Establishing a Dedicated Lung Cancer Biobank at the University Center Hospital of Nice (France). Why and How?

 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Quantitative Data
2.2. Qualitative Data
2.3. Data Concerning the Activity
2.4. Diffusion of Information and Communication
2.5. Economic Model
2.6. Identification of the Populations of Interest and Securisation by Sample Duplication
3. Discussion
4. Materials and Methods
4.1. Global Strategy of the Nice Hospital-Integrated Lung Tumor Biobank/BB-0033-00025
4.2. Surrogate Indicators
- (i)
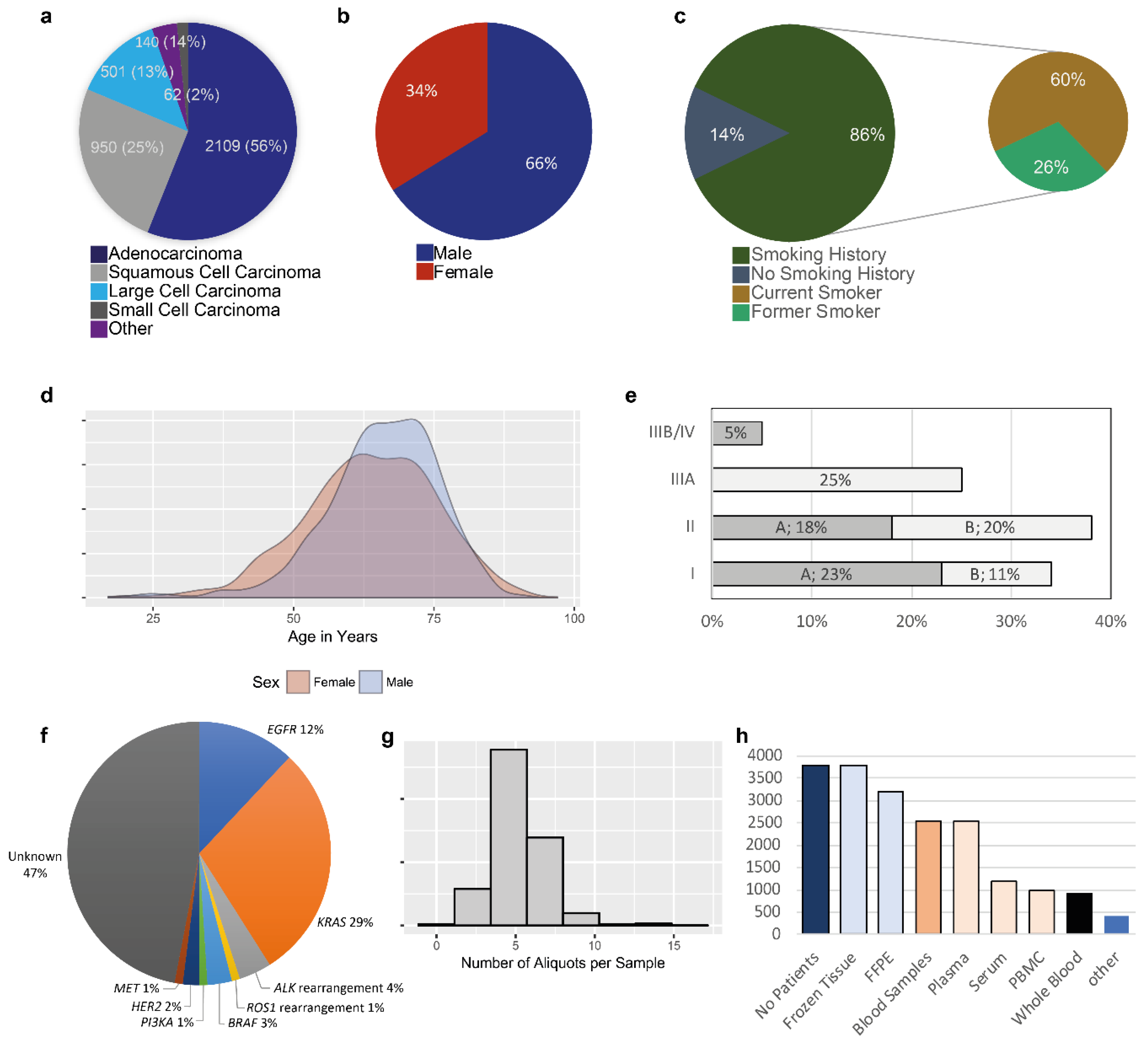
- Quantitative data. The number of patients who gave signed informed consent for the collection of their biological samples was registered each year. Frozen tumor tissue samples were initially registered in the clinical-biological database. Associated clinical data to the biological samples collection included smoking and professional exposure (s) history (obtained by means of a questionnaire), patient and family medical history (including history of cancer), follow up after surgery [tumor recurrence, metastatic site (s), progression free survival, treatment, overall survival]. The aim was to associated the frozen tumor tissues with some other biological resources including ideally for each patient frozen non-tumor tissue, fixed tumor and non-tumor tissue included in paraffin, blood samples (whole blood, plasma, serum, PBMC). The fragments of fresh tissue selected by senior thoracic pathologists were placed in cryotubes and weighed before freezing. Depending on the size of the tumor and on the presence of non-tumor tissue several fragments were frozen with a limit of eight fragments for each tumor and non-tumor tissue. Likewise, the number of fixed tissue blocks and of tubes of sampled blood depended on the amount of the available biological resource.
