The Prevalence of CD146 Expression in Breast Cancer Subtypes and Its Relation to Outcome

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. CD146 Expression and the Relationship with Patient and Tumor Characteristics
2.2. CD146 and EpCAM Expression in the Diverse Breast Cancer Subtypes
2.3. Relationship of CD146 Expression with Expression of EMT-Related Genes
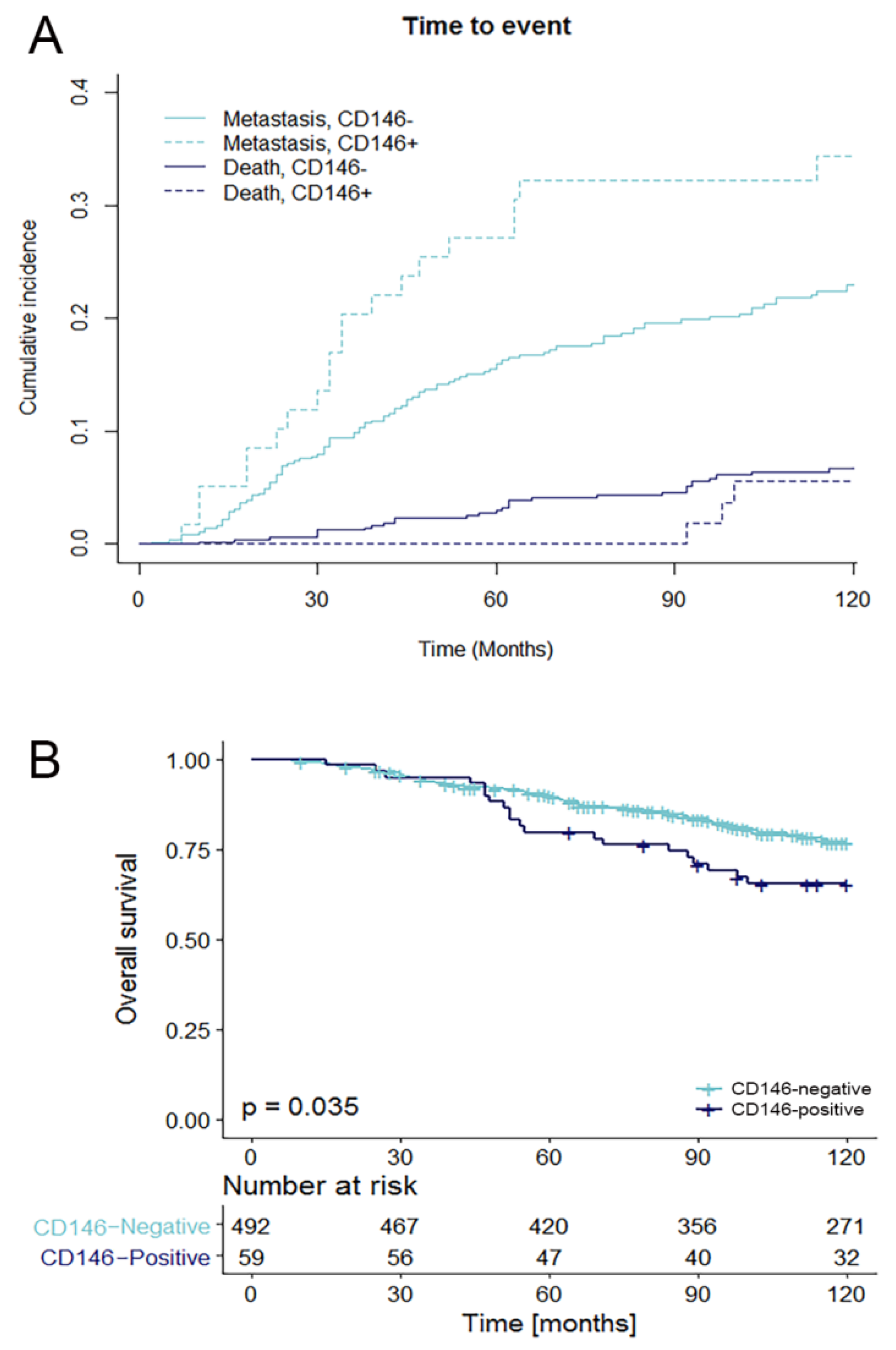
2.4. Relationship of CD146 Expression with Prognosis
2.5. CD146 Status and Outcome to Tamoxifen Treatment
3. Discussion
4. Materials and Methods
4.1. Patient and Tissue Samples
4.2. Tissue Microarray and Immunohistochemistry
4.3. Epithelial-to-Mesenchymal Transition
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lehmann, J.M.; Riethmuller, G.; Johnson, J.P. MUC18, a marker of tumor progression in human melanoma, shows sequence similarity to the neural cell adhesion molecules of the immunoglobulin superfamily. Proc. Natl. Acad. Sci. USA 1989, 86, 9891–9895. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Zhang, P.; Wu, Z.; Xue, P.; Lu, D.; Ye, Z.; Zhang, X.; Huang, Z.; Feng, J.; Song, L.; et al. Quantitative proteomics reveals ER-alpha involvement in CD146-induced epithelial-mesenchymal transition in breast cancer cells. J. Proteom. 2014, 103, 153–169. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Li, W.; Lu, D.; Wu, Z.; Duan, H.; Luo, Y.; Feng, J.; Yang, D.; Fu, L.; Yan, X. CD146, an epithelial-mesenchymal transition inducer, is associated with triple-negative breast cancer. Proc. Natl. Acad. Sci. USA 2012, 109, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Imbert, A.M.; Garulli, C.; Choquet, E.; Koubi, M.; Aurrand-Lions, M.; Chabannon, C. CD146 expression in human breast cancer cell lines induces phenotypic and functional changes observed in epithelial to mesenchymal transition. PLoS ONE 2012, 7, e43752. [Google Scholar] [CrossRef] [PubMed]
- Jang, M.H.; Kim, H.J.; Kim, E.J.; Chung, Y.R.; Park, S.Y. Expression of epithelial-mesenchymal transition-related markers in triple-negative breast cancer: ZEB1 as a potential biomarker for poor clinical outcome. Hum. Pathol. 2015, 46, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Micalizzi, D.S.; Ford, H.L. Epithelial-mesenchymal transition in development and cancer. Future Oncol. 2009, 5, 1129–1143. [Google Scholar] [CrossRef] [PubMed]
