mHealth for Smoking Cessation Programs: A Systematic Review

Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
| (Millions) | Per 100 Inhabitants | |||||||
|---|---|---|---|---|---|---|---|---|
| 2010 | 2011 | 2012 | 2013 | 2010 | 2011 | 2012 | 2013 | |
| Mobile-cellular subscriptions | ||||||||
| Developed | 1418 | 1475 | 1538 | 1600 | 115.0 | 119.0 | 123.6 | 128.2 |
| Developing | 3901 | 4487 | 4872 | 5235 | 69.0 | 78.3 | 84.3 | 89.4 |
| World | 5320 | 5962 | 6411 | 6835 | 77.2 | 85.5 | 91.2 | 96.2 |
| Active mobile-broadband subscriptions | ||||||||
| Developed | 529 | 683 | 788 | 934 | 42.9 | 55.1 | 63.3 | 74.8 |
| Developing | 249 | 472 | 768 | 1162 | 4.4 | 8.2 | 13.3 | 19.8 |
| World | 778 | 1155 | 1556 | 2096 | 11.3 | 16.6 | 22.1 | 29.5 |
| Individuals using the Internet | ||||||||
| Developed | 830 | 875 | 913 | 958 | 67.3 | 70.5 | 73.4 | 76.8 |
| Developing | 1193 | 1398 | 1584 | 1791 | 21.2 | 24.5 | 27.5 | 30.7 |
| World | 2023 | 2273 | 2497 | 2749 | 29.5 | 32.7 | 35.7 | 38.8 |

2. Background
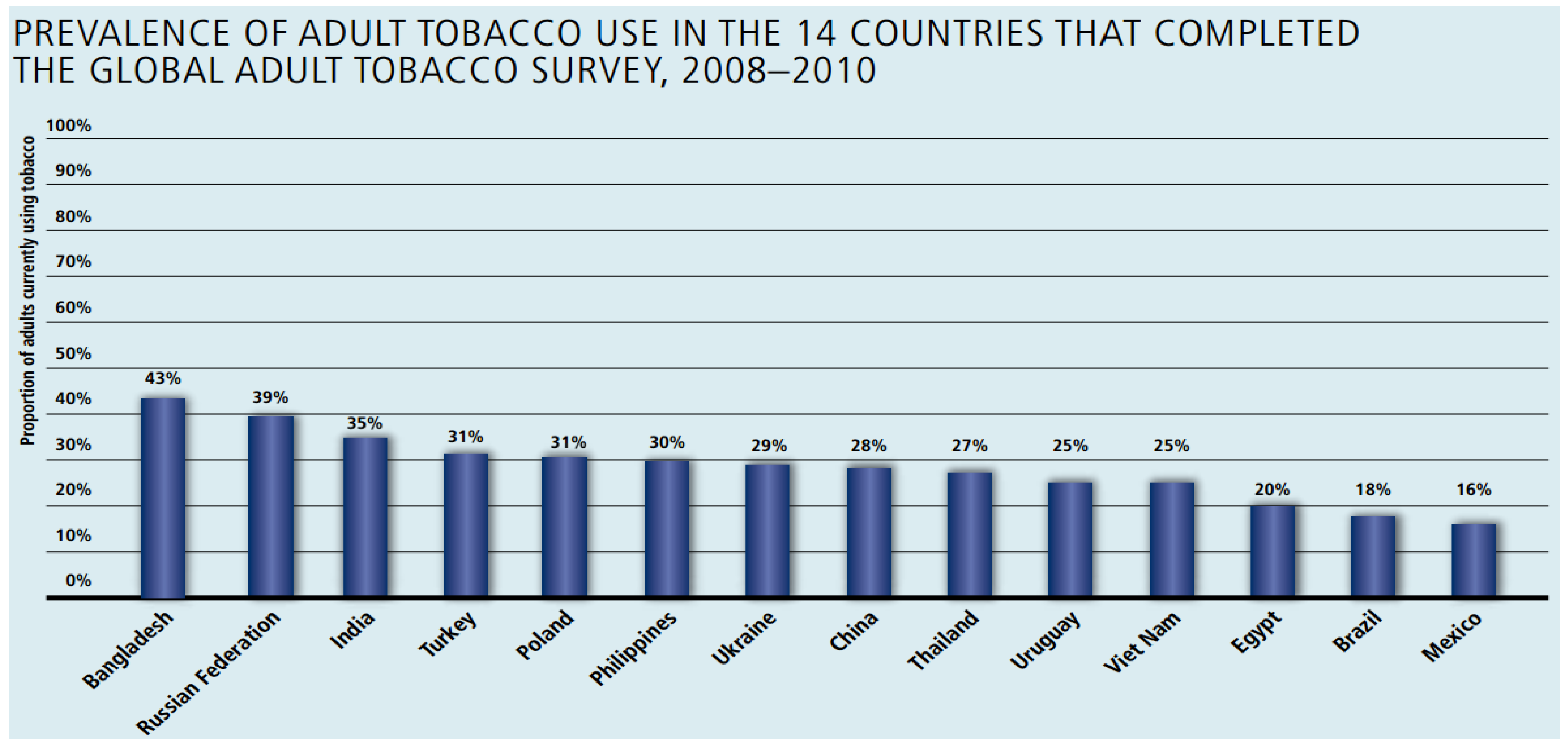
Smoking Prevalence

3. Methods, Results and Discussion
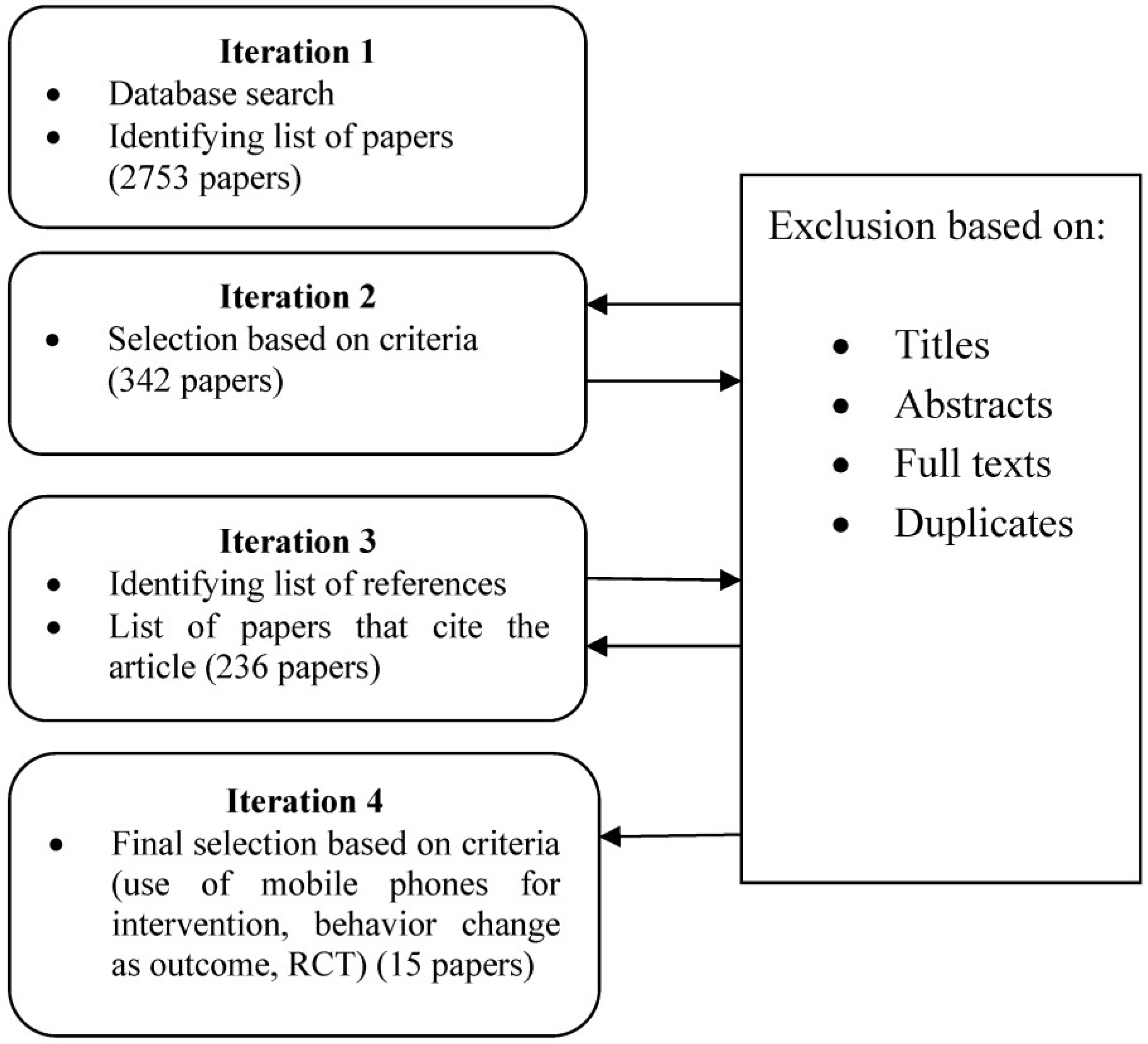
3.1. Resource Identification
3.2. Selection of Studies
- Would focus on smoking cessation
- Would be peer reviewed
- Would be in English Language only
- Would have mobile phone as one of the modes of communication throughout the intervention
- Study should include at least a randomized controlled trial or quasi-experimental controlled trial
- Should have mobile phone as a primary mode of communication in the intervention
- Behavior change for smoking cessation was one of the major intervention outcomes.