- (ii)
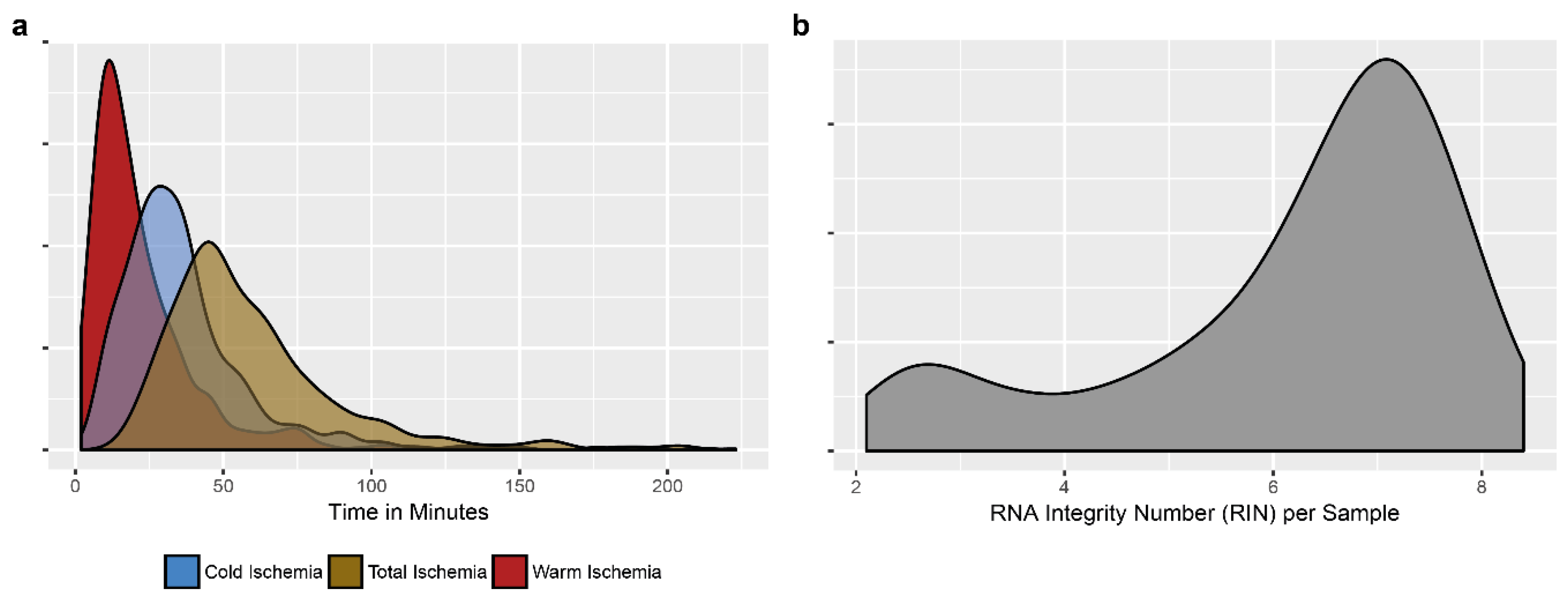
- Qualitative data. The duration of warm and cold ischemia time for the tissue and of the delay between the sampling of the blood and delivery/centrifugation in the laboratory were registered systematically. Quality controls were performed monthly on two randomly selected tissues from cryotubes (one frozen tumor tissue and one frozen non-tumor tissue) by analyzing the RNA integrating number on an Agilent bioanalyzer. A block of fixed tissue (tumor and non-tumor), taken as a mirror sample of the frozen sample, was sectioned and stained with hematoxylin eosin to confirm the tumor and non-tumor character of the corresponding frozen sample and to quantify the percentage of tumor cells and the presence of area of necrosis. These qualitative data reflected the handling of the pre-analytical phase, indicators that are critical to the management of the biobank [71,72,73].
