Increases in Alcohol Intakes Are Concurrent with Higher Energy Intakes: Trends in Alcohol Consumption in Australian National Surveys from 1983, 1995 and 2012


Abstract
:1. Introduction
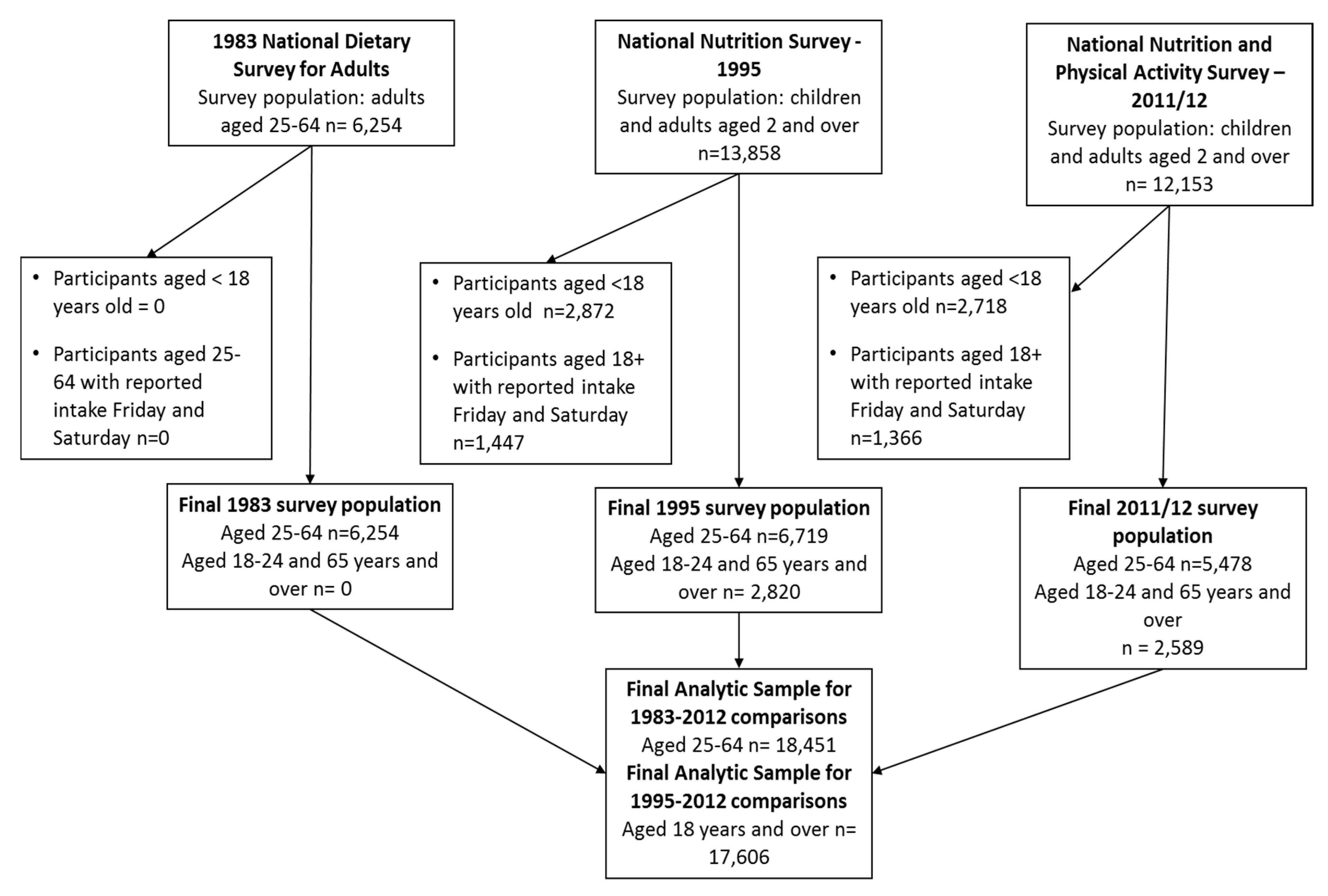
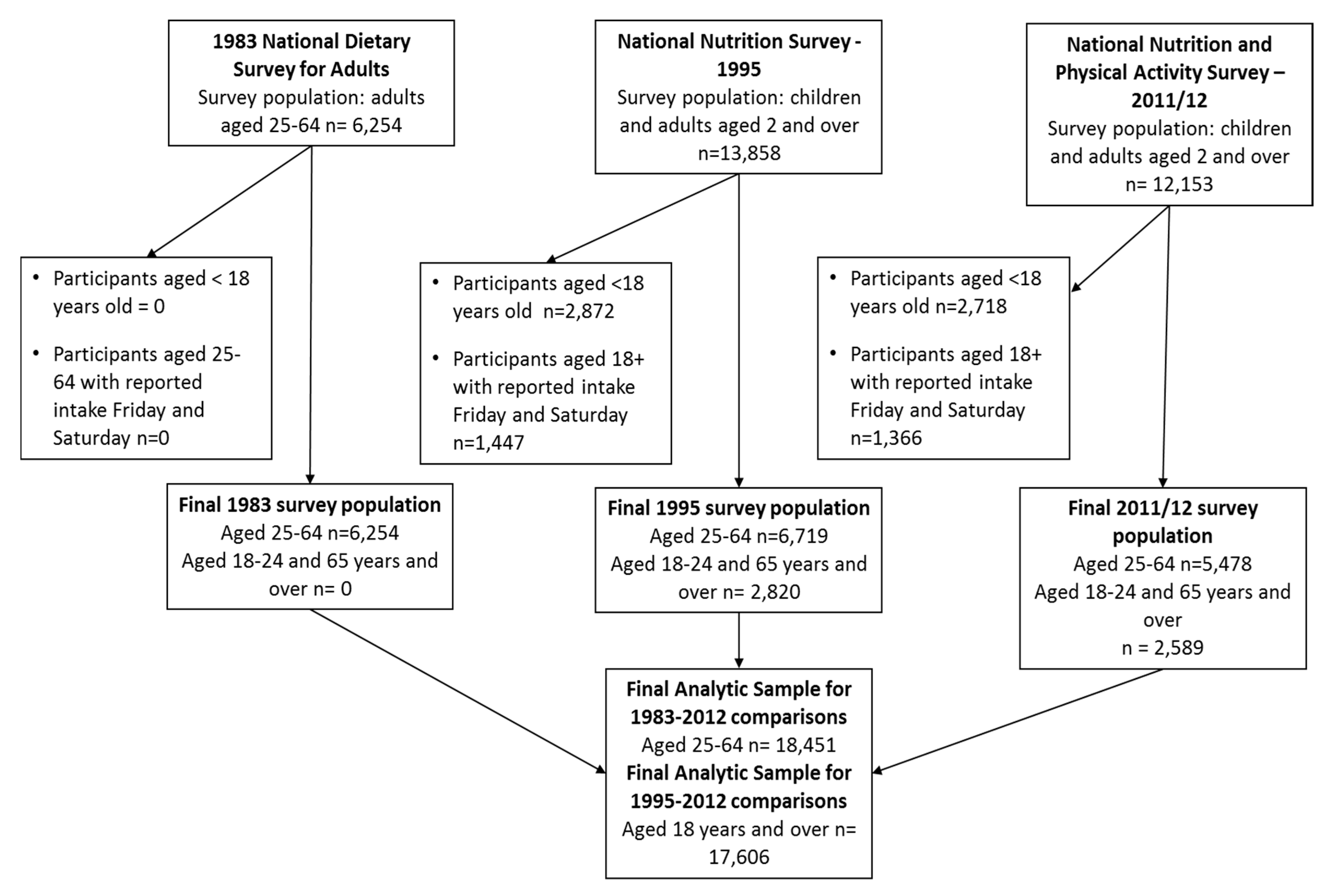
2. Materials and Methods
2.1. Dietary Assessment
2.2. Sensitivity Analysis
2.3. Low Energy Reporting
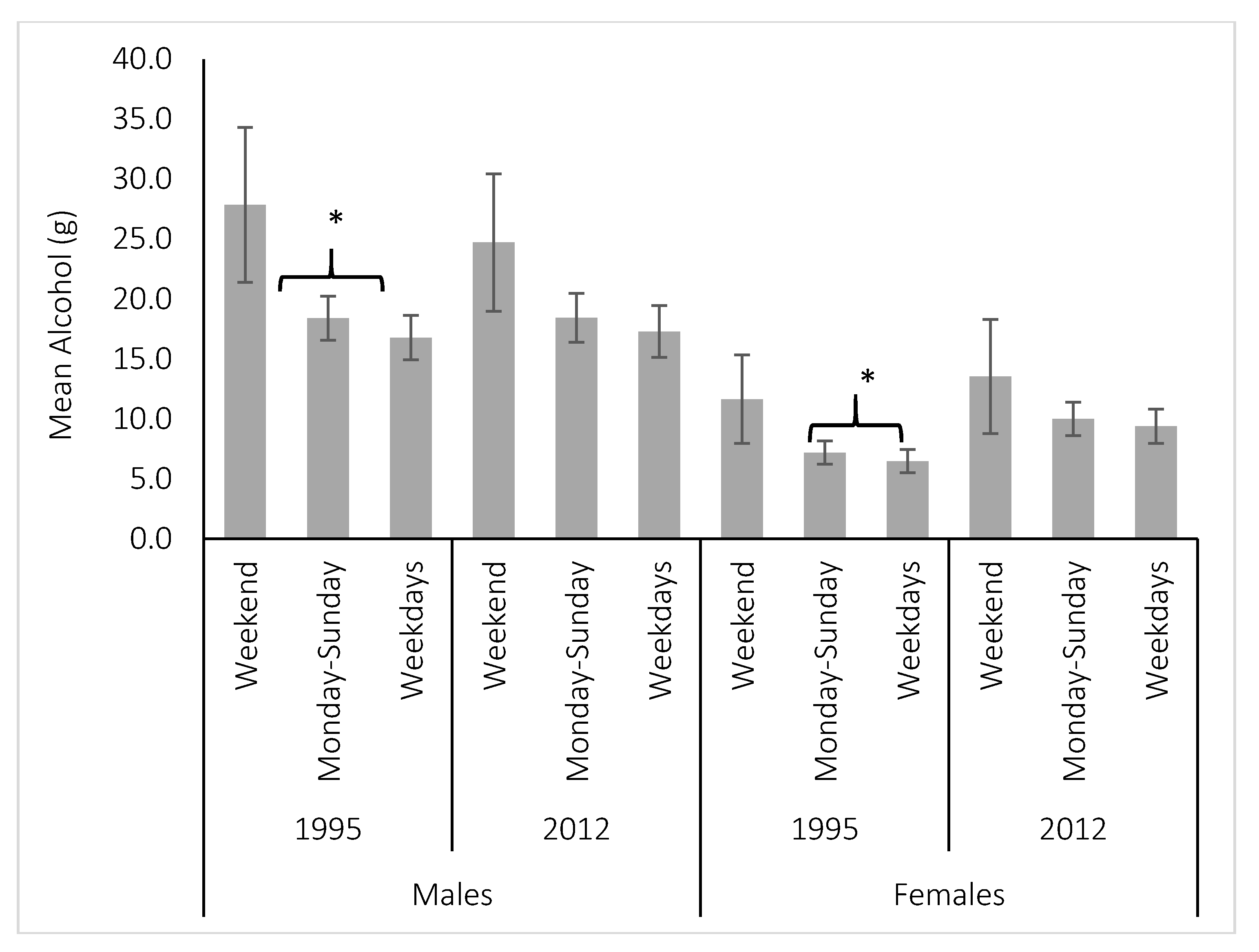
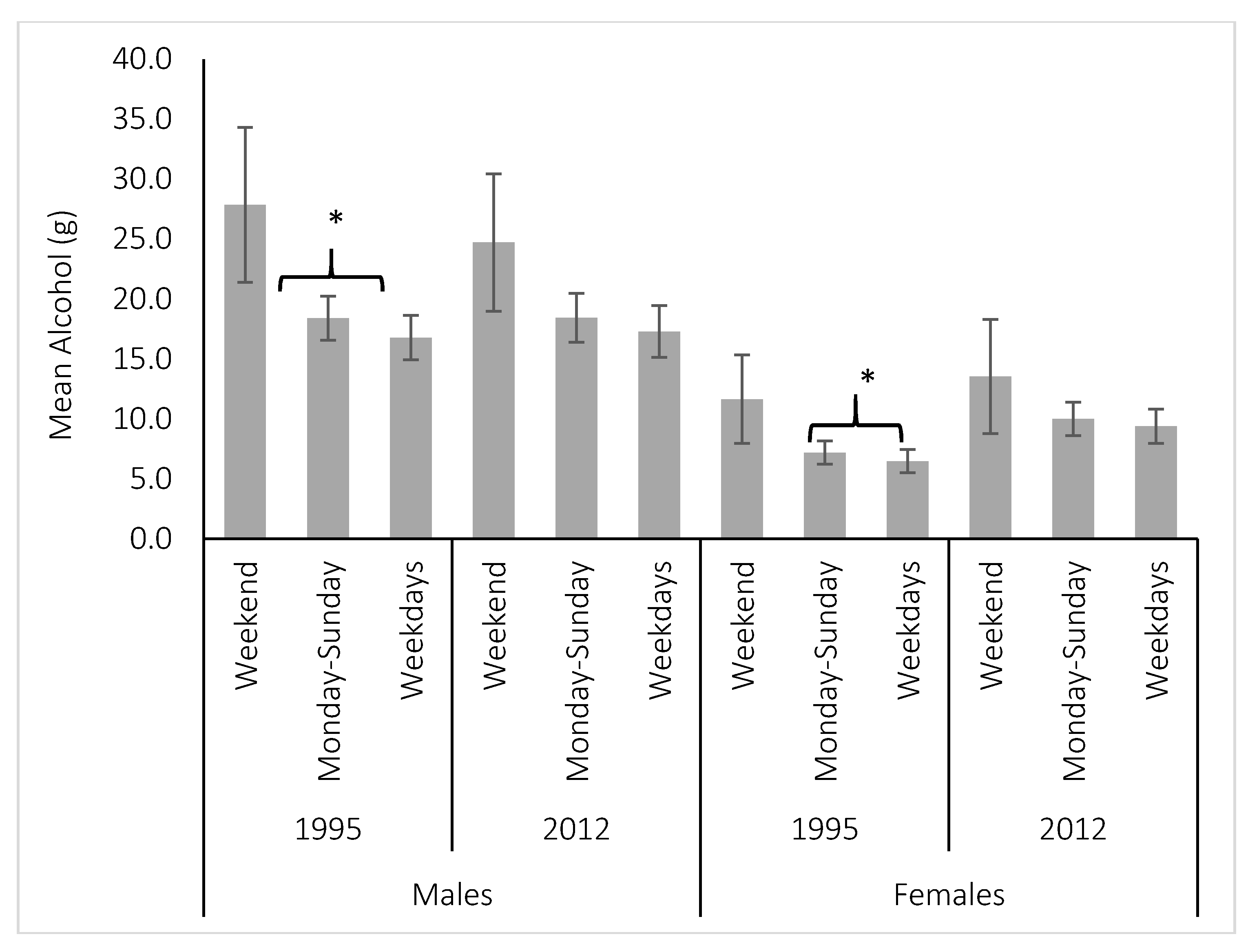
2.4. Period Trends
2.5. Statistical Analysis
3. Results
3.1. Sensitivity Analysis
3.2. Proportion Consuming
3.3. Per Capita Intake
3.4. Per-Consumer Intake
3.5. Types of Alcoholic Beverages Consumed
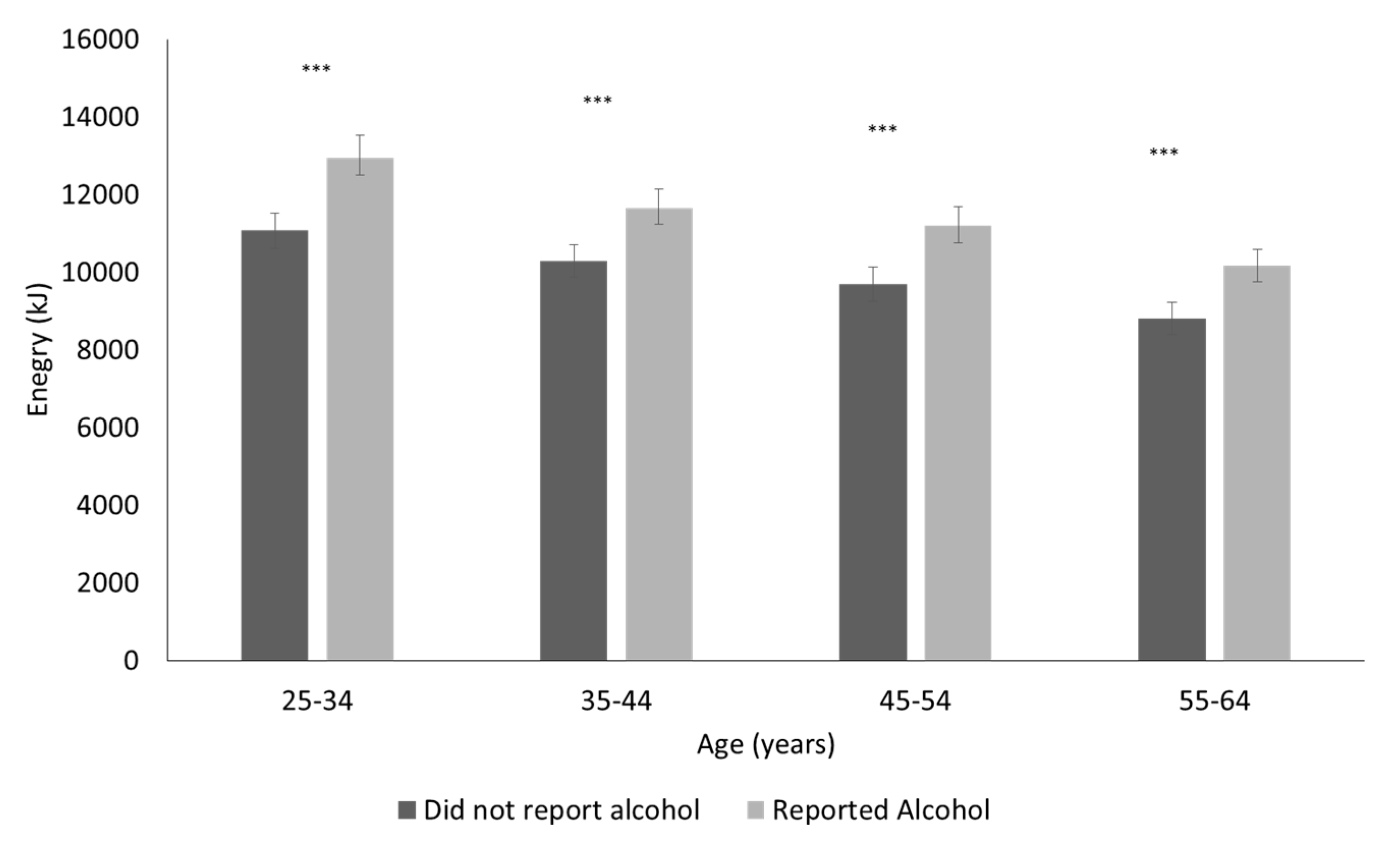
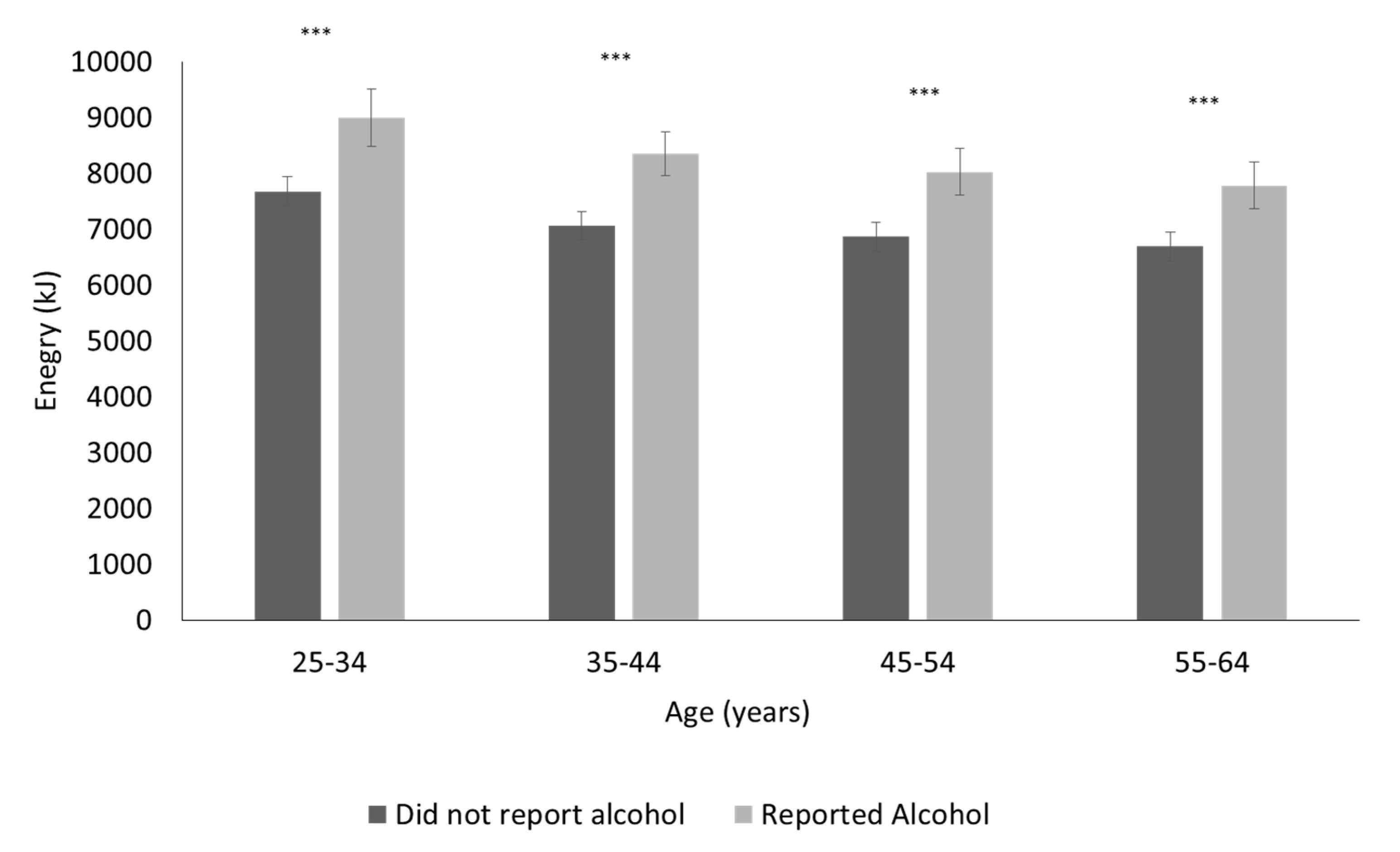
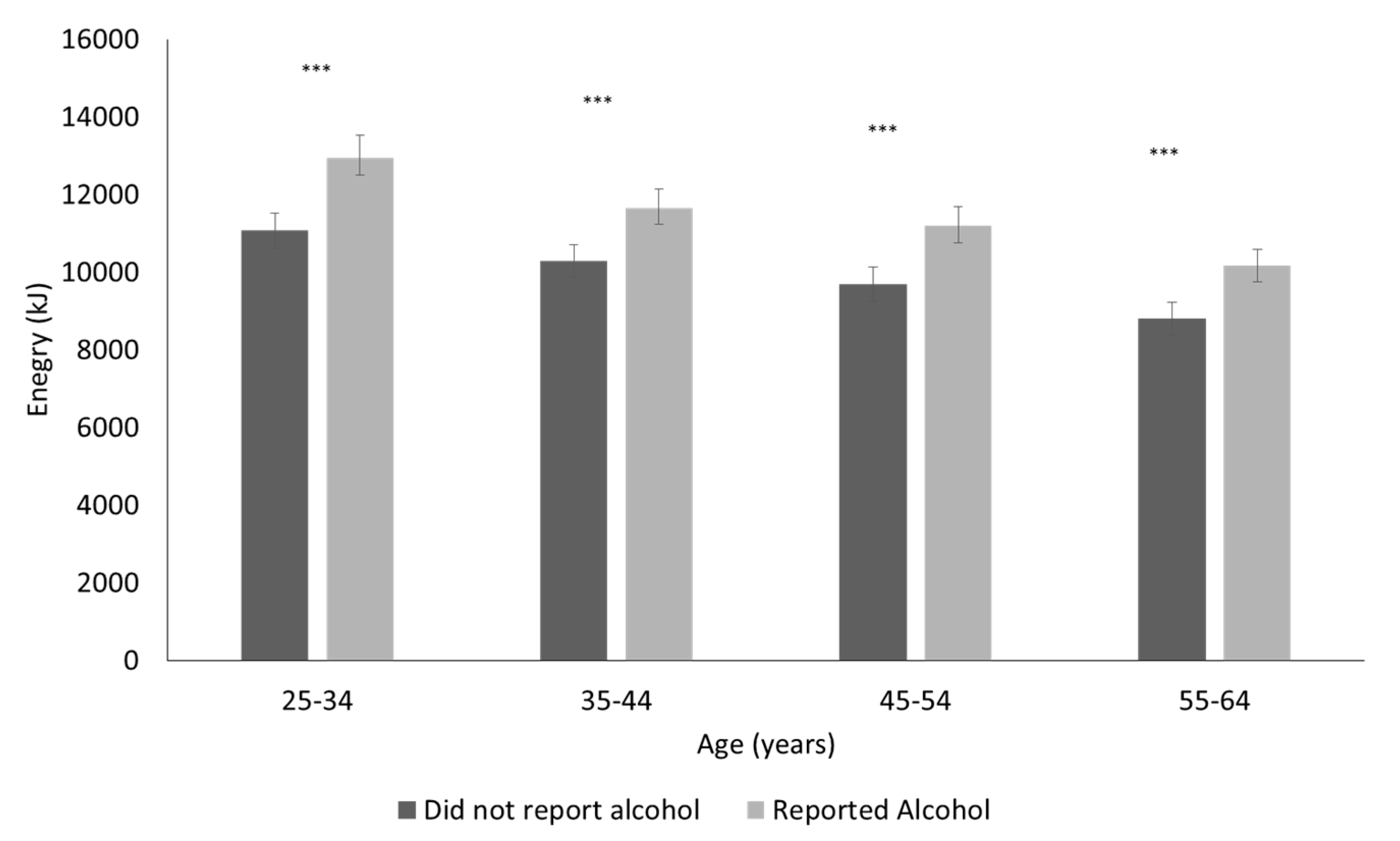
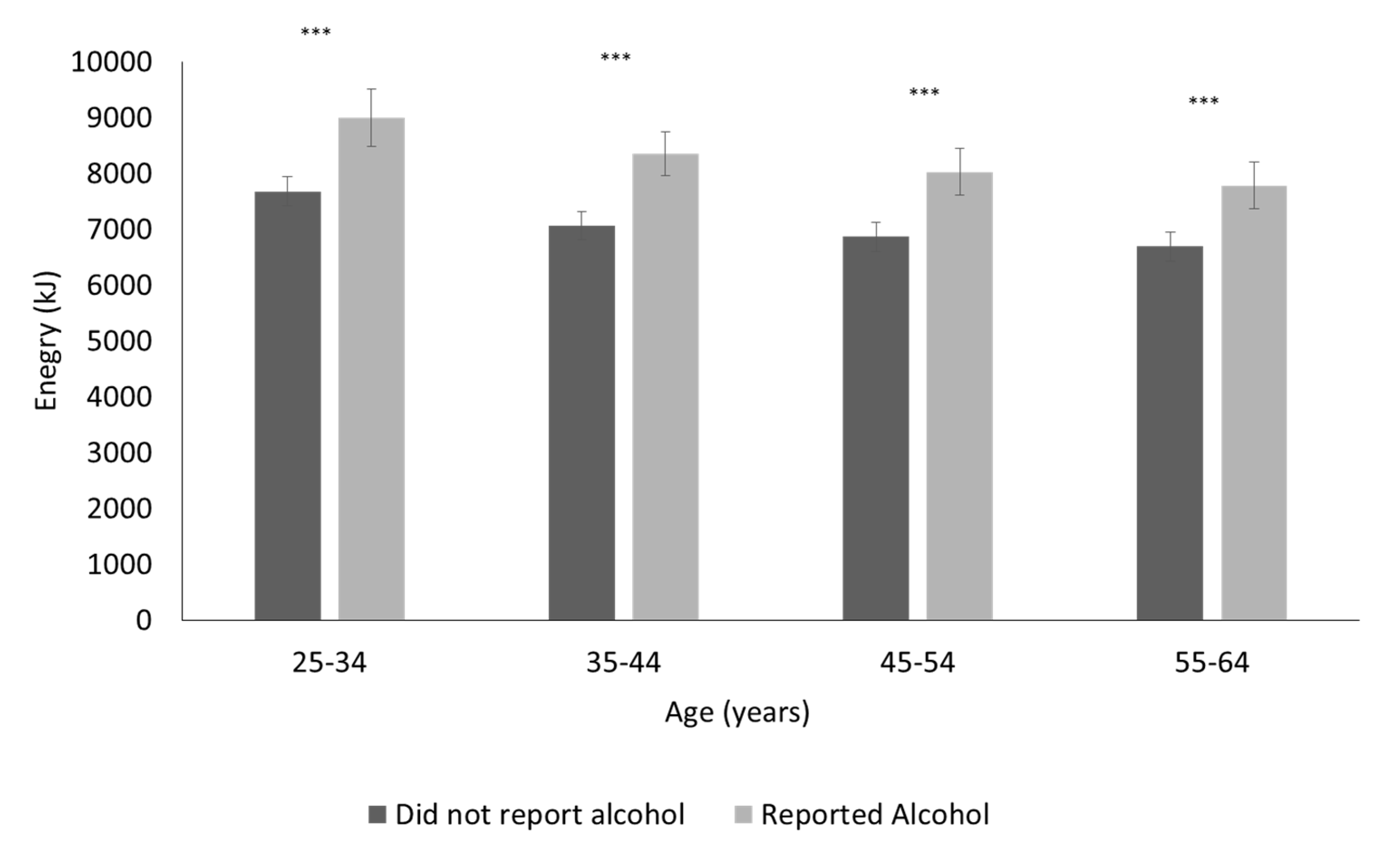
3.6. Energy Intakes of Alcohol Consumers
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Fox, K.; Marsh, P. Social and Cultural Aspects of Drinking: A Report to the Amsterdam Group; Social Issues Research Centre: Oxford, UK, 1998. [Google Scholar]
- Rehm, J.; Mathers, C.; Popova, S.; Thavorncharoensap, M.; Teerawattananon, Y.; Patra, J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009, 373, 2223–2233. [Google Scholar] [CrossRef]
- World Health Organization. WHO Expert Committee on Problems Related to Alcohol Consumption; Second Report; World Health Organization (WHO): Geneva, Switzerland, 2007; p. 1. [Google Scholar]