| Type of Intervention | Description | References |
|---|---|---|
| Mode of Smoking Cessation Intervention Delivery | Smoking cessation intervention SMS/Multi Media Messages | [5,10,11,19,20,21,22,23] |
| SMS & Internet | [4,6,12,24,25] | |
| Mobile/Telephone for Telecounselling | [26,27] | |
| Personal Tailoring of SMS | Tailoring of SMS done on the basis of participant name, gender, age, participant history, goals and medical condition | [5,6,10,11,19,20,21,24,25] |
| User Initiated Craving Support | Quit help lines of motivational messages triggered by a CRAVE or HELP message from the participant | [4,5,19,20,21,25] |
3.3. Data Extraction and Synthesis
3.4. Characteristics of Studies
3.5. Smoking Cessation Interventions
3.5.1. Mobile Interventions
- -
- SMS based quit smoking services
- -
- Tele-counseling
- -
- Multimedia messages based service (Not as widely used and tested as the first two)
3.5.2. Mobile based Smoking Cessation Intervention Designs
3.6. Overall Findings
- (1)
- None of the studies include System Framework/Design component for behavior change services. mHealth applications are integrated with health information systems in advanced countries, where data are shared both by community health workers (CHWs) and clinicians. Although the quality of mHealth services largely depends on the quality of Information Systems (IS)/technology designs, this study found a paucity of research focusing on this stream. Lack of studies on multi-intervention services for behavior change using Smartphones
- (2)
- None of the studies include user acceptance tests of the smoking cessation services.
3.7. Discussion
3.8. Limitations
4. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Kaplan, W.A. Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries. Global Health 2006, 2, e9. [Google Scholar] [CrossRef]
- International Telecommunication Union The World in 2013: ICT Facts and Figures. Available online: http://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2013-e.pdf (accessd on 30 June 2014).
- Van der Heijden, H.; Junglas, I. Introduction to the special issue on mobile user behaviour. Eur. J. Inf. Syst. 2006, 15, 249–251. [Google Scholar]
- Brendryen, H.; Kraft, P. Happy Ending: A randomized controlled trial of a digital multi-media smoking cessation intervention. Addiction 2008, 103, 478–484. [Google Scholar]
- Free, C.; Knight, R.; Robertson, S.; Whittaker, R.; Edwards, P.; Zhou, W.; Rodgers, A.; Cairns, J.; Kenward, M.G.; Roberts, I. Smoking cessation support delivered via mobile phone text messaging (txt2stop): A single-blind, randomised trial. Lancet 2011, 378, 49–55. [Google Scholar] [CrossRef]
- Riley, W.; Obermayer, J.; Jean-Mary, J. Internet and mobile phone text messaging intervention for college smokers. J. Am. Coll. Health 2008, 57, 245–248. [Google Scholar] [CrossRef]
- Tufano, J.T.; Karras, B.T. Mobile eHealth interventions for obesity: A timely opportunity to leverage convergence trends. J. Med. Internet Res. 2005, 7, e58. [Google Scholar] [CrossRef]
- Durrani, H.; Khoja, S. A systematic review of the use of telehealth in Asian countries. J. Telemed. Telecare 2009, 15, 175–181. [Google Scholar] [CrossRef]
- Question 14-2/2—Mobile eHealth solutions for Developing Countries. Available online: http://www.itu.int/publ/D-STG-SG02.14.2-2010/en (accessed on 29 May 2011).
