Real Time Monitoring of Children, and Adults with Mental Disabilities Using a Low-Cost Non-Invasive Electronic Device

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
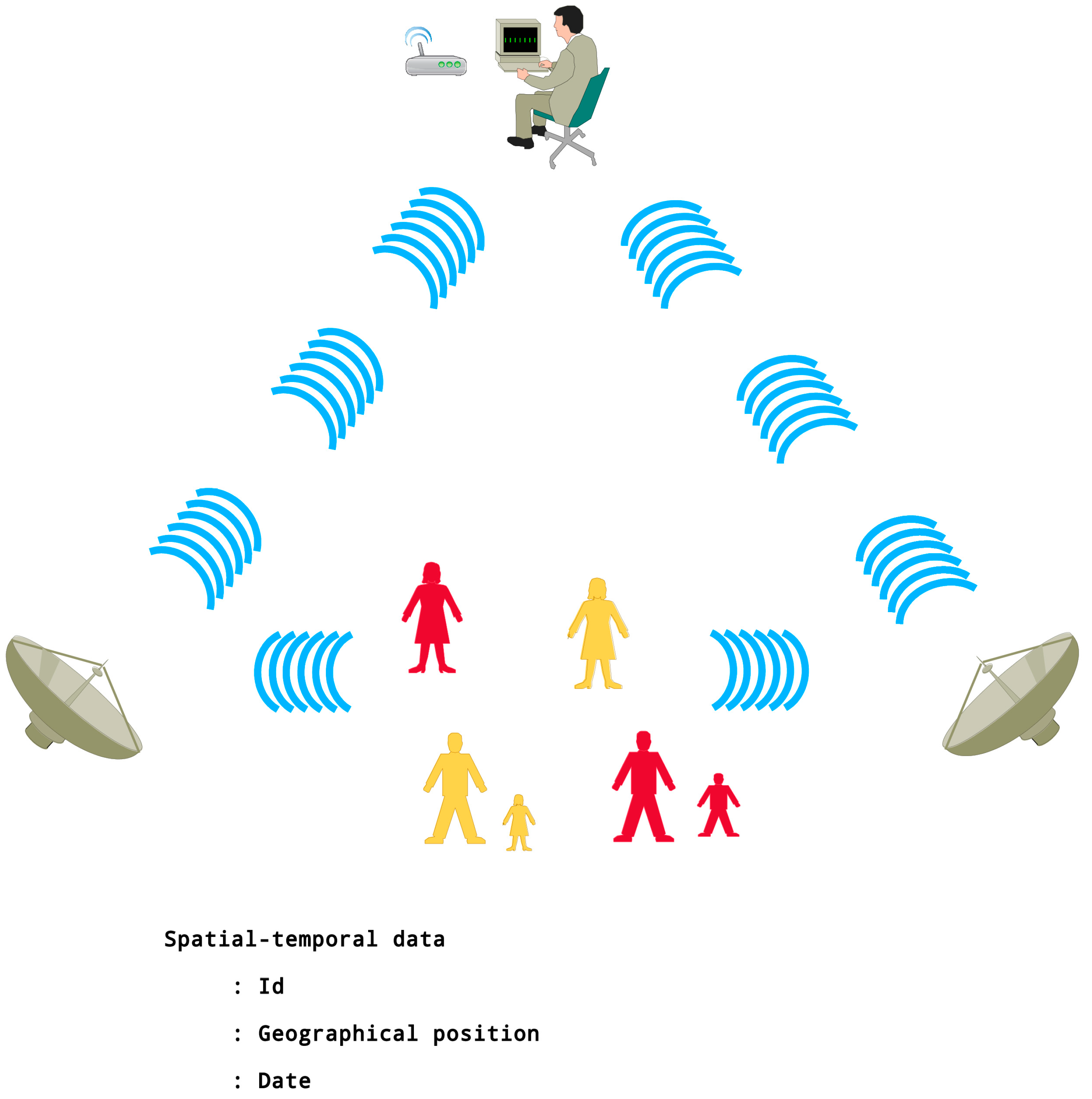
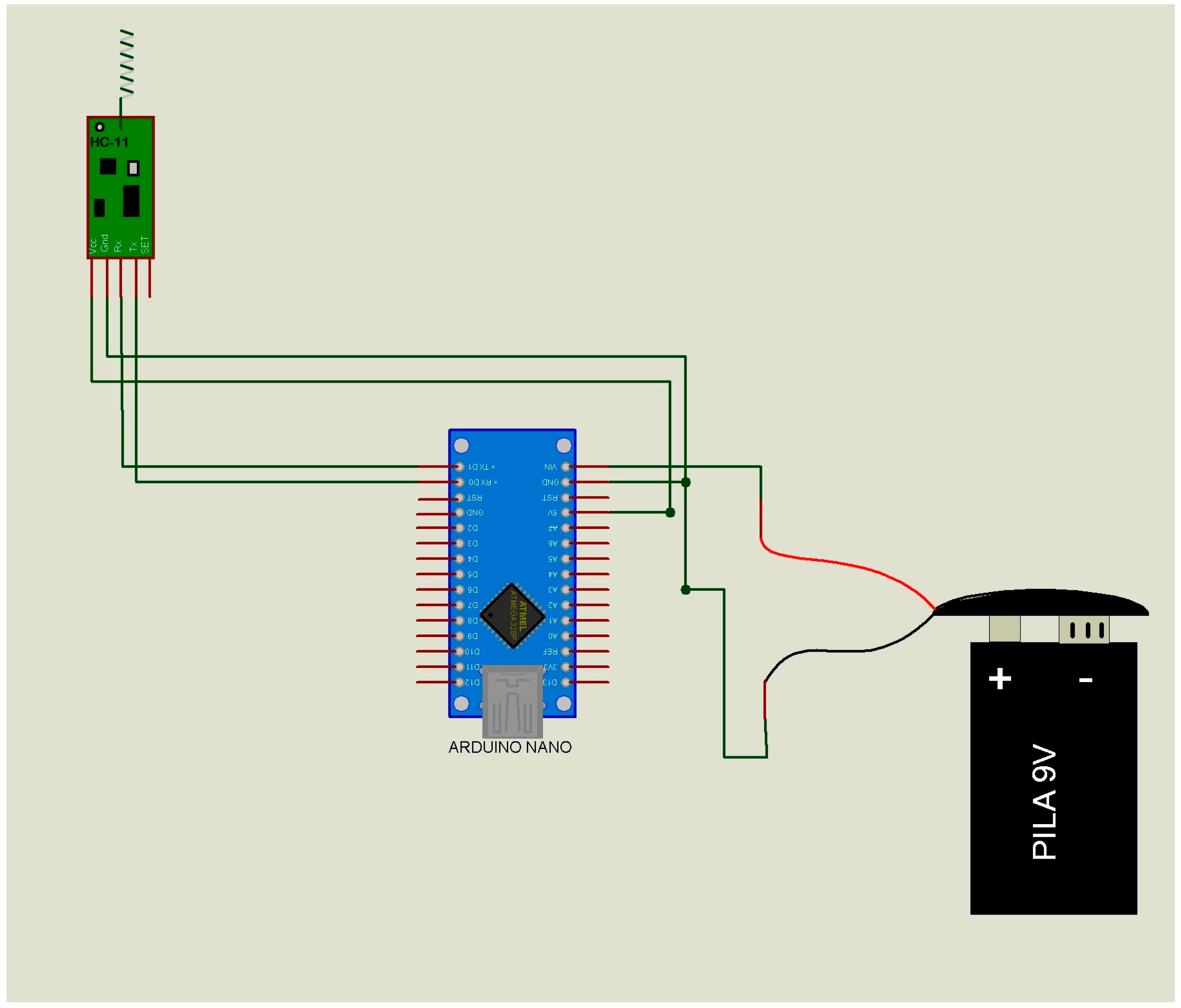
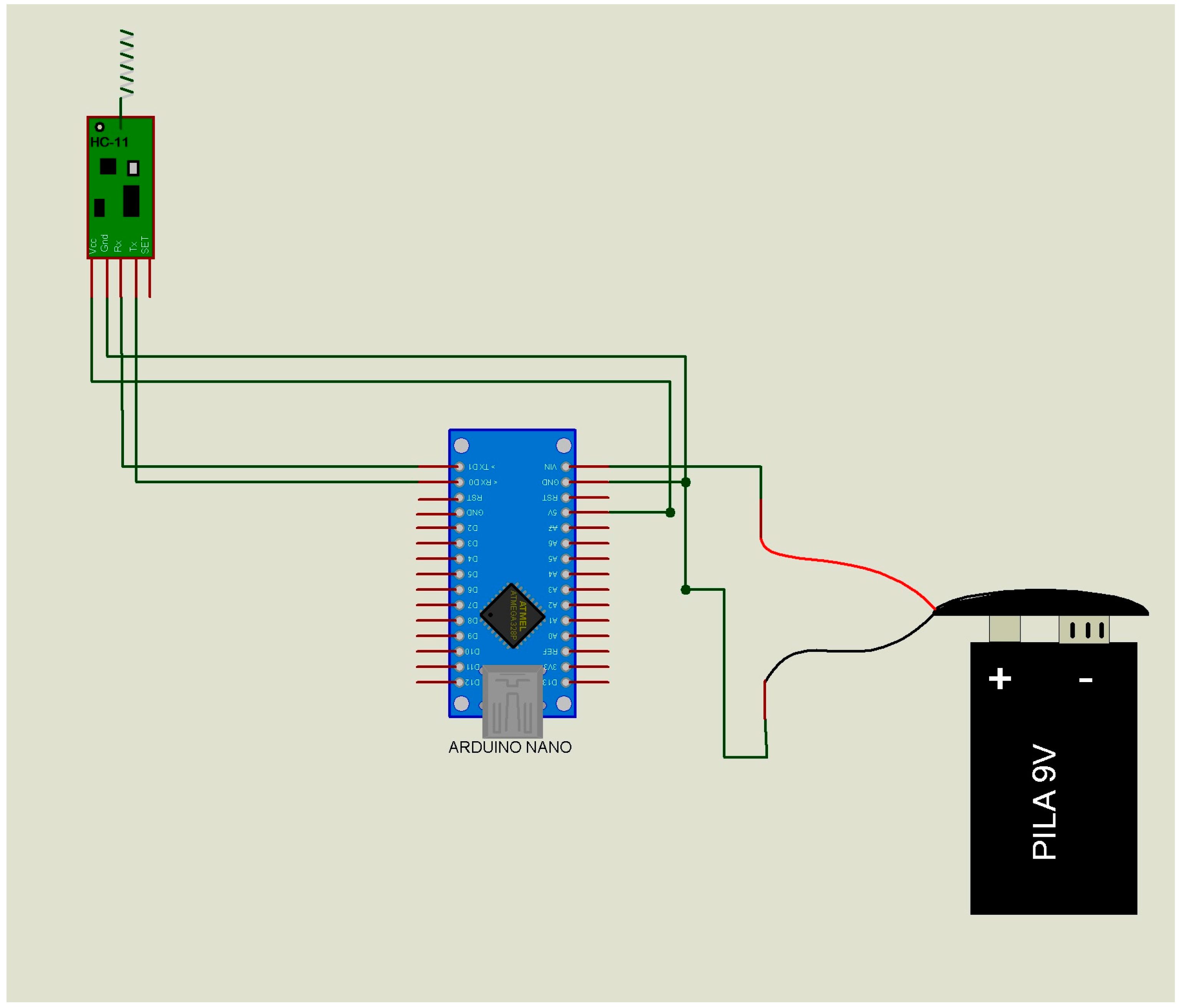
- The data transmitter module or “slave” (Figure 2) has only one function, namely to send the ID of the subject to the data receiver module or “master” (Table 1 (A,B)). When the “master” receives this ID, it emits a confirmation. If the ID does not match, there will be no message confirmation. This passive way of communicating will substantially reduce the power consumption of the “slave” device of the end users (children and adults).
