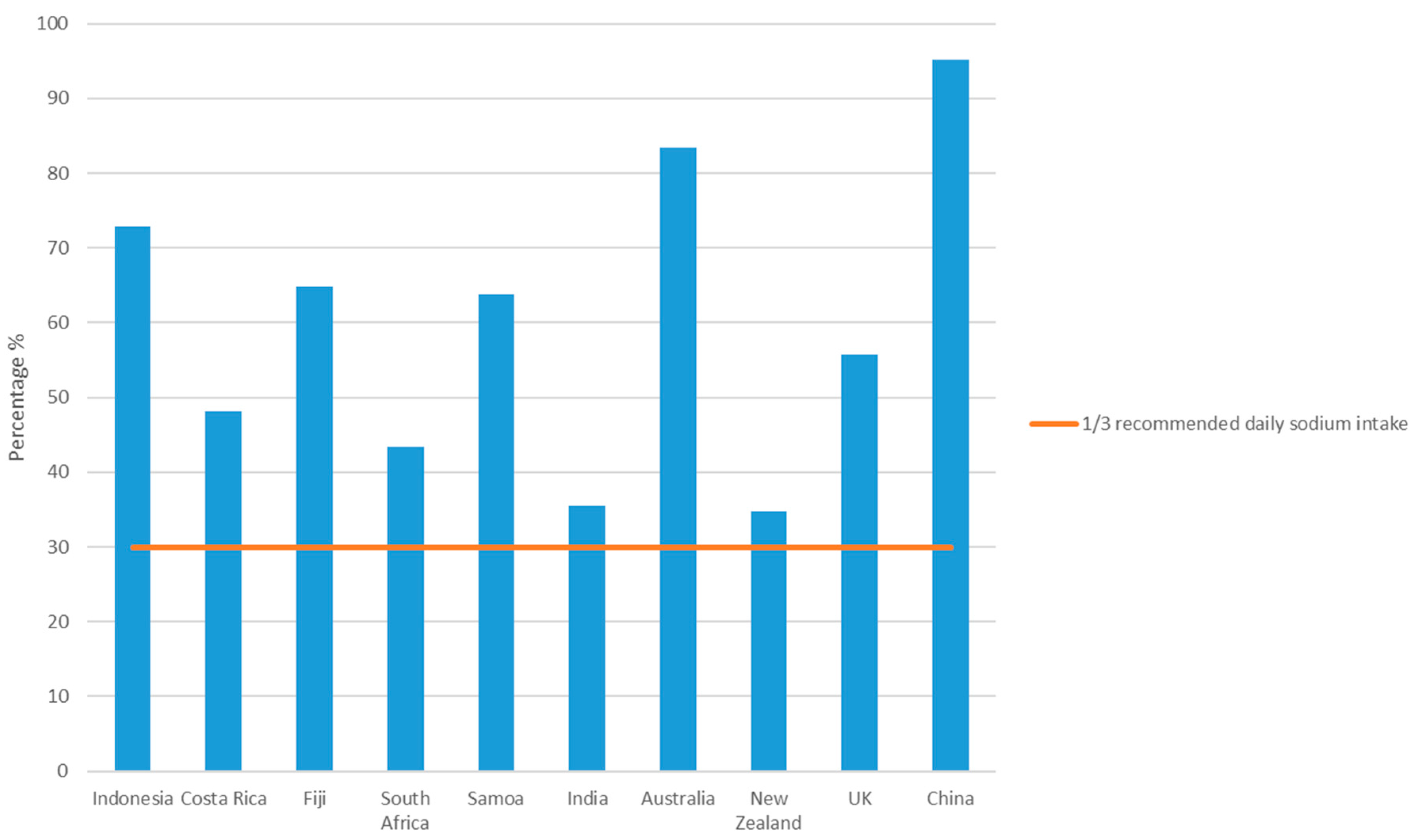
3.3. Percentage of Products which Meet Targets
3.4. Average Pack Size
3.5. Comparison of Sodium Levels in Instant Noodles between High-Income Countries and Middle-Income Countries
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Global Status Report on Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2014.
- Wang, G.; Labarthe, D. The cost-effectiveness of interventions designed to reduce sodium intake. J. Hypertens. 2011, 29, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013.