- Obermayer, J.L.; Riley, W.T.; Asif, O.; Jean-Mary, J. College smoking-cessation using cell phone text messaging. J. Am. Coll. Health 2004, 53, 71–78. [Google Scholar] [CrossRef]
- Whittaker, R.; Dorey, E.; Bramley, D.; Bullen, C.; Denny, S.; Elley, C.R.; Maddison, R.; McRobbie, H.; Parag, V.; Rodgers, A. A theory-based video messaging mobile phone intervention for smoking cessation: Randomized controlled trial. J. Med. Internet Res. 2011, 13, e10. [Google Scholar] [CrossRef]
- Strecher, V.J.; Shiffman, S.; West, R. Randomized controlled trial of a web-based computer-tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction 2005, 100, 682–688. [Google Scholar] [CrossRef]
- Google Our mobile planet. Available online: http://www.marketingmag.com.au/tags/our-mobile-planet/#.U7C5YfmSxyU (accessed on 30 June 2014).
- World Bank Tobacco Control in Developing Countries. Available online: http://www.worldbank.org/en/country (accessed on 13 August 2013).
- Bloom, D.E.; Cafiero, E.T.; McGovern, M.E.; Prettner, K.; Stanciole, A.; Weiss, J.; Bakkila, S.; Rosenberg, L. The Economic Impact of Non-communicable Disease in China and India: Estimates, Projections, and Comparisons; National Bureau of Economic Research: Cambridge, MA, USA, 2013. [Google Scholar]
- Global adult Tobacco Survey GATTS India (2009–2010); Ministry of Health and Family Welfare, Government of India: Mumbai, India, 2010.
- Kitchenham, B. Procedures for Performing Systematic Reviews; Keele University: Keele, UK, 2004. [Google Scholar]
- Dieste, O.; Grimán, A.; Juristo, N. Developing search strategies for detecting relevant experiments. Empir. Softw. Eng. 2009, 14, 513–539. [Google Scholar] [CrossRef]
- Rodgers, A.; Corbett, T.; Bramley, D.; Riddell, T.; Wills, M.; Lin, R.-B.; Jones, M. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob. Control 2005, 14, 255–261. [Google Scholar] [CrossRef]
- Bramley, D.; Riddell, T.; Whittaker, R.; Corbett, T.; Lin, R.-B.; Wills, M.; Jones, M.; Rodgers, A. Smoking cessation using mobile phone text messaging is as effective in Maori as non-Maori. N. Z. Med. J. 2005, 118, e1216. [Google Scholar]
- Naughton, F.; Prevost, A.T.; Gilbert, H.; Sutton, S. Randomized controlled trial evaluation of a tailored leaflet and SMS text message self-help intervention for pregnant smokers (MiQuit). Nicot. Tob. Res. 2012, 14, 569–577. [Google Scholar] [CrossRef]
- Vidrine, D.J.; Arduino, R.C.; Lazev, A.B.; Gritz, E.R. A randomized trial of a proactive cellular telephone intervention for smokers living with HIV/AIDS. Aids 2006, 20, 253–260. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Holtrop, J.S.; Prescott, T.L.; Rahbar, M.H.; Strong, D. Pilot RCT results of stop my smoking USA: A text messaging-based smoking cessation program for young adults. Nicot. Tob. Res. 2013, 15, 1388–1399. [Google Scholar] [CrossRef]
- Abroms, L.C.; Ahuja, M.; Kodl, Y.; Thaweethai, L.; Sims, J.; Winickoff, J.P.; Windsor, R.A. Text2Quit: Results from a pilot test of a personalized, interactive mobile health smoking cessation program. J. Health Commun. 2012, 17, 44–53. [Google Scholar] [CrossRef]
- Brendryen, H.; Drozd, F.; Kraft, P. A digital smoking cessation program delivered through internet and cell phone without nicotine replacement (happy ending): Randomized controlled trial. J. Med. