Avid 18F-FDG Uptake in Idiopathic Tumoral Calcinosis Mimicking Lymph Node Metastasis


1
Department of Nuclear Medicine, Aalborg University Hospital, Hobrovej 18-22, DK-9000 Aalborg, Denmark
2
Department of Clinical Medicine, Aalborg University, DK-9000 Aalborg, Denmark
*
Author to whom correspondence should be addressed.
Diagnostics 2017, 7(4), 60; https://doi.org/10.3390/diagnostics7040060
Submission received: 7 September 2017
/
Revised: 7 December 2017
/
Accepted: 11 December 2017
/
Published: 13 December 2017
(This article belongs to the Special Issue Functional and Molecular Imaging of Kidney and Urogenital Disease)
{kind=link}
Abstract
:Tumoral calcinosis is a benign condition characterized by periarticular calcified lesions that is frequently observed in patients with chronic renal failure. Tumoral calcinosis often presents with subcutaneous masses and joint swelling. We present a case of tumoral calcinosis with dramatically increased 18F-fluoro-2-deoxy-d-glucose (18F-FDG) uptake on positron emission tomography/computed tomography (PET/CT) that mimicked lymphoma or lymph node metastases.
1. Introduction
Tumoral calcinosis may occur in all tissues [1]. This condition is a rare complication of chronic renal failure, and the genesis of the disease is related to high levels of calcium and phosphorus products and/or advanced secondary hyperparathyroidism after long-term dialysis [2,3]. High PTH (parathyroid hormone) can cause very high levels of plasma calcium. Additionally, extracellular phosphate concentration is often increased, secondary to kidney malfunction; hence, phosphate cannot be properly excreted. Therefore, the body fluids become supersaturated with calcium and phosphate, and calcium phosphate crystals begin to be deposited in tissue [4].
Patients often present with localized swelling around joints and reduced mobility. The most common locations of tumoral calcinosis are the hips, elbows, shoulders, feet, and wrists [5]. The treatment of tumoral calcinosis involves eliminating the underlying causes of either hyperphosphatemia or hypercalcemia and may include renal transplantation or parathyroidectomy [6].
18F-Fludeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) is used for the evaluation and initial staging of lymphomas. This method can detect more lesions than CT-scans can due to its ability to detect metabolic changes before structural changes become visible [7].
2. Case Report
The study subject is a 57-year-old man with chronic terminal kidney disease due to focal segmental glomerulosclerosis (FSGS) diagnosed in 1997, and secondary/tertiary hyperparathyroidism with severe hyperphosphatemia. His blood values remained stable for 18 years after the diagnosis of FSGS. However, since 2015 he developed increasing uremia with serum creatinine rose from 350 to 550 corresponding to a glomerular filtration rate of approximately 10 mL/min, but dialysis was not yet required. During the same time span PTH increased from 25 to 100 pmol/L with concomitant fluctuating values for phosphate (2.5–3.5 mmol/L). The total plasma Ca2+ level remained within the normal range during the entire period from diagnosis to present.
The patient presented with complaints of rapid development of palpable subcutaneous swellings in his right shoulder, axilla, and on the right side of his neck with neither pain nor sensory disturbances for 7–10 days. Apart from fatigue, no B-symptoms, fever or signs of upper respiratory tract infection were present, but several palpable lymph nodes on the right side of the neck along the sternocleidomastoid muscle and in the right axilla were noted. Blood samples revealed slightly elevated infection parameters. The patient was referred to the Department of Hematology at Aalborg University Hospital, where malignant lymphoma was suspected.
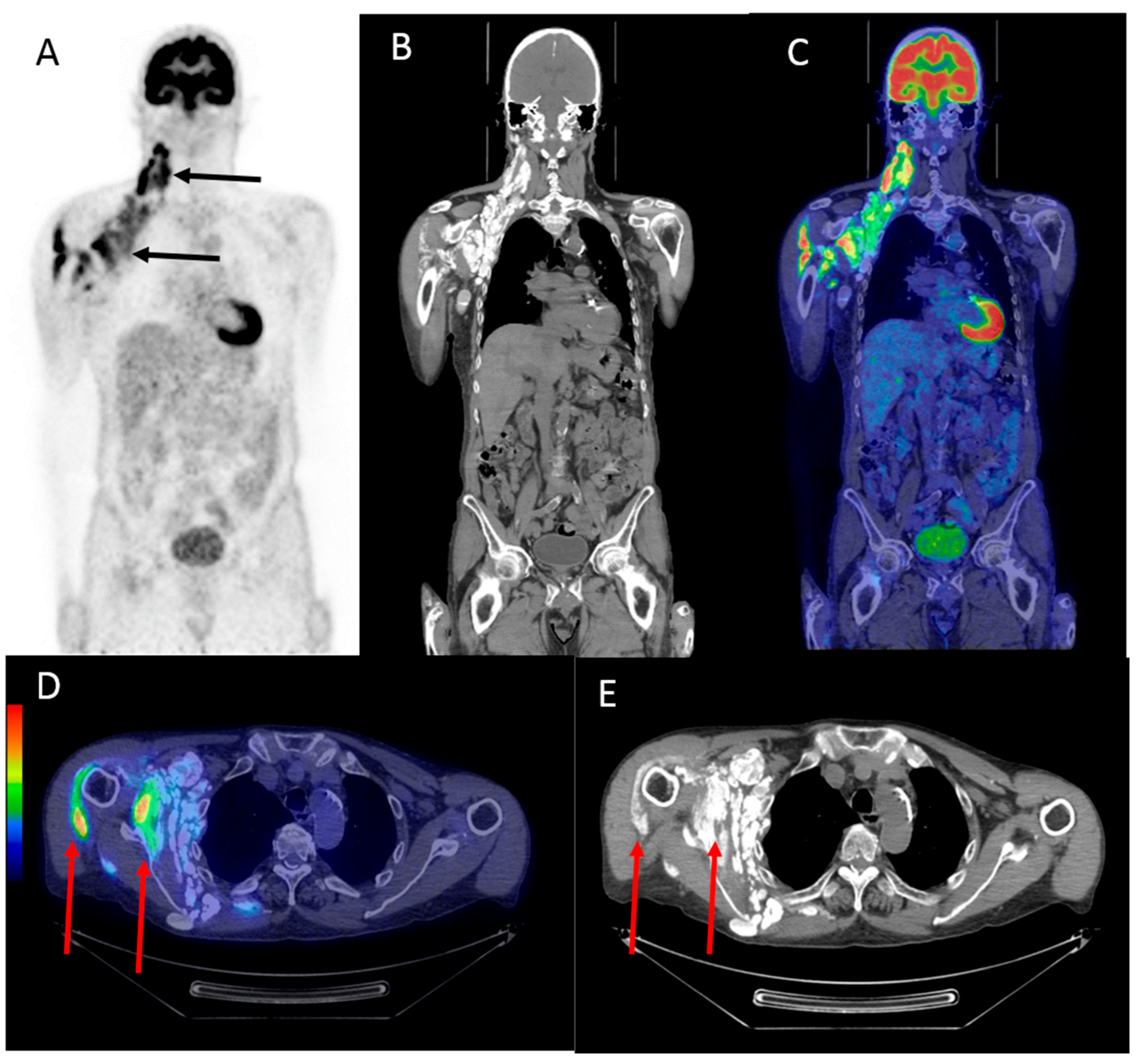
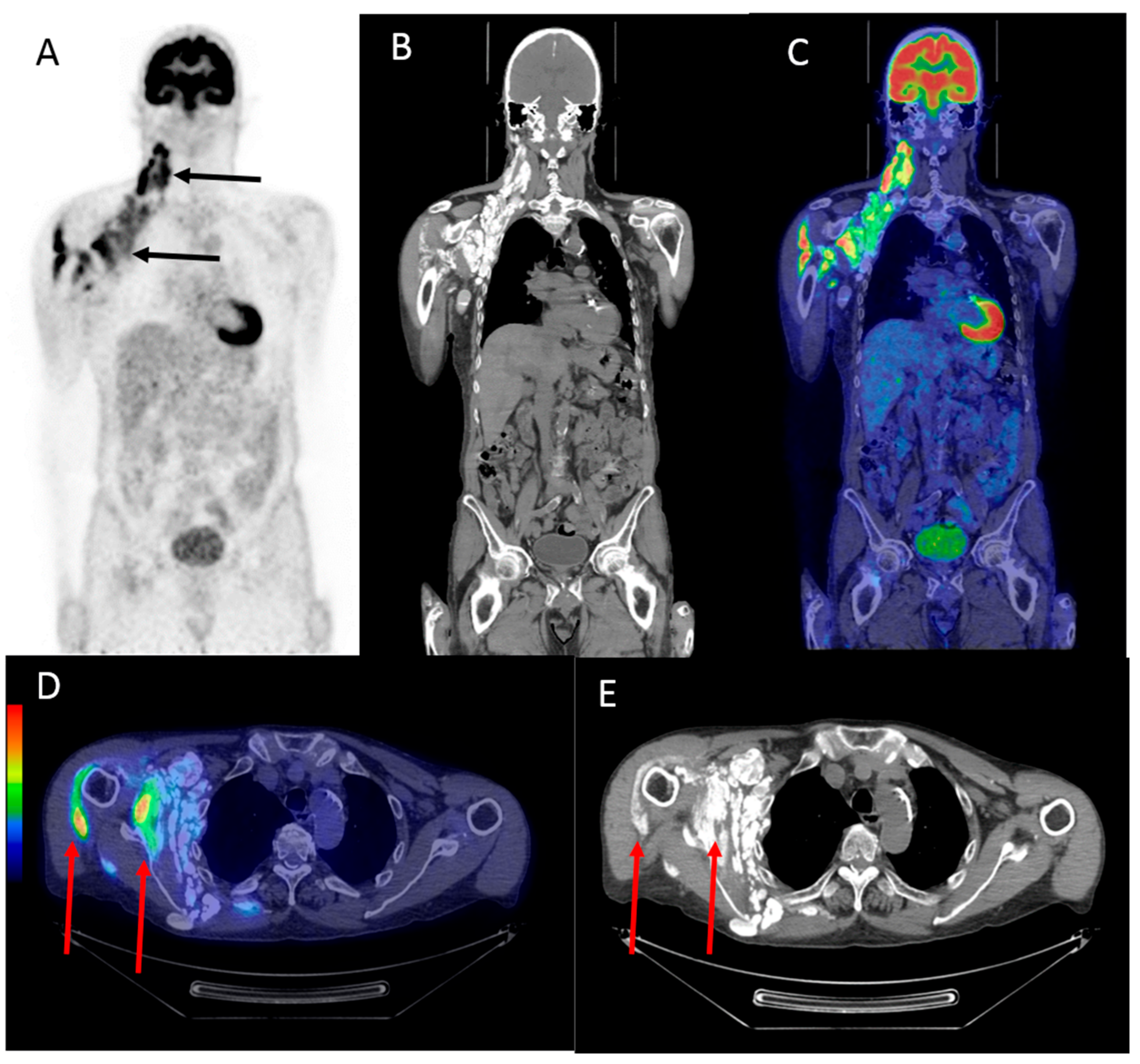
A lymph node biopsy from the right side of the neck revealed cystic material with calcification and no malignant cells. The patient then underwent a 18F-FDG PET/CT scan, which showed multiple sites of severe calcification of the right side of the neck and in the right axilla with increased 18F-FDG uptake that mimicked multiple lymph node metastases (Figure 1). Additional avid 18F-FDG uptake was observed in the shoulder muscles. To reach a final diagnosis, a lymphadenectomy was performed. Histopathology revealed fat and connective tissue as well as calcifications with surrounding foreign body reaction/inflammation. There were no signs of malignancy or premalignacy but histology revealed multiple calcifications, most likely due to the disturbed calcium-phosphate balance resulting from the patient’s chronic renal failure. Additional culturing of the cyst content did not reveal any infectious agents. Apart from physiotherapy to improve the minor movement limitations of his right arm, no other treatment was required.
3. Discussion
18F-FDG uptake in tumoral calcinosis has only been sporadically described. Okuyama et al. reported a case of tumoral calcinosis in the right cheek with increased 18F-FDG uptake [8]. Additionally, Liu reported a case of tumoral calcinosis in the neck, elbow, wrist, hand, thighs, perineum, and paraspinal muscles with increased uptake on 18F-FDG PET/CT [5]. The raised PTH causing the disturbances in calcium-homeostasis and subsequent tumoral calcinosis can also be secondary to a PTH-producing tumor [9].
In the present case the patient suffered from chronic renal failure, and the histology of the removed lymph nodes revealed extensive foreign body reaction/inflammation. This may explain the increased 18F-FDG-uptake in and around the calcified areas. During chronic stages of soft tissue calcification less inflammation is presented and subsequently less—if any—18F-FDG-uptake would be expected during a chronic situation. Tumoral calcinosis is a rare condition and may mimic lymphoma or lymph node metastases when it presents as palpable masses; this is further supported when the masses exhibit high 18F-FDG uptake. However, the association of calcifications in the muscles in a patient with chronic renal failure should raise the attention of the physician interpreting the PET/CT images.
