Assessment of Urinary Deoxynivalenol Biomarkers in UK Children and Adolescents

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
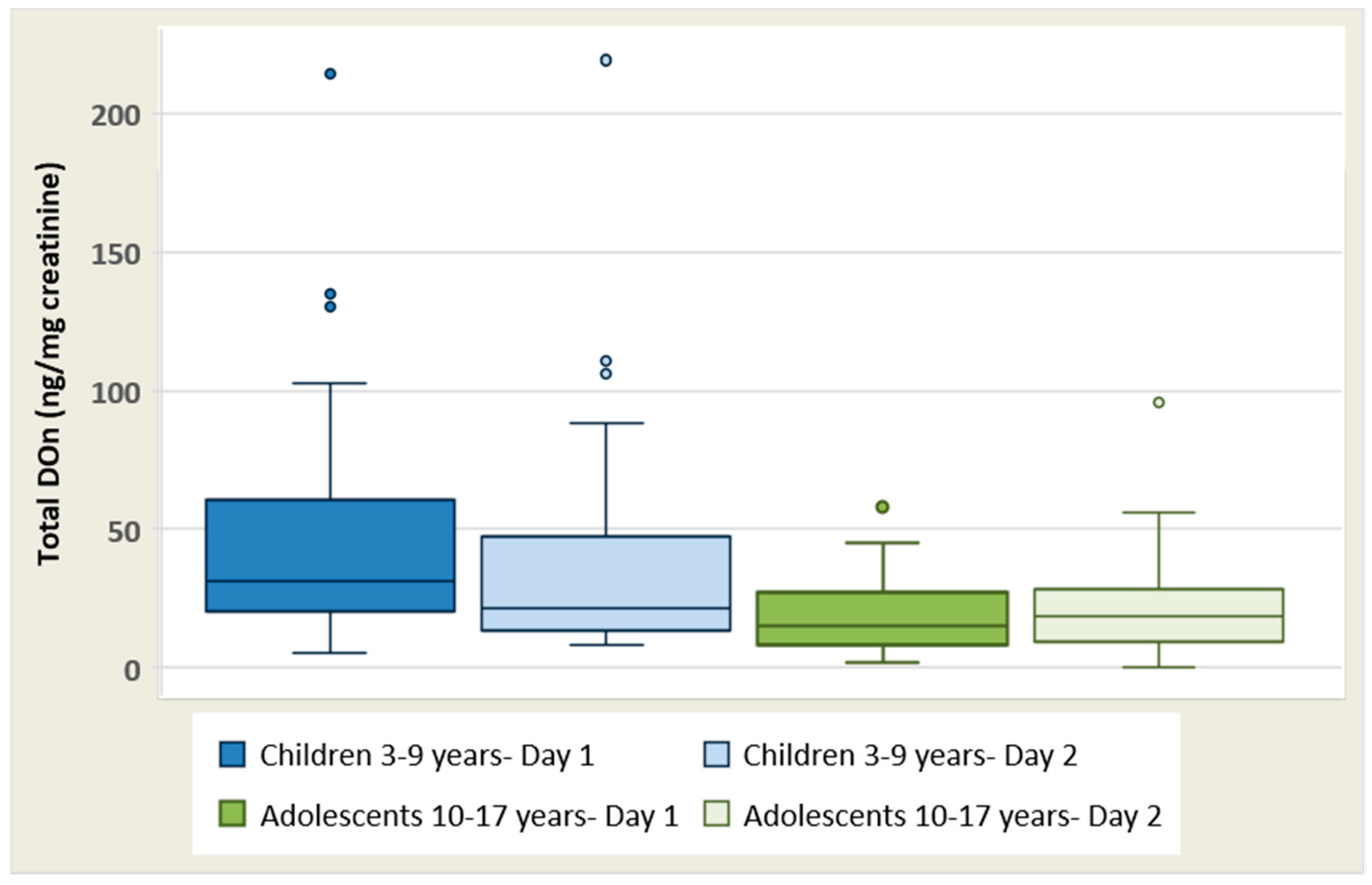
2.2. DON Biomarker Levels in Urine Samples
2.3. Estimated Dietary Intake of DON Based on Urinary Analysis
2.4. Correlation between Urinary DON, Demographic and Anthropometric Characteristics
2.5. Correlation between Urinary Total DON and Food Intake
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Participants Selection and Recruitment
5.2. Study Design
5.3. Laboratory Analysis
5.3.1. Sample Preparation
5.3.2. HPLC-MS Analysis: DON Determination
5.3.3. LC-MS Analysis: DOM-1 Determination
5.3.4. Creatinine Analysis
5.4. Estimated Dietary Intake of DON Based on Urinary Levels and Comparison with PMTDI
- Estimated dietary intake DON (μg/kg b.w./day) =
- ER = urinary excretion rate of DON is 72% [13].