- Mani, S.A.; Guo, W.; Liao, M.J.; Eaton, E.N.; Ayyanan, A.; Zhou, A.Y.; Brooks, M.; Reinhard, F.; Zhang, C.C.; Shipitsin, M.; et al. The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell 2008, 133, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Hyun, K.A.; Koo, G.B.; Han, H.; Sohn, J.; Choi, W.; Kim, S.I.; Jung, H.I.; Kim, Y.S. Epithelial-to-mesenchymal transition leads to loss of EpCAM and different physical properties in circulating tumor cells from metastatic breast cancer. Oncotarget 2016, 7, 24677–24687. [Google Scholar] [CrossRef] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development and disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Aktas, B.; Tewes, M.; Fehm, T.; Hauch, S.; Kimmig, R.; Kasimir-Bauer, S. Stem cell and epithelial-mesenchymal transition markers are frequently overexpressed in circulating tumor cells of metastatic breast cancer patients. Breast Cancer Res. 2009, 11, R46. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Bardia, A.; Wittner, B.S.; Stott, S.L.; Smas, M.E.; Ting, D.T.; Isakoff, S.J.; Ciciliano, J.C.; Wells, M.N.; Shah, A.M.; et al. Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science (New York) 2013, 339, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.K.; Zeng, D.; Xiao, Y.S.; Wu, Y.; Ouyang, Y.X.; Chen, M.; Li, Y.C.; Lin, H.Y.; Wei, X.L.; Zhang, Y.Q.; et al. MCAM/CD146 promotes tamoxifen resistance in breast cancer cells through induction of epithelial-mesenchymal transition, decreased ERα expression and AKT activation. Cancer Lett. 2017, 386, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Mostert, B.; Kraan, J.; Bolt-de Vries, J.; van der Spoel, P.; Sieuwerts, A.M.; Schutte, M.; Timmermans, A.M.; Foekens, R.; Martens, J.W.; Gratama, J.W.; et al. Detection of circulating tumor cells in breast cancer may improve through enrichment with anti-CD146. Breast Cancer Res. Treat. 2011, 127, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Sieuwerts, A.M.; Kraan, J.; Bolt, J.; van der Spoel, P.; Elstrodt, F.; Schutte, M.; Martens, J.W.; Gratama, J.W.; Sleijfer, S.; Foekens, J.A. Anti-epithelial cell adhesion molecule antibodies and the detection of circulating normal-like breast tumor cells. J. Natl. Cancer Inst. 2009, 101, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.J.; Fu, P.; Chiang, C.F.; Huss, W.J.; Greenberg, N.M.; Wu, M.W. Increased expression of MUC18 correlates with the metastatic progression of mouse prostate adenocarcinoma in the TRAMP model. J. Urol. 2005, 173, 1778–1783. [Google Scholar] [CrossRef] [PubMed]
- Aldovini, D.; Demichelis, F.; Doglioni, C.; Di Vizio, D.; Galligioni, E.; Brugnara, S.; Zeni, B.; Griso, C.; Pegoraro, C.; Zannoni, M.; et al. M-CAM expression as marker of poor prognosis in epithelial ovarian cancer. Int. J. Cancer 2006, 119, 1920–1926. [Google Scholar] [CrossRef] [PubMed]
- Shih, I.M.; Elder, D.E.; Hsu, M.Y.; Herlyn, M. Regulation of Mel-CAM/MUC18 expression on melanocytes of different stages of tumor progression by normal keratinocytes. Am. J. Pathol. 1994, 145, 837–845. [Google Scholar] [PubMed]
