Nanoparticles in Sentinel Lymph Node Assessment in Breast Cancer

Abstract
:1. Introduction
2. History of the Sentinel Lymph Node
3. Alternatives to SLNB for Staging of the Axilla in Breast Cancer
4. Nanoparticles
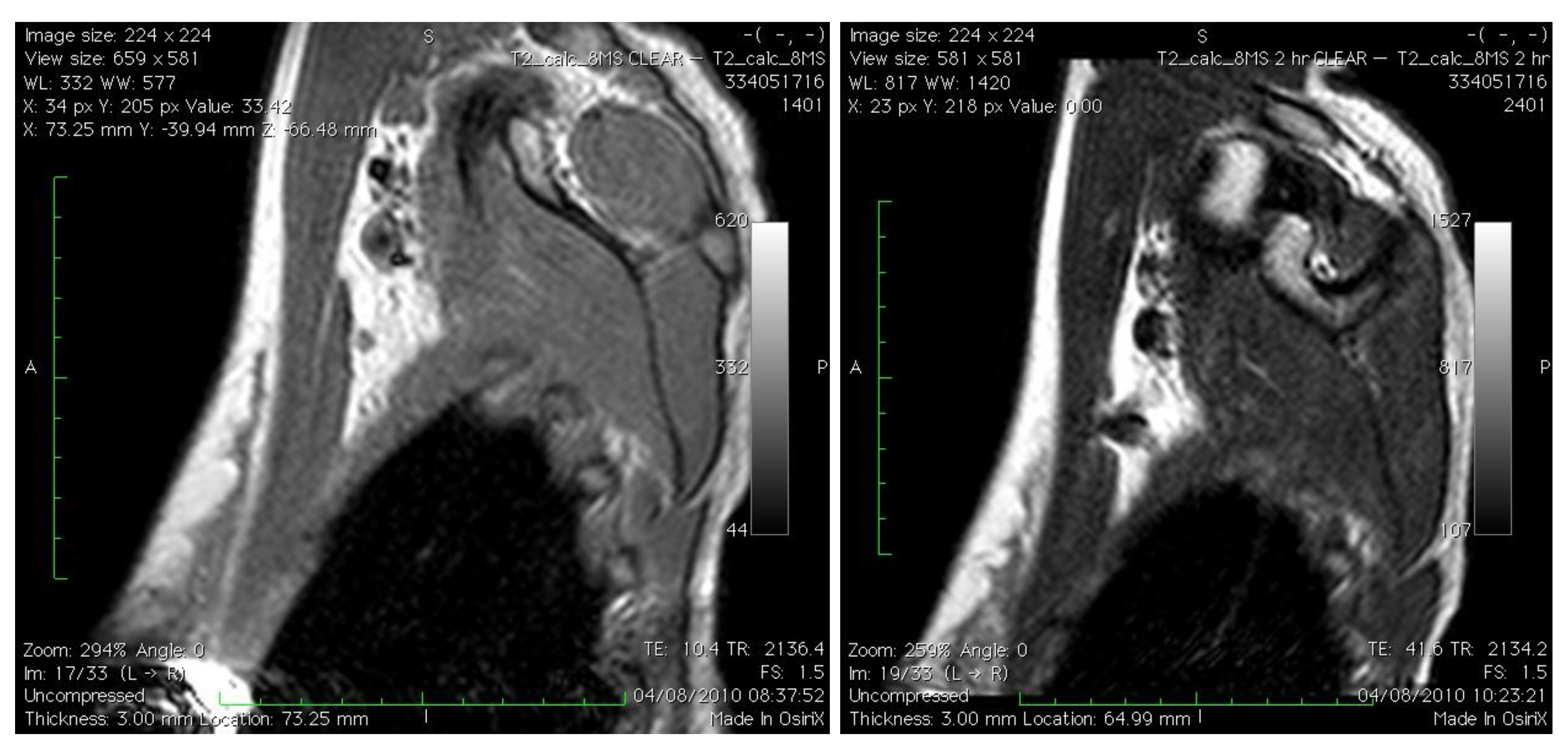
4.1. Pre-Operative (Non-Invasive) Staging of the Axillary Sentinel Lymph Node Using Nanoparticles

{kind=link}
| Group | Description |
|---|---|
| 1 | Normal morphology with uniform or central signal drop (categorized as normal) |
| 2 | Normal morphology without or with partial signal drop (categorized as partial or total invasion) |
| 3 | Focal or global volume increase without or with partial signal drop (characterized as partial or total invasion |
4.2. Intraoperative Identification of the Axillary SLN

4.3. In vivo Treatment of the Axillary SLN
5. Challenges in the Clinical Translation of Novel Nanoparticles
6. Conclusions
References
- Cabanas, R.M. An approach for the treatment of penile carcinoma. Cancer 1977, 39, 456–466. [Google Scholar] [CrossRef]
- Morton, D.L.; Wen, D.R.; Wong, J.H.; Economou, J.S.; Cagle, L.A.; Storm, F.K.; Foshag, L.J.; Cochran, A.J. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch. Surg. 1992, 127, 392–399. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Kirgan, D.M.; Guenther, J.M.; Morton, D.L. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann. Surg. 1994, 220, 391-398; discussion 398-401. [Google Scholar] [CrossRef]
- Giuliano, A.E. Sentinel lymphadenectomy in primary breast carcinoma: An alternative to routine axillary dissection. J. Surg. Oncol. 1996, 62, 75–77. [Google Scholar] [CrossRef]
- van der Veen, H.; Hoekstra, O.S.; Paul, M.A.; Cuesta, M.A.; Meijer, S. Gamma probe-guided sentinel node biopsy to select patients with melanoma for lymphadenectomy. Br. J. Surg. 1994, 81, 1769–1770. [Google Scholar] [CrossRef]
- Botteri, E.; Rotmensz, N.; Sangalli, C.; Toesca, A.; Peradze, N.; De Oliveira Filho, H.R.; Sagona, A.; Intra, M.; Veronesi, P.; Galimberti, V.; Luini, A.; Veronesi, U.; Gentilini, O. Unavoidable mastectomy for ipsilateral breast tumour recurrence after conservative surgery: Patient outcome. Ann. Oncol. 2009, 20, 1008–1012. [Google Scholar] [CrossRef]
- Krag, D.N.; Weaver, D.L.; Alex, J.C.; Fairbank, J.T. Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg. Oncol. 1993, 2, 335-339; discussion 340. [Google Scholar] [CrossRef]
- Albertini, J.J.; Lyman, G.H.; Cox, C.; Yeatman, T.; Balducci, L.; Ku, N.; Shivers, S.; Berman, C.; Wells, K.; Rapaport, D.; Shons, A.; Horton, J.; Greenberg, H.; Nicosia, S.; Clark, R.; Cantor, A.; Reintgen, D.S. Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA 1996, 276, 1818–1822. [Google Scholar] [CrossRef]