- (iii)
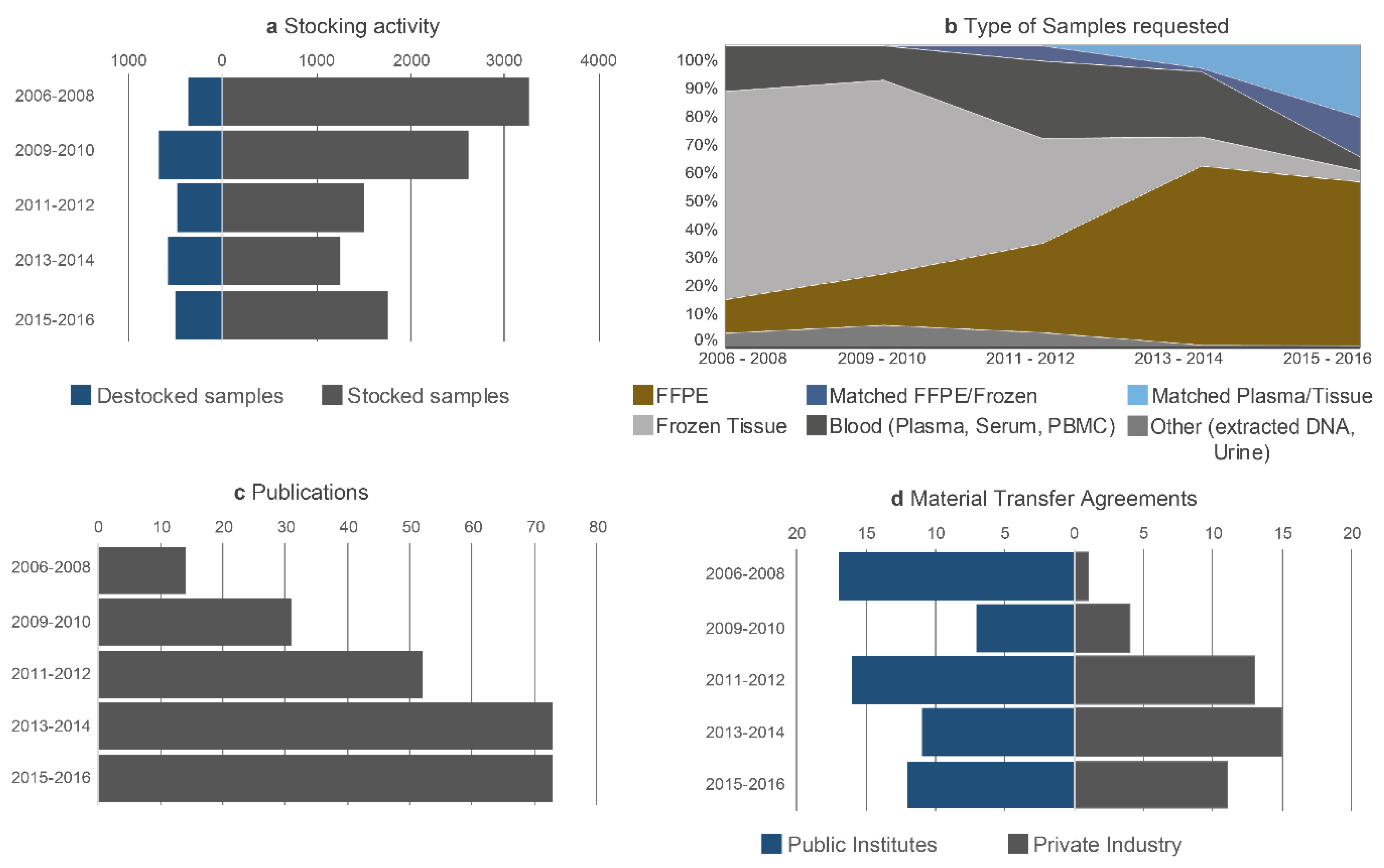
- Data linked to the work. The ratio between the number of samples collected and stored and the number of samples used for research programs (stocking–destocking ratio) was determined annually. The accumulated impact factor of the publications citing the biobank was also noted annually. The number of contracts and MTAs signed each year was monitored, distinguishing between the contracts signed by the academic and industrial partners, both at the national and international levels. Participation in thematic networks, groups of experts and consortium of excellence and in granted research projects was included in this chapter.
- (iv)
- Data associated to the dissemination of the activity of the biobank. This is certainly a challenging criteria to be used for evaluation but several elements were noted: The number of conference presentations, in particular on a topic relative to biobanking, the affiliation of the biobank to international societies of biobanking, training support and teaching related to the activities of biobanks.