- World Health Organization. Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation; Food Agriculture Organization United Nations: Rome, Italy, 2004. [Google Scholar]
- Suter, P.M.; Tremblay, A. Is alcohol consumption a risk factor for weight gain and obesity? Crit. Rev. Clin. Lab. Sci. 2005, 42, 197–227. [Google Scholar] [CrossRef]
- Yeomans, M.R. Alcohol, appetite and energy balance: Is alcohol intake a risk factor for obesity? Physiol. Behav. 2010, 100, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.A. Body-weight regulation: Causes of obesity. Proc. Nutr. Soc. 2000, 59, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Traversy, G.; Chaput, J.P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 2015, 4, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, M.R.; Caton, S.; Hetherington, M.M. Alcohol and food intake. Curr. Opin. Clin. Nutr. Metab. Care 2003, 6, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Alcohol consumption and body weight: A systematic review. Nutr. Rev. 2011, 69, 419–431. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Dietary Guidelines for Australian Adults; National Health and Medical Research Council (NHMRC): Canberra, Australia, 2003.
- National Health and Medical Research Council. Alcohol Guidelines: Reducing the Health Risks; National Health and Medical Research Council (NHMRC): Canberra, Australia, 2009.
- Butler, L.; Poti, J.M.; Popkin, B.M. Trends in energy intake from alcoholic beverages among us adults by sociodemographic characteristics, 1989–2012. J. Acad. Nutr. Diet. 2016, 116, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Wymond, B.; Dickinson, K.; Riley, M. Alcoholic beverage intake throughout the week and contribution to dietary energy intake in Australian adults. Public Health Nutr. 2016, 19, 2592–2602. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. National Statement on Ethical Conduct in Human Research, 2007 (National Statement); National Health and Medical Research Council: Canberra, Australia, 2015.
- Australian Bureau of Statistics. National Nutrition Survey Users’ Guide, Australia 1995; Australian Bureau of Statistics (ABS): Canberra, Australia, 1996.
- Cook, P.; Coles-Rutishauser, I.; Allsopp, R. The Bridging Study-Comparing Results from the 1983, 1985 and 1995 Australian National Nutrition Surveys; Health and Aged Care: Canberra, Australia, 2001.
- Australian Bureau of Statistics. Australian Health Survey: Users’ Guide 2011–2012; Australian Bureau of Statistics (ABS): Canberra, Australia, 2013.
- National Heart Foundation. National Dietary Survey of Adults, Australia, 1983; Australian Data Archive, The Australian National University: Canberra, Australia, 1983. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4307.0.55.001—Apparent Consumption of Alcohol, Australia, 2013–2014; Australian Bureau of Statistics: Canberra, Australia, 2015.