- Lucci, A.; McCall, L.M.; Beitsch, P.D.; Whitworth, P.W.; Reintgen, D.S.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; Hunt, K.K.; Giuliano, A.E. Surgical complications associated with sentinel lymph node dissection (slnd) plus axillary lymph node dissection compared with slnd alone in the american college of surgeons oncology group trial z0011. J. Clin. Oncol. 2007, 25, 3657–3663. [Google Scholar] [CrossRef]
- Blanchard, D.K.; Donohue, J.H.; Reynolds, C.; Grant, C.S. Relapse and morbidity in patients undergoing sentinel lymph node biopsy alone or with axillary dissection for breast cancer. Arch. Surg. 2003, 138, 482-487; discussion 487-488. [Google Scholar] [CrossRef]
- Clarke, D.; Newcombe, R.G.; Mansel, R.E. The learning curve in sentinel node biopsy: The almanac experience. Ann. Surg. Oncol. 2004, 11, 211S–215S. [Google Scholar]
- Veronesi, U.; Paganelli, G.; Viale, G.; Galimberti, V.; Luini, A.; Zurrida, S.; Robertson, C.; Sacchini, V.; Veronesi, P.; Orvieto, E.; De Cicco, C.; Intra, M.; Tosi, G.; Scarpa, D. Sentinel lymph node biopsy and axillary dissection in breast cancer: Results in a large series. J. Natl. Cancer Inst. 1999, 91, 368–373. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Sneige, N.; Bedi, D.G.; Edieken, B.S.; Fornage, B.D.; Kuerer, H.M.; Singletary, S.E.; Hunt, K.K. Role of ultrasound-guided fine-needle aspiration of indeterminate and suspicious axillary lymph nodes in the initial staging of breast carcinoma. Cancer 2002, 95, 982–988. [Google Scholar] [CrossRef]
- Swinson, C.; Ravichandran, D.; Nayagam, M.; Allen, S. Ultrasound and fine needle aspiration cytology of the axilla in the pre-operative identification of axillary nodal involvement in breast cancer. Eur. J. Surg. Oncol. 2009, 35, 1152–1157. [Google Scholar] [CrossRef]
- Sianesi, M.; Ceci, G.; Ghirarduzzi, A.; Del Rio, P.; Guazzi, A.; Pisanelli, B.; Martella, E.; Ardizzoni, A.; Di Blasio, B.; Arcuri, M.F. Use of axillary ultrasonography in breast cancer: A useful tool to reduce sentinel node procedures. Ann. Ital. Chir. 2009, 80, 315–318. [Google Scholar]
- Kim, J.; Lee, J.; Chang, E.; Kim, S.; Suh, K.; Sul, J.; Song, I.; Kim, Y.; Lee, C. Selective sentinel node plus additional non-sentinel node biopsy based on an fdg-pet/ct scan in early breast cancer patients: Single institutional experience. World J. Surg. 2009, 33, 943–949. [Google Scholar] [CrossRef]
- Dessureault, S.; Koven, I.; Reilly, R.M.; Couture, J.; Schmocker, B.; Damani, M.; Kirsh, J.; Ichise, M.; Sidlofsky, S.; McEwan, A.J.; Boniface, G.; Stern, H.; Gallinger, S. Pre-operative assessment of axillary lymph node status in patients with breast adenocarcinoma using intravenous 99mtechnetium mab-170h.82 (tru-scint ad). Breast Cancer Res. Treat 1997, 45, 29–37. [Google Scholar]
- Feynman, R. There's plenty of room at the bottom. Available online: http://www.zyvex.com/nanotech/feynman.html (accessed on 16 November 2010).
