Radiotherapy for T1N0M0 Esophageal Cancer: Analyses of the Predictive Factors and the Role of Endoscopic Submucosal Dissection in the Local Control

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
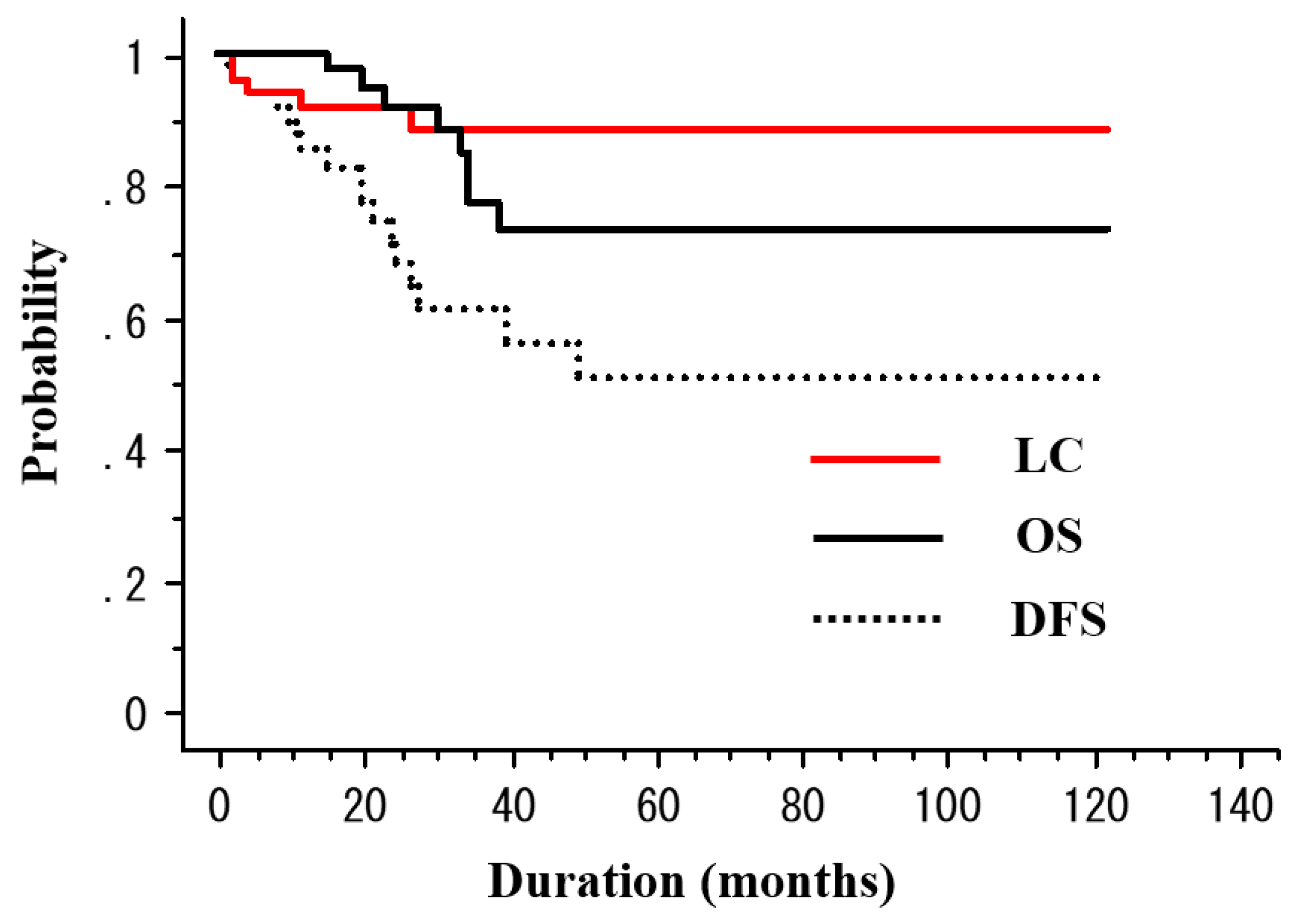
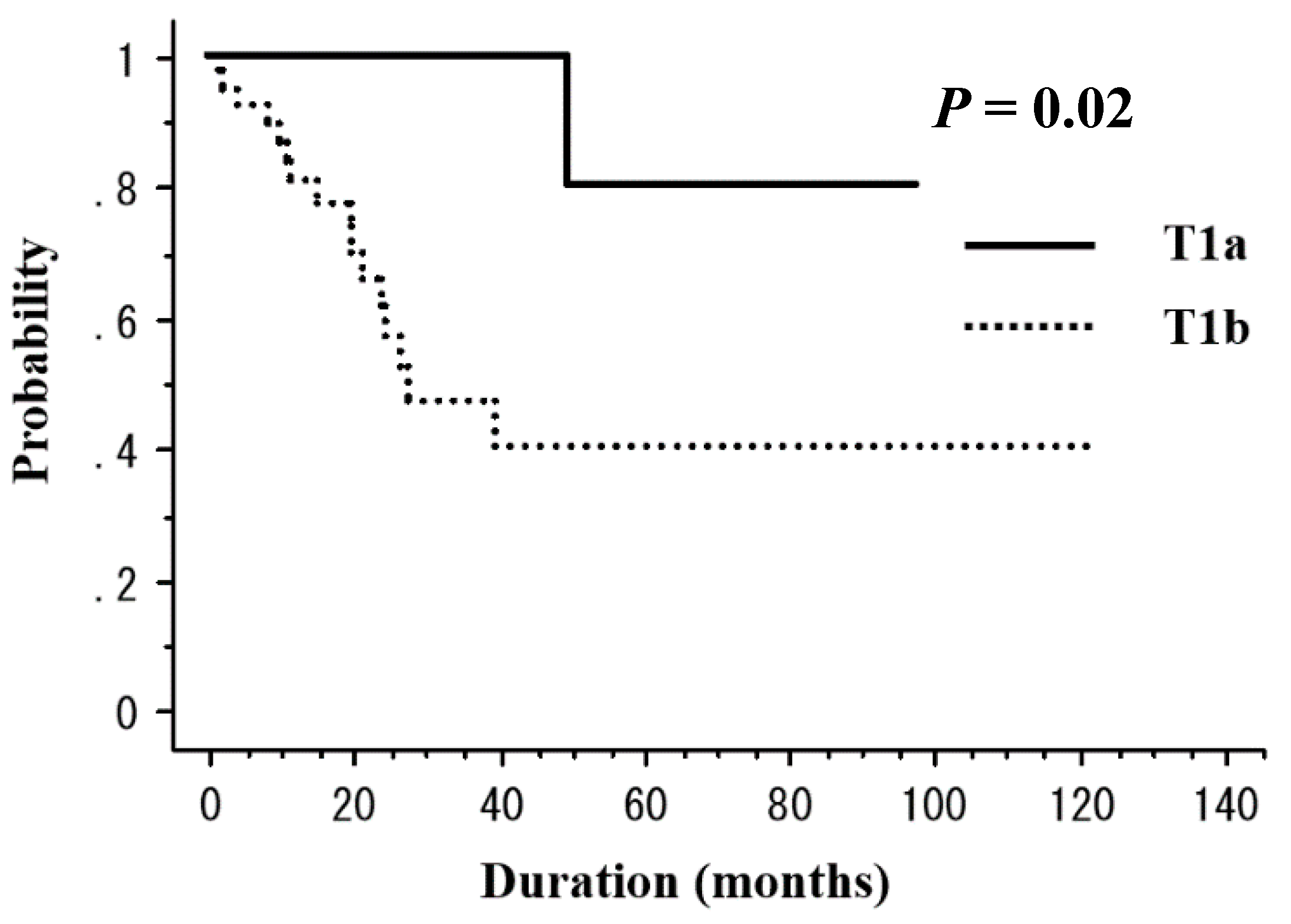
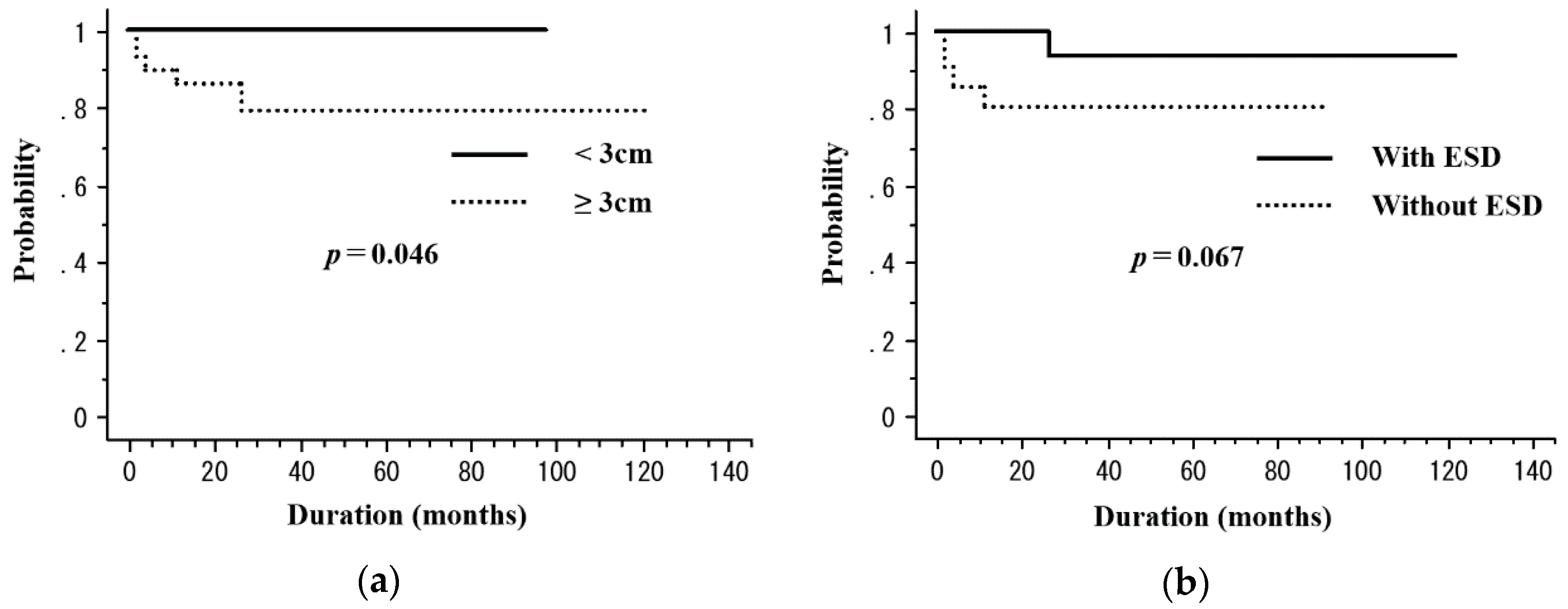
2.2. Treatment Outcomes
2.3. Toxicity
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Treatment
4.3. Follow-Up and Evaluation
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wang, G.Q.; Jiao, G.G.; Chang, F.B.; Fang, W.H.; Song, J.X.; Lu, N.; Lin, D.M.; Xie, Y.Q.; Yang, L. Long-term results of operation for 420 patients with early squamous cell esophageal carcinoma discovered by screening. Ann. Thorac. Surg. 2004, 77, 1740–1744. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, M.; Hirahara, N.; Kinugasa, S.; Yoshimura, H. Clinicopathologic Features of Superficial Esophageal Cancer: Results of Consecutive 100 Patients. Ann. Surg. Oncol. 2008, 15, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Igaki, H.; Kato, H.; Tachimori, Y.; Daiko, H.; Fukaya, M.; Yajima, S.; Nakanishi, Y. Clinicopathologic characteristics and survival of patients with clinical Stage I squamous cell carcinomas of the thoracic esophagus treated with three-field lymph node dissection. Eur. J. Cardio Thorac. Surg. 2001, 20, 1089–1094. [Google Scholar] [CrossRef] [Green Version]
- Griffin, M.S.; Shaw, I.H.; Dresner, S.M. Early complications after Ivor Lewis subtotal esophagectomy with two-field lymphadenectomy: Risk factors and management. J. Am. Coll. Surg. 2002, 194, 285–297. [Google Scholar] [CrossRef]
- Tachibana, M.; Kinugasa, S.; Hiroshi, Y.; Shibakita, M.; Tonomoto, Y.; Dhar, D.; Nagasue, N. Clinical outcomes of extended esophagectomy with three-field lymph node dissection for esophageal squamous cell carcinoma. J. Am. Coll. Surg. 2005, 189, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Fujishiro, M.; Niimi, K.; Goto, O.; Kodashima, S.; Yamamichi, N.; Omata, M. Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest. Endosc. 2009, 70, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Hassan, C.; Carlino, A.; Pagano, N.; Zullo, A.; Rando, G.; Strangio, G.; Romeo, F.; Nicita, R.; Rosati, R.; et al. Endoscopic submucosal dissection in patients with early esophageal squamous cell carcinoma: results from a prospective Western series. Gastrointest. Endosc. 2010, 71, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Sato, A.; Fukuda, H.; Kagami, Y.; Udagawa, H.; Togo, A.; Ando, N.; Tanaka, O.; Shinoda, M.; Yamana, H.; et al. A phase II trial of chemoradiotherapy for stage I esophageal squamous cell carcinoma: Japan Clinical Oncology Group Study (JCOG9708). Jpn. J. Clin. Oncol. 2009, 39, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Koide, Y.; Kodaira, T.; Tachibana, H.; Tomita, N.; Makita, C.; Itoh, M.; Abe, T.; Muro, K.; Tajika, M.; Niwa, Y.; et al. Clinical outcome of definitive radiation therapy for superficial esophageal cancer. Jpn. J. Clin. Oncol. 2017, 47, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Kam, T.Y.; Kountouri, M.; Roth, A.; Jean-Loui, F.; Huber, O.; Mönig, S.; Zilli, T. Endoscopic resection with adjuvant chemo-radiotherapy for superficial esophageal squamous cell carcinoma: A critical review. Crit. Rev. Oncol. Hematol. 2018, 124, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Ishihara, R.; Motoori, M.; Kawaguchi, Y.; Uedo, N.; Takeuchi, Y.; Higashino, K.; Yano, M.; Nakamura, S.; Iishi, H. Comparison Between Definitive Chemoradiotherapy and Esophagectomy in Patients with Clinical Stage I Esophageal Squamous Cell Carcinoma. Am. J. Gastroenterol. 2011, 106, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Motoori, M.; Yano, M.; Ishihara, R.; Yamamoto, S.; Kawaguchi, Y.; Tanaka, K.; Kishi, K.; Miyashiro, I.; Fujiwara, Y.; Shingai, T.; et al. Comparison Between Radical Esophagectomy and Definitive Chemoradiotherapy in Patients with Clinical T1bN0M0 Esophageal Cancer. Ann. Surg. Oncol. 2012, 19, 2135–2141. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, G.; Sasamoto, R.; Abe, E.; Ohta, A.; Sato, H.; Tanaka, K.; Maruyama, K.; Kaizu, M.; Ayukawa, F.; Yamana, N.; et al. The effectiveness of endoscopic submucosal dissection followed by chemoradiotherapy for superficial esophageal cancer. Radiat. Oncol. 2015, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Morita, M.; Kumashiro, R.; Hisamatsu, Y.; Nakanishi, R.; Egashira, A.; Saeki, H.; Oki, E.; Ohga, T.; Kakeji, Y.; Tsujitani, S.; et al. Clinical significance of salvage esophagectomy for remnant or recurrent cancer following definitive chemoradiotherapy. J. Gastroenterol. 2011, 46, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Hamada, K.; Ishihara, R.; Yamasaki, Y.; Hanaoka, N.; Yamamoto, S.; Arao, M.; Suzuki, S.; Iwatsubo, T.; Kato, M.; Tonai, Y.; et al. Efficacy and Safety of Endoscopic Resection Followed by Chemoradiotherapy for Superficial Esophageal Squamous Cell Carcinoma: A Retrospective Study. Clin. Transl. Gastroenterol. 2017, 8, 110. [Google Scholar] [CrossRef] [PubMed]
- Uchinami, Y.; Myojin, M.; Takahashi, H.; Harada, K.; Shimizu, S.; Hosokawa, M. Prognostic factors in clinical T1N0M0 thoracic esophageal squamous cell carcinoma invading the muscularis mucosa or submucosa. Radiat. Oncol. 2016, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, Y.; Muto, M.; Minashi, K.; Boku, N.; Fukuda, H. A phase II trial of combined treatment of endoscopic mucosal resection and chemoradiotherapy for clinical stage I esophageal carcinoma: Japan clinical oncology group study (JCOG0508). Jpn. J. Clin. Oncol. 2009, 39, 686–689. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Fujishiro, M.; Niimi, K.; Goto, O.; Kodashima, S.; Yamamichi, N.; Omata, M. Predictors of postoperative stricture after esophageal endoscopic submucosal dissection for superficial squamous cell neoplasms. Endoscopy 2009, 41, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Hisano, O.; Nonoshita, T.; Hirata, H.; Sasaki, T.; Watanabe, H.; Wakiyama, H.; Ono, M.; Ohga, S.; Honda, H. Additional radiotherapy following endoscopic submucosal dissection for T1a-MM/T1b-SM esophageal squamous cell carcinoma improves locoregional control. Radiat. Oncol. 2018, 13, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, H.; Takenaka, R.; Omori, M.; Imae, T.; Okuma, K.; Ohtomo, K.; Nakagawa, K. Involved-field radiotherapy (IFRT) versus elective nodal irradiation (ENI) in combination with concurrent chemotherapy for 239 esophageal cancers: A single institutional retrospective study. Radiat. Oncol. 2015, 10, 171. [Google Scholar] [CrossRef] [PubMed]
- Onozawa, M.; Nihei, K.; Ishikura, S.; Minashi, K.; Yano, T.; Muto, M.; Ohtsu, A.; Ogino, T. Elective nodal irradiation (ENI) in definitive chemoradiotherapy (CRT) for squamous cell carcinoma of the thoracic esophagus. Radiother. Oncol. 2009, 92, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Ma, J.B.; Liu, G.; Wu, K.; Shi, X.; Jiang, G.L. Three-dimensional conformal radiation therapy for esophageal squamous cell carcinoma: is elective nodal irradiation necessary? Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Kuwano, H.; Nishimura, Y.; Oyama, T.; Kato, H.; Kitagawa, Y.; Kusano, M.; Shimada, H.; Takiuchi, H.; Toh, Y.; Doki, Y.; et al. Guidelines for diagnosis and treatment of carcinoma of the Esophagus April 2012 edited by the Japan esophageal society. Esophagus 2015, 12, 1–30. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Cancer. Common Terminology Criteria for Adverse Events (CTCAE); National Institute of Cancer: Rockville, MD, USA, 2010. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ESD 2 Group | Non-ESD Group | p Value | |
|---|---|---|---|
| Characteristic | (n = 29) | (n = 21) | |
| Age (years) | |||
