Increased Level of Phosphorylated ShcA Measured by Chemiluminescence-Linked Immunoassay Is a Predictor of Good Prognosis in Primary Breast Cancer Expressing Low Levels of Estrogen Receptor

Abstract
:1. Introduction
2. Results and Discussion
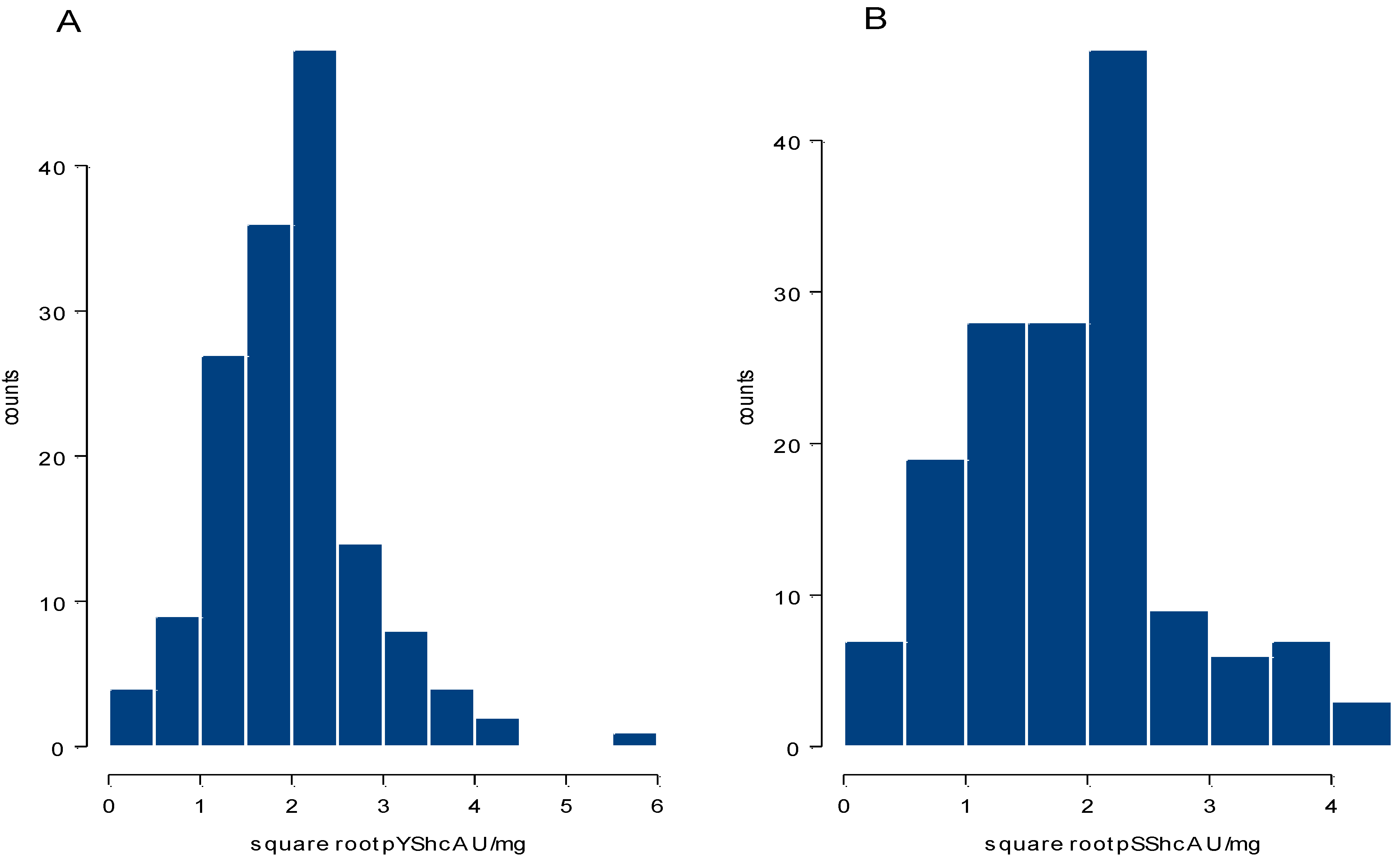
2.1. Distribution of Phosphorylated ShcA Levels and Their Correlation with Tumor Characteristics


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ErbB2 | pTErbB2 | pAkt | ER | pYShcA | pSShcA | |
|---|---|---|---|---|---|---|
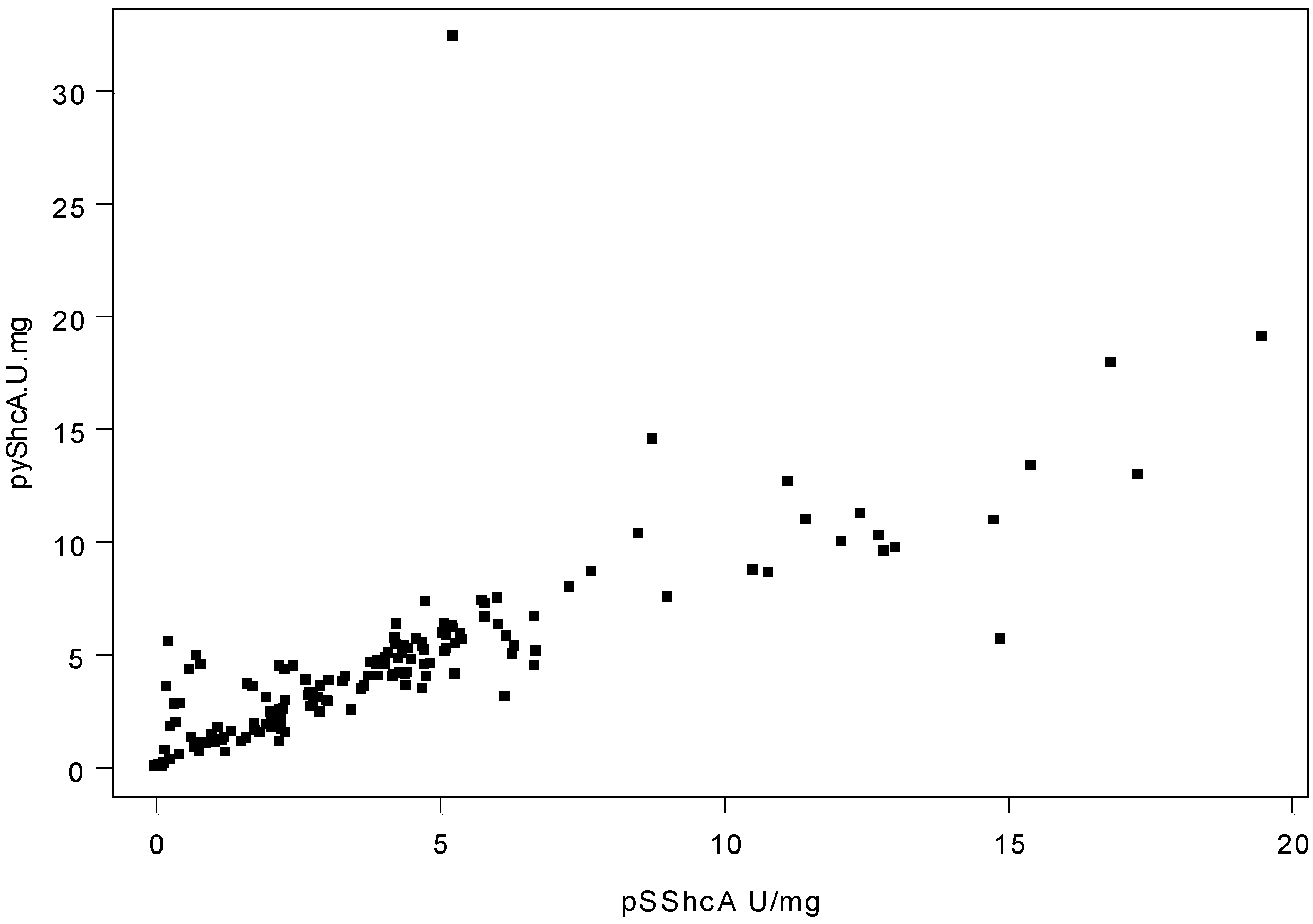
| pYShcA | rs = -0.17 | rs = 0.27 | rs = -0.27 | rs = -0.16 | rs = 1 | rs = 0.88 |
| (p = 0.03) | (p = 0.01) | (p = 0.01) | (p = 0.05) | (p < 0.001) | ||
| pSShcA | n.s. | rs = 0.21 | rs = -0.28 | rs = -0.16 | rs = 0.88 | rs = 1 |
| (p = 0.01) | (p < 0.001) | (p = 0.05) | (p < 0.001) |
2.2. Correlation of Phosphorylated ShcA Levels and Levels of Other Tumor Markers

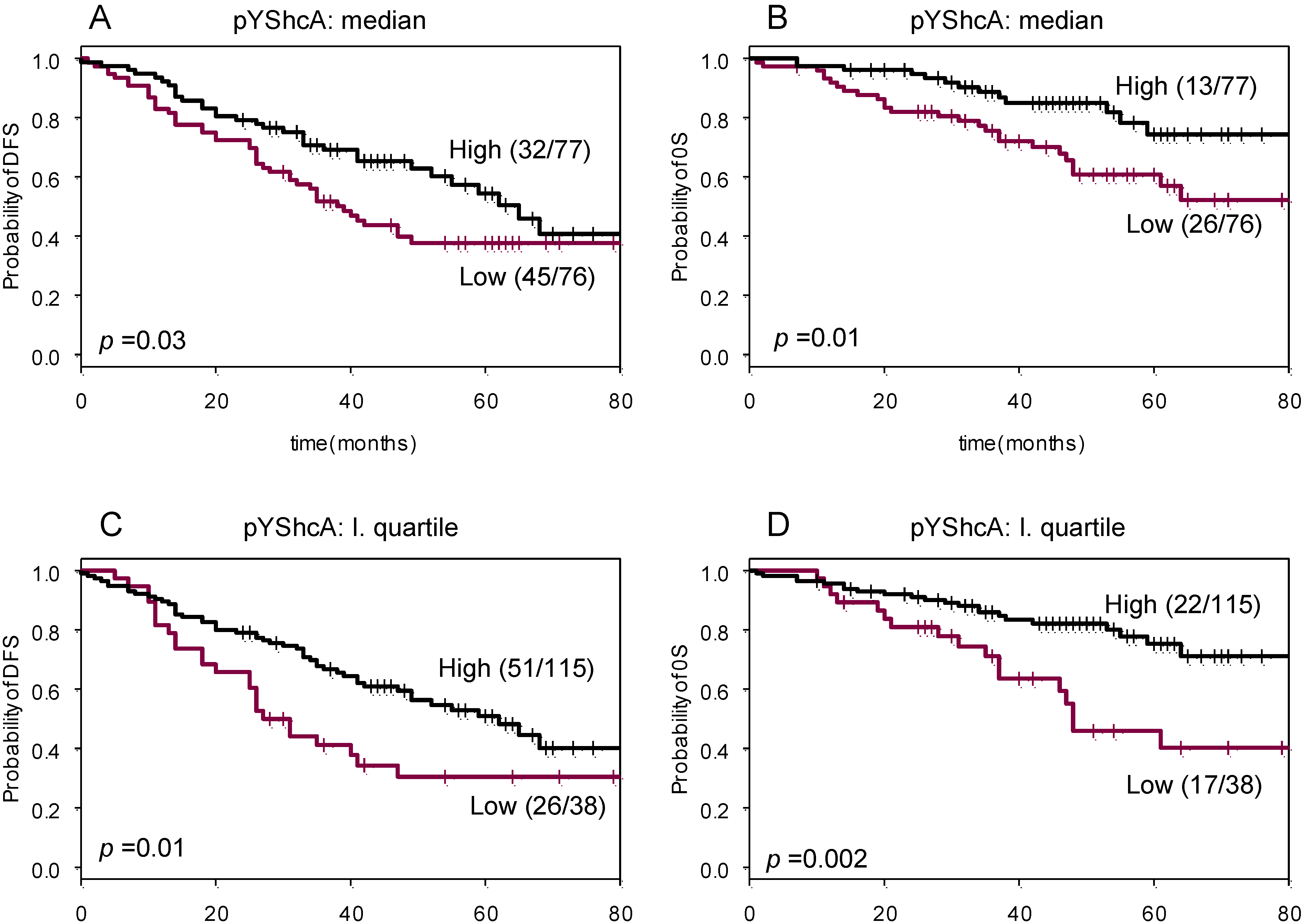
2.3. Prognostic Significance of Tyrosine Phosphorylated ShcA

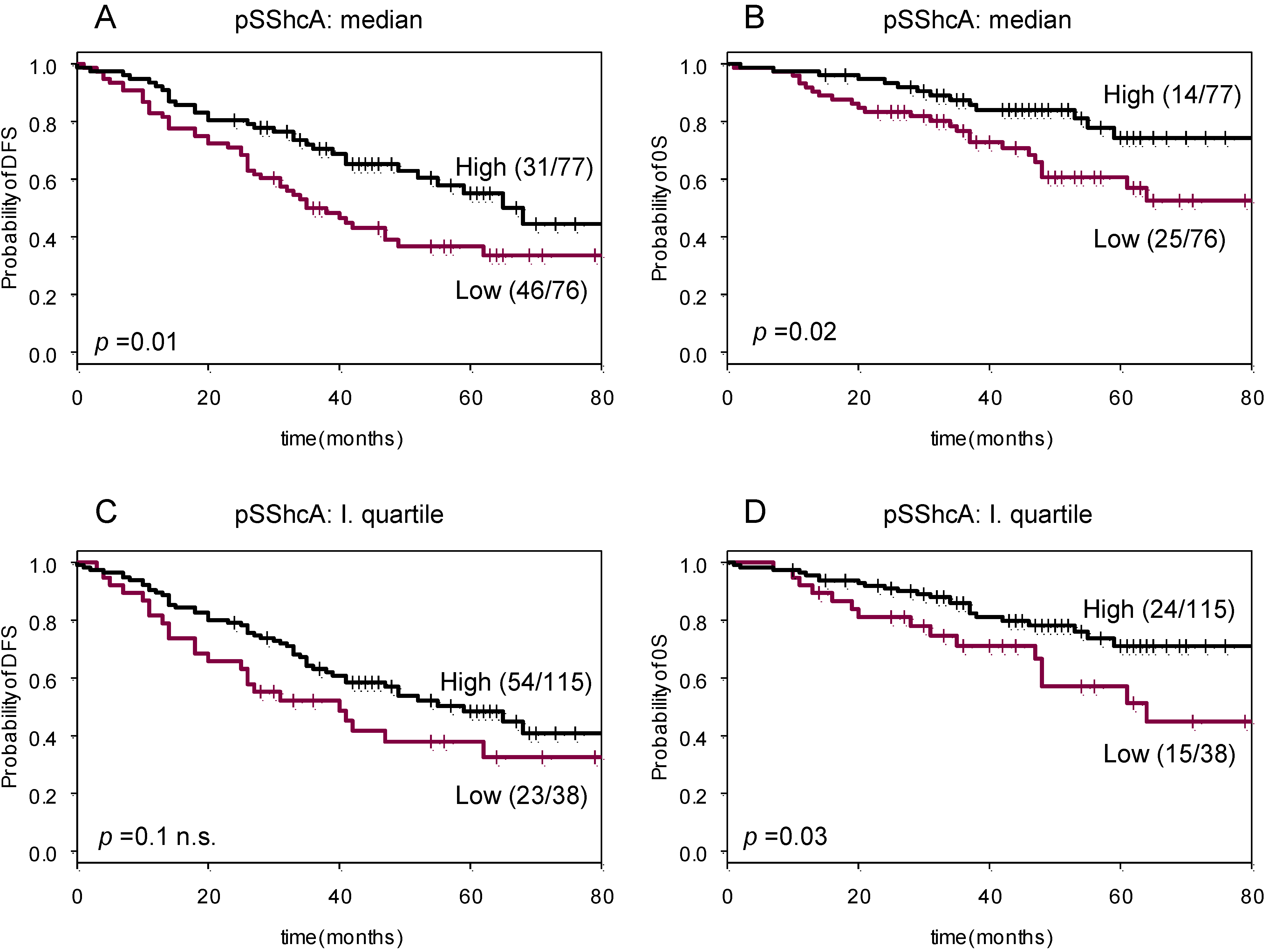
2.4. Prognostic Significance of Serine Phosphorylated ShcA

2.5. Discussion
3. Experimental
3.1. Tumor and Patient Characteristics
| Feature | Number of patients (%) | |
|---|---|---|
| Patients enrolled | 153 | |