- World Health Organization. Global Status Report on Alcohol and Health, 2014; World Health Organization (WHO): Geneva, Switzerland, 2014. [Google Scholar]
- Devaux, M.; Sassi, F. Alcohol Consumption and Harmful Drinking: Trends and Social Disparities across Oecd Countries; OECD: Paris, France, 2015. [Google Scholar]
- Australian Bureau of Statistics. 4364.0.55.008—Australian Health Survey: Usual Nutrient Intakes; Australian Bureau of Statistics: Canberra, Australia, 2015.
- Australian Bureau of Statistics. Australian Health Survey: First Results, 2011–12; Australian Bureau of Statistics: Canberra, Australia, 2012.
- NHS Digital. Statistics on Alcohol, England, 2017; NHS Digital: Leeds, UK, 2017. [Google Scholar]
- Livingston, M.; Raninen, J.; Slade, T.; Swift, W.; Lloyd, B.; Dietze, P. Understanding trends in Australian alcohol consumption-an age-period-cohort model. Addiction 2016, 111, 1590–1598. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Holmes, J.; Hill-McManus, D.; Brennan, A.; Meier, P.S. Trend analysis and modelling of gender-specific age, period and birth cohort effects on alcohol abstention and consumption level for drinkers in great britain using the general lifestyle survey 1984–2009. Addiction 2014, 109, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Kraus, L.; Tinghog, M.E.; Lindell, A.; Pabst, A.; Piontek, D.; Room, R. Age, period and cohort effects on time trends in alcohol consumption in the swedish adult population 1979–2011. Alcohol Alcohol. 2015, 50, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Alati, R.; Betts, K.S.; Williams, G.M.; Najman, J.M.; Hall, W.D. Generational increase in young women’s drinking: A prospective analysis of mother-daughter dyads. JAMA Psychiatry 2014, 71, 952–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Withnall, J.; Hill, S.B.; Bourgeois, S. Alcohol, women and midlife. Subst. Natl. Mag. Alcohol Tob. Other Drugs 2009, 7, 14–15. [Google Scholar]
- Slade, T.; Chapman, C.; Swift, W.; Keyes, K.; Tonks, Z.; Teesson, M. Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open 2016, 6, e011827. [Google Scholar] [CrossRef] [PubMed]
- Lyons, A.C.; Willott, S.A. Alcohol consumption, gender identities and women’s changing social positions. Sex Roles 2008, 59, 694–712. [Google Scholar] [CrossRef]
- Hayes, A.J.; Lung, T.W.C.; Bauman, A.; Howard, K. Modelling obesity trends in Australia: Unravelling the past and predicting the future. Int. J. Obes. 2016, 41, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 2071.0—Reflecting a Nation: Stories from the 2011 Census, 2012–2013; Australian Bureau of Statistics: Canberra, Australia, 2012.