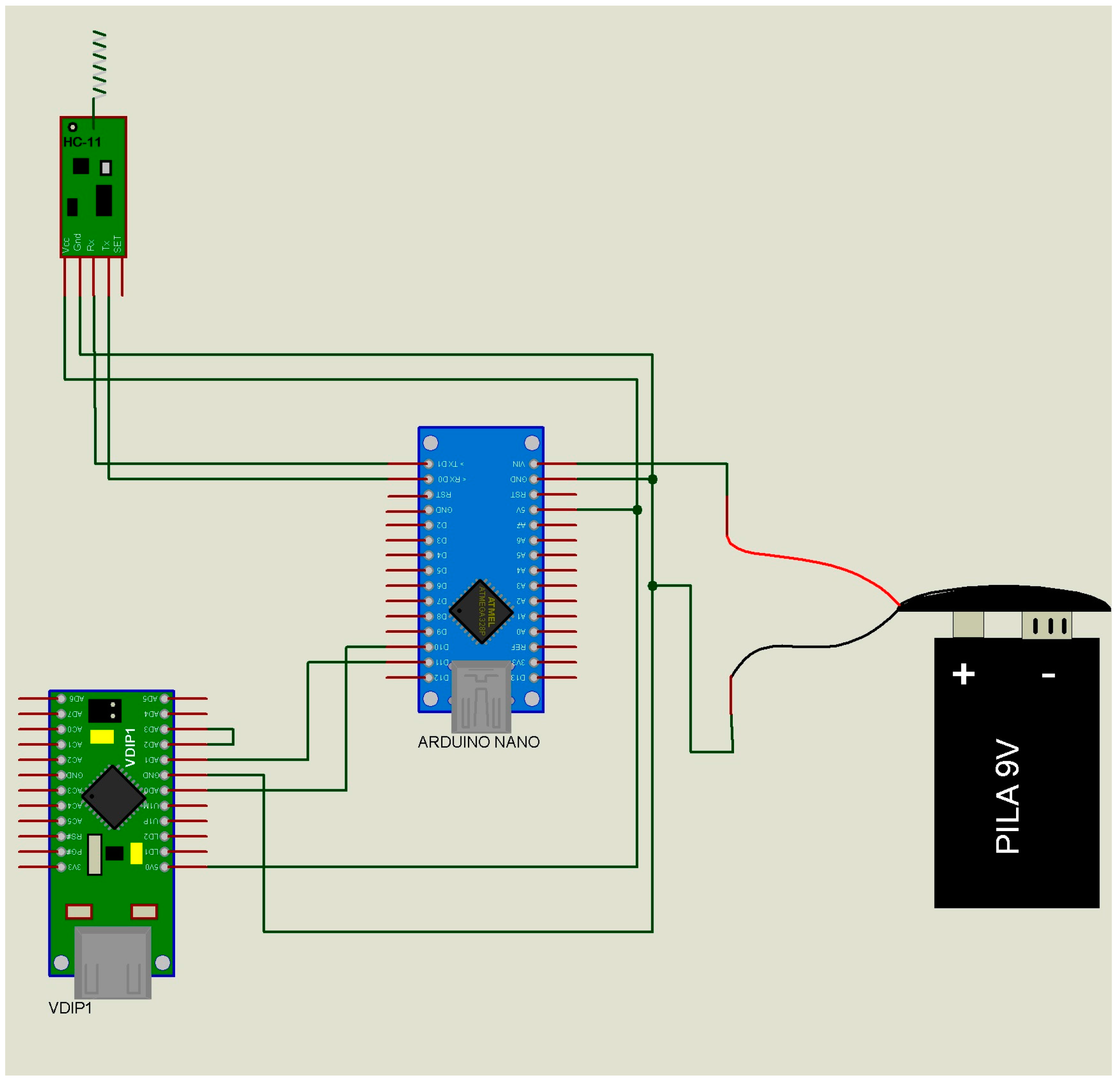
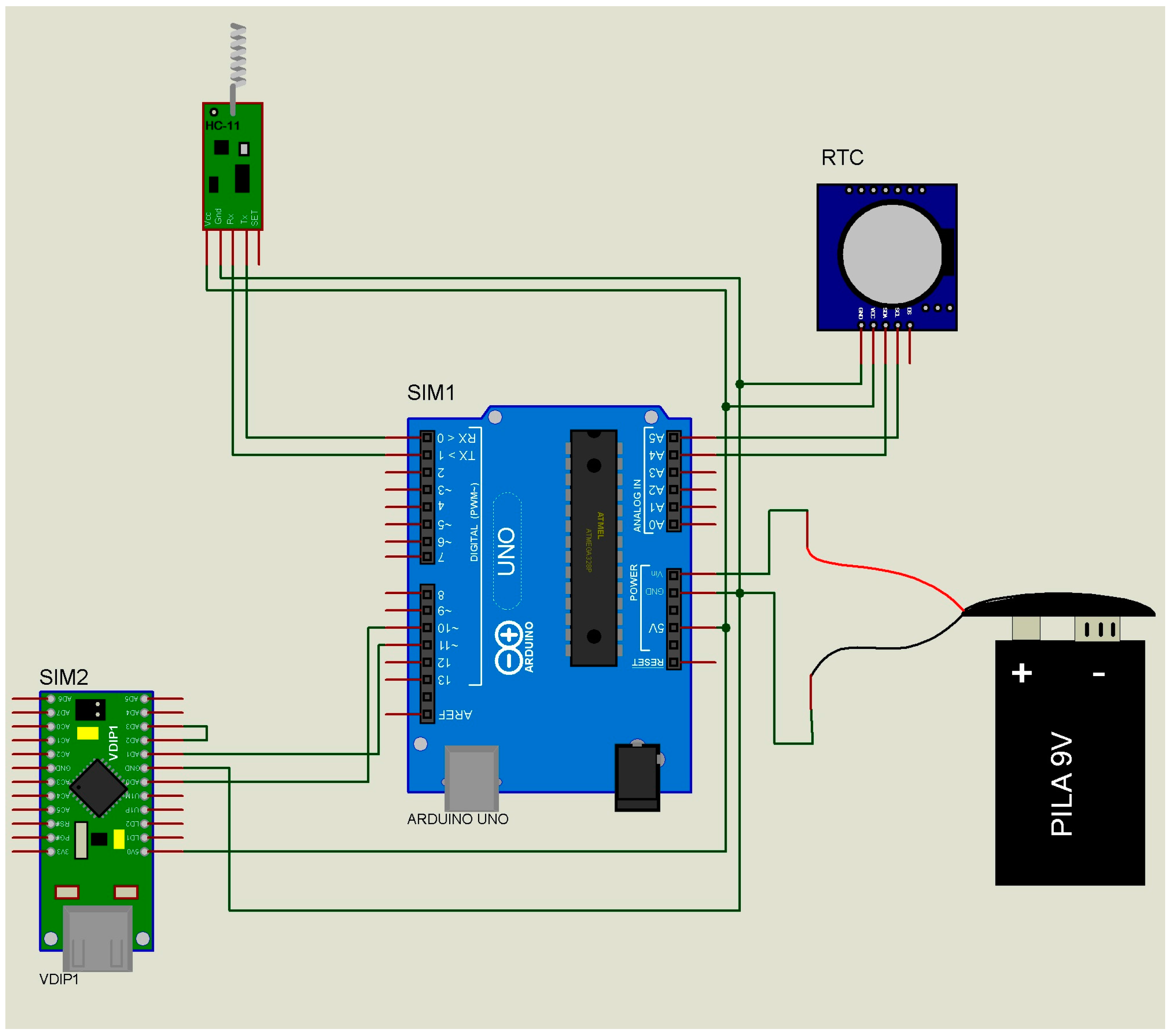
- The data receiver module or “master” (Figure 3) performs three functions: (i) It receives the list of the IDs to be located from the “supervisor”; (ii) It sends the ID searched to all the “slaves” (Table 2 (A)); (iii) in the case of successfully identifying a “slave” (Table 2 (B,C)), it sends to the data “supervisor” module the “slave” ID, the “master” ID, and the recording date and time (year, month, day, hour, minute) (Table 3). This is the device that has to be installed at fixed sites and whose geographical address is transmitted to the “slaves”.