- V = estimated urine volume (mL/day) for children and adolescents. Minimum, maximum, and mean values within the range provided for children (1–2 mL/kg b.w./h) and adolescents (0.5–1 mL/kg b.w./h) [25] were tested.
- b.w. = body weight (kg) reported in the questionnaire
5.5. Dietary Analysis
5.6. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European Food Safety Authority (EFSA). Deoxynivalenol in food and feed: Occurrence and exposure. EFSA J. 2013, 11, 3379–3435. [Google Scholar]
- Pestka, J.J. Deoxynivalenol: Mechanisms of action, human exposure, and toxicological relevance. Arch. Toxicol. 2010, 84, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Council for Agricultural Science and Technology (CAST). Mycotoxins: Risks in Plant, Animal, and Human Systems; CAST: Ames, IA, USA, 2003. [Google Scholar]
- Van der Lee, T.; Zhang, H.; van Diepeningen, A.; Waalwijk, C. Biogeography of Fusarium graminearum species complex and chemotypes: A review. Food Addit. Contam. A Chem. Anal. Control Expo. Risk Assess. 2015, 32, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Food (SCF). Opinion of the Scientific Committee on Food on Fusarium-Toxins Part 1: Deoxynivalenol (DON). Available online: http://ec.europa.eu/food/fs/sc/scf/out44_en.pdf (accessed on 13 December 2017).
- Joint Expert Committee on Food and Additives (JECFA). Evaluation of certain food additives and contaminants. In Report of the Seventy-Second Meeting of the Joint FAO/WHO Expert Committee on Food Additives; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Pieters, M.N.; Freijer, J.; Baars, B.J.; Fiolet, D.C.; van Klaveren, J.; Slob, W. Risk assessment of deoxynivalenol in food: Concentration limits, exposure and effects. Adv. Exp. Med. Biol. 2002, 504, 235–248. [Google Scholar] [PubMed]
- Schneider, E.; Curtui, V.; Seidler, C.; Dietrich, R.; Usleber, E.; Martlbauer, E. Rapid methods for deoxynivalenol and other trichothecenes. Toxicol. Lett. 2004, 153, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.W.; Klich, M. Mycotoxins. Clin. Microbiol. Rev. 2003, 16, 497–516. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Takino, M.; Sugita-Konishi, Y.; Tanaka, T.; Leeman, D.; Toriba, A.; Hayakawa, K. Determination of Fusarium mycotoxins by liquid chromatography/tandem mass spectrometry coupled with immunoaffinity extraction. Rapid Commun. Mass Spectrom. 2010, 24, 2445–2452. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Burley, V.J.; Rothwell, J.A.; White, K.L.; Cade, J.E.; Wild, C.P. Deoxynivalenol: Rationale for development and application of a urinary biomarker. Food Addit. Contam. A Chem. Anal. Control Expo. Risk Assess. 2008, 25, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Rothwell, J.A.; White, K.L.; Gong, Y.; Cade, J.E.; Wild, C.P. Urinary deoxynivalenol is correlated with cereal intake in individuals from the United kingdom. Environ. Health Perspect. 2008, 116, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; White, K.L.; Burley, V.J.; Hopton, R.P.; Rajendram, A.; Fisher, J.; Cade, J.E.; Wild, C.P. A comparison of deoxynivalenol intake and urinary deoxynivalenol in UK adults. Biomarkers 2010, 15, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Warth, B.; Sulyok, M.; Krska, R. LC-MS/MS-based multibiomarker approaches for the assessment of human exposure to mycotoxins. Anal. Bioanal. Chem. 2013, 405, 5687–5695. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Hopton, R.P.; Lecluse, Y.; White, K.L.; Fisher, J.; Lebailly, P. Determinants of urinary deoxynivalenol and de-epoxy deoxynivalenol in male farmers from Normandy, France. J. Agric. Food Chem. 2010, 58, 5206–5212. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Blaszkewicz, M.; Degen, G.H. Assessment of deoxynivalenol exposure among Bangladeshi and German adults by a biomarker-based approach. Toxicol. Lett. 2016, 258, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Follmann, W.; Ali, N.; Blaszkewicz, M.; Degen, G.H. Biomonitoring of Mycotoxins in Urine: Pilot Study in Mill Workers. J. Toxicol. Environ. Health A 2016, 79, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Wells, L.; Hardie, L.; Williams, C.; White, K.; Liu, Y.; De Santis, B.; Debegnach, F.; Moretti, G.; Greetham, S.; Brera, C.; et al. Deoxynivalenol Biomarkers in the Urine of UK Vegetarians. Toxins (Basel) 2017, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- Wells, L.; Hardie, L.; Williams, C.; White, K.; Liu, Y.; De Santis, B.; Debegnach, F.; Moretti, G.; Greetham, S.; Brera, C.; et al. Determination of deoxynivalenol in the urine of pregnant women in the UK. Toxins (Basel) 2016, 8, 306. [Google Scholar] [CrossRef] [PubMed]
- Brera, C.; de Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Lanzone, A.; Del Sordo, G.; Buonsenso, D.; Chiaretti, A.; Hardie, L.; et al. Experimental study of deoxynivalenol biomarkers in urine. EFSA Support. Publ. 2015, 12, 818E. [Google Scholar] [CrossRef]
- Heyndrickx, E.; Sioen, I.; Huybrechts, B.; Callebaut, A.; De Henauw, S.; De Saeger, S. Human biomonitoring of multiple mycotoxins in the Belgian population: Results of the BIOMYCO study. Environ. Int. 2015, 84, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Carrasco, Y.; Molto, J.C.; Manes, J.; Berrada, H. Development of a GC-MS/MS strategy to determine 15 mycotoxins and metabolites in human urine. Talanta 2014, 128, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Makri, A.; Goveia, M.; Balbus, J.; Parkin, R. Children’s susceptibility to chemicals: A review by developmental stage. J. Toxicol. Environ. Health B Crit. Rev. 2004, 7, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Hopton, R.P.; White, K.L.; Fisher, J.; Cade, J.E.; Wild, C.P. Assessment of deoxynivalenol metabolite profiles in UK adults. Food Chem. Toxicol. 2011, 49, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Hazinski, M.F. Normal urine output in children. In Nursing Care of the Critically Ill Child, 3rd ed.; Elsevier: St. Louis, MO, USA, 2013. [Google Scholar]
- Gerding, J.; Ali, N.; Schwartzbord, J.; Cramer, B.; Brown, D.L.; Degen, G.H.; Humpf, H.U. A comparative study of the human urinary mycotoxin excretion patterns in Bangladesh, Germany, and Haiti using a rapid and sensitive LC-MS/MS approach. Mycotoxin Res. 2015, 31, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Srey, C.; Kimanya, M.E.; Routledge, M.N.; Shirima, C.P.; Gong, Y.Y. Deoxynivalenol exposure assessment in young children in Tanzania. Mol. Nutr. Food Res. 2014, 58, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Ezekiel, C.N.; Warth, B.; Ogara, I.M.; Abia, W.A.; Ezekiel, V.C.; Atehnkeng, J.; Sulyok, M.; Turner, P.C.; Tayo, G.O.; Krska, R.; et al. Mycotoxin exposure in rural residents in northern Nigeria: A pilot study using multi-urinary biomarkers. Environ. Int. 2014, 66, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Warth, B.; Sulyok, M.; Fruhmann, P.; Mikula, H.; Berthiller, F.; Schuhmacher, R.; Hametner, C.; Abia, W.A.; Adam, G.; Frohlich, J.; et al. Development and validation of a rapid multi-biomarker liquid chromatography/tandem mass spectrometry method to assess human exposure to mycotoxins. Rapid Commun. Mass Spectrom. 