Acknowledgments
An unrestricted fund was received from the Danielsen Foundation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tezelamn, S.; Siperstein, A.E.; Duh, Q.Y.; Clark, O.H. Tumoral calcinosis Controversies on the etiology and alternatives in the treatment. Arch. Surg. 1993, 128, 737–744. [Google Scholar] [CrossRef]
- Binnani, P.; Aggarwal, V.; Bahadur, M.M.; Fulara, N. Tumoral calcinosis (Teutschlander disease) in a dialysis patient. Indian J. Nephrol. 2008, 18, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Grellier, J.-F.; Lussato, D.; Queneau, M.; Guernou, M.; Songy, B. Secondary Hyperparathyroidism with “Superscan-Like” Hypermetabolic FDG PET/CT Pattern. Clin. Nucl. Med. 2015, 40, 888–889. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E. Guyton and Hall Textbook of Medical Physiology; W.B. Saunders: Philadelphia, PA, USA, 2016. [Google Scholar]
- Liu, Y. Scintigraphic Images of Massive Tumoral Calcinosis. Clin. Nucl. Med. 2016, 41, 504–505. [Google Scholar] [CrossRef] [PubMed]
- Olsen, K.M.; Chew, F.S. Tumoral Calcinosis: Pearls polemics and alternative possibilities. Radiographics 2006, 26, 871–885. [Google Scholar] [CrossRef] [PubMed]
- D’souza, M.; Jaimini, A.; Bansal, A.; Tripathi, M.; Sharma, R.; Mondal, A.; Tripathi, R.P. FDG-PET/CT in lymphoma. Indian J. Radiol. Imaging 2013, 23, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, C.; Kubota, T.; Matsushima, S.; Ushijima, Y.; Nishimura, T. Intense F-18 FDG accumulation idiopathic tumoral calcinosis. Clin. Nucl. Med. 2009, 34, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, K.K.; Karunanithi, S.; Jain, S.; Kumar, R. Ovarian carcinoma producing parathyroid hormone-related protein causing hypercalcemia and metastatic calcification detected on (18)F-FDG PET-CT. Indian J. Nucl. Med. 2013, 28, 237–239. [Google Scholar] [PubMed]
Figure 1.
The maximum intensity projection (MIP) of the 18F-Fludeoxyglucose (18F-FDG) positron emission tomography (PET) image in the anterior view (A) showing multiple lesions with high 18F-FDG uptake located on the right side of the neck, around the right shoulder, and in the right axillar region (black arrows). A coronal computed tomography (CT) image (B) and a fused coronal image (C) of the head, neck, and upper body showing the same regions with high 18F-FDG uptake seen in the anterior view (A). Fused transversal images (D) and transversal CT images (E) showing the intramuscular high 18F-FDG uptake in the right axillary region (red arrows).
Figure 1.
The maximum intensity projection (MIP) of the 18F-Fludeoxyglucose (18F-FDG) positron emission tomography (PET) image in the anterior view (A) showing multiple lesions with high 18F-FDG uptake located on the right side of the neck, around the right shoulder, and in the right axillar region (black arrows). A coronal computed tomography (CT) image (B) and a fused coronal image (C) of the head, neck, and upper body showing the same regions with high 18F-FDG uptake seen in the anterior view (A). Fused transversal images (D) and transversal CT images (E) showing the intramuscular high 18F-FDG uptake in the right axillary region (red arrows).
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Strandberg, J.; Zacho, H.D. Avid 18F-FDG Uptake in Idiopathic Tumoral Calcinosis Mimicking Lymph Node Metastasis. Diagnostics 2017, 7, 60. https://doi.org/10.3390/diagnostics7040060
AMA Style
Strandberg J, Zacho HD. Avid 18F-FDG Uptake in Idiopathic Tumoral Calcinosis Mimicking Lymph Node Metastasis. Diagnostics. 2017; 7(4):60. https://doi.org/10.3390/diagnostics7040060
Chicago/Turabian StyleStrandberg, Jesper, and Helle D. Zacho. 2017. "Avid 18F-FDG Uptake in Idiopathic Tumoral Calcinosis Mimicking Lymph Node Metastasis" Diagnostics 7, no. 4: 60. https://doi.org/10.3390/diagnostics7040060
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.