Molecular Characterization of a Long-Term Survivor Double Metastatic Non-Small Cell Lung Cancer and Pancreatic Ductal Adenocarcinoma Treated with Gefitinib in Combination with Gemcitabine Plus Nab-Paclitaxel and mFOLFOX6 as First and Second Line Therapy

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Experimental Section
2.1. Patient Record
2.2. DNA Extraction
2.3. Variant Calling
3. Results
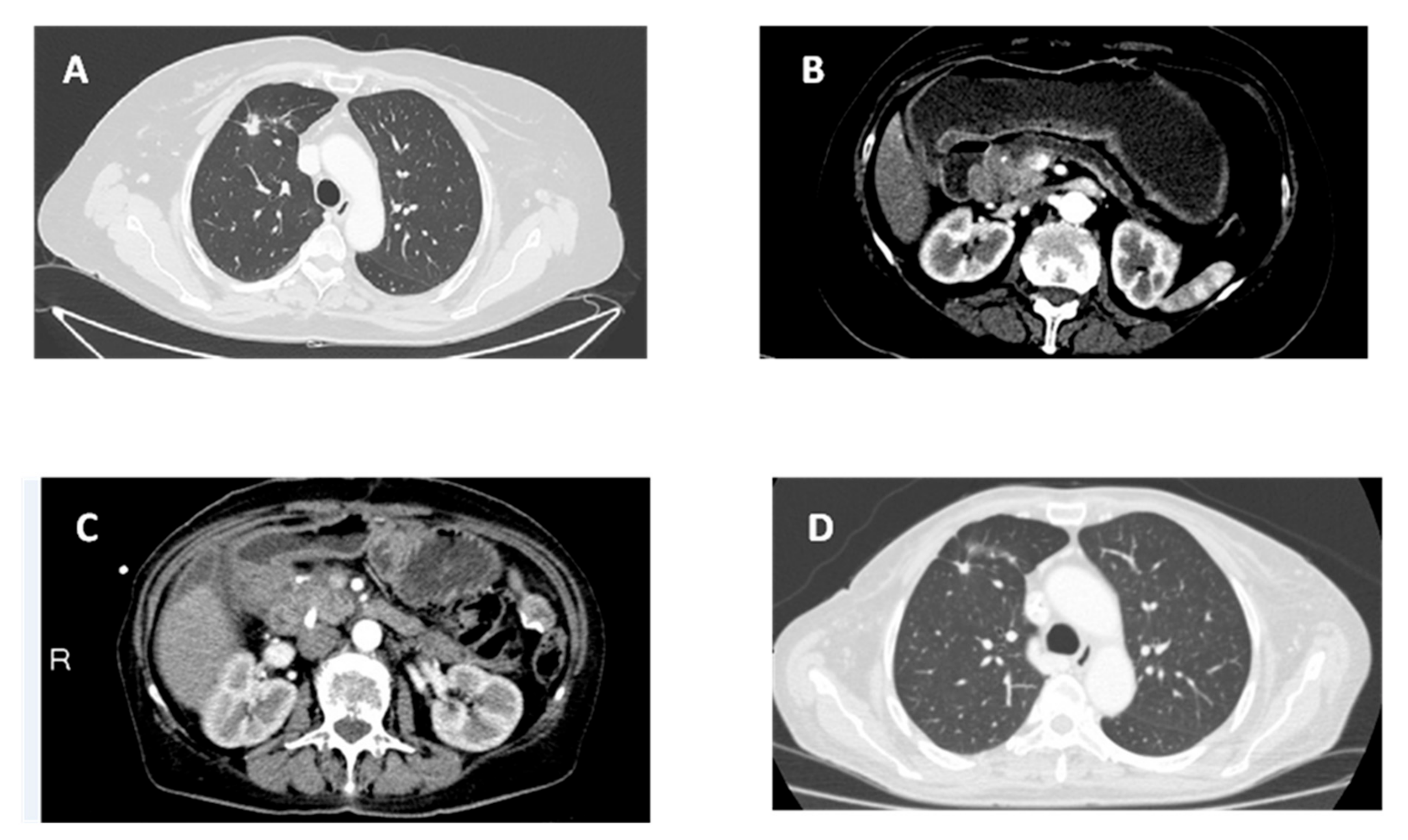
3.1. Patient’s History
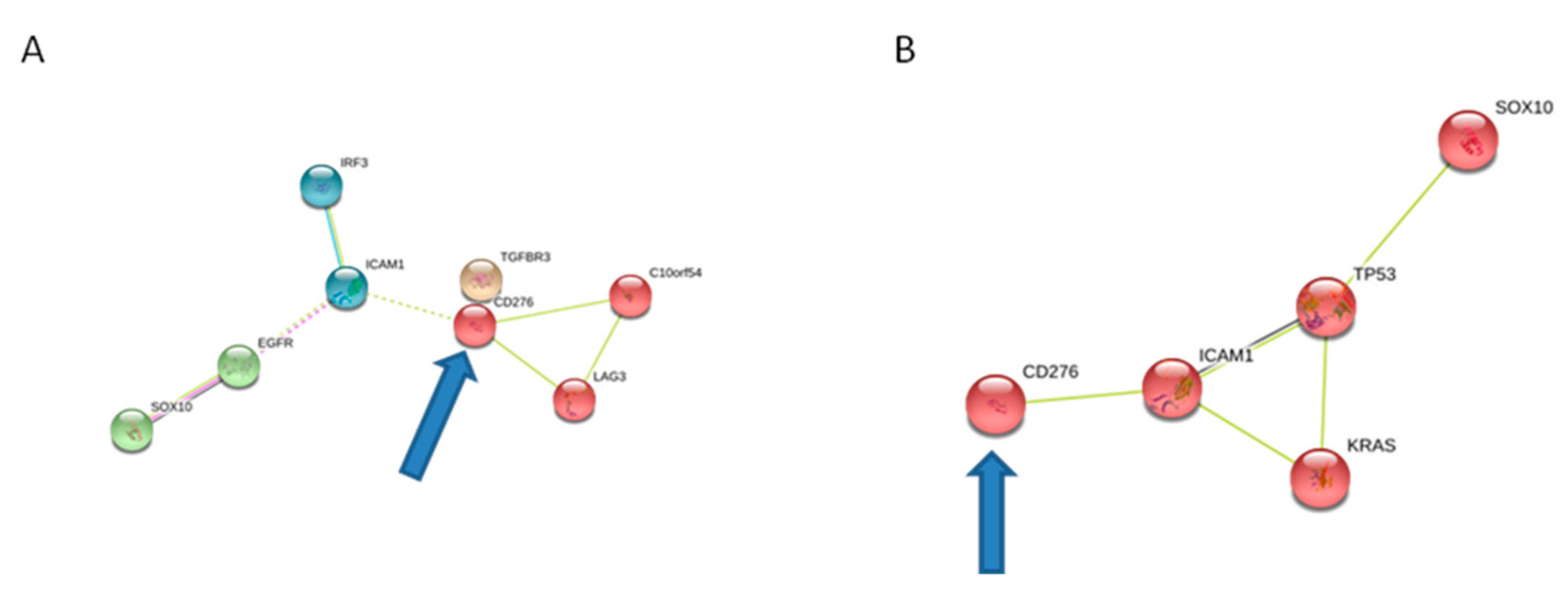
3.2. Molecular Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hayat, M.J.; Howlader, N.; Reichman, M.E.; Edwards, B.K. Cancer statistics, trends, and multiple primary cancer analyses from the Surveillance, Epidemiology, and End Results (SEER) Program. Oncologist 2007, 12, 20–37. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.J.; Park, H.; Sung, Y.N.; Yoo, C.; Hwang, D.W.; Park, J.H.; Kim, K.P.; Lee, S.S.; Ryoo, B.Y.; Seo, D.W. Prognosis of Pancreatic Cancer Patients with Synchronous or Metachronous Malignancies from Other Organs Is Better than Those with Pancreatic Cancer Only. Cancer Res. Treat 2018, 50, 1175–1185. [Google Scholar] [CrossRef]
- Gerdes, B.; Ziegler, A.; Ramaswamy, A.; Wild, A.; Langer, P.; Bartsch, D.K. Multiple primaries in pancreatic cancer patients: indicator of a genetic predisposition? Int. J. Epidemiol. 2000, 29, 999–1003. [Google Scholar] [CrossRef]
- Tagawa, T.; Ito, K.; Fukuzawa, K.; Okamoto, T.; Fujinaga, A.; Kawasaki, T.; Masuda, T.; Iwaki, K.; Terashi, T.; Okamoto, M.; et al. Surgical outcomes of non-small cell lungcancer in patients with a history of pancreatic obiliary cancer. Anticancer Res. 2017, 37, 3307–3309. [Google Scholar] [CrossRef]
- Moertel, C.G.; Dockerty, M.B.; Baggenstoss, A.H. Multiple primarymalignant neoplasm. Introduction and presentation of data. Cancer 1961, 14, 221–230. [Google Scholar] [CrossRef]