| Median (range) | 68 (50–82) | 75 (59–87) | 0.018 |
| Sex, n | |||
| Male | 24 | 17 | 0.99 |
| Female | 5 | 4 | |
| Performance status, n | |||
| 0 | 25 | 16 | 0.59 |
| ≥1 | 4 | 5 | |
| Main tumor location, n | |||
| Upper thorax | 4 | 4 | 0.44 |
| Middle thorax | 13 | 10 | |
| Lower thorax | 12 | 7 | |
| T Stage, n | |||
| T1a | 8 | 3 | 0.44 |
| T1b | 21 | 18 | |
| Tumor length (cm) | |||
| Median (range) | 2.3 (1–10) | 5 (1–20) | 0.017 |
| Tumor number, n | |||
| 1 | 5 | 6 | 0.34 |
| ≥2 | 24 | 15 | |
| Concurrent chemotherapy, n | |||
| yes | 28 | 18 | 0.39 |
| no | 1 | 3 | |
| Radiation field, n | |||
| ENI 1 | 13 | 4 | 0.11 |
| Non-ENI | 16 | 17 | |
| Total radiation dose, n | |||
| ≤50.4 Gy | 26 | 12 | 0.02 |
| >50.4 Gy | 3 | 9 |
| Number (%) | Depth of Invasion | ||||
|---|---|---|---|---|---|
| All Patients | M3 | SM1 | SM2 | SM3 | |
| Number | 29 | 8 | 4 | 16 | 1 |
| Resection status | |||||
| R0 1 resection | 19 (66%) | 6 | 2 | 11 | 0 |
| R1 2 resection | 10 (34%) | 2 | 2 | 5 | 1 |
| Lymphovascular invasion | |||||
| Positive | 20 (69%) | 5 | 3 | 11 | 1 |
| Negative | 9 (31%) | 3 | 1 | 5 | 0 |
| Poorly differentiated histology | |||||
| Yes | 4 (14%) | 1 | 0 | 3 | 0 |
| No | 25 (86%) | 7 | 4 | 13 | 1 |
| Age | Sex | PS 12 | T Stage | Tumor Length (cm) | RT 13 Field | RT Dose (Gy) | ESD 8 | Resection Status | Lymphovasucular Invasion | Depth of Invasion | Poorly Differentiated Histology | CCRT 4 | Months to Disease Recurrence | Recurrence Site | Salvage Therapy | Status at Last Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 68 | Male | 0 | T1b | 2 | ENI 7 | 40 | + | R0 14 | + | SM1 | – | + | 11 | Metachronous esohageal lesion (IF 9) | ESD | ANED 1 20 m 11 |
| 60 | Male | 0 | T1b | 8 | ENI | 50 | + | R1 15 | + | SM3 | – | + | 24 | Distance | chemo | DID 5 33 m |
| 69 | Male | 1 | T1b | 2.1 | ENI | 40 | + | R0 | + | SM2 | – | + | 10 | Metachronous esohageal lesion (OF 10) | ESD | ANED 45 m |
| 59 | Male | 0 | T1a | 3.4 | Non-ENI | 50.4 | + | R0 | – | M3 | + | + | 50 | Metachronous esohageal lesion (OF) | ESD | ANED 79 m |
| 61 | Male | 0 | T1b | 1 | Non-ENI | 50 | + | R0 | + | SM2 | – | + | 40 | Regional (OF) | CRT | ANED 98 m |
| 75 | Male | 1 | T1b | 2.5 | Non-ENI | 60 | + | R1 | + | SM2 | + | + | 9 | Regional (OF) | chemo | AWD 3 21 m |
| 65 | Male | 0 | T1b | 10 | Non-ENI | 40 | + | R0 | – | SM2 | – | + | 27 | Local | APC 2 | ANED 112 m |
| 57 | Male | 0 | T1b | 1 | Non-ENI | 60 | + | R1 | + | SM2 | – | – | 24 | Regional (IF) | chemo | DID 34 m |
| 86 | Male | 0 | T1b | 6 | Non-ENI | 42 | – | – | 2 | Local | chemo | DID 31 m | ||||
| 61 | Male | 0 | T1b | 5 | ENI | 50.4 | – | + | 4 | Metachronous esohageal lesion (OF) | ESD | ANED 65 m | ||||
| 71 | Male | 0 | T1b | 6 | Non-ENI | 50.4 | – | + | 12 | Local | chemo | DID 34 m | ||||
| 75 | Male | 0 | T1b | 1.5 | Non-ENI | 60 | – | + | 20 | Metachronous esohageal lesion (OF) | ESD | ANED 92 m | ||||
| 83 | Female | 2 | T1b | 3 | Non-ENI | 50 | – | + | 2 | Local | no | AWD 39 m | ||||
| 80 | Male | 1 | T1b | 8 | Non-ENI | 54 | – | + | 22 | Regional (OF) | no | DOD 6 23 m | ||||
| 70 | Male | 0 | T1b | 1.5 | Non-ENI | 60 | – | + | 28 | Distance | chemo | DID 38 m |
| N | 3-Year DFS 1 (%) | p Value | 3-Year LC 4 (%) | p Value | |
|---|---|---|---|---|---|
| Age (years) | |||||
| ≤70 | 24 | 62.2 | 0.99 | 87.9 | 0.63 |
| >70 | 26 | 61.1 | 89 | ||
| Sex | |||||
| Male | 41 | 57.8 | 0.38 | 88.3 | 0.82 |
| Female | 9 | 90 | 90 | ||
| PS 5 | |||||
| 0 | 41 | 66.1 | 0.08 | 88.1 | 0.86 |
| ≥1 | 9 | 38.1 | 90 | ||
| T stage | |||||
| T1a | 11 | 100 | 0.02 | 100 | 0.18 |
| T1b | 39 | 47.1 | 83.8 | ||
| Tumor number | |||||
| 1 | 39 | 67.7 | 0.43 | 87.7 | 0.89 |
| ≥2 | 11 | 39 | 100 | ||
| Tumor length | |||||
| <3 cm | 21 | 55.1 | 0.55 | 100 | 0.046 |
| ≥3 cm | 29 | 65.1 | 79.3 | ||
| Radiation dose | |||||
| ≤50.4 Gy | 38 | 63.9 | 0.94 | 84.5 | 0.19 |
| >50.4 Gy | 12 | 53.9 | 100 | ||
