Genetically Guided Statin Therapy on Statin Perceptions, Adherence, and Cholesterol Lowering: A Pilot Implementation Study in Primary Care Patients


Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
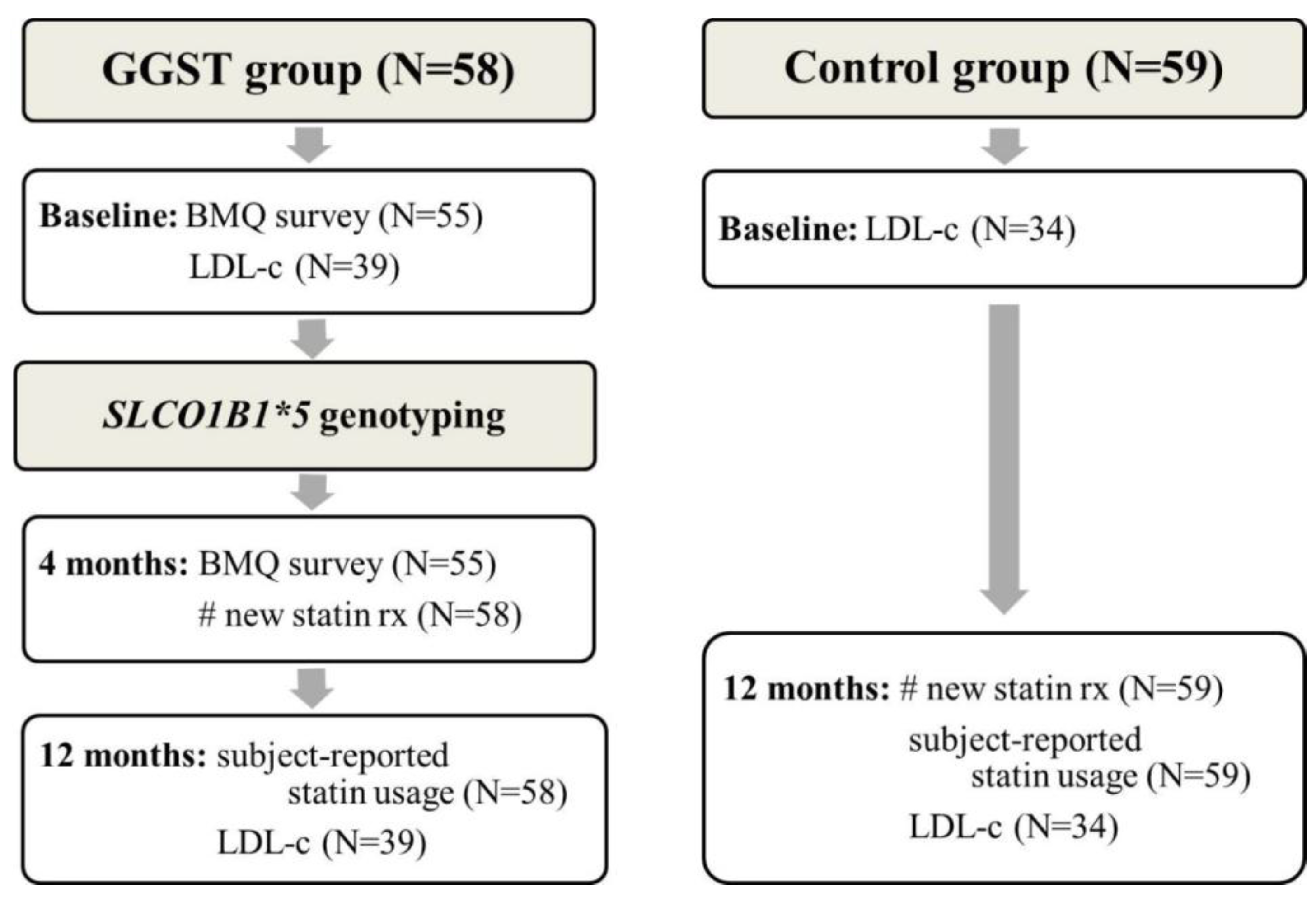

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | GGST (N = 58) | Control (N = 59) | p* |
|---|---|---|---|
| Age (SD) | 63.6 (9.0) | 63.6 (13.3) | 0.98 |
| Sex, male (%) | 21 (36.2) | 14 (23.7) | 0.16 |
| Race, white (%) | 46 (79.3) | 38 (64.4) | 0.10 |
| BMI (SD) | 30.4 (5.3) | 32.2 (9.7) | 0.22 |
| History of smoking (%) | 11 (19.0) | 16 (27.1) | 0.38 |
| Number of medical comorbidities (SD) | 3.8 (1.6) | 3.6 (1.2) | 0.41 |
| Total cholesterol, mg/dL (SD), N = 98 | 217.3 (57.0) | 198.2 (42.6) | 0.06 |
| HDL-c, mg/dL (SD), N = 98 | 51.0 (12.7) | 49.9 (13.4) | 0.69 |
| LDL-c, mg/dL (SD), N = 99 | 146.4 (51.9) | 122.8 (35.6) | 0.009 |
| NCEP goal at baseline (%), N = 99 | 16 (44.4) | 20 (55.6) | 0.25 |
| Clinic, Pickett Road (%) | 54 (93.1) | 57 (96.6) | 0.44 |
2.1.1. Change in the Beliefs about Medications Questionnaire (BMQ) from Baseline to Four Months
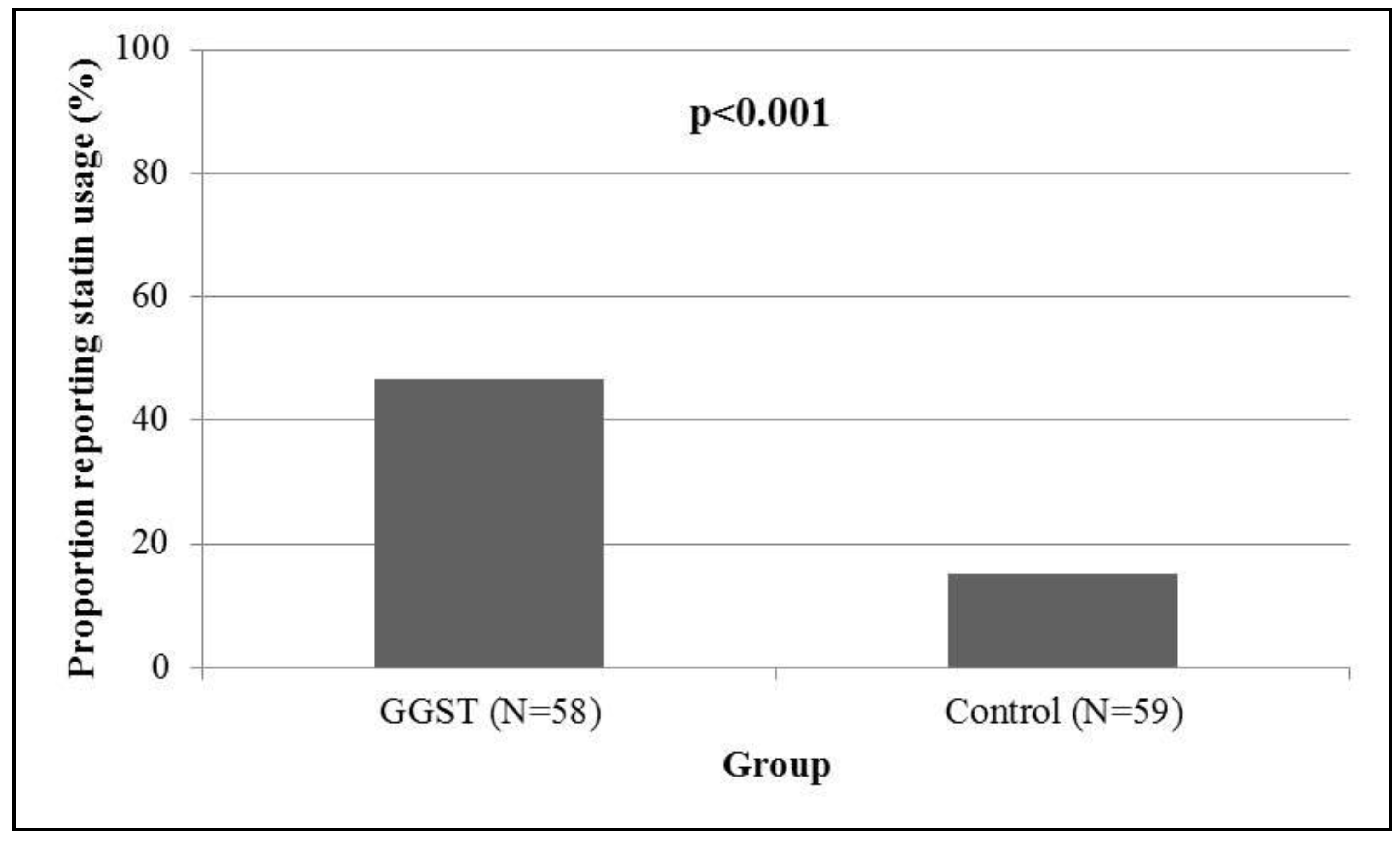
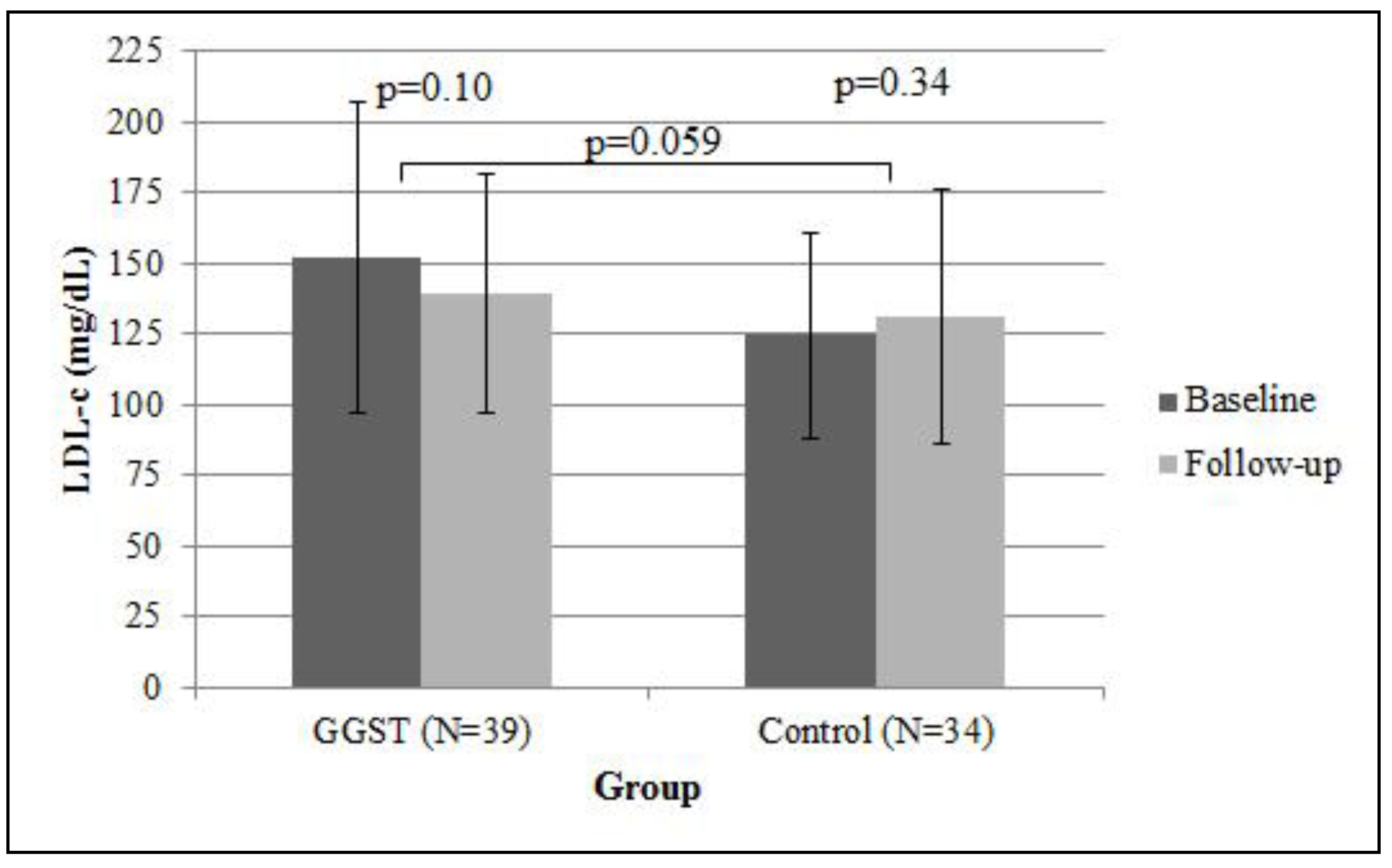
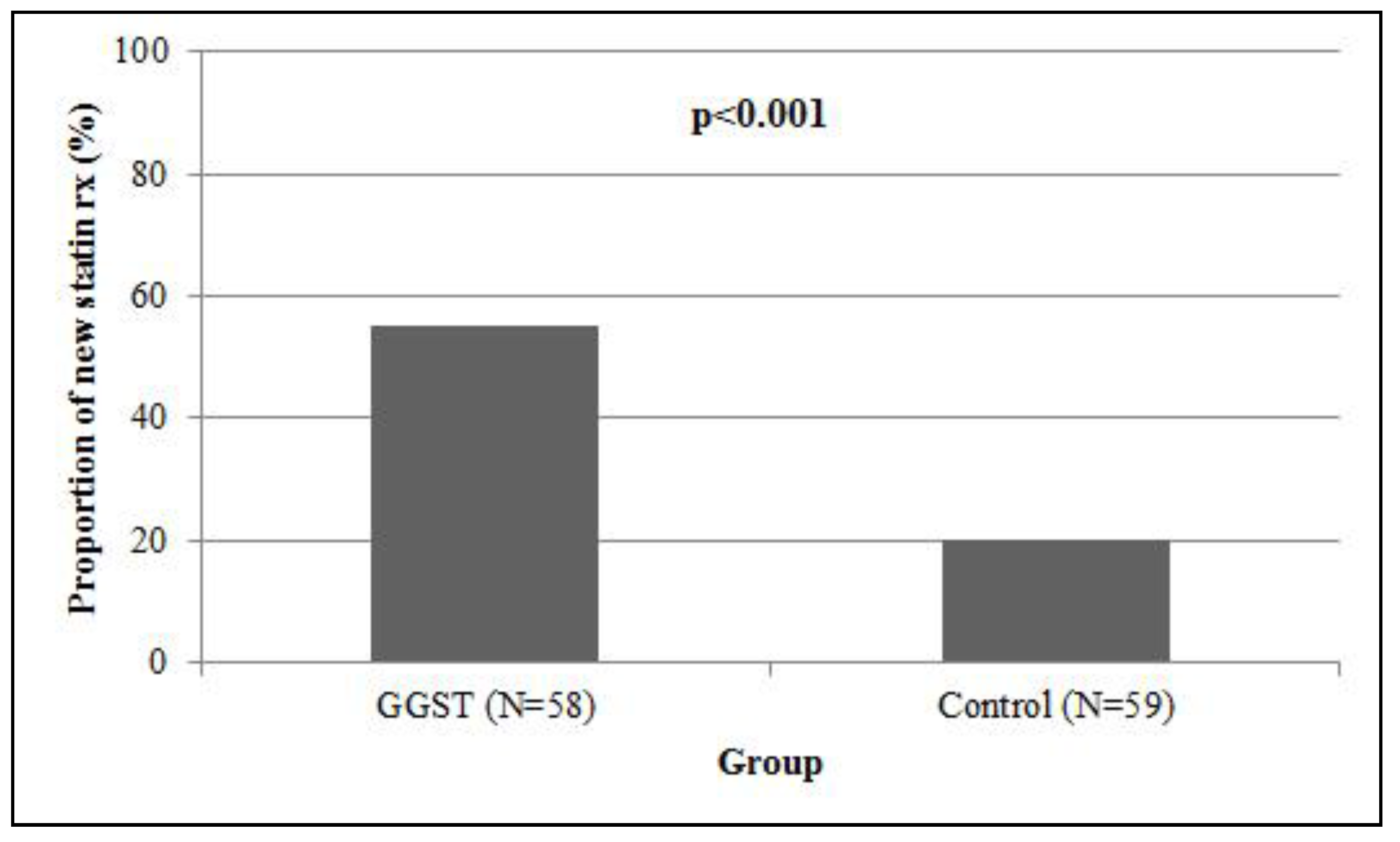
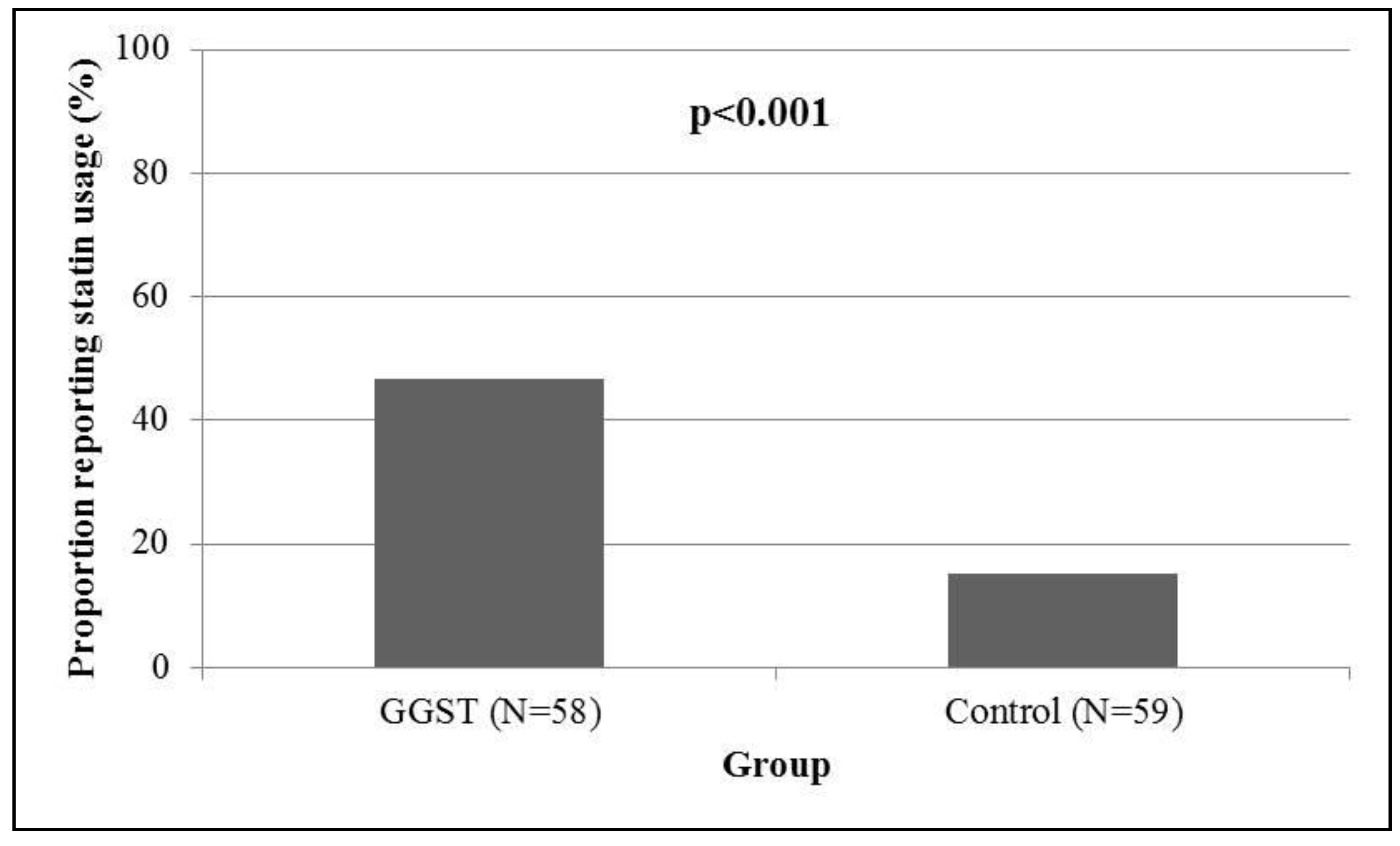
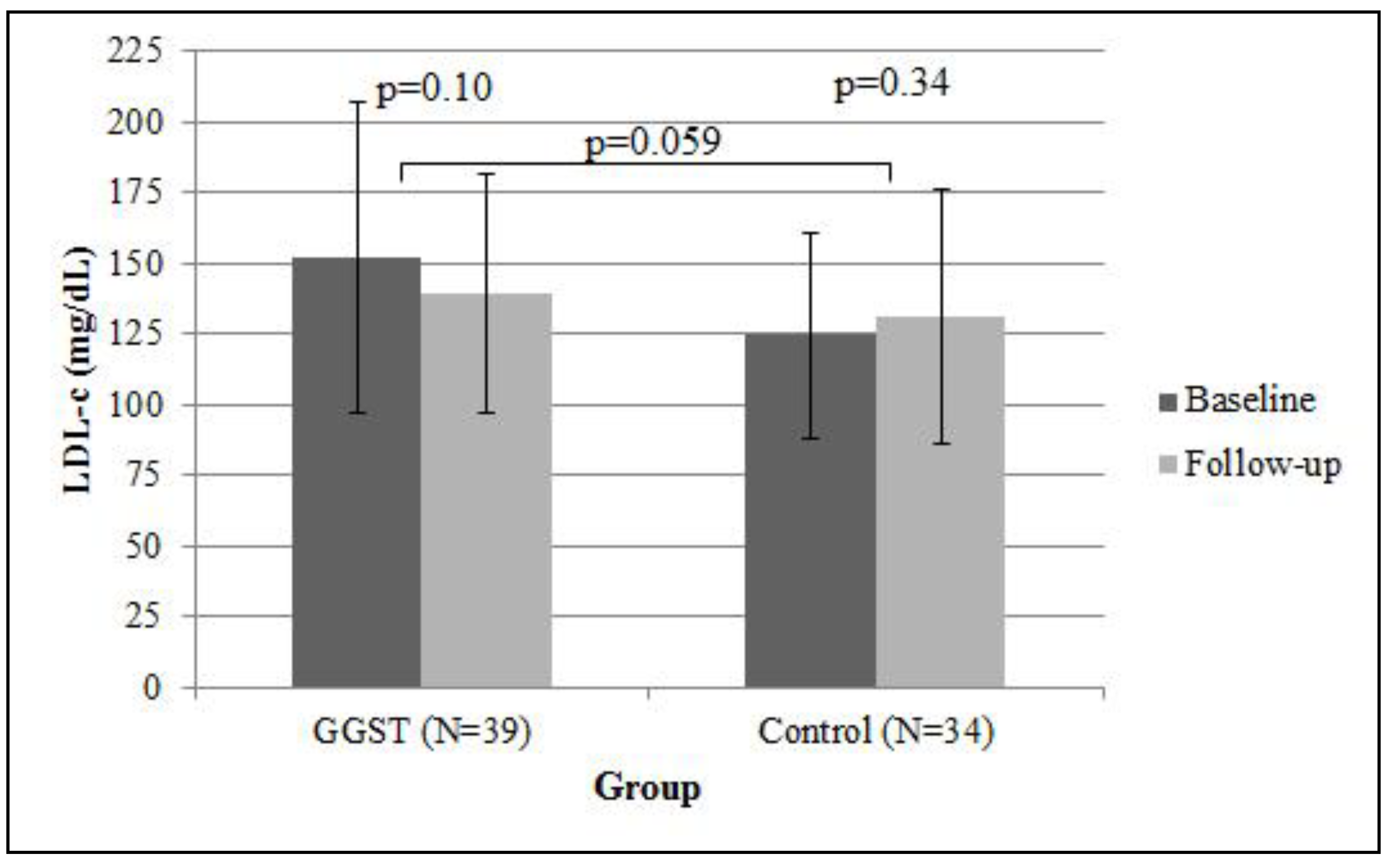
2.1.2. Secondary Outcomes
| Mean score (SD) | Mean score (SD) | p | |
|---|---|---|---|
| at baseline | at 4 months | ||
| Necessity questions | |||
| Lowering my cholesterol requires medications | 3.7 (1.0) | 3.5 (1.2) | 0.18 |
| My life would have been impossible without medications to lower my cholesterol | 2.4 (0.9) | 2.5 (1.0) | 0.46 |
| Without medicine to lower my cholesterol, I may have become very ill | 3.0 (0.9) | 3.2 (1.0) | 0.14 |
| My health depended on medicine to lower my cholesterol | 3.1 (1.1) | 3.2 (1.0) | 0.72 |
| My medicine to lower my cholesterol protected me from becoming sick | 2.9 (0.9) | 3.3 (0.9) | <0.001 |
| Concern questions | |||
| Having to take medicine to lower my cholesterol worried me | 3.2 (1.3) | 3.1 (1.2) | 0.38 |
| My medicine to lower my cholesterol was a mystery to me | 2.4 (1.1) | 2.4 (1.0) | 0.81 |
| My medicine to lower my cholesterol disrupted my life | 3.2 (1.4) | 2.8 (1.2) | 0.006 |
| I sometimes worried about becoming too dependent on medicine to lower my cholesterol | 2.5 (1.2) | 2.7 (1.2) | 0.35 |
| I sometimes worried about the long-term effects of medicine to lower my cholesterol | 3.9 (1.1) | 3.8 (1.1) | 0.56 |
| Mean necessity score | 15.1 (3.8) | 15.6 (4.0) | 0.24 |
| Mean concern score | 15.2 (4.2) | 14.7 (4.3) | 0.24 |
| Mean differential (necessity – concern) | −0.2 (6.3) | 0.9 (6.8) | 0.12 |
2.1.3. Stratified Analyses by *5 Carrier Status
2.2. Discussion
2.2.1. Limitations
3. Experimental
3.1. Study Population
3.2. Study Intervention
3.3. Study Definitions and Outcomes
3.3.1. Patient characteristics
3.3.2. Beliefs about Medications Questionnaire (BMQ)
3.3.3. Secondary Outcomes
3.4. Statistical Analysis
4. Conclusions
Supplementary Files
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pasternak, R.C.; Smith, S.C., Jr.; Bairey-Merz, C.N.; Grundy, S.M.; Cleeman, J.I.; Lenfant, C. ACC/AHA/NHLBI Clinical Advisory on the Use and Safety of Statins. Circulation 2002, 106, 1024–1028. [Google Scholar]
- Jackevicius, C.A.; Mamdani, M.; Tu, J.V. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA 2002, 288, 462–467. [Google Scholar]
- Ho, P.M.; Magid, D.J.; Shetterly, S.M.; Olson, K.L.; Maddox, T.M.; Peterson, P.N.; Masoudi, F.A.; Rumsfeld, J.S. Medication nonadherence is associated with a broad range of adverse outcomes in patients with coronary artery disease. Am. Heart J. 2008, 155, 772–779. [Google Scholar]
- Pittman, D.G.; Chen, W.; Bowlin, S.J.; Foody, J.M. Adherence to statins, subsequent healthcare costs, and cardiovascular hospitalizations. Am. J. Cardiol. 2011, 107, 1662–1666. [Google Scholar]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar]
- Mancini, G.B.; Baker, S.; Bergeron, J.; Fitchett, D.; Frohlich, J.; Genest, J.; Gupta, M.; Hegele, R.A.; Ng, D.; Pope, J. Diagnosis, prevention, and management of statin adverse effects and intolerance: Proceedings of a Canadian Working Group Consensus Conference. Can. J. Cardiol. 2011, 27, 635–662. [Google Scholar]
- Cohen, J.D.; Brinton, E.A.; Ito, M.K.; Jacobson, T.A. Understanding Statin Use in America and Gaps in Patient Education (USAGE): An internet-based survey of 10,138 current and former statin users. J. Clin. Lipidol. 2012, 6, 208–215. [Google Scholar] [Green Version]
- Jacobson, T.A. Toward “pain-free” statin prescribing: Clinical algorithm for diagnosis and management of myalgia. Mayo Clin. Proc. 2008, 83, 687–700. [Google Scholar]
- Garavalia, L.; Garavalia, B.; Spertus, J.A.; Decker, C. Exploring patients’ reasons for discontinuance of heart medications. J. Cardiovasc. Nurs. 2009, 24, 371–379. [Google Scholar]
- Fung, V.; Sinclair, F.; Wang, H.; Dailey, D.; Hsu, J.; Shaber, R. Patients’ perspectives on nonadherence to statin therapy: A focus-group study. Perm. J. 2010, 14, 4–10. [Google Scholar]
- Fernandez, G.; Spatz, E.S.; Jablecki, C.; Phillips, P.S. Statin myopathy: A common dilemma not reflected in clinical trials. Cleve Clin. J. Med. 2011, 78, 393–403. [Google Scholar]
- Rallidis, L.S.; Fountoulaki, K.; Anastasiou-Nana, M. Managing the underestimated risk of statin-associated myopathy. Int. J. Cardiol. 2012, 159, 169–176. [Google Scholar]
- Zhang, H.; Plutzky, J.; Skentzos, S.; Morrison, F.; Mar, P.; Shubina, M.; Turchin, A. Discontinuation of statins in routine care settings: A cohort study. Ann. Intern. Med. 2013, 158, 526–534. [Google Scholar]
- Group, S.C.; Link, E.; Parish, S.; Armitage, J.; Bowman, L.; Heath, S.; Matsuda, F.; Gut, I.; Lathrop, M.; Collins, R. SLCO1B1 variants and statin-induced myopathy—A genomewide study. N. Engl. J. Med. 2008, 359, 789–799. [Google Scholar]
- Voora, D.; Shah, S.H.; Spasojevic, I.; Ali, S.; Reed, C.R.; Salisbury, B.A.; Ginsburg, G.S. The SLCO1B1*5 genetic variant is associated with statin-induced side effects. J. Am. Coll. Cardiol. 2009, 54, 1609–1616. [Google Scholar]
- Donnelly, L.A.; Doney, A.S.; Tavendale, R.; Lang, C.C.; Pearson, E.R.; Colhoun, H.M.; McCarthy, M.I.; Hattersley, A.T.; Morris, A.D.; Palmer, C.N. Common nonsynonymous substitutions in SLCO1B1 predispose to statin intolerance in routinely treated individuals with type 2 diabetes: A go-DARTS study. Clin. Pharmacol. Ther. 2011, 89, 210–216. [Google Scholar]
- Puccetti, L.; Ciani, F.; Auteri, A. Genetic involvement in statins induced myopathy. Preliminary data from an observational case-control study. Atherosclerosis 2010, 211, 28–29. [Google Scholar] [CrossRef]
- Danik, J.S.; Chasman, D.I.; Macfadyen, J.G.; Nyberg, F.; Barratt, B.J.; Ridker, P.M. Lack of association between SLCO1B1 polymorphisms and clinical myalgia following rosuvastatin therapy. Am. Heart J. 2013, 165, 1008–1014. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.; Brewer, H.B., Jr.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C., Jr.; Stone, N.J. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 1999, 47, 555–567. [Google Scholar]
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health. 1999, 14, 1–24. [Google Scholar]
- Phatak, H.M.; Thomas, J. Relationships between beliefs about medications and nonadherence to prescribed chronic medications. Ann. Pharmacother. 2006, 40, 1737–1742. [Google Scholar]
- Green, R.C.; Roberts, J.S.; Cupples, L.A.; Relkin, N.R.; Whitehouse, P.J.; Brown, T.; Eckert, S.L.; Butson, M.; Sadovnick, A.D.; Quaid, K.A.; et al. Disclosure of APOE genotype for risk of Alzheimer's disease. N. Engl. J. Med. 2009, 361, 245–254. [Google Scholar] [CrossRef]
- Haga, S.B.; Lapointe, N.M. The potential impact of pharmacogenetic testing on medication adherence. Pharmacogenomics J. 2013, 13, 481–483. [Google Scholar] [CrossRef]
- Maningat, P.; Gordon, B.R.; Breslow, J.L. How do we improve patient compliance and adherence to long-term statin therapy? Curr. Atheroscler. Rep. 2013, 15, e291. [Google Scholar]
- Nieuwkerk, P.T.; Nierman, M.C.; Vissers, M.N.; Locadia, M.; Greggers-Peusch, P.; Knape, L.P.; Kastelein, J.J.; Sprangers, M.A.; de Haes, H.C.; Stroes, E.S. Intervention to improve adherence to lipid-lowering medication and lipid-levels in patients with an increased cardiovascular risk. Am. J. Cardiol. 2012, 110, 666–672. [Google Scholar] [CrossRef]
- Charland, S.L.; Agatep, B.C.; Epstein, R.S.; Frueh, F.W.; Herrera, V.; Devlin, J.; Superko, H.; Stanek, E.J. Patient knowledge of pharmacogenetic information improves adherence to statin therapy: Results of the Additional KIF6 Risk Offers Better Adherence to Statins (AKROBATS) trial. J. Am. Coll. Cardiol. 2012, 59. [Google Scholar] [CrossRef]
- Iakoubova, O.A.; Tong, C.H.; Rowland, C.M.; Kirchgessner, T.G.; Young, B.A.; Arellano, A.R.; Shiffman, D.; Sabatine, M.S.; Campos, H.; Packard, C.J.; et al. Association of the Trp719Arg polymorphism in kinesin-like protein 6 with myocardial infarction and coronary heart disease in 2 prospective trials: the CARE and WOSCOPS trials. J. Am. Coll. Cardiol. 2008, 51, 435–443. [Google Scholar] [CrossRef]
- Iakoubova, O.A.; Sabatine, M.S.; Rowland, C.M.; Tong, C.H.; Catanese, J.J.; Ranade, K.; Simonsen, K.L.; Kirchgessner, T.G.; Cannon, C.P.; Devlin, J.J.; et al. Polymorphism in KIF6 gene and benefit from statins after acute coronary syndromes: Results from the PROVE IT-TIMI 22 study. J. Am. Coll. Cardiol. 2008, 51, 449–455. [Google Scholar] [CrossRef]
- Stewart, A.F.; Dandona, S.; Chen, L.; Assogba, O.; Belanger, M.; Ewart, G.; LaRose, R.; Doelle, H.; Williams, K.; Wells, G.A.; et al. Kinesin family member 6 variant Trp719Arg does not associate with angiographically defined coronary artery disease in the Ottawa Heart Genomics Study. J. Am. Coll. Cardiol. 2009, 53, 1471–1472. [Google Scholar] [CrossRef]
- Assimes, T.L.; Holm, H.; Kathiresan, S.; Reilly, M.P.; Thorleifsson, G.; Voight, B.F.; Erdmann, J.; Willenborg, C.; Vaidya, D.; Xie, C.; et al. Lack of association between the Trp719Arg polymorphism in kinesin-like protein-6 and coronary artery disease in 19 case-control studies. J. Am. Coll. Cardiol. 2010, 56, 1552–1563. [Google Scholar] [CrossRef] [Green Version]
- Hopewell, J.C.; Parish, S.; Clarke, R.; Armitage, J.; Bowman, L.; Hager, J.; Lathrop, M.; Collins, R. No impact of KIF6 genotype on vascular risk and statin response among 18,348 randomized patients in the heart protection study. J. Am. Coll. Cardiol. 2011, 57, 2000–2007. [Google Scholar] [CrossRef]
- Horvath, M.M.; Winfield, S.; Evans, S.; Slopek, S.; Shang, H.; Ferranti, J. The DEDUCE Guided Query tool: providing simplified access to clinical data for research and quality improvement. J. Biomed. Inform. 2011, 44, 266–276. [Google Scholar] [CrossRef]
- Statin Therapy to Improve Medication Adherence – ClinicalTrials.gov. Available online: http://clinicaltrials.gov/ct2/show/NCT01894217 (accesssed on 18 March 2014).
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Li, J.H.; Joy, S.V.; Haga, S.B.; Orlando, L.A.; Kraus, W.E.; Ginsburg, G.S.; Voora, D. Genetically Guided Statin Therapy on Statin Perceptions, Adherence, and Cholesterol Lowering: A Pilot Implementation Study in Primary Care Patients. J. Pers. Med. 2014, 4, 147-162. https://doi.org/10.3390/jpm4020147
Li JH, Joy SV, Haga SB, Orlando LA, Kraus WE, Ginsburg GS, Voora D. Genetically Guided Statin Therapy on Statin Perceptions, Adherence, and Cholesterol Lowering: A Pilot Implementation Study in Primary Care Patients. Journal of Personalized Medicine. 2014; 4(2):147-162. https://doi.org/10.3390/jpm4020147
Chicago/Turabian StyleLi, Josephine H., Scott V. Joy, Susanne B. Haga, Lori A. Orlando, William E. Kraus, Geoffrey S. Ginsburg, and Deepak Voora. 2014. "Genetically Guided Statin Therapy on Statin Perceptions, Adherence, and Cholesterol Lowering: A Pilot Implementation Study in Primary Care Patients" Journal of Personalized Medicine 4, no. 2: 147-162. https://doi.org/10.3390/jpm4020147