- Ikematsu, Y.; Tamura, H.; Hayashi, T.; Tokunaga, Y.; Misawa, Y.; Mori, H.; Hasegawa, S.; Okawada, T.; Ozawa, T.; Momiki, S.; et al. Metachronous double cancer after curative resection for pancreatic adenocarcinoma: report of four cases. Clin. J. Gastroenterol. 2012, 5, 108–112. [Google Scholar] [CrossRef]
- Eriguchi, N.; Aoyagi, S.; Hara, M.; Okuda, K.; Tamae, T.; Fukuda, S.; Hashino, K.; Sato, S.; Fujiki, K.; Furukawa, S.; et al. Synchronous or metachronous double cancers of the pancreas and other organs: report on 12 cases. Surg. Today 2000, 30, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Loukeri, A.A.; Kampolis, C.F.; Ntokou, A.; Tsoukalas, G.; Syrigos, K. Metachronous and synchronous primary lung cancers: diagnostic aspects, surgical treatment, and prognosis. Clin. Lung Cancer 2015, 16, 15–23. [Google Scholar] [CrossRef]
- Quatrale, A.E.; Porcelli, L.; Silvestris, N.; Colucci, G.; Angelo, A.; Azzariti, A. EGFR tyrosine kinases inhibitors in cancer treatment: In vitro and in vivo evidence. Front Biosci. 2011, 16, 1962–1972. [Google Scholar] [CrossRef]
- Yan, H.; Li, H.; Li, Q.; Zhao, P.; Wang, W.; Cao, B. The Efficacy of Synchronous Combination of Chemotherapy and EGFR TKIs for the First-Line Treatment of NSCLC: A Systematic Analysis. PLoS ONE 2015, 10, e0135829. [Google Scholar] [CrossRef]
- Nakamura, A.; Inoue, A.; Morita, S.; Hosomi, Y.; Kato, T.; Fukuhara, T.; Gemma, A.; Takahashi, K.; Fujita, Y.; Harada, T.; Minato, K.; et al. Phase III study comparing gefitinib monotherapy (G) to combination therapy with gefitinib, carboplatin, and pemetrexed (GCP) for untreated patients (pts) with advanced non-small cell lung cancer (NSCLC) with EGFR mutations (NEJ009). J. Clin. Oncol. 2018, 36 (Suppl. 15), 9005. [Google Scholar] [CrossRef]
- Cohen, S.J.; O’Neil, B.H.; Berlin, J.; Ames, P.; McKinley, M.; Horan, J.; Catalano, P.M.; Davies, A.; Davies, A.; Weekes, C.D.; Leichman, L. A phase 1b study of erlotinib in combination with gemcitabine and nab-paclitaxel in patients with previously untreated advanced pancreatic cancer: an Academic Oncology GI Cancer Consortium study. Cancer Chemother. Pharmacol. 2016, 77, 693–701. [Google Scholar] [PubMed]
- Lai, Z.; Markovets, A.; Ahdesmaki, M.; Chapman, B.; Hofmann, O.; McEwen, R.; Johnson, J.; Dougherty, B.; Barrett, J.C.; Dry, J.R. VarDict: A novel and versatile variant caller for next-generation sequencing in cancer research. Nucleic Acids Res. 2016, 44, e108. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Handsaker, B.; Wysoker, A.; Fennell, T.; Ruan, J.; Homer, N.; Marth, G.; Abecasis, G.; Durbin, R. 1000 Genome Project Data Processing Subgroup. The Sequence Alignment/Map format and SAMtools. Bioinformatics 2009, 25, 2078–2079. [Google Scholar] [CrossRef]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef] [PubMed]
- Wellcome Sanger Institute. Available online: http://www.sanger.ac.uk/cosmic (accessed on 4 October 2018).
- STRING Protein Interacting Network. Available online: https://string-db.org/ (accessed on 4 October 2018).
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Gill, S.; Ko, Y.J.; Cripps, C.; Beaudoin, A.; Dhesy-Thind, S.; Zulfiqar, M.; Zalewski, P.; Do, T.; Cano, P.; Lam, W.Y.H.; et al. PANCREOX: A Randomized Phase III Study of Fluorouracil/Leucovorin With or Without Oxaliplatin for Second-Line Advanced Pancreatic Cancer in Patients Who Have Received Gemcitabine- Based Chemotherapy. J. Clin. Oncol. 2016, 34, 3914–3920. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; Campos, D.; et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef]
- Wu, S.; Zhao, X.; Wu, S.; Du, R.; Zhu, Q.; Fang, H.; Zhang, X.; Zhang, C.; Zheng, W.; Yang, J.; et al. Overexpression of B7-H3 correlates with aggressive clinicopathological characteristics in non-small cell lung cancer. Oncotarget 2016, 7, 81750–81756. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, G.; Sheng, S.; Zhou, Q.; Pan, Y.; Guan, S. Upregulation of soluble B7-H3 in NSCLC-derived malignant pleural effusion: A potential diagnostic biomarker correlated with NSCLC staging. Clin. Chim. Acta 2016, 457, 81–85. [Google Scholar] [CrossRef]
- Zhao, J.; Meng, Z.; Xie, C.; Yang, C.; Liu, Z.; Wu, S.; Wang, B.; Fan, P.; Jin, X.; Wu, H. B7-H3 is regulated by BRD4 and promotes TLR4 expression in pancreatic ductal adenocarcinoma. Int. J. Biochem. Cell Biol. 2019, 108, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Takazawa, Y.; Inoue, Y.; Yokouchi, Y.; Kobayashi, M.; Saiura, A.; Shibutani, T.; Ishikawa, Y. Tumor B7-H3 (CD276) Expression and Survival in Pancreatic Cancer. J. Clin. Med. 2018, 7, e172. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, J.; Zhou, J.; Zhan, S.; Huang, Y.; Wang, F.; Zhang, Z.; Zhu, D.; Zhao, H.; Li, D. B7-H3 combats apoptosis induced by chemotherapy by delivering signals to pancreatic cancer cells. Oncotarget 2017, 8, 74856–74868. [Google Scholar] [CrossRef]
- Liu, H.L.; Tekle, C.; Chen, Y.W.; Kristian, A.; Kristian, Y.; Zhou, M.; Liu, Z.; Ding, Y.; Wang, B.; Mælandsmo, G.M.; et al. B7-H3 silencing increases paclitaxel sensitivity by abrogating Jak2/Stat3 phosphorylation. Mol. Cancer Ther. 2011, 10, 960–971. [Google Scholar] [CrossRef] [PubMed]
- Nunes-Xavier, C.; Karlsen, K.F.; Tekle, C.; Pedersen, C.; Øyjord, T.; Hongisto, V.; Nesland, J.M.; Tan, M.; Sahlberg, K.K.; Fodstad, Ø. Decreased expression of B7-H3 reduces the glycolytic capacity and sensitizes breast cancer cells to AKT/mTOR inhibitors. Oncotarget 2016, 7, 6891–6901. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| NSCLC Sample | |
|---|---|
| TGFBR3 c.* 1C > T | 3′UTR |
| VSIR c.C770T:p.A257V | Non synonimous |
| LAG3 c.C1360T:p.L454F | Non synonimous |
| ICAM1 c.G457A:p.G153R | Non synonimous |
| IRF3 c.G77A:p.W26X | Stop gain |
| SOX10 c.C1358T:p.T453I | Non synonimous |
| PDAC Sample | |
| ICAM1 c.C628T:p.Q210X | Non synonimous |
| SOX10 c.G955A:p.G319R | Stop gain |
| Common Mutation | |