- He, F.J.; MacGregor, G.A. Reducing population salt intake worldwide: From evidence to implementation. Progr. Cardiovasc. Dis. 2010, 52, 363–382. [Google Scholar] [CrossRef] [PubMed]
- Jaenke, R.; Barzi, F.; McMahon, E.; Webster, J.; Brimblecombe, J. Consumer Acceptance of Reformulated Food Products: A Systematic Review and Meta-analysis of Salt-reduced Foods. Crit. Rev. Food Sci. Nutr. 2017, 57, 3357–3372. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.E.; Langford, K.; Kaldor, J. Innovative and Collaborative Strategies to Reduce Population-Wide Sodium Intake. Curr. Nutr. Rep. 2015, 4, 279–289. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14, 21–28. [Google Scholar] [CrossRef]
- Gulia, N.; Dhaka, V.; Khatkar, B.S. Instant Noodles: Processing, Quality, and Nutritional Aspects. Crit. Rev. Food Sci. Nutr. 2014, 54, 1386–1399. [Google Scholar] [CrossRef] [PubMed]
- World Instant Noodles Association. Global Report; World Instant Noodles Association: Tokyo, Japan, 2016. [Google Scholar]
- Kim, S.G. Instant noodles. In Pasta and Noodle Technology; Kruger, J.H., Matsuo, R.B., Dick, J.W., Eds.; American Association of Cereal Chemistry: St. Paul, MN, USA, 1996; pp. 195–225. [Google Scholar]
- Fu, B.X. Asian noodles: History, classification, raw materials and processing. Food Res. Int. 2008, 41, 888–902. [Google Scholar] [CrossRef]
- Park, J.; Lee, J.S.; Jang, Y.A.; Chung, H.R.; Kim, J. A comparison of food and nutrient intake between instant noodle consumers and non-instant noodle consumers in Korean adults. Nutr. Res. Prac. 2011, 5, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Cho, E.; Lee, H.J.; Fung, T.T.; Rimm, E.; Rosner, B.; Manson, J.E.; Wheelan, K.; Hu, F.B. Instant noodle intake and dietary patterns are associated with distinct cardiometabolic risk factors in Korea. J. Nutr. 2014, 144, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Trieu, K.; Dunford, E.; Hawkes, C. Target Salt 2025: A Global Overview of National Programs to Encourage the Food Industry to Reduce Salt in Foods. Nutrients 2014, 6, 3274–3287. [Google Scholar] [CrossRef] [PubMed]
- Public Health Responsibility Deal: UK Salt Reduction Targets for 2017; UK Department of Health: London, UK, 2014.
- Government Gazette: No. R. 214 Foodstuffs, Cosmetics and Disinfectants Act, 1972 (Act 54 of 1972) Regulations Relating to the Reduction of Sodium in Certain Foodstuffs and Related Matters The Heart and Stroke Foundation South Africa; South Africa Government: Pretoria, South Africa, 2013.
- Pacific Salt Reduction Targets: Why Setting Targets for Salt in Food? Western Pacific Region; World Health Organization: Geneva, Switzerland, 2014.
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Ni Mhurchu, C.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; et al. Maulik PK International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- CODEX Alimentarius: Standard for Instant Noodles CODEX STAN 249-2006; Food and Agriculture Organization of the United Nations and World Health Organization: Rome, Italy, 2016.
- The World Bank. World Bank List of economies (December 2016). Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 5 June 2017).
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Charlton, K.E.; Webster, J.; Kowai, P. To Legislate or Not to Legislate? A Comparison of the UK and South African Approaches to the Development and Implementation of the Salt Reduction Programs Nutrients. Nutrients 2014, 6, 3672. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871S–873S. [Google Scholar] [PubMed]
- CODEX Alimentarius: Guidelines on Nutrition Labelling; Food and Agriculture Organization of the United Nations and World Health Organization: Rome, Italy, 2011.
- Food Safety and Standards (Packaging and Labelling) Regulations; Food Safety and Standards Authority of India (FSSAI): New Delhi, India, 2011.
- Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold Through Retail Outlets. In Obesity and Healthy Eating Divison; Department of Health: London, UK, 2013.