| Age | <40 | 10 (6.5) |
| 40–60 | 88 (57.5) | |
| >60 | 55 (36) | |
| Histology type | ||
| Ductal | 104 (68) | |
| Lobular | 9 (6) | |
| Other | 40 (26) | |
| Tumor size | ||
| T1 | 39 (25) | |
| T2 | 87 (57) | |
| T3-4 | 24 (16) | |
| Unknown | 3 (2) | |
| Lymph-node status | ||
| Node-negative | 58 (38) | |
| Node-positive | 75 (49) | |
| Unknown | 20 (13) | |
| Histopathological grade | ||
| I + II | 49 (32) | |
| III | 57 (37) | |
| Not analyzed | 47 (31) | |
| Estrogen receptor (ER) | ||
| Positive (>20 fmol/mg) | 55 (36) | |
| Negative (≤20 fmol/mg) | 98 (64) | |
| Progesterone receptor (PgR) | ||
| Positive (>20 fmol/mg) | 40 (26) | |
| Negative (≤20 fmol/mg) | 113 (73) | |
| ErbB2 | ||
| Positive (>260 ng/mg) | 81 (53) | |
| Negative (≤260 ng/mg) | 72 (47) | |
3.2. Cell Lines and Tissue Preparation
3.3. Measurement of ER, PgR and ErbB-2 Protein Levels in Tumor Extracts by EIA
3.4. Immunoassay of pYShcA and PSShcA Levels
3.5. Statistical Methods
4. Conclusions
Acknowledgements
References
- Cicenas, J.; Urban, P.; Küng, W.; Vuaroqueaux, V.; Labuhn, M.; Wight, E.; Eppenberger, U.; Eppenberger-Castori, S. Increased level of phosphorylated akt measured by chemiluminescence-linked immunosorbent assay is a predictor of poor prognosis in primary breast cancer overexpressing ErbB-2. Breast Cancer Res. 2005, 7, R394–R401. [Google Scholar] [CrossRef] [Green Version]