| CD276 c.T410A:p.L137H | Non synonimous |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunetti, O.; Badalamenti, G.; De Summa, S.; Calabrese, A.; Argentiero, A.; Fucci, L.; Longo, V.; Galetta, D.; Perrotti, P.M.S.; Pinto, R.; et al. Molecular Characterization of a Long-Term Survivor Double Metastatic Non-Small Cell Lung Cancer and Pancreatic Ductal Adenocarcinoma Treated with Gefitinib in Combination with Gemcitabine Plus Nab-Paclitaxel and mFOLFOX6 as First and Second Line Therapy. Cancers 2019, 11, 749. https://doi.org/10.3390/cancers11060749
Brunetti O, Badalamenti G, De Summa S, Calabrese A, Argentiero A, Fucci L, Longo V, Galetta D, Perrotti PMS, Pinto R, et al. Molecular Characterization of a Long-Term Survivor Double Metastatic Non-Small Cell Lung Cancer and Pancreatic Ductal Adenocarcinoma Treated with Gefitinib in Combination with Gemcitabine Plus Nab-Paclitaxel and mFOLFOX6 as First and Second Line Therapy. Cancers. 2019; 11(6):749. https://doi.org/10.3390/cancers11060749
Chicago/Turabian StyleBrunetti, Oronzo, Giuseppe Badalamenti, Simona De Summa, Angela Calabrese, Antonella Argentiero, Livia Fucci, Vito Longo, Domenico Galetta, Pia Maria Soccorsa Perrotti, Rosamaria Pinto, and et al. 2019. "Molecular Characterization of a Long-Term Survivor Double Metastatic Non-Small Cell Lung Cancer and Pancreatic Ductal Adenocarcinoma Treated with Gefitinib in Combination with Gemcitabine Plus Nab-Paclitaxel and mFOLFOX6 as First and Second Line Therapy" Cancers 11, no. 6: 749. https://doi.org/10.3390/cancers11060749
APA StyleBrunetti, O., Badalamenti, G., De Summa, S., Calabrese, A., Argentiero, A., Fucci, L., Longo, V., Galetta, D., Perrotti, P. M. S., Pinto, R., Petriella, D., Danza, K., Tommasi, S., Leonetti, F., & Silvestris, N. (2019). Molecular Characterization of a Long-Term Survivor Double Metastatic Non-Small Cell Lung Cancer and Pancreatic Ductal Adenocarcinoma Treated with Gefitinib in Combination with Gemcitabine Plus Nab-Paclitaxel and mFOLFOX6 as First and Second Line Therapy. Cancers, 11(6), 749. https://doi.org/10.3390/cancers11060749