- (v)
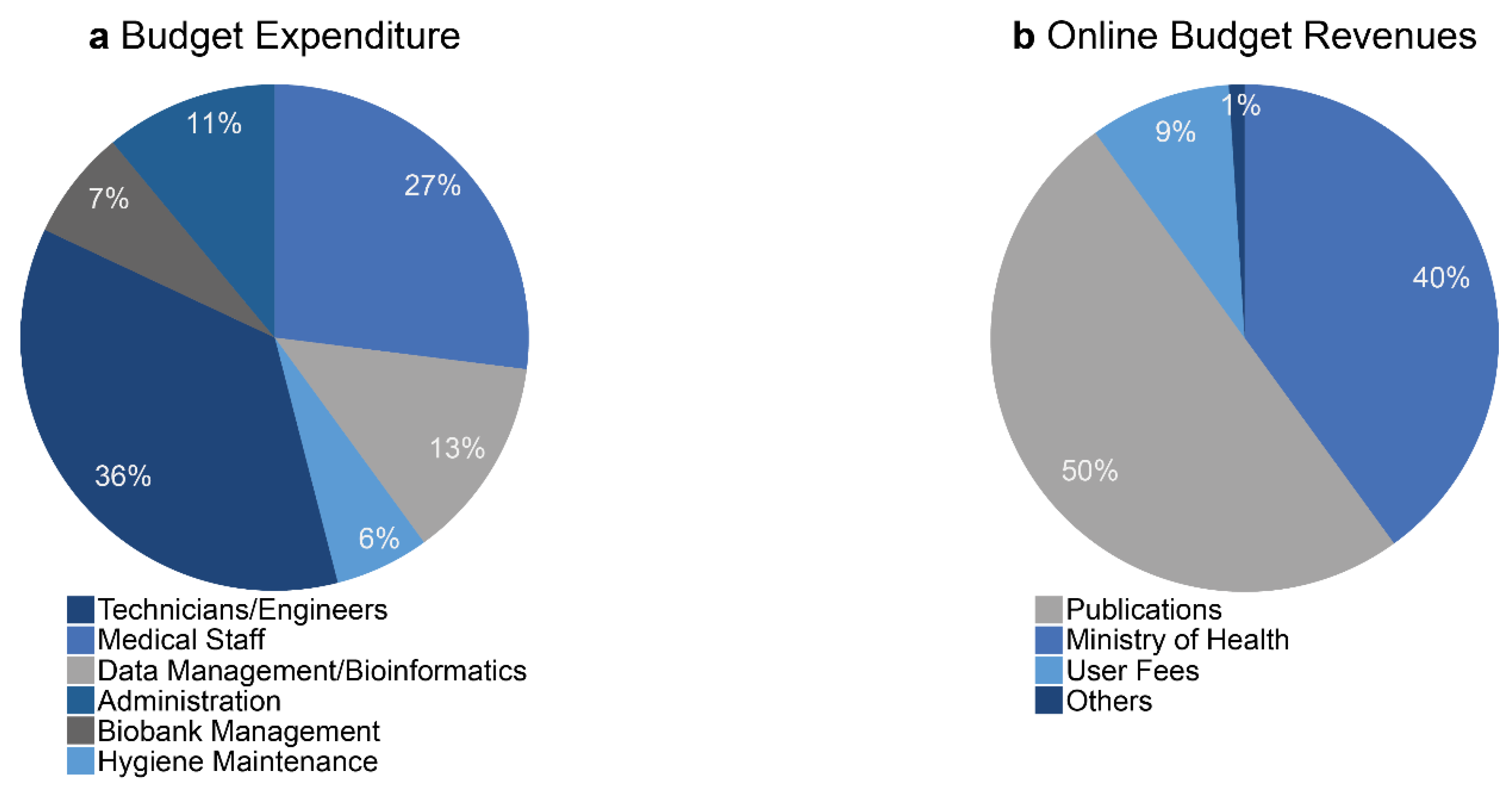
- Economic data. The most critical indicators to monitor include the revenues and expenses since they finally allow the biobank to adapt its working strategy. Annual evaluation of the budget balance is required to invest, pay staff, maintain the equipment and develop innovative projects.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Didkowska, J.; Wojciechowska, U.; Mańczuk, M.; Łobaszewski, J. Lung cancer epidemiology: Contemporary and future challenges worldwide. Ann. Transl. Med. 2016, 4, 150. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Devarakonda, S.; Masood, A.; Govindan, R. Next-Generation Sequencing of Lung Cancers: Lessons Learned and Future Directions. Hematol. Oncol. Clin. North Am. 2017, 31, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Oberndorfer, F.; Müllauer, L. Molecular pathology of lung cancer: Current status and perspectives. Curr. Opin. Oncol. 2018, 30, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Schallenberg, S.; Merkelbach-Bruse, S.; Buettner, R. Lung cancer as a paradigm for precision oncology in solid tumours. Virchows Arch. 2017, 471, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Khagi, Y.; Kurzrock, R.; Patel, S.P. Next generation predictive biomarkers for immune checkpoint inhibition. Cancer Metastasis Rev. 2017, 36, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Mascaux, C.; Tsao, M.-S.; Hirsch, F.R. Genomic Testing in Lung Cancer: Past, Present, and Future. J. Natl. Compr. Cancer Netw. 2018, 16, 323–334. [Google Scholar] [CrossRef]
- Akhtar, N.; Bansal, J.G. Risk factors of Lung Cancer in nonsmoker. Curr. Probl. Cancer 2017, 41, 328–339. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, S.; Heederik, D.; Burdorf, A.; Colosio, C.; Cullinan, P.; Henneberger, P.K.; Olsson, A.; Raynal, A.; Rooijackers, J.; Santonen, T.; et al. European Respiratory Society Environment and Health Committee Current and new challenges in occupational lung diseases. Eur. Respir. Rev. 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, R.E. Biobanking: The foundation of personalized medicine. Curr. Opin. Oncol. 2011, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Zatloukal, K.; Hainaut, P. Human tissue biobanks as instruments for drug discovery and development: Impact on personalized medicine. Biomark. Med. 2010, 4, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Plebani, M. The detection and prevention of errors in laboratory medicine. Ann. Clin. Biochem. 2010, 47, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.P.; Cockburn, I.M.; Simcoe, T.S. The Economics of Reproducibility in Preclinical Research. PLoS Biol. 2015, 13, e1002165. [Google Scholar] [CrossRef] [PubMed]
- Botti, G.; Franco, R.; Cantile, M.; Ciliberto, G.; Ascierto, P.A. Tumor biobanks in translational medicine. J. Transl. Med. 2012, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Botti, G.; De Cecio, R.; Cantile, M. Tumor biobank as fundamental bio-resource for RNA analysis technologies. Minerva Biotecnol. 2017, 29, 106–107. [Google Scholar] [CrossRef]
- Braun, L.; Lesperance, M.; Mes-Massons, A.-M.; Tsao, M.S.; Watson, P.H. Individual Investigator Profiles of Biospecimen Use in Cancer Research. Biopreserv. Biobank. 2014, 12, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Washetine, K.; Long, E.; Hofman, V.; Lassalle, S.; Ilie, M.; Lespinet, V.; Bonnetaud, C.; Bordone, O.; Gavric-Tanga, V.; Selva, E.; et al. The accreditation of a surgical pathology and somatic genetic laboratory (LPCE, CHU of Nice) according to the ISO 15189 norm: Sharing of experience. Ann. Pathol. 2013, 33, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.; Betsou, F. Quality assurance in cancer biobanking. Biopreserv. Biobank. 2011, 9, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P. Liquid biopsy and therapeutic targets: Present and future issues in thoracic oncology. Cancers 2017, 9, 154. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P. Liquid biopsy for early detection of lung cancer. Curr. Opin. Oncol. 2017, 29, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Hofman, V.; Long, E.; Bordone, O.; Selva, E.; Washetine, K.; Marquette, C.H.; Hofman, P. Current challenges for detection of circulating tumor cells and cell-free circulating nucleic acids, and their characterization in non-small cell lung carcinoma patients. What is the best blood substrate for personalized medicine? Ann. Transl. Med. 2014, 2, 107. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, C.; Mack, P.C.; Scagliotti, G.V.; Baas, P.; Barlesi, F.; Bivona, T.G.; Herbst, R.S.; Mok, T.S.; Peled, N.; Pirker, R.; Raez, L.E.; et al. IASLC Statement Paper: Liquid Biopsy for Advanced Non-Small Cell Lung Cancer (NSCLC). J. Thorac. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Brahimi-Horn, M.C.; Ben-Hail, D.; Ilie, M.; Gounon, P.; Rouleau, M.; Hofman, V.; Doyen, J.; Mari, B.; Shoshan-Barmatz, V.; Hofman, P.; et al. Expression of a truncated active form of VDAC1 in lung cancer associates with hypoxic cell survival and correlates with progression to chemotherapy resistance. Cancer Res. 2012, 72, 2140–2150. [Google Scholar] [CrossRef] [PubMed]
- Fouret, R.; Laffaire, J.; Hofman, P.; Beau-Faller, M.; Mazieres, J.; Validire, P.; Girard, P.; Camilleri-Broet, S.; Vaylet, F.; Leroy-Ladurie, F.; et al. A Comparative and Integrative Approach Identifies ATPase Family, AAA Domain Containing 2 as a Likely Driver of Cell Proliferation in Lung Adenocarcinoma. Clin. Cancer Res. 2012, 18, 5606–5616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italiano, A.; Cortot, A.B.; Ilie, M.; Martel-Planche, G.; Fabas, T.; Pop, D.; Mouroux, J.; Hofman, V.; Hofman, P.; Pedeutour, F. EGFR and KRAS status of primary sarcomatoid carcinomas of the lung: Implications for anti-EGFR treatment of a rare lung malignancy. Int. J. Cancer 2009, 125, 2479–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Job, B.; Bernheim, A.; Beau-Faller, M.; Camilleri-Broët, S.; Girard, P.; Hofman, P.; Mazières, J.; Toujani, S.; Lacroix, L.; Laffaire, J.; et al. LG Investigators Genomic aberrations in lung adenocarcinoma in never smokers. PLoS ONE 2010, 5, e15145. [Google Scholar] [CrossRef] [PubMed]
- Hofman, V.; Ilie, M.I.; Long, E.; Selva, E.; Bonnetaud, C.; Molina, T.; Vénissac, N.; Mouroux, J.; Vielh, P.; Hofman, P. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: Comparison of the efficacy of the CellSearch Assay™ and the isolation by size of epithelial tumor cell method. Int. J. Cancer 2011, 129, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P.; Ilie, M.; Hofman, V.; Roux, S.; Valent, A.; Bernheim, A.; Alifano, M.; Leroy-Ladurie, F.; Vaylet, F.; Rouquette, I.; et al. Immunohistochemistry to identify EGFR mutations or ALK rearrangements in patients with lung adenocarcinoma. Ann. Oncol. 2012, 23, 1738–1743. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.I.; Hofman, V.; Bonnetaud, C.; Havet, K.; Lespinet-Fabre, V.; Coëlle, C.; Gavric-Tanga, V.; Vénissac, N.; Mouroux, J.; Hofman, P. Usefulness of tissue microarrays for assessment of protein expression, gene copy number and mutational status of EGFR in lung adenocarcinoma. Virchows Arch. 2010, 457, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Mazure, N.M.; Hofman, V.; Ammadi, R.E.; Ortholan, C.; Bonnetaud, C.; Havet, K.; Venissac, N.; Mograbi, B.; Mouroux, J.; et al. High levels of carbonic anhydrase IX in tumour tissue and plasma are biomarkers of poor prognostic in patients with non-small cell lung cancer. Br. J. Cancer 2010, 102, 1627–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, M.; Khambata-Ford, S.; Copie-Bergman, C.; Huang, L.; Juco, J.; Hofman, V.; Hofman, P. Use of the 22C3 anti-PD-L1 antibody to determine PD-L1 expression in multiple automated immunohistochemistry platforms. PLoS ONE 2017, 12, e0183023. [Google Scholar] [CrossRef]
- Ilie, M.; Juco, J.; Huang, L.; Hofman, V.; Khambata-Ford, S.; Hofman, P. Use of the 22C3 anti-programmed death-ligand 1 antibody to determine programmed death-ligand 1 expression in cytology samples obtained from non-small cell lung cancer patients. Cancer Cytopathol. 2018, 126, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Szafer-Glusman, E.; Hofman, V.; Long-Mira, E.; Suttmann, R.; Darbonne, W.; Butori, C.; Lalvée, S.; Fayada, J.; Selva, E.; et al. Expression of MET in circulating tumor cells correlates with expression in tumor tissue from advanced-stage lung cancer patients. Oncotarget 2017, 8, 26112–26121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazières, J.; Rouquette, I.; Lepage, B.; Milia, J.; Brouchet, L.; Guibert, N.; Beau-Faller, M.; Validire, P.; Hofman, P.; Fouret, P. Specificities of Lung Adenocarcinoma in Women Who Have Never Smoked. J. Thorac. Oncol. 2013, 8, 923–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, M.I.; Hofman, V.; Ortholan, C.; Ammadi, R. El; Bonnetaud, C.; Havet, K.; Venissac, N.; Mouroux, J.; Mazure, N.M.; Pouysségur, J.; Hofman, P. Overexpression of carbonic anhydrase XII in tissues from resectable non-small cell lung cancers is a biomarker of good prognosis. Int. J. Cancer 2011, 128, 1614–1623. [Google Scholar] [CrossRef] [PubMed]