- Cicenas, J.; Urban, P.; Vuaroqueaux, V.; Labuhn, M.; Küng, W.; Wight, E.; Mayhew, M.; Eppenberger, U.; Eppenberger-Castori, S. Phosphorylation of tyrosine 1248-ERBB2 measured by chemiluminescence-linked immunoassay is an independent predictor of poor prognosis in primary breast cancer patients. Eur. J. Cancer 2006, 42, 636–645. [Google Scholar] [CrossRef]
- Bonfini, L.; Migliaccio, L.; Pelicci, G; Lanfrancone, L.; Pelicci, P.G. Not all Shc’s roads lead to Ras. Trends Biochem. Sci. 1996, 21, 257–261. [Google Scholar]
- Marshall, M.S. Ras target proteins in eukaryotic cells. FASEB 1995, 91, 311–318. [Google Scholar]
- Salcini, AE.; McGlade, J.; Pelicci, G.; Nicoletti, I.; Pawson, TP.; Pelicci, PG. Formation of Shc–Grb2 complexes is necessary to induce neoplastic transformation by overexpression of Shc proteins. Oncogene 1994, 9, 2827–2836. [Google Scholar]
- Gotoh, N.; Toyoda, M.; Shibuya, M. Tyrosine phosphorylation sites at amino acids 239 and 240 of Shc are involved in epidermal growth factor-induced mitogenic signalling that is distinct from Ras/mitogen-activated protein kinase activation. Mol. Cell Biol. 1997, 17, 1824–1831. [Google Scholar]