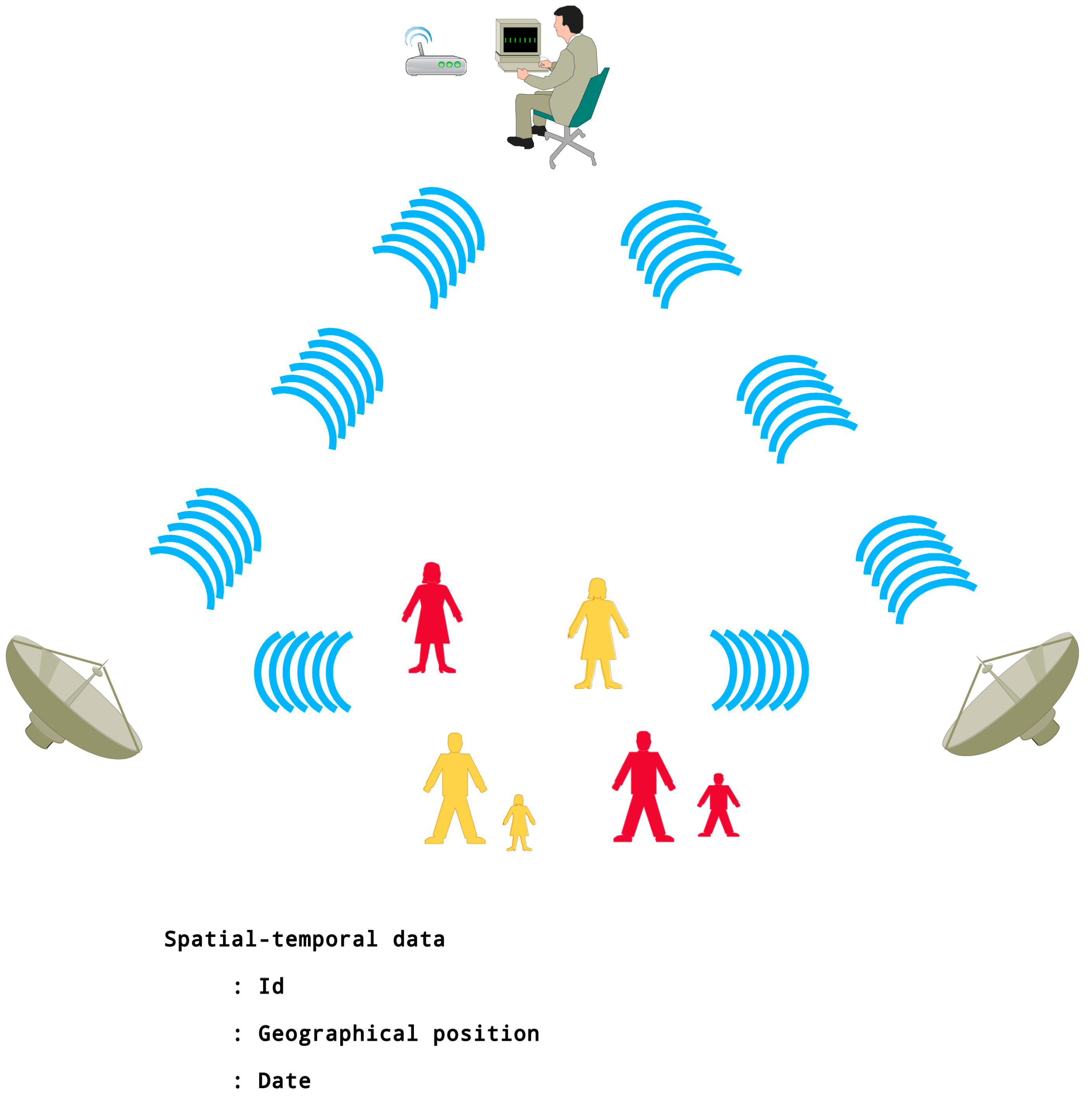
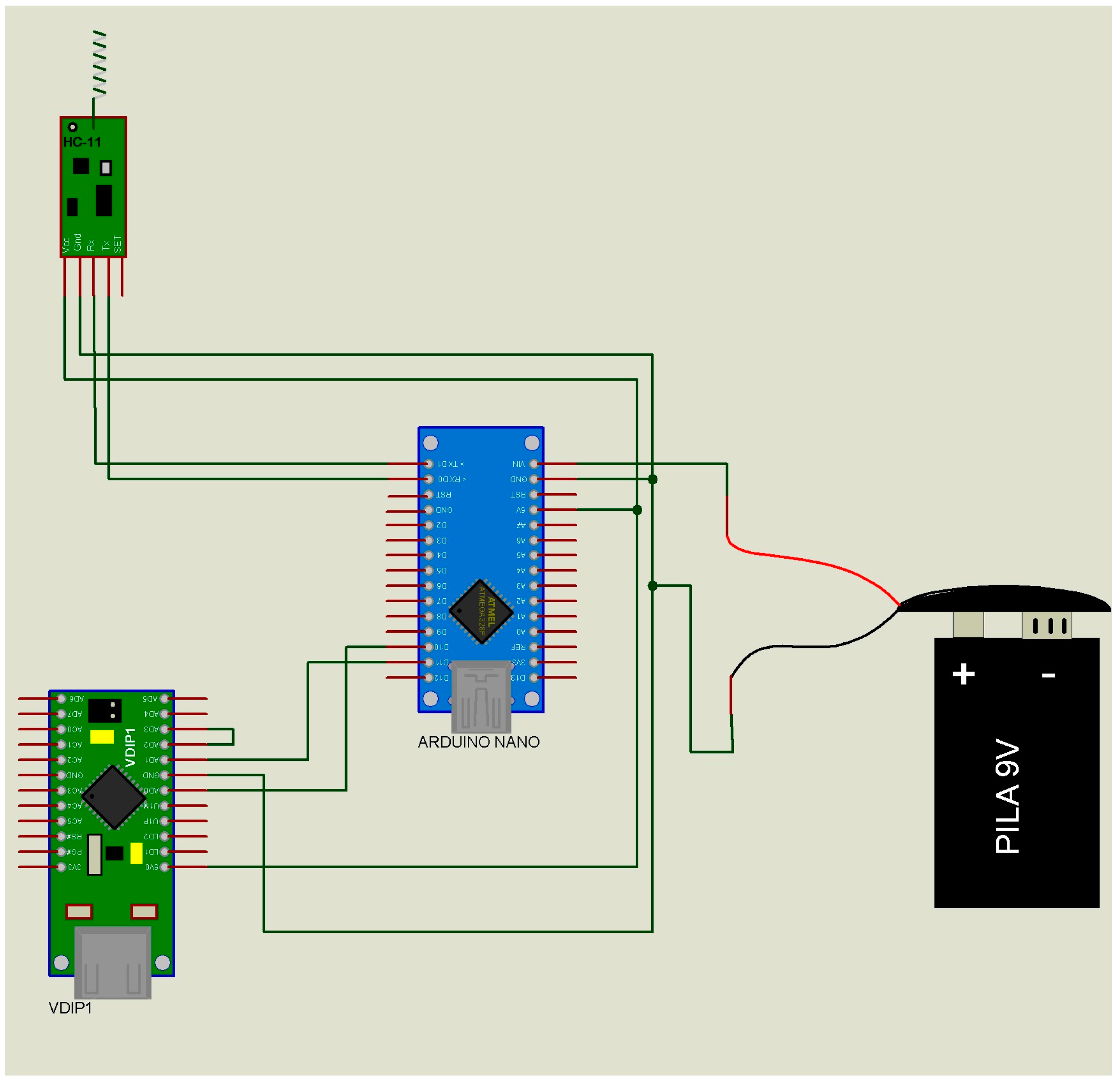
- The data “supervisor” module (Figure 4) has three functions: (i) It updates the list of IDs that have to be located (Table 4 (A)); (ii) It sends this list of IDs to the “masters” (Table 2 (C)); and (iii) It receives the list of the located IDs from the “masters” (Table 4 (B)). This device updates the list of missing individuals from “masters”, and has the list of individuals located by the “slaves.”