- Puisségur, M.-P.; Mazure, N.M.; Bertero, T.; Pradelli, L.; Grosso, S.; Robbe-Sermesant, K.; Maurin, T.; Lebrigand, K.; Cardinaud, B.; Hofman, V.; et al. miR-210 is overexpressed in late stages of lung cancer and mediates mitochondrial alterations associated with modulation of HIF-1 activity. Cell Death Differ. 2011, 18, 465–478. [Google Scholar] [CrossRef]
- Rakha, E.; Pajares, M.J.; Ilie, M.; Pio, R.; Echeveste, J.; Hughes, E.; Soomro, I.; Long, E.; Idoate, M.A.; Wagner, S.; et al. Stratification of resectable lung adenocarcinoma by molecular and pathological risk estimators. Eur. J. Cancer 2015, 51, 1897–1903. [Google Scholar] [CrossRef] [PubMed]
- Sanfiorenzo, C.; Ilie, M.I.; Belaid, A.; Barlési, F.; Mouroux, J.; Marquette, C.-H.; Brest, P.; Hofman, P. Two panels of plasma microRNAs as non-invasive biomarkers for prediction of recurrence in resectable NSCLC. PLoS ONE 2013, 8, e54596. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Long, E.; Butori, C.; Hofman, V.; Coelle, C.; Mauro, V.; Zahaf, K.; Marquette, C.H.; Mouroux, J.; Paterlini-Bréchot, P.; et al. ALK-gene rearrangement: A comparative analysis on circulating tumour cells and tumour tissue from patients with lung adenocarcinoma. Ann. Oncol. 2012, 23, 2907–2913. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Hofman, V.; Ortholan, C.; Bonnetaud, C.; Coëlle, C.; Mouroux, J.; Hofman, P. Predictive clinical outcome of the intratumoral CD66b-positive neutrophil-to-CD8-positive T-cell ratio in patients with resectable nonsmall cell lung cancer. Cancer 2012, 118, 1726–1737. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Hofman, V.; Zangari, J.; Chiche, J.; Mouroux, J.; Mazure, N.M.; Pouysségur, J.; Brest, P.; Hofman, P. Response of CAIX and CAXII to in vitro re-oxygenation and clinical significance of the combined expression in NSCLC patients. Lung Cancer 2013, 82, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Long, E.; Hofman, V.; Dadone, B.; Marquette, C.H.; Mouroux, J.; Vignaud, J.M.; Begueret, H.; Merlio, J.P.; Capper, D.; et al. Diagnostic value of immunohistochemistry for the detection of the BRAFV600E mutation in primary lung adenocarcinoma Caucasian patients. Ann. Oncol. 2013, 24, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Nunes, M.; Blot, L.; Hofman, V.; Long-Mira, E.; Butori, C.; Selva, E.; Merino-Trigo, A.; Vénissac, N.; Mouroux, J.; et al. Setting up a wide panel of patient-derived tumor xenografts of non-small cell lung cancer by improving the preanalytical steps. Cancer Med. 2015, 4, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Ilié, M.; Szafer-Glusman, E.; Hofman, V.; Chamorey, E.; Lalvée, S.; Selva, E.; Leroy, S.; Marquette, C.-H.; Kowanetz, M.; Hedge, P.; et al. Detection of PD-L1 in circulating tumor cells and white blood cells from patients with advanced non-small-cell lung cancer. Ann. Oncol. 2018, 29, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Long, E.; Hofman, V.; Selva, E.; Bonnetaud, C.; Boyer, J.; Vénissac, N.; Sanfiorenzo, C.; Ferrua, B.; Marquette, C.-H.; et al. Clinical value of circulating endothelial cells and of soluble CD146 levels in patients undergoing surgery for non-small cell lung cancer. Br. J. Cancer 2014, 110, 1236–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chabannon, C.; Honstettre, A.; Daufresne, L.-M.; Martin, P.-M.; Bonnetaud, C.; Birtwisle-Peyrottes, I.; Romain, S.; Achache, K.; Mery, O.; Bordonne, O.; et al. Publication of biological samples collections catalogues by tumor banks. Bull. Cancer 2010, 97, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Chalabreysse, L.; Thomas De Montpreville, V.; De Muret, A.; Hofman, V.; Lantuejoul, S.; Parrens, M.; Payan, M.-J.; Rouquette, I.; Secq, V.; Girard, N.; et al. Rythmic-pathology: The French national pathology network for thymic epithelial tumours. Ann. Pathol. 2014, 34, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Doucet, M.; Becker, K.F.; Björkman, J.; Bonnet, J.; Clément, B.; Daidone, M.-G.; Duyckaerts, C.; Erb, G.; Haslacher, H.; Hofman, P.; et al. Quality Matters: 2016 Annual Conference of the National Infrastructures for Biobanking. Biopreserv. Biobank. 2017, 15, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Galateau-Sallé, F.; Gilg Soit Ilg, A.; Le Stang, N.; Brochard, P.; Pairon, J.C.; Astoul, P.; Frenay, C.; Blaizot, G.; Chamming’s, S.; Ducamp, S.; et al. The French mesothelioma network from 1998 to 2013. Ann. Pathol. 2014, 34, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Biobank Unit of the Centre Hospitalo-Universitaire (CHU) de Nice (Biobank06). Biopreserv. Biobank. 2011, 9, 5–6. [CrossRef]