- Jiang, G.; Zhang, L.; Zhu, Q.; Bai, D.; Zhang, C.; Wang, X. CD146 promotes metastasis and predicts poor prognosis of hepatocellular carcinoma. J. Exp. Clin. Cancer Res. 2016, 35, 38. [Google Scholar] [CrossRef] [PubMed]
- Zabouo, G.; Imbert, A.M.; Jacquemier, J.; Finetti, P.; Moreau, T.; Esterni, B.; Birnbaum, D.; Bertucci, F.; Chabannon, C. CD146 expression is associated with a poor prognosis in human breast tumors and with enhanced motility in breast cancer cell lines. Breast Cancer Res. 2009, 11, R1. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.; Dales, J.P.; Charafe-Jauffret, E.; Carpentier-Meunier, S.; Andrac-Meyer, L.; Jacquemier, J.; Andonian, C.; Lavaut, M.N.; Allasia, C.; Bonnier, P.; et al. Poor prognosis in breast carcinomas correlates with increased expression of targetable CD146 and c-Met and with proteomic basal-like phenotype. Hum. Pathol. 2007, 38, 830–841. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Kalabis, J.; Xu, X.; Meier, F.; Oka, M.; Bogenrieder, T.; Herlyn, M. Reciprocal regulation of MelCAM and AKT in human melanoma. Oncogene 2003, 22, 6891–6899. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.S.; West, K.; Streicher, S.; Dennis, P.A. Constitutive and inducible AKT activity promotes resistance to chemotherapy, trastuzumab, or tamoxifen in breast cancer cells. Mol. Cancer Ther. 2002, 1, 707–717. [Google Scholar] [PubMed]
- The Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar]
- Curtis, C.; Shah, S.P.; Chin, S.F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Pareja, F.; Geyer, F.C.; Marchio, C.; Burke, K.A.; Weigelt, B.; Reis-Filho, J.S. Triple-negative breast cancer: The importance of molecular and histologic subtyping, and recognition of low-grade variants. NPJ Breast Cancer 2016, 2, 16036. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, J.; Wang, Z.; Lu, D.; Feng, J.; Yang, D.; Chen, X.; Yan, X. CD146 is a potential marker for the diagnosis of malignancy in cervical and endometrial cancer. Oncol. Lett. 2013, 5, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wu, Z.; Li, J.; Yang, X.; Wang, Y.; Yu, Y.; Ye, J.; Xu, C.; Qin, W.; Zhang, Z. MCAM is a novel metastasis marker and regulates spreading, apoptosis and invasion of ovarian cancer cells. Tumour Biol. 2012, 33, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Domagala, W.; Markiewski, M.; Harezga, B.; Dukowicz, A.; Osborn, M. Prognostic significance of tumor cell proliferation rate as determined by the MIB-1 antibody in breast carcinoma: Its relationship with vimentin and p53 protein. Clin. Cancer Res. 1996, 2, 147–154. [Google Scholar] [PubMed]