- Livingston, M. Understanding Recent Trends in Australian Alcohol Consumption; Foundation for Alcohol Research and Education: Canberra, Australia, 2015. [Google Scholar]
- Sim, F. Alcoholic drinks contribute to obesity and should come with mandatory calorie counts. BMJ Br. Med. J. 2015, 350, h2407. [Google Scholar] [CrossRef] [PubMed]
- Kerr, W.C.; Greenfield, T.K.; Tujague, J.; Brown, S.E. The alcohol content of wine consumed in the us and per capita consumption: New estimates reveal different trends. Alcohol. Clin. Exp. Res. 2006, 30, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Chikritzhs, T.N.; Allsop, S.J.; Moodie, A.R.; Hall, W.D. Per capita alcohol consumption in Australia: Will the real trend please step forward. Med. J. Aust. 2010, 193, 594–597. [Google Scholar] [PubMed]
- Marteau, T.M.; Hollands, G.J.; Shemilt, I.; Jebb, S.A. Downsizing: Policy options to reduce portion sizes to help tackle obesity. BMJ 2015, 351. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Lewis, H.B.; Wei, Y.; Higgins, J.; Ogilvie, D. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Libr. 2015. [Google Scholar] [CrossRef]
- Callinan, S. How big is a self-poured glass of wine for Australian drinkers? Drug Alcohol Rev. 2015, 34, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.D.; Chan, G. Commentary on ogeil et al. (2016): Explaining increased alcohol-related harm and stable per capita consumption in Australia. Addiction 2016, 111, 635–636. [Google Scholar] [CrossRef] [PubMed]
- Giesbrecht, N.; Wettlaufer, A.; Cukier, S.; Geddie, G.; Gonçalves, A.-H.; Reisdorfer, E. Do alcohol pricing and availability policies have differential effects on sub-populations? A commentary. Int. J. Alcohol Drug Res. 2016, 5, 89–99. [Google Scholar] [CrossRef]
- Jones, S.C.; Gordon, R. Regulation of alcohol advertising: Policy options for Australia. Evid. Base 2013, 2013, 1–37. [Google Scholar]
- Martin-Moreno, J.M.; Harris, M.E.; Breda, J.; Moller, L.; Alfonso-Sanchez, J.L.; Gorgojo, L. Enhanced labelling on alcoholic drinks: Reviewing the evidence to guide alcohol policy. Eur. J. Public Health 2013, 23, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Guenther, P.M.; Dodd, K.W.; Krebs-Smith, S.M.; Midthune, D. The population distribution of ratios of usual intakes of dietary components that are consumed every day can be estimated from repeated 24-h recalls. J. Nutr. 2010, 140, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.; Callinan, S. Underreporting in alcohol surveys: Whose drinking is underestimated? J. Stud. Alcohol Drugs 2015, 76, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Stockwell, T.; Thomas, G. An adaptation of the yesterday method to correct for under-reporting of alcohol consumption and estimate compliance with Canadian low-risk drinking guidelines. Can. J. Public Health 2015, 106, e204–e209. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Size (n) | Proportion Reporting Alcohol (95% CI) | Mean Alcohol (g) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Demographic | 1995 | 2011/12 | 1995 | 2011/12 | 1995 | 2011/12 | ||
| Men | Age | ||||||||
| 18–24 | 550 | 373 | 30.5 | (25.1–32.7) | 24.1 | (19.8–28.5) | 14.9 | 10.4 | |
| 25–34 | 1084 | 747 | 42.1 | (39.3–45.2) | 37.9 | (34.1–41.0) | 19.8 | 17.1 | |
| 35–44 | 1056 | 846 | 43.9 | (40.6–46.6) | 38.7 | (36.1–42.7) | 19.6 | 18.3 | |
| 45–54 | 882 | 781 | 49.8 | (45.7–52.2) | 46.3 | (41.2–48.2) | 19.7 | 23.4 | |
| 55–64 | 672 | 672 | 48.9 | (45.6–53.2) | 45.4 | (42.1–49.6) | 20.9 | 22.7 | |
| 65+ | 902 | 910 | 43.1 | (39.8–46.4) | 44.0 | (40.7–47.2) | 14.7 | 17.4 | |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||
| Day of the Week | |||||||||
| Sunday–Thursday | 4436 | 3660 | 42.0 | (40.3–43.2) | 39.2 | (37.6–40.7) | 16.8 | 17.3 | |
| Friday–Saturday | 710 | 669 | 53.9 | (45.2–52.8) | 49.0 | (45.2–52.8) | 27.8 | 24.7 | |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||
| Season | |||||||||
| December–April | 2058 | 2208 | 45.0 | (42.6–46.9) | 41.3 | (39.1–34.4) | 19.1 | 18.1 | |
| May–November | 3088 | 2301 | 42.8 | (40.7–44.2) | 40.2 | (38.1–42.2) | 18.0 | 18.6 | |
| p | p = 0.11 | p = 0.46 | p = 0.27 | p = 0.65 | |||||
| Geographic Area | |||||||||
| Metropolitan | 2626 | 2833 | 42.9 | (40.7–44.5) | 39.7 | (37.9–41.5) | 17.9 | 17.6 | |
| Other | 2520 | 1496 | 44.4 | (42.1–46.0) | 42.6 | (40.1–45.1) | 19.1 | 20.6 | |
| p | p = 0.30 | p = 0.07 | p = 0.19 | p = 0.04 | |||||
| Women | Age | ||||||||
| 18–24 | 645 | 407 | 17.0 | (13.7–19.6) | 16.5 | (12.8–20.1) | 6.2 | 5.8 | |
| 25–34 | 1268 | 870 | 22.0 | (19.4–24.0) | 19.1 | (15.6–20.7) | 6.7 | 7.3 | |
| 35–44 | 1117 | 997 | 30.1 | (26.8–32.1) | 26.3 | (23.8–29.3) | 9.6 | 11.4 | |
| 45–54 | 987 | 879 | 30.4 | (28.1–33.9) | 33.0 | (28.8–34.4) | 9.4 | 12.3 | |