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- CAPEA Centro de Atención a Personas Extraviadas y Ausentes. Available online: http://www.pgj.cdmx.gob.mx/nuestros-servicios/en-linea/mp-virtual/capea-c entro-de-atencion-personas-extraviadas-y-ausentes (accessed on 23 December 2016).
- Clarke, J.N. The case of the missing person: Alzheimer’s disease in mass print magazines 1991–2001. Health Commun. 2006, 19, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.; Muschert, G.W.; Kinney, J.; Robbins, E.; Petonito, G.; Manning, L.; Brown, J.S. Silver alerts and the problem of missing adults with dementia. Gerontologist 2010, 50, 149–157. [Google Scholar] [CrossRef]
- Rowe, A.R.; Vandeveer, S.S.; Greenblum, C.A.; List, C.N.; Fernandez, R.M.; Mixson, N.E.; Hyo, C.A. Persons with dementia missing in the community: Is it wandering or something unique? BMC Geriatr. 2011, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Polanco, C.; Islas Vazquez, I.; Castañón González, J.A.; Buhse, T.; Arias-Estrada, M. Electronic Devices That Identify Individuals with Fever in Crowded Places: A Prototype. Micromachines 2017, 8, 202. [Google Scholar] [CrossRef]
- Brand, O. Microsensor integration into systems-on-chip. Proc. IEEE 2006, 94, 94–1160. [Google Scholar] [CrossRef]
- Buratti, C.; Conti, A.; Dardari, D.; Verdone, R. An Overview on Wireless Sensor Networks Technology and Evolution. Sensors 2009, 9, 6869–6896. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Lee, Y.D.; Chung, W.Y.; Myllyla, R. Vital sign monitoring system with life emergency event detection using wireless sensor network. In Proceedings of the Conference on Sensors, Daegu, Korea, 22–25 October 2006. [Google Scholar]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. NeuroEng. Rehabil. 2012, 9, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghavendra, C.; Sivalingam, K.; Znati, T. Wireless Sensor Networks; Springer: New York, NY, USA, 2004. [Google Scholar]
- Patel, V.; Kleinman, A. Poverty and common mental disorders in developing countries. Bull. World Health Organ. 2003, 81, 609–615. [Google Scholar] [PubMed]
- Silberberg, D.; Anand, P.; Michels, K.; Kalaria, R. Brain and other nervous system disorders across the lifespan—Global challenges and opportunities. Nature 2015, 527, S151–S154. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Ortiz, A.L.; Acosta-Castillo, I.; Prince, M.J. Epidemiology of dementias and Alzheimer’s disease Arch. Med. Res. 2012, 43, 600–608. [Google Scholar]
- Bonato, P. Advances in wearable technology and its medical applications. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2010, 2010, 2021–2024. [Google Scholar] [PubMed]
- D’Onofrio, G.; Sancarlo, D.; Ricciardi, F.; Panza, F.; Seripa, D.; Carvallo, F.; Giuliani, F.; Greco, A. Information and communication technologies for the activities of daily living in older patients with dementia: A systematic review. J. Alzheimers Dis. 2017, 57, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Williamson, B.; Aplin, T.; de Jonge, D.; Goyne, M. Tracking down a solution: Exploring the acceptability and value of wearable GPS devices for older persons, individuals with a disability and their support persons. Disabil. Rehabil. Assist. Technol. 2017, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Polanco, C.; Buhse, T.; Samaniego, J.L.; Castañón González, J.A. Detection of respiratory disease outbreaks by CUSUM-based Overcrowd-Severe Respiratory Disease index model. Comput. Math. Methods Med. 2013, 2013, 213206. [Google Scholar] [CrossRef] [PubMed]
- Polanco, C.; Castañón-González, J.A.; Buhse, T.; Samaniego-Mendoza, J.L.; Arreguín-Nava, R.; Villanueva-Martínez, S. Índice de Saturación Modificado en el Servicio de Urgencias Médicas. Gac. Med. Mex. 2013, 149, 417–424. [Google Scholar]
- Sharp, P.; Jacks, T.; Hockfield, S. Capitalizing on convergence for health care. Science 2016, 352, 1522–1523. [Google Scholar] [CrossRef] [PubMed]
- Navarro, V.; Parker, R.; White, K.L. A Stochastic and Deterministic Model of Medical Care Utilization. Health Serv. Res. 1970, 5, 342–357. [Google Scholar] [PubMed]
- Polanco, C.; Arias Estrada, M.; Castañón González, J.A. Zika virus disease: Electronic devices (Letter to the Editor) The next steps on Zika. Nature 2016, 530, 5. [Google Scholar] [CrossRef]
- Polanco, C.; Buhse, T.; Samaniego, J.L.; Castañón González, J.A. Detection of selective antibacterial peptides by the Polarity Profile method. Acta Biochim. Pol. 2013, 60, 183–199. [Google Scholar] [PubMed]
- Polanco, C.; Castañón-González, J.A. Cross-sectional bioinformatics analysis on proteins associated to the Ebola virus. (Letter to the Editor) Hantel, A.; Olusola-Olopade, C. Drug and Vaccine Access in the Ebola Epidemic: Advising Caution in Compassionate Use. Ann. Intern. Med. 2015, 162, 141–142. Ann. Intern. Med. 2014. [Google Scholar] [CrossRef]
- Polanco, C.; Castañón-González, J.A.; Samaniego, J.L.; Buhse, T. A novel Mathematical-Computational approach that helps manufacturing new drugs. (Letter to the Editor) Howard, S.J.; Hopwood, S.; Davies, S.C. Antimicrobial Resistance: A Global Challenge. Sci. Transl. Med. 2014, 6, 236ed10. Sci. Transl. Med. 2014. [Google Scholar] [CrossRef]
- Polanco, C.; Buhse, T.; Samaniego, J.L.; Castañón-González, J.A. Precision medicine and portable embedded system devices. (Letter to the Editor) Schork, N.J. Personalized medicine: Time for one-person trials. Nature 2015, 50, 609–611. [Google Scholar] [CrossRef]
- Polanco, C.; Buhse, T.; Vizcaíno, G.; Levy Picciotto, J. The polar profile of ancient proteins: A computational extrapolation from prebiotics to paleobiochemistry. Acta Biochim. Pol. 2017, 64, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Bourzac, K. Millimeter-Scale Computers: Now with Deep-Learning Neural Networks on Board. IEEE Spectrum. 10 February 2017. Available online: http://spectrum.ieee.org/techtalk/robotics/artificialintelligence/millimeterscale-computers-now-with-deep-learning-neural-networks-on-board (accessed on 18 April 2017).
- Atmel. Atmel SoC Solutions for Wearables. Available online: http://www.atmel.com/applications/wearables/ (accessed on 18 April 2017).
- Microchip. Wearable Activity Monitors. Available online: http://www.microchip.com/design-centers/medical/applications/wearable-activity-monitors (accessed on 18 April 2017).
- NXP. Healthcare and Medical Applications with NXP Microelectronics Technology, Some Use Cases and Reference Designs. Available online: http://www.nxp.com/applications/solutions-for-the-iot-and-adas/internet-of-things/smart-things/healthcare-medical:HEALTHCARE-MEDICAL (accessed on 18 April 2017).
- Intel. Intel Curie: A Computer the Size of a Button. Available online: http://www.intel.com/content/www/us/en/wearables/wearable-soc.html (accessed on 18 April 2017).
- Glukhovsky, A. Wireless capsule endoscopy. Sens. Rev. 2003, 23, 128–133. [Google Scholar] [CrossRef]
- El-Kady, M.; Kaner, R. How a Microscopic Supercapacitor Will Supercharge Mobile Electronics. IEEE Spèctrum. 28 September 2015. Available online: http://spectrum.ieee.org/semiconductors/materials/how-a-microscopic-supercapacitor-will-supercharge-mobile-electronics (accessed on 18 April 2017).