- Lanfrancone, L.; Pelicci, G.; Brizzi, M.F.; Aronica, M.G.; Casciari, C.; Giuli, S.; Pegoraro, L.; Pawson, T.; Pelicci, P.G.; Arouica, M.G. Overexpression of Shc proteins potentiates the proliferative response to the granulocyte-macrophage colony-stimulating factor and recruitment of Grb2/SoS and Grb2/p140 complexes to the beta receptor subunit. Oncogene 1995, 10, 907–917. [Google Scholar]
- Lai, K.M.; Pawson, T. The ShcA phosphotyrosine docking protein sensitizes cardiovascular signalling in the mouse embryo. Genes Dev. 2000, 14, 1132–1145. [Google Scholar]
- Migliaccio, E.; Mele, S.; Salcini, A.E.; Pelicci, G.; Lai, K.M.; Superti-Furga, G.; Pawson, T.; Di Fiore, P.P.; Lanfrancone, L.; Pelicci, P.G. Opposite effects of the p52shc/p46shc and p66shc splicing isoforms on the EGF receptor-MAP kinase-fos signalling pathway. EMBO J. 1997, 16, 706–716. [Google Scholar] [CrossRef]
- Okada, S.; Kao, A.W.; Ceresa, B.P.; Blaikie, P.; Margolis, B.; Pessin, J.E. The 66-kDa Shc isoform is a negative regulator of the epidermal growth factor-stimulated mitogen-activated protein kinase pathway. J. Biol. Chem. 1997, 272, 28042–28049. [Google Scholar]
- Le, S.; Connors, T.J.; Maroney, A.C. c-Jun N-terminal kinase specifically phosphorylates p66ShcA at serine 36 in response to ultraviolet irradiation. J. Biol. Chem. 2001, 276, 48332–48336. [Google Scholar]