- Johnson, L.; Gunasekera, A.; Douek, M. Applications of nanotechnology in cancer. Discov. Med. 2010, 9, 374–379. [Google Scholar]
- Maeda, H. The enhanced permeability and retention (epr) effect in tumor vasculature: The key role of tumor-selective macromolecular drug targeting. Adv. Enzyme Regul. 2001, 41, 189–207. [Google Scholar] [CrossRef]
- Sumer, B.; Gao, J. Theranostic nanomedicine for cancer. Nanomedicine (Lond) 2008, 3, 137–140. [Google Scholar] [CrossRef]
- Jain, R.; Dandekar, P.; Patravale, V. Diagnostic nanocarriers for sentinel lymph node imaging. J. Control. Release 2009, 138, 90–102. [Google Scholar] [CrossRef]
- Corot, C.; Robert, P.; Idee, J.M.; Port, M. Recent advances in iron oxide nanocrystal technology for medical imaging. Adv. Drug Deliv. Rev. 2006, 58, 1471–1504. [Google Scholar] [CrossRef]
- Ferrari, M. Cancer nanotechnology: Opportunities and challenges. Nat. Rev. Cancer 2005, 5, 161–171. [Google Scholar] [CrossRef]
- Michel, S.C.; Keller, T.M.; Frohlich, J.M.; Fink, D.; Caduff, R.; Seifert, B.; Marincek, B.; Kubik-Huch, R.A. Preoperative breast cancer staging: Mr imaging of the axilla with ultrasmall superparamagnetic iron oxide enhancement. Radiology 2002, 225, 527–536. [Google Scholar] [CrossRef]
- Koh, D.M.; Brown, G.; Temple, L.; Blake, H.; Raja, A.; Toomey, P.; Bett, N.; Farhat, S.; Norman, A.R.; Daniels, I.; Husband, J.E. Distribution of mesorectal lymph nodes in rectal cancer: In vivo mr imaging compared with histopathological examination. Initial observations. Eur. Radiol. 2005, 15, 1650–1657. [Google Scholar] [CrossRef]
- Stadnik, T.W.; Everaert, H.; Makkat, S.; Sacre, R.; Lamote, J.; Bourgain, C. Breast imaging. Preoperative breast cancer staging: Comparison of uspio-enhanced mr imaging and 18f-fluorodeoxyglucose (fdc) positron emission tomography (pet) imaging for axillary lymph node staging--initial findings. Eur. Radiol. 2006, 16, 2153–2160. [Google Scholar] [CrossRef]
- Joshi, T.; Pankhurst, Q.; Hattersley, S.; Brazdeikis, A.; Hall-Craggs, M.; De Vita, E.; Bainbridge, A.; Sainsbury, R.; Sharma, A.; Douek, M. Magnetic nanoparticles for detecting sentinel lymph nodes. Eur. J. Surg. Oncol. 2007, 1135. [Google Scholar]
- Song, K.H.; Kim, C.; Cobley, C.M.; Xia, Y.; Wang, L.V. Near-infrared gold nanocages as a new class of tracers for photoacoustic sentinel lymph node mapping on a rat model. Nano. Lett. 2009, 9, 183–188. [Google Scholar] [CrossRef]
- Cuenca, A.G.; Jiang, H.; Hochwald, S.N.; Delano, M.; Cance, W.G.; Grobmyer, S.R. Emerging implications of nanotechnology on cancer diagnostics and therapeutics. Cancer 2006, 107, 459–466. [Google Scholar] [CrossRef]
- Surguladze, B.; Zhorzoliani, R.; Tskitishvili, T. Novel method of sentinel lymph node detection in malignant tumors using preparation 'unimag'. Breast Cancer Res. 2007, 9 (Suppl 1), 15. [Google Scholar] [CrossRef]
- Sever, A.; Jones, S.; Cox, K.; Weeks, J.; Mills, P.; Jones, P. Preoperative localization of sentinel lymph nodes using intradermal microbubbles and contrast-enhanced ultrasonography in patients with breast cancer. Br. J. Surg. 2009, 96, 1295–1299. [Google Scholar] [CrossRef]