- Gormally, E.; Hardy, I.; Caboux, E.; di Donato, J.-H.; Hainaut, P.; Hofman, P. Training the Next Generation of Biobankers: A Two-Year Master’s Course in the Management of Biobanks. Biopreserv. Biobank. 2017, 15, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Lagardere, C.H.P. French Biobank Secures Specimens. Available online: http://www.rfidjournal.com/article/view/8303 (accessed on 17 February 2018).
- Les missions d’enseignement, de recherche, de référence et d’innovation—MERRI. Available online: http://solidarites-sante.gouv.fr/systeme-de-sante-et-medico-social/recherche-et-innovation/l-innovation-et-la-recherche-clinique/article/les-missions-d-enseignement-de-recherche-de-reference-et-d-innovation-merri (accessed on 15 June 2018).
- Washetine, K.; Kara-borni, M.; Heeke, S.; Bonnetaud, C.; Jean-marc, F.; Ribeyre, L.; Bence, C.; Ili, M.; Bordone, O.; Pedro, M.; et al. Ensuring the Safety and Security of Frozen Lung Cancer Tissue Collections through the Encapsulation of Dried DNA. Cancers 2018, 10, 195. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, G.; Bosman, F.; Dassesse, T.; Höfler, H.; Janin, A.; Langer, R.; Larsimont, D.; Morente, M.M.; Riegman, P.; Schirmacher, P.; et al. The role of the pathologist in tissue banking: European Consensus Expert Group Report. Virchows Arch. 2010, 456, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P.; Bréchot, C.; Zatloukal, K.; Dagher, G.; Clément, B. Public–private relationships in biobanking: A still underestimated key component of open innovation. Virchows Arch. 2014, 464, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, R.; Hainaut, P. Biobanking in a Fast Moving World: An International Perspective. JNCI Monogr. 2011, 2011, 50–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaught, J.; Lockhart, N.C. The evolution of biobanking best practices. Clin. Chim. Acta 2012, 413, 1569–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Pelayo, T.; Babinszky, S.; LeBlanc, J.; Watson, P.H. The Importance of Biobanking in Cancer Research. Biopreserv. Biobank. 2015, 13, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.; Cheah, S.; Dee, S.; Hughes, S.; Watson, P.H. Biospecimen Use Correlates with Emerging Techniques in Cancer Research: Impact on Planning Future Biobanks. Biopreserv. Biobank. 2012, 10, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.E.; Barnes, R.O.; Watson, P.H. Biospecimen use in cancer research over two decades. Biopreserv. Biobank. 2010, 8, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Clément, B.; Yuille, M.; Zaltoukal, K.; Wichmann, H.-E.; Anton, G.; Parodi, B.; Kozera, L.; Bréchot, C.; Hofman, P.; Dagher, G. EU-US Expert Group on cost recovery in biobanks Public biobanks: Calculation and recovery of costs. Sci. Transl. Med. 2014, 6, 261fs45. [Google Scholar] [CrossRef]
- Gonzalez-Sanchez, M.B.; Lopez-Valeiras, E.; Morente, M.M.; Fernández Lago, O. Cost Model for Biobanks. Biopreserv. Biobank. 2013, 11, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Cambon-Thomsen, A.; Thorisson, G.A.; Mabile, L. BRIF Workshop Group The role of a bioresource research impact factor as an incentive to share human bioresources. Nat. Genet. 2011, 43, 503–504. [Google Scholar] [CrossRef] [PubMed]
- Mabile, L.; Dalgleish, R.; Thorisson, G.A.; Deschênes, M.; Hewitt, R.; Carpenter, J.; Bravo, E.; Filocamo, M.; Gourraud, P.A.; Harris, J.R.; et al. Quantifying the use of bioresources for promoting their sharing in scientific research. Gigascience 2013, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- Hofman, V.; Bonnetaud, C.; Gaziello, M.C.; Ilie, M.; Lassalle, S.; Butori, C.; Lerda, N.; Selva, E.; Gavric-Tanga, V.; Castillo, L.; et al. The Nice CHU biobank experience to collect patients’ informed consent for research context (2004–2009). Ann. Pathol. 2010, 30, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.boutique.afnor.org/norme/v2/nf-s96-900/qualite-des-centres-de-ressources-biologiques-crb-systeme-de-management-d-un-crb-et-qualite-des-ressources-biologiques/article/747984/fa169771 (accessed on 22 April 2018).