| 55–64 | 765 | 760 | 25.1 | (22.1–28.3) | 31.7 | (28.9–35.2) | 5.8 | 13.4 | |
| 65+ | 1058 | 1193 | 21.6 | (19.2–24.1) | 26.8 | (24.3–29.3) | 4.6 | 9.1 | |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||
| Day of the Week | |||||||||
| Sunday-Thursday | 5103 | 4409 | 23.4 | (22.1–24.4) | 25.5 | (24.2–26.8) | 6.5 | 9.4 | |
| Friday-Saturday | 737 | 697 | 34.3 | (31.0–37.9) | 30.1 | (26.7–33.5) | 11.6 | 13.5 | |
| p | <0.0001 | 0.01 | <0.0001 | <0.0001 | |||||
| Season | |||||||||
| December-April | 2373 | 2384 | 24.8 | (23.0–26.5) | 26.2 | (24.4–27.9) | 7.3 | 10.0 | |
| May-November | 3467 | 2722 | 24.6 | (23.1–26.0) | 26.1 | (24.5–27.8) | 7.1 | 10.0 | |
| p | p = 0.85 | p = 0.97 | p = 0.70 | p = 0.99 | |||||
| Geographic Area | |||||||||
| Metropolitan | 3005 | 3218 | 25.1 | (23.5–26.6) | 27.3 | (25.7–28.8) | 7.2 | 10.3 | |
| Other | 2835 | 1888 | 24.5 | (22.6–25.8) | 24.2 | (22.3–26.1) | 7.2 | 9.3 | |
| p | p = 0.45 | p = 0.02 | p = 0.95 | p = 0.24 | |||||
| Sample Size (n) | Proportion (95% CI) Consuming Alcohol (%) | Per-Capita Alcohol (g) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | 1983 | 1995 | 2011/12 | 1983 | 1995 | 2011/12 | p † | 1983 | 1995 | 2011/12 | p ‡ | |||
| Men | 18–24 | 0 | 474 | 322 | 26.2 | (22.2–30.1) | 22.4 | (17.8–26.9) | >0.05 | 11.5 | 10.3 | 0.22 | |||
| 25–34 | 823 | 902 | 597 | 50.2 | (45.7–52.7) | 39.6 | (36.4–42.8) | 34.0 | (30.2–37.8) | <0.0001 | 22.5 a | 18.2 a,b | 14.0 b | 0.08 | |
| 35–44 | 823 | 889 | 671 | 53.0 | (49.6–56.6) | 41.6 | (38.4–44.9) | 37.0 | (33.3–40.6) | <0.0001 | 26.5 a | 17.4 b | 16.8 b | 0.002 | |
| 45–54 | 703 | 771 | 644 | 51.0 | (46.7–54.7) | 47.9 | (44.3–51.4) | 43.2 | (39.3–47.0) | 0.03 | 25.9 | 18.9 | 22.2 | 0.11 | |
| 55–64 | 672 | 584 | 583 | 54.0 | (50.1–57.1) | 48.5 | (44.4–52.5) | 45.3 | (41.2–49.3) | 0.009 | 25.7 | 20.0 | 22.7 | 0.03 | |
| 65+ | 0 | 816 | 843 | 42.7 | (39.3–46.0) | 43.7 | (40.3–47.0) | >0.05 | 14.3 | 17.1 | 0.28 | ||||
| 25–64 § | 3021 | 3205 | 2579 | 52.0 | (49.7–53.3) | 44.2 | (42.1–45.6) | 39.8 | (37.9–41.7) | <0.0001 | 25.2 a | 18.6 b | 18.8 b | <0.0001 | |
| 18+ § | 0 | 4436 | 3660 | 41.4 | (40.3–43.2) | 39.2 | (37.6–40.7) | 0.02 | 17.7 | 17.9 | 0.7 | ||||
| Women | 18–24 | 0 | 568 | 340 | 15.0 | (12.0–17.9) | 16.2 | (12.3–20.1) | >0.5 | 5.1 | 6.1 | 0.63 | |||
| 25–34 | 869 | 1079 | 740 | 30.8 | (27.3–33.3) | 19.5 | (17.1–21.8) | 17.3 | (14.6–20.0) | <0.0001 | 8.8 | 6.0 | 5.6 | 0.06 | |
| 35–44 | 895 | 950 | 827 | 34.2 | (31.4–37.4) | 28.1 | (25.2–31.0) | 24.4 | (21.5–27.4) | <0.0001 | 11.0 | 8.6 | 10.4 | 0.44 | |
| 45–54 | 727 | 851 | 754 | 32.5 | (28.6–35.6) | 29.8 | (26.8–32.9) | 30.9 | (27.6–34.2) | >0.5 | 8.2 a | 8.8 a,b | 11.5 b | 0.08 | |
| 55–64 | 742 | 693 | 662 | 28.6 | (25.3–31.3) | 24.4 | (21.2–27.6) | 32.2 | (28.6–35.7) | 0.01 | 7.5 a | 5.6 a | 13.1 b | 0.0018 | |
| 65+ | 0 | 962 | 1086 | 20.8 | (18.2–23.4) | 27.1 | (24.5–29.7) | <0.0001 | 4.4 | 9.3 | <0.0001 | ||||
| 25–64 § | 3233 | 3633 | 3076 | 31.6 | (29.9–33.9) | 25.7 | (23.8–26.6) | 25.7 | (24.4–27.6) | <0.0001 | 8.9 a,b | 7.2 a | 9.9 b | 0.09 | |
| 18+ § | 0 | 5103 | 4409 | 23.2 | (22.1–24.4) | 25.5 | (24.2–26.8) | 0.009 | 6.9 | 9.6 | <0.0001 | ||||
| All | 25–64 § | 6254 | 6838 | 5655 | 41.1 | (39.9–42.9) | 34.2 | (32.8–35.1) | 32.3 | (31.1–33.5) | <0.0001 | 16.4 a | 12.8 b | 14.2 b | <0.001 |
| 18+ § | 0 | 9539 | 8069 | 32.3 | (30.9–32.8) | 31.7 | (30.7–32.7) | >0.05 | 12.2 | 13.7 | <0.0004 | ||||
| Gender | Variable | Age | 1983 | 1995 | 2012 | p * | |||
|---|---|---|---|---|---|---|---|---|---|
| Men | Alcohol (g) | 18–24 | 28.6 | (14.3–51.7) | 36.4 | (13.6–68.2) | >0.05 | ||
| 25–34 | 28.5 | (14.3–55.5) | 28.6 | (15.4–59.0) | 35.2 | (17.7–54.6) | >0.05 | ||
| 35–44 | 34.9 | (21.1–62.0) | 34.4 | (17.8–58.1) | 37.7 | (16.3–58.4) | >0.05 | ||
| 45–54 | 35.8 | (18.5–59.9) | 32.3 | (17.5–50.2) | 40.9 | (20.7–77.6) | 0.002 | ||
| 55–64 | 30.2 | (17.5–55.5) | 32.3 | (16.9–53.6) | 40.9 | (25.0–73.4) | <0.0001 | ||
| 65+ | 28.8 | (15.8–52.1) | 26.4 | (14.3–45.8) | 0.03 | ||||
| Alcohol (%E) | 18–24 | 8.8 | (4.6–16.5) | 15.1 | (6.4–22.2) | 0.03 | |||
| 25–34 | 8.5 | (4.5–16.8) | 10.3 | (5.3–18.3) | 11.8 | (6.7–18.8) | 0.01 | ||
| 35–44 | 12.0 | (6.6–20.2) | 12.1 | (6.9–20.1) | 13.1 | (7.1–23.3) | >0.05 | ||
| 45–54 | 12.9 | (7.4–20.7) | 11.8 | (6.5–18.7) | 15.1 | (8.6–24.5) | <0.0001 | ||
| 55–64 | 12.4 | (6.3–21.0) | 12.9 | (6.9–20.0) | 15.7 | (8.9–25.1) | <0.0001 | ||
| 65+ | 10.9 | (7.4–20.5) | 12.2 | (6.4–21.2) | 0.03 | ||||
| Women | Alcohol (g) | 18–24 | 23.8 | (14.1–42.9) | 22.9 | (13.6–49.0) | >0.05 | ||
| 25–34 | 19.6 | (10.9–31.2) | 23.4 | (14.3–42.7) | 27.3 | (14.3–45.7) | 0.0003 | ||
| 35–44 | 18.6 | (11.6–34.9) | 23.9 | (12.7–39.5) | 29.4 | (15.3–54.5) | <0.0001 | ||