- Cicenas, J. The potential role of Akt phosphorylation in human cancers. Int. J. Bio. Markers 2008, 23, 1–9. [Google Scholar]
- Wu, Y.; Mohamed, H.; Chillarm, R.; Ali, I.; Clayton, S.; Slamon, D.; Vadgama, J.V. Clinical significance of Akt and HER2/neu overexpression in African-American and Latina women with breast cancer. Breast Cancer Res. 2008, 10, R3–R22. [Google Scholar] [CrossRef]
- Cicenas, J. The potential role of the EGFR/ERBB2 heterodimer in breast cancer. Expert. Opin. Ther. Pat. 2007, 17, 607–616. [Google Scholar]
- Xia, W.; Chen, J.S.; Zhou, X.; Sun, P.R.; Lee, D.F.; Liao, Y.; Zhou, B.P.; Hung, M.C. Phosphorylation/cytoplasmic localization of p21Cip1/WAF1 is associated with HER2/neu overexpression and provides a novel combination predictor for poor prognosis in breast cancer patients. Clin. Cancer Res. 2004, 10, 3815–3824. [Google Scholar] [CrossRef]
- Clarke, R.B. p27KIP1 phosphorylation by PKB/Akt leads to poor breast cancer prognosis. Breast Cancer Res. 2003, 5, 162–163. [Google Scholar] [CrossRef]
- Eppenberger-Castori, S.; Kueng, W.; Benz, C.; Caduff, R.; Varga, Z.; Bannwart, F.; Fink, D.; Dieterich, H.; Hohl, M.; Müller, H.; et al. Prognostic and predictive significance of ErbB-2 breast tumor levels measured by enzyme immunoassay. J. Clin. Oncol. 2001, 19, 645–656. [Google Scholar]