- Inic, Z.; Zegarac, M.; Inic, M.; Markovic, I.; Kozomara, Z.; Djurisic, I.; Inic, I.; Pupic, G.; Jancic, S. Difference between luminal A and luminal B subtypes according to Ki-67, tumor size, and progesterone receptor negativity providing prognostic information. Clin. Med. Insights Oncol. 2014, 8, 107–111. [Google Scholar] [CrossRef] [PubMed]
- McCall, M.N.; Bolstad, B.M.; Irizarry, R.A. Frozen robust multiarray analysis (fRMA). Biostatistics 2010, 11, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Huang da, W.; Sherman, B.T.; Lempicki, R.A. Bioinformatics enrichment tools: Paths toward the comprehensive functional analysis of large gene lists. Nucleic Acids Res. 2009, 37, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Huang da, W.; Sherman, B.T.; Lempicki, R.A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 2009, 4, 44–57. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | N | CD146-Negative | CD146-Positive | p-Value |
|---|---|---|---|---|
| Age | p < 0.001 * | |||
| ≤40 | 127 | 96 | 31 | |
| 41–55 | 431 | 383 | 48 | |
| ≥55 | 467 | 433 | 34 | |
| T-Stage | p = 0.016 | |||
| T1 | 602 | 547 | 55 | |
| T2–T4 | 408 | 351 | 57 | |
| N-Stage | p = 0.577 * | |||
| N0 | 576 | 511 | 65 | |
| N1 | 347 | 308 | 39 | |
| N2 | 102 | 93 | 9 | |
| Menopausal status | p < 0.001 | |||
| Pre-menopausal | 477 | 405 | 72 | |
| Post-menopausal | 548 | 507 | 41 | |
| Tumor grade | p < 0.001 * | |||
| Grade I | 211 | 205 | 6 | |
| Grade II | 473 | 451 | 22 | |
| Grade III | 341 | 256 | 85 | |
| Ki-67 status | p < 0.001 | |||
| Low (<10%) | 621 | 595 | 26 | |
| High (≥10%) | 404 | 317 | 87 | |
| ER status | p < 0.001 | |||
| Positive | 861 | 831 | 30 | |
| Negative | 164 | 81 | 83 | |
| PR status | p < 0.001 | |||
| Positive | 657 | 639 | 18 | |
| Negative | 368 | 273 | 95 | |
| HER2 status | p = 0.200 | |||
| Positive | 119 | 110 | 9 | |
| Negative | 906 | 802 | 104 |
| CD146 Expression | |||
|---|---|---|---|
| Tumor types | Negative N (%) | Positive N (%) | p-Value |
| All tumors (n = 1025) | 912 (89.0) | 113 (11.0) | |
| Histological subtype | p < 0.001 | ||
| Invasive ductal carcinoma | 751 (88.5) | 98 (11.5) | |
| Invasive lobular carcinoma | 117 (99.2) | 1 (0.8) | |
| Medullary | 12 (52.2) | 11 (47.8) | |
| Mucinous | 18 (100) | 0 (0.0) | |
| Tubular | 11 (91.7) | 1 (8.3) | |
| Papillary | 3 (60.0) | 2 (40.0) | |
| Molecular subtype | p < 0.001 | ||
| Luminal A | 437 (98.0) | 9 (2.0) | |
| Luminal B HER2-negative | 322 (94.4) | 19 (5.6) | |
| Luminal B HER2-positive | 72 (97.3) | 2 (2.7) | |
| HER2-positive | 38 (84.4) | 7 (15.6) | |
| Triple negative | 43 (36.1) | 76 (63.9) | |
| Characteristics | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | ||||||