2012, 26, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Gratz, S.W.; Richardson, A.J.; Duncan, G.; Holtrop, G. Annual variation of dietary deoxynivalenol exposure during years of different Fusarium prevalence: A pilot biomonitoring study. Food. Addit. Contam. A Chem. Anal. Control. Expo. Risk Assess. 2014, 31, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, E.; Schittenhelm, S. Effect of plant water deficit on the deoxynivalenol concentration in Fusarium-infected maize kernels. Mycotoxin Res. 2012, 28, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Bullerman, L.B.; Bianchini, A. Stability of mycotoxins during food processing. Int. J. Food Microbiol. 2007, 119, 140–146. [Google Scholar] [CrossRef] [PubMed]
- De Santis, B.; Brera, C.; Mezzelani, A.; Soricelli, S.; Ciceri, F.; Moretti, G.; Debegnach, F.; Bonaglia, M.C.; Villa, L.; Molteni, M.; et al. Role of mycotoxins in the pathobiology of autism: A first evidence. Nutr. Neurosci. 2017, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gratz, S.W.; Duncan, G.; Richardson, A.J. The human fecal microbiota metabolizes deoxynivalenol and deoxynivalenol-3-glucoside and may be responsible for urinary deepoxy-deoxynivalenol. Appl. Environ. Microbiol. 2013, 79, 1821–1825. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of multi-mycotoxin exposure in southern Italy by urinary multi-biomarker determination. Toxins (Basel) 2014, 6, 523–538. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Burley, V.J.; Rothwell, J.A.; White, K.L.; Cade, J.E.; Wild, C.P. Dietary wheat reduction decreases the level of urinary deoxynivalenol in UK adults. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Yu, M.; Wu, Q.; Peng, Z.; Wang, D.; Kuca, K.; Yao, P.; Yan, H.; Nussler, A.K.; Liu, L.; et al. Gender and geographical variability in the exposure pattern and metabolism of deoxynivalenol in humans: A review. J. Appl. Toxicol. 2017, 37, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Food (SCF). Opinion of the Scientific Committee on Food on Fusarium Toxins. Part 6: Group Evaluation of T-2 Toxin, HT-2 Toxin, Nivalenol and Deoxynivalenol. Available online: http://ec.europa.eu/food/fs/sc/scf/out123_en.pdf (accessed on 3 March 2017).
- Hepworth, S.J.; Hardie, L.J.; Fraser, L.K.; Burley, V.J.; Mijal, R.S.; Wild, C.P.; Azad, R.; McKinney, P.A.; Turner, P.C. Deoxynivalenol exposure assessment in a cohort of pregnant women from Bradford, UK. Food Addit. Contam. A Chem. Anal. Control Expo. Risk Assess. 2012, 29, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Agency. Food Portion Sizes, 3rd ed.; TSO: London, UK, 2005. [Google Scholar]
- Cheyette, C.; Balolia, Y. A Visual Guide to Carbohydrate & Calorie Counting for People with Diabetes, 4th ed.; Chello Publishing Limited: London, UK, 2010. [Google Scholar]
- European Food Safety Authority (EFSA). Evaluation of the FoodEx, the food classification system applied to the development of the EFSA Comprehensive European Food Consumption Database. EFSA J. 2011, 9, 1970. [Google Scholar]