- Milde-Langosch, K.; Bamberger, A.M.; Rieck, G.; Grund, D.; Hemminger, G.; Müller, V.; Löning, T. Expression and prognostic relevance of activated extracellular-regulated kinases (ERK1/2) in breast cancer. Br. J. Cancer 2005, 92, 2206–2215. [Google Scholar] [CrossRef]
- Svensson, S.; Jirström, K.; Rydén, L.; Roos, G.; Emdin, S.; Ostrowski, M.C.; Landberg, G. ERK phosphorylation is linked to VEGFR2 expression and Ets-2 phosphorylation in breast cancer and is associated with tamoxifen treatment resistance and small tumors with good prognosis. Oncogene 2005, 24, 4370–4379. [Google Scholar] [CrossRef]
- Bergqvist, J.; Elmberger, G.; Ohd, J.; Linderholm, B.; Bjohle, J.; Hellborg, H.; Nordgren, H.; Borg, A.L.; Skoog, L.; Bergh, J. Activated ERK1/2 and phosphorylated oestrogen receptor alpha are associated with improved breast cancer survival in women treated with tamoxifen. Eur. J. Cancer 2006, 42, 1104–1112. [Google Scholar] [CrossRef]
- Schmitt, M.; Mengele, K.; Schueren, E.; Sweep, F.C.; Foekens, J.A.; Brünner, N.; Laabs, J.; Malik, A.; Harbeck, N.; European Organisation for Research and Treatment of Cancer Pathobiology Group. European Organisation for Research and Treatment of Cancer (EORTC) Pathobiology Group standard operating procedure for the preparation of human tumour tissue extracts suited for the quantitative analysis of tissue-associated biomarkers. Eur. J. Cancer 2007, 43, 835–844. [Google Scholar] [CrossRef]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Cicenas, J.; Küng, W.; Eppenberger, U.; Eppenberger-Castori, S. Increased Level of Phosphorylated ShcA Measured by Chemiluminescence-Linked Immunoassay Is a Predictor of Good Prognosis in Primary Breast Cancer Expressing Low Levels of Estrogen Receptor. Cancers 2010, 2, 153-164. https://doi.org/10.3390/cancers2010153
Cicenas J, Küng W, Eppenberger U, Eppenberger-Castori S. Increased Level of Phosphorylated ShcA Measured by Chemiluminescence-Linked Immunoassay Is a Predictor of Good Prognosis in Primary Breast Cancer Expressing Low Levels of Estrogen Receptor. Cancers. 2010; 2(1):153-164. https://doi.org/10.3390/cancers2010153
Chicago/Turabian StyleCicenas, Jonas, Willy Küng, Urs Eppenberger, and Serenella Eppenberger-Castori. 2010. "Increased Level of Phosphorylated ShcA Measured by Chemiluminescence-Linked Immunoassay Is a Predictor of Good Prognosis in Primary Breast Cancer Expressing Low Levels of Estrogen Receptor" Cancers 2, no. 1: 153-164. https://doi.org/10.3390/cancers2010153