- Cobos-Sánchez, C.; Glover, P.; Power, H.; Bowtell, R. Calculation of the electric field resulting from human body rotation in a magnetic field. Phys. Med. Biol. 2012, 57, 4739–4753. [Google Scholar] [CrossRef] [PubMed]
- Mateen, H.; Basar, R.; Ahmed, A.U.; Ahmad, M.Y. Localization of Wireless Capsule Endoscope: A Systematic Review. IEEE Sens. J. 2017, 17, 17–1197. [Google Scholar] [CrossRef]
- Proa-Coronado, S. Fabricación de Nanobiosensores Tipo FET Basados en Grafeno. Master’s Thesis, Centro de Investigación en Computación-IPN, Mexico City, Mexico, 4 March 2016. [Google Scholar]
- Dubey, A.; Dave, S.; Lakhani, M.; Sharma, A. Applications of graphene for communication, electronics and medical fields: A review. In Proceedings of the International Conference on Electrical, Electronics, and Optimization Techniques (ICEEOT), Chennai, India, 3–5 March 2016; pp. 2435–2439. [Google Scholar]
- Sajal, S.; Braaten, B.D.; Tolstedt, T.; Asif, S.; Schroeder, M.J. Design of a conformal monopole antenna on a paper substrate using the properties of graphene-based conductors. Microw. Opt. Technol. Lett. 2017, 59, 1229–1474. [Google Scholar] [CrossRef]
- Zhang, H.; Jiang, Y.; Wang, J.; Cao, W.; Gao, X.; Yu, X.; Wang, L. A broadband terahertz antenna using graphene. In Proceedings of the 11th Antennas, Propagation and EM Theory (ISAPE) International Symposium, Guilin, China, 18–21 October 2016; pp. 149–152. [Google Scholar]
- Huang, X.; Leng, T.; Zhu, M.; Zhang, X.; Chen, J.; Chang, K.; Hu, Z. Highly Flexible and Conductive Printed Graphene for Wireless Wearable Communications Applications. Sci. Rep. 2015, 5, 18298. [Google Scholar] [CrossRef] [PubMed]
- Mansor, M.M.; Rahim, S.K.A.; Hashim, U. A 2.45 GHz wearable antenna using conductive graphene and polymer substrate. Int. Symp. Technol. Manag. Emerg. Technol. 2014, 29–32. [Google Scholar] [CrossRef]
- Ludwig, J.A.; Weinstein, J.N. Biomarkers in cancer staging, prognosis and treatment selection. Nat. Rev. Cancer 2005, 5, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.M.; Thaxton, C.S.; Mirkin, C.A. Nanoparticle-based bio-bar codes for the ultrasensitive detection of proteins. Science 2003, 301, 1884–1886. [Google Scholar] [CrossRef] [PubMed]
- Rifai, N.; Gillette, M.A.; Carr, S.A. Protein biomarker discovery and validation: The long and uncertain path to clinical utility. Nat. Biotechnol. 2006, 24, 971–983. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Start | Master ID | Slave ID | DD | MO | YY | HH | MM | DF | End |
|---|---|---|---|---|---|---|---|---|---|
| (A) | |||||||||
| @ | 1 | A | 29 | 06 | 16 | 22 | 19 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 20 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 21 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 22 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 23 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 24 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 25 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 26 | ! | & |
| (B) | |||||||||
| @ | 2 | B | 29 | 06 | 16 | 22 | 19 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 20 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 21 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 22 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 23 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 24 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 25 | ! | & |
| @ | 2 | B | 29 | 06 | 16 | 22 | 26 | ! | & |
| Start | ID Master | ID Slave | DD | MO | YY | HH | MM | DF | End |
|---|---|---|---|---|---|---|---|---|---|
| (A) | |||||||||
| @ | A | ! | & | ||||||
| (B) | |||||||||
| @ | 1 | A | 29 | 06 | 16 | 22 | 19 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 20 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 21 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 22 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 23 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 24 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 25 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 26 | ! | & |
| (C) | |||||||||
| No data | |||||||||
| Field | Symbol | Description |
|---|---|---|
| Identificator slave | ID slave | Alphabetic code that identifies the “slave” data transmitter module. This code has the personal information and the address of the user. |
| Identificator master | ID master | Numerical code that identifies the “master” data receiver module. This code has the physical address where it was located. |
| Day | DD | The day the “slave” data transmitter module sends a confirmation to the “master” data receiver module. |
| Month | MO | The month the “slave” data transmitter module sends a confirmation to the “master” data receiver module. |
| Year | YY | The year the “slave” data transmitter module sends a confirmation to the “master” data receiver module. |
| Hour | HH | The hour the “slave” data transmitter module sends a confirmation to the “master” data receiver module. |
| Minute | MM | The minute the “slave” data transmitter module sends a confirmation to the “master” data receiver module. |
| Start | Master ID | Slave ID | DD | MO | YY | HH | MM | DF | End |
|---|---|---|---|---|---|---|---|---|---|
| (A) | |||||||||
| @ | 1 | A | 29 | 06 | 16 | 22 | 19 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 20 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 21 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 22 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 23 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 24 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 25 | ! | & |
| @ | 1 | A | 29 | 06 | 16 | 22 | 26 | ! | & |
| (B) | |||||||||
| @ | A | ! | & | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polanco, C.; Vazquez, I.I.; Martinez-Rivas, A.; Arias-Estrada, M.; Buhse, T.; Calva, J.J.; Aguilar Salinas, C.; Pimentel Hernández, C.; Uversky, V.N. Real Time Monitoring of Children, and Adults with Mental Disabilities Using a Low-Cost Non-Invasive Electronic Device. Micromachines 2017, 8, 292. https://doi.org/10.3390/mi8100292
Polanco C, Vazquez II, Martinez-Rivas A, Arias-Estrada M, Buhse T, Calva JJ, Aguilar Salinas C, Pimentel Hernández C, Uversky VN. Real Time Monitoring of Children, and Adults with Mental Disabilities Using a Low-Cost Non-Invasive Electronic Device. Micromachines. 2017; 8(10):292. https://doi.org/10.3390/mi8100292
Chicago/Turabian StylePolanco, Carlos, Ignacio Islas Vazquez, Adrian Martinez-Rivas, Miguel Arias-Estrada, Thomas Buhse, Juan J. Calva, Carlos Aguilar Salinas, Claudia Pimentel Hernández, and Vladimir N. Uversky. 2017. "Real Time Monitoring of Children, and Adults with Mental Disabilities Using a Low-Cost Non-Invasive Electronic Device" Micromachines 8, no. 10: 292. https://doi.org/10.3390/mi8100292