- Hofman, V.; Ilie, M.; Long, E.; Washetine, K.; Chabannon, C.; Figarella-Branger, D.; Clément, B.; Mabile, L.; Cambon-Thomsen, A.; Boucher, P.; et al. Measuring the contribution of tumor biobanks to research in oncology: Surrogate indicators and bibliographic output. Biopreserv. Biobank. 2013, 11, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.H.; Dry, S.M.; Shabihkhani, M. A practical approach to clinical and research biobanking. Methods Mol. Biol. 2014, 1180, 137–162. [Google Scholar] [CrossRef] [PubMed]
- Ellervik, C.; Vaught, J. Preanalytical variables affecting the integrity of human biospecimens in biobanking. Clin. Chem. 2015, 61, 914–934. [Google Scholar] [CrossRef] [PubMed]
- Hubel, A.; Spindler, R.; Skubitz, A.P.N. Storage of human biospecimens: Selection of the optimal storage temperature. Biopreserv. Biobank. 2014, 12, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Dai, H.; Kong, X. Impact of warm ischemia on gene expression analysis in surgically removed biosamples. Anal. Biochem. 2012, 423, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Basik, M.; Aguilar-Mahecha, A.; Rousseau, C.; Diaz, Z.; Tejpar, S.; Spatz, A.; Greenwood, C.M.T.; Batist, G. Biopsies: Next-generation biospecimens for tailoring therapy. Nat. Rev. Clin. Oncol. 2013, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Diaz, Z.; Aguilar-Mahecha, A.; Paquet, E.R.; Basik, M.; Orain, M.; Camlioglu, E.; Constantin, A.; Benlimame, N.; Bachvarov, D.; Jannot, G.; et al. Next-generation biobanking of metastases to enable multidimensional molecular profiling in personalized medicine. Mod. Pathol. 2013, 26, 1413–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Guo, X.-R.; Tang, X.-J.; Sun, X.-Y.; Yang, Z.-S.; Zhang, Y.; Dai, L.-J.; Warnock, G.L. Intravital biobank and personalized cancer therapy: The correlation with omics. Int. J. Cancer 2014, 135, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Wei, B.-R.; Simpson, R.M. Digital pathology and image analysis augment biospecimen annotation and biobank quality assurance harmonization. Clin. Biochem. 2014, 47, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Bottlenecks and Limitations in Current Functioning of the BB-0033-00025 | Proposed Solutions to Improve the Future Development for Research Projects |
|---|---|
|
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Washetine, K.; Heeke, S.; Bonnetaud, C.; Kara-Borni, M.; Ilié, M.; Lassalle, S.; Butori, C.; Long-Mira, E.; Marquette, C.H.; Cohen, C.; et al. Establishing a Dedicated Lung Cancer Biobank at the University Center Hospital of Nice (France). Why and How? Cancers 2018, 10, 220. https://doi.org/10.3390/cancers10070220
Washetine K, Heeke S, Bonnetaud C, Kara-Borni M, Ilié M, Lassalle S, Butori C, Long-Mira E, Marquette CH, Cohen C, et al. Establishing a Dedicated Lung Cancer Biobank at the University Center Hospital of Nice (France). Why and How? Cancers. 2018; 10(7):220. https://doi.org/10.3390/cancers10070220
Chicago/Turabian StyleWashetine, Kevin, Simon Heeke, Christelle Bonnetaud, Mehdi Kara-Borni, Marius Ilié, Sandra Lassalle, Catherine Butori, Elodie Long-Mira, Charles Hugo Marquette, Charlotte Cohen, and et al. 2018. "Establishing a Dedicated Lung Cancer Biobank at the University Center Hospital of Nice (France). Why and How?" Cancers 10, no. 7: 220. https://doi.org/10.3390/cancers10070220