- Kim, J.S.; Yoon, T.J.; Yu, K.N.; Kim, B.G.; Park, S.J.; Kim, H.W.; Lee, K.H.; Park, S.B.; Lee, J.K.; Cho, M.H. Toxicity and tissue distribution of magnetic nanoparticles in mice. Toxicol. Sci. 2006, 89, 338–347. [Google Scholar]
- Jeon, Y.H.; Kim, Y.H.; Choi, K.; Piao, J.Y.; Quan, B.; Lee, Y.S.; Jeong, J.M.; Chung, J.K.; Lee, D.S.; Lee, M.C.; Lee, J.; Chung, D.S.; Kang, K.W. In vivo imaging of sentinel nodes using fluorescent silica nanoparticles in living mice. Mol. Imag. Biol. 2010, 12, 155–162. [Google Scholar] [CrossRef]
- Ballou, B.; Ernst, L.A.; Andreko, S.; Harper, T.; Fitzpatrick, J.A.; Waggoner, A.S.; Bruchez, M.P. Sentinel lymph node imaging using quantum dots in mouse tumor models. Bioconjug. Chem. 2007, 18, 389–396. [Google Scholar] [CrossRef]
- Gopee, N.V.; Roberts, D.W.; Webb, P.; Cozart, C.R.; Siitonen, P.H.; Warbritton, A.R.; Yu, W.W.; Colvin, V.L.; Walker, N.J.; Howard, P.C. Migration of intradermally injected quantum dots to sentinel organs in mice. Toxicol. Sci. 2007, 98, 249–257. [Google Scholar] [CrossRef]
- Robe, A.; Pic, E.; Lassalle, H.P.; Bezdetnaya, L.; Guillemin, F.; Marchal, F. Quantum dots in axillary lymph node mapping: Biodistribution study in healthy mice. BMC Cancer 2008, 8, 111. [Google Scholar] [CrossRef]
- Hama, Y.; Koyama, Y.; Urano, Y.; Choyke, P.L.; Kobayashi, H. Two-color lymphatic mapping using ig-conjugated near infrared optical probes. J. Invest. Dermatol. 2007, 127, 2351–2356. [Google Scholar] [CrossRef]
- Tomalia, D.A.; Reyna, L.A.; Svenson, S. Dendrimers as multi-purpose nanodevices for oncology drug delivery and diagnostic imaging. Biochem. Soc. Trans. 2007, 35, 61–67. [Google Scholar] [CrossRef]
- Koyama, Y.; Talanov, V.S.; Bernardo, M.; Hama, Y.; Regino, C.A.; Brechbiel, M.W.; Choyke, P.L.; Kobayashi, H. A dendrimer-based nanosized contrast agent dual-labeled for magnetic resonance and optical fluorescence imaging to localize the sentinel lymph node in mice. J. Magn. Reson. Imag. 2007, 25, 866–871. [Google Scholar] [CrossRef]
- Galanzha, E.I.; Kokoska, M.S.; Shashkov, E.V.; Kim, J.-W.; RTuchin, V.V.; Zharov, V.P. In vivo fiber-based milticolor photoacoustic detection and photothermal purging of metastasis in sentinel lymph nodes targeted by nanoparticles. J. Biophotonics 2009, 528–539. [Google Scholar]
- Farquhar, C.M.; Stryer, D.; Slutsky, J. Translating research into practice: The future ahead. Int. J. Qual. Health Care 2002, 14, 233–249. [Google Scholar] [CrossRef]
- Bradley, E.H.; Webster, T.R.; Baker, D.; Schlesinger, M.; Inouye, S.K.; Barth, M.C.; Lapane, K.L.; Lipson, D.; Stone, R.; Koren, M.J. Translating research into practice: Speeding the adoption of innovative health care programs. Issue Brief (Commonw Fund) 2004, 1–12. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Johnson, L.; Charles-Edwards, G.; Douek, M. Nanoparticles in Sentinel Lymph Node Assessment in Breast Cancer. Cancers 2010, 2, 1884-1894. https://doi.org/10.3390/cancers2041884
Johnson L, Charles-Edwards G, Douek M. Nanoparticles in Sentinel Lymph Node Assessment in Breast Cancer. Cancers. 2010; 2(4):1884-1894. https://doi.org/10.3390/cancers2041884
Chicago/Turabian StyleJohnson, Laura, Geoff Charles-Edwards, and Michael Douek. 2010. "Nanoparticles in Sentinel Lymph Node Assessment in Breast Cancer" Cancers 2, no. 4: 1884-1894. https://doi.org/10.3390/cancers2041884