- Kim, S.K. Overview of the Korean noodle industry. Food Sci. Biotechnol. 1997, 6, 125–130. [Google Scholar]
- Spohrer, R.; Larson, M.; Maurin, C.; Laillou, A.; Capanzana, M.; Garrett, G.S. The growing importance of staple foods and condiments used as ingredients in the food industry and implications for large-scale food fortification programs in Southeast Asia. Food Nutr. Bull. 2013, 34, S50–S61. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Date of Data Collection | Data Source | Country | Total No. of Products Collected | Products with Sodium Data | Products with Sodium Data “as Sold” | Products with Sodium Data “as Prepared” | Average Pack Size (g) | Average Serving Size (g) as Prepared | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||||||
| 2016 | FCD | UK | 137 | 132 | 96 | 11 | 8 | 121 | 92 | 84 | 282 |
| 2015 | FCD | New Zealand | 85 | 83 | 98 | 42 | 51 | 41 | 49 | 87 | 343 |
| 2014 | FCD | Australia | 58 | 58 | 100 | 9 | 16 | 49 | 84 | 86 | 308 |
| 2015 | FCD | China | 283 | 283 | 100 | 283 | 100 | 0 | 0 | 98 | - |
| 2012 | FCD | India | 47 | 15 | 32 | 15 | 100 | 0 | 0 | - | - |
| 2013 | Shop survey | Samoa | 44 | 43 | 98 | 28 | 65 | 15 | 35 | 69 | - |
| 2015 | FCD | South Africa | 37 | 37 | 100 | 28 | 76 | 9 | 24 | 72 | 300 |
| 2013 | Shop survey | Fiji | 28 | 28 | 100 | 23 | 82 | 5 | 18 | 69 | 143 |
| 2015 | Shop survey | Indonesia | 28 | 28 | 100 | 28 | 100 | 0 | 0 | 76 | - |
| 2013 | FCD | Costa Rica | 18 | 18 | 100 | 18 | 100 | 0 | 0 | 57 | - |
| Totals | 765 | 725 * | 95 | 485 | 67 | 240 | 33 | 78 | 275 | ||
| Country (World Bank Group) | Products with Sodium Data “as Sold” | Products with Sodium Data “as Prepared” | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean Sodium (mg/100 g) as Sold | Range of Sodium (mg/100 g) as Sold | Median Sodium and IQR (mg/100 g) as Sold | Products Known to Meet Pacific Salt Reduction Target (1600 mg/100 g as Sold) | Products Known to Meet South Africa 2016 Target (1500 mg/100 g as Sold) | n | Mean Sodium (mg/100 g) as Prepared | Range (mg/100 g) as Prepared | Median Sodium and IQR (mg/100 g) as Prepared | Products Known to Meet UK 2017 Max Sodium Target (350 mg/100 g as Consumed) | ||||
| n | % | n | % | n | % | |||||||||
| New Zealand (HIC) | 42 | 798 | 249–2380 | 508 (429) | 35 | 83 | 35 | 83 | 41 | 388 | 222–725 | 360 (106) | 19 | 46 |
| UK (HIC) | 11 | 1323 | 488–2650 | 948 (1620) | 6 | 55 | 6 | 55 | 121 | 220 | 120–440 | 200 (100) | 109 | 90 |
| Australia (HIC) | 9 | 1939 | 950–3050 | 2110 (951) | 3 | 33 | 3 | 33 | 49 | 378 | 205–635 | 350 (181) | 25 | 51 |
| China (MIC) | 283 | 1944 | 397–3678 | 2062 (757) | 74 | 26 | 67 | 24 | 0 | - | - | - | - | - |
| Samoa (MIC) | 28 | 1854 | 970–3360 | 1751 (610) | 11 | 39 | 6 | 21 | 15 | 334 | 245–590 | 280 (75) | 12 | 80 |
| Indonesia (MIC) | 28 | 1916 | 770–7584 | 1388 (1025) | 15 | 54 | 15 | 54 | 0 | - | - | - | - | - |
| South Africa (MIC) | 28 | 1206 | 350–1640 | 1314 (202) | 27 | 96 | 24 | 86 | 9 | 331 | 266–475 | 290 (90) | 5 | 56 |
| Fiji (MIC) | 23 | 1892 | 845–3510 | 1913 (767) | 6 | 26 | 6 | 26 | 5 | 317 | 200–443 | 300 (184) | 3 | 60 |
| Costa Rica (MIC) | 18 | 1703 | 1148–2278 | 1766 (242) | 4 | 22 | 4 | 22 | 0 | - | - | - | - | - |
| India (MIC) | 15 | 910 | 280–1932 | 590 (1067) | 12 | 80 | 12 | 80 | 0 | - | - | - | - | - |
| HICs sub-total | 62 | 1057 | 249–3050 | 605 (1280) * | 44 | 71 * | 44 | 71 * | 211 | 289 | 120–725 | 270 (180) | 153 | 73 |
| MICs subtotal | 423 | 1838 | 280–7584 | 1889 (926) | 149 | 35 | 134 | 32 | 29 | 330 | 200–590 | 290 (98) | 20 | 69 |
| Totals | 485 | 1738 | 249–7584 | 1823 (1029) | 193 | 40 | 178 | 37 | 240 | 294 | 120–725 | 273 (160) | 173 | 72 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farrand, C.; Charlton, K.; Crino, M.; Santos, J.; Rodriguez-Fernandez, R.; Ni Mhurchu, C.; Webster, J. Know Your Noodles! Assessing Variations in Sodium Content of Instant Noodles across Countries. Nutrients 2017, 9, 612. https://doi.org/10.3390/nu9060612
Farrand C, Charlton K, Crino M, Santos J, Rodriguez-Fernandez R, Ni Mhurchu C, Webster J. Know Your Noodles! Assessing Variations in Sodium Content of Instant Noodles across Countries. Nutrients. 2017; 9(6):612. https://doi.org/10.3390/nu9060612
Chicago/Turabian StyleFarrand, Clare, Karen Charlton, Michelle Crino, Joseph Santos, Rodrigo Rodriguez-Fernandez, Cliona Ni Mhurchu, and Jacqui Webster. 2017. "Know Your Noodles! Assessing Variations in Sodium Content of Instant Noodles across Countries" Nutrients 9, no. 6: 612. https://doi.org/10.3390/nu9060612