| Radiation field | |||||
| ENI 2 | 17 | 69.9 | 0.65 | 100 | 0.53 |
| Non-ENI | 33 | 58.5 | 85.6 | ||
| ESD 3 | |||||
| Yes | 29 | 70 | 0.37 | 93.3 | 0.067 |
| No | 21 | 52.4 | 80.4 |
| Age (Years) | Sex | Adverse Event | Grade | RT Field | ESD 3 | CRT 1 | Tumor Length (cm) | Tumor Circumferential Extension | RT 4 Dose (Gy) |
|---|---|---|---|---|---|---|---|---|---|
| 80 | Female | Pericardial effusion | 2 | Non-ENI 2 | − | + | 20 | Entire | 50 |
| 70 | Female | Pericardial effusion | 2 | Non-ENI | − | + | 15 | Entire | 60 |
| 54 | Female | Esophageal strictures | 2 | ENI | + | + | 5 | 1/2 | 40 |
| 65 | Male | Esophageal strictures | 2 | ENI | + | + | 7.4 | 2/3 | 40 |
| 60 | Male | Esophageal strictures | 2 | ENI | + | + | 8 | 2/3 | 50 |
| 59 | Male | Esophageal strictures | 2 | Non-ENI | − | + | 14 | Entire | 50.4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, G.; Yamazaki, H.; Aibe, N.; Masui, K.; Shimizu, D.; Kimoto, T.; Nishimura, T.; Nakashima, A.; Takenaka, T.; Dohi, O.; et al. Radiotherapy for T1N0M0 Esophageal Cancer: Analyses of the Predictive Factors and the Role of Endoscopic Submucosal Dissection in the Local Control. Cancers 2018, 10, 259. https://doi.org/10.3390/cancers10080259
Suzuki G, Yamazaki H, Aibe N, Masui K, Shimizu D, Kimoto T, Nishimura T, Nakashima A, Takenaka T, Dohi O, et al. Radiotherapy for T1N0M0 Esophageal Cancer: Analyses of the Predictive Factors and the Role of Endoscopic Submucosal Dissection in the Local Control. Cancers. 2018; 10(8):259. https://doi.org/10.3390/cancers10080259
Chicago/Turabian StyleSuzuki, Gen, Hideya Yamazaki, Norihiro Aibe, Koji Masui, Daisuke Shimizu, Takuya Kimoto, Takeshi Nishimura, Akihiro Nakashima, Tadashi Takenaka, Osamu Dohi, and et al. 2018. "Radiotherapy for T1N0M0 Esophageal Cancer: Analyses of the Predictive Factors and the Role of Endoscopic Submucosal Dissection in the Local Control" Cancers 10, no. 8: 259. https://doi.org/10.3390/cancers10080259