| 45–54 | 16.0 | (8.8–33.3) | 21.2 | (11.7–37.6) | 27.9 | (15.3–48.3) | <0.0001 | ||
| 55–64 | 14.1 | (8.8–27.4) | 17.8 | (10.7–35.0) | 30.5 | (18.4–58.8) | <0.0001 | ||
| 65+ | 17.3 | (9.8–28.3) | 26.1 | (14.7–42.1) | 0.03 | ||||
| Alcohol (%E) | 18–24 | 11.6 | (6.4–21.2) | 11.0 | (7.2–18.1) | >0.05 | |||
| 25–34 | 8.4 | (4.4–13.2) | 9.6 | (5.7–15.8) | 10.2 | (7.5–18.4) | 0.003 | ||
| 35–44 | 8.4 | (5.0–15.5) | 10.0 | (5.9–18.1) | 13.2 | (7.6–21.7) | <0.0001 | ||
| 45–54 | 8.6 | (4.6–15.2) | 8.9 | (5.3–16.7) | 12.5 | (7.6–20.2) | <0.0001 | ||
| 55–64 | 7.5 | (4.4–13.6) | 7.9 | (4.9–14.5) | 15.1 | (8.8–23.0) | <0.0001 | ||
| 65+ | 8.9 | (5.4–13.3) | 11.5 | (7.7–18.1) | <0.0001 | ||||
| Total | Alcohol (g) | 25–64 | 27.9 | (13.9–48.8) | 28.6 | (15.1–47.9) | 32.7 | (18.0–61.4) | <0.0001 |
| Alcohol (%E) | 25–64 | 9.9 | (5.4–17.1) | 11.1 | (6.0–18.3) | 13.4 | (6.2–18.8) | <0.0001 | |
| Gender | Beverage | Variable | Median Per-Consumer (IQR) | p * | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1983 | 1995 | 2012 | |||||||
| Men | Beer | Consumer (%) | 31.6 | (31.0–35.4) | 29.0 | (26.6–30.4) | 23.1 | (21.0–25.3) | <0.0001 |
| Alcohol (g) | 28.5 | (14.3–57.0) | 28.6 | (14.3–55.7) | 29.6 | (13.6–54.5) | 0.8 | ||
| Alcohol (%E) | 10.8 | (5.8–19.2) | 11.5 | (5.9–20.0) | 12.1 | (6.6–20.3) | 0.01 | ||
| Alcohol (kJ) | 1125 | (563–2250) | 1127 | (563–2252) | 1145 | (542–2166) | 0.4 | ||
| Wine | Consumer (%) | 23.5 | (22.0–25.0) | 15.6 | (14.6–17.2) | 14.0 | (13.2–15.9) | <0.0001 | |
| Alcohol (g) | 27.0 | (15.5–42.6) | 28.7 | (17.6–43.1) | 40.8 | (24.5–68.6) | <0.0001 | ||
| Alcohol (%E) | 7.9 | (4.5–13.2) | 8.5 | (5.0–12.8) | 12.1 | (7.6–20.1) | <0.0001 | ||
| Alcohol (kJ) | 878 | (473–1415) | 931 | (555–1414) | 1203 | (770–2072) | <0.0001 | ||
| Spirits | Consumer (%) | 8.7 | (8.7–7.7) | 5.0 | (5.1–4.3) | 6.0 | (6.4–5.5) | <0.0001 | |
| Alcohol (g) | 17.6 | (8.8–26.8) | 17.8 | (9.7–29.3) | 18.3 | (14.3–42.0) | <0.0001 | ||
| Alcohol (%E) | 4.8 | (2.6–7.7) | 4.8 | (2.8–7.6) | 8.3 | (4.4–17.3) | <0.0001 | ||
| Alcohol (kJ) | 511 | (256–780) | 518 | (280–1011) | 981 | (514–1970) | <0.0001 | ||
| Other † | Consumer (%) | 1.9 | (1.4–2.3) | 1.4 | (1.0–1.8) | 1.1 | (0.7–1.5) | 0.006 | |
| Alcohol (g) | 9.9 | (6.2–15.7) | 12.7 | (5.8–24.6) | 14.4 | (4.3–26.5) | 0.5 | ||
| Alcohol (%E) | 5.6 | (3.1–10.0) | 5.0 | (3.5–10.1) | 7.3 | (4.3–12.8) | 0.2 | ||
| Alcohol (kJ) | 660 | (454–1040) | 709 | (430–1206) | 704 | (439–1296) | 0.1 | ||
| Women | Beer | Consumer (%) | 5.4 | (4.4–6.4) | 4.8 | (3.9–5) | 4.2 | (3.0–4.7) | 0.2 |
| Alcohol (g) | 10.8 | (5.3–21.5) | 14.6 | (8.1–28.6) | 20.5 | (12.7–38.7) | <0.0001 | ||
| Alcohol (%E) | 6.0 | (3.4–11.0) | 8.8 | (5.1–18.0) | 9.4 | (6.2–16.8) | <0.0001 | ||
| Alcohol (kJ) | 461 | (249–878) | 583 | (395–1127) | 824 | (506–1538) | <0.0001 | ||
| Wine | Consumer (%) | 22.8 | (21.4–24.3) | 16.9 | (15.4–18.3) | 18.9 | (17.0–20.7) | <0.0001 | |
| Alcohol (g) | 18.6 | (11.6–32.0) | 23.5 | (14.4–38.3) | 30.5 | (19.8–54.5) | <0.0001 | ||
| Alcohol (%E) | 8.3 | (4.8–13.3) | 9.5 | (5.9–15.8) | 12.9 | (7.7–20.9) | <0.0001 | ||
| Alcohol (kJ) | 663 | (354–1061) | 708 | (486–1217) | 927 | (609–1604) | <0.0001 | ||
| Spirits | Consumer (%) | 6.6 | (6.6–5.7) | 4.3 | (4.3–3.7) | 3.5 | (3.7–3.0) | <0.0001 | |
| Alcohol (g) | 9.1 | (8.8–17.6) | 11.8 | (6.0–18.5) | 19.6 | (13.7–37.1) | <0.0001 | ||
| Alcohol (%E) | 4.2 | (2.6–7.3) | 4.6 | (2.6–8.8) | 12.1 | (7.4–21.3) | <0.0001 | ||
| Alcohol (kJ) | 264 | (256–511) | 345 | (174–690) | 984 | (514–1733) | <0.0001 | ||
| Other † | Consumer (%) | 1.9 | (1.4–2.3) | 1.4 | (1.0–1.8) | 1.1 | (0.7–1.5) | 0.048 | |
| Alcohol (g) | 6.3 | (4.4–10.5) | 10.6 | (4.4–17.4) | 12.0 | (8.0–14.4) | 0.007 | ||
| Alcohol (%E) | 6.4 | (3.2–9.4) | 6.5 | (3.9–14.8) | 7.2 | (4.2–9.6) | 0.6 | ||
| Alcohol (kJ) | 495 | (330–825) | 591 | (430–1013) | 558 | (432–704) | 0.5 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grech, A.; Rangan, A.; Allman-Farinelli, M. Increases in Alcohol Intakes Are Concurrent with Higher Energy Intakes: Trends in Alcohol Consumption in Australian National Surveys from 1983, 1995 and 2012. Nutrients 2017, 9, 944. https://doi.org/10.3390/nu9090944
Grech A, Rangan A, Allman-Farinelli M. Increases in Alcohol Intakes Are Concurrent with Higher Energy Intakes: Trends in Alcohol Consumption in Australian National Surveys from 1983, 1995 and 2012. Nutrients. 2017; 9(9):944. https://doi.org/10.3390/nu9090944
Chicago/Turabian StyleGrech, Amanda, Anna Rangan, and Margaret Allman-Farinelli. 2017. "Increases in Alcohol Intakes Are Concurrent with Higher Energy Intakes: Trends in Alcohol Consumption in Australian National Surveys from 1983, 1995 and 2012" Nutrients 9, no. 9: 944. https://doi.org/10.3390/nu9090944