| 40–55 vs. <40 | 0.69 | 0.41–1.17 | 0.170 | |||
| >55 vs. <40 | 0.48 | 0.28–0.81 | 0.006 | 0.63 | 0.35–1.15 | 0.130 |
| T-stage | ||||||
| T2–T4 vs. T1 | 1.94 | 1.36–2.76 | <0.001 | 1.77 | 1.22–2.59 | 0.003 |
| Tumor grade | ||||||
| II vs. I | 2.44 | 1.38–4.30 | 0.002 | |||
| III vs. I | 2.94 | 1.64–5.27 | <0.001 | |||
| ER | ||||||
| Pos vs. neg | 0.74 | 0.47–1.18 | 0.210 | |||
| PR | ||||||
| Pos vs. neg | 0.85 | 0.59–1.23 | 0.390 | 1.29 | 0.83–1.99 | 0.260 |
| HER2 | ||||||
| Pos vs. neg | 2.92 | 1.92–4.46 | <0.001 | 2.64 | 1.65–4.22 | <0.001 |
| Ki-67 | ||||||
| Pos vs. neg | 1.82 | 1.28–2.59 | <0.001 | 1.37 | 0.92–2.05 | 0.120 |
| Additions to the base model | ||||||
| CD146 | ||||||
| Pos vs. neg | 1.77 | 1.09–2.87 | 0.020 | 1.51 | 0.79–2.87 | 0.210 |
| Characteristics | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | ||||||
| 40–55 vs. <40 | 0.68 | 0.39–1.18 | 0.170 | |||
| >55 vs. <40 | 0.76 | 0.44–1.30 | 0.311 | |||
| T-stage | ||||||
| T2–T4 vs. T1 | 1.98 | 1.39–2.83 | <0.001 | 1.86 | 1.30–2.66 | <0.001 |
| Tumor grade | ||||||
| II vs. I | 2.06 | 1.19–3.59 | 0.010 | |||
| III vs. I | 2.51 | 1.43–4.41 | 0.001 | |||
| ER | ||||||
| Pos vs. neg | 0.63 | 0.41–0.97 | 0.035 | |||
| PR | ||||||
| Pos vs. neg | 0.63 | 0.44–0.90 | 0.011 | |||
| HER2 | ||||||
| Pos vs. neg | 2.55 | 1.68–3.87 | <0.001 | 2.15 | 1.39–3.31 | <0.001 |
| Ki-67 | ||||||
| Pos vs. neg | 1.71 | 1.20–2.43 | 0.003 | |||
| Additions to the base model | ||||||
| CD146 | ||||||
| Pos vs. neg | 1.67 | 1.03–2.69 | 0.037 | 1.42 | 0.84–2.38 | 0.191 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Kruijff, I.E.; Timmermans, A.M.; Den Bakker, M.A.; Trapman-Jansen, A.M.A.C.; Foekens, R.; Meijer-Van Gelder, M.E.; Oomen-de Hoop, E.; Smid, M.; Hollestelle, A.; Van Deurzen, C.H.M.; et al. The Prevalence of CD146 Expression in Breast Cancer Subtypes and Its Relation to Outcome. Cancers 2018, 10, 134. https://doi.org/10.3390/cancers10050134
De Kruijff IE, Timmermans AM, Den Bakker MA, Trapman-Jansen AMAC, Foekens R, Meijer-Van Gelder ME, Oomen-de Hoop E, Smid M, Hollestelle A, Van Deurzen CHM, et al. The Prevalence of CD146 Expression in Breast Cancer Subtypes and Its Relation to Outcome. Cancers. 2018; 10(5):134. https://doi.org/10.3390/cancers10050134
Chicago/Turabian StyleDe Kruijff, Ingeborg E., Anna M. Timmermans, Michael A. Den Bakker, Anita M.A.C. Trapman-Jansen, Renée Foekens, Marion E. Meijer-Van Gelder, Esther Oomen-de Hoop, Marcel Smid, Antoinette Hollestelle, Carolien H.M. Van Deurzen, and et al. 2018. "The Prevalence of CD146 Expression in Breast Cancer Subtypes and Its Relation to Outcome" Cancers 10, no. 5: 134. https://doi.org/10.3390/cancers10050134