{kind=link}
| Age Group | Day | Gender (a) | Total DON (ng/mL Urine) | Total DON (ng/mg Creatinine) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | Range (b) | P50–P75 | Mean | Range (b) | P50–P75 | |||
| Children (3–9 years) (n = 40) | 1 | F (20) | 38.2 | 3.0–138 | 22.5–47.1 | 56.3 | 6.8–214.0 | 44.1–73.9 |
| M (20) | 22.5 | 1.2–86.5 | 18.3–31.0 | 33.9 | 5.3–130.0 | 25.3–37.3 | ||
| 2 | F (20) | 35.4 | 1.4–140.9 | 23.7–51.0 | 43.8 | 8.0–219.0 | 23.1–52.9 | |
| M (20) | 20.6 | 4.1–52.0 | 15.9–32.4 | 32.1 | 8.2–88.4 | 20.6–44.3 | ||
| Adolescents (10–17 years) (n = 39) | 1 | F (20) | 26.0 | 3.1–104.3 | 19.6–30.8 | 19.4 | 2.1–58.0 | 15.4–27.3 |
| M (19) | 20.6 | 1.6–52.5 | 18.2–30.9 | 19.0 | 1.8–45.3 | 15.0–31.9 | ||
| 2 | F (20) | 28.8 | 0–67.2 | 24.9–48.0 | 20.8 | 0–51.8 | 18.5–25.1 | |
| M (19) | 27.0 | 2.9–66.3 | 19.7–40.2 | 25.0 | 2.2–95.6 | 14.5–32.9 | ||
| Age Group | Day | Gender (a) | Free DON (ng /mg Creatinine) | DON-GlcA (ng /mg Creatinine) | DOM-1 (ng /mg Creatinine) |
|---|---|---|---|---|---|
| Children (3–9 years) (n = 40) | 1 | F (20) | 12.4 (0.0–51.0) | 43.9 (5.0–168) | nd |
| M (20) | 7.5 (1.5–32.8) | 26.5 (3.8–97.5) | nd | ||
| 2 | F (20) | 6.8 (0.0–55.2) | 38.2 (6.0–182) | nd | |
| M (20) | 6.8 (1.1–29.4) | 25.2 (7.1–59.8) | nd | ||
| Adolescent (10–17 years) (n = 39) | 1 | F (20) | 2.8 (0.0–10.2) | 16.7 (2.1–47.9) | nd |
| M (19) | 3.7 (0.0–8.9) | 17.6 (0.0–45.2) | nd | ||
| 2 | F (20) | 2.7 (0.0–6.9) | 15.3 (1.8–37.7) | nd | |
| M (19) | 5.3 (0.0–17.0) | 19.7 (1.1–78.6) | nd |
| Age Group | Estimated Urine Volume | DON (μg/kg·b.w./Day) | % Exceeding TDI |
|---|---|---|---|
| Children (3–9 years) (n = 40) | 1 mL/kg b.w./h | 0.97 (0.14–4.6) | 33 (13/40) |
| 1.5 mL/kg b.w./h | 1.46 (0.20–6.96) | 50 (20/40) | |
| 2 mL/kg b.w./h | 1.95 (0.30–9.28) | 63 (25/40) | |
| Adolescents (10–17 years) (n = 39) | 0.5 mL/kg b.w./h | 0.47 (0.03–1.22) | 5 (2/39) |
| 0.75 mL/kg b.w./h | 0.64 (0.04–1.75) | 21 (8/39) | |
| 1 mL/kg b.w./h | 0.95 (0.05–2.44) | 46 (18/39) |
| Food Category | Children (3–9 Years) (n = 40) | Adolescents (10–17 Years) (n = 39) |
|---|---|---|
| Bread (g/d) (a) | 107 ± 62 (23–315) | 95 ± 58 (0–225) |
| Breakfast cereals (g/d) | 20 ± 15 (0–65) | 19 ± 16 (0–63) |
| Sweet snacks (g/d) (b) | 44 ± 33 (0–112) | 57 ± 55 (0–198) |
| Pizza (g/d) | 19 ± 28 (0–85) | 31 ± 53 (0–213) |
| Pasta (g/d) | 63 ± 62 (0–190) | 62 ± 76 (0–290) |
| Total (g/d) | 252 ± 89 (95–454) | 264 ± 102 (116–516) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papageorgiou, M.; Wells, L.; Williams, C.; White, K.; De Santis, B.; Liu, Y.; Debegnach, F.; Miano, B.; Moretti, G.; Greetham, S.; et al. Assessment of Urinary Deoxynivalenol Biomarkers in UK Children and Adolescents. Toxins 2018, 10, 50. https://doi.org/10.3390/toxins10020050
Papageorgiou M, Wells L, Williams C, White K, De Santis B, Liu Y, Debegnach F, Miano B, Moretti G, Greetham S, et al. Assessment of Urinary Deoxynivalenol Biomarkers in UK Children and Adolescents. Toxins. 2018; 10(2):50. https://doi.org/10.3390/toxins10020050
Chicago/Turabian StylePapageorgiou, Maria, Liz Wells, Courtney Williams, Kay White, Barbara De Santis, Yunru Liu, Francesca Debegnach, Brunella Miano, Giorgio Moretti, Stephanie Greetham, and et al. 2018. "Assessment of Urinary Deoxynivalenol Biomarkers in UK Children and Adolescents" Toxins 10, no. 2: 50. https://doi.org/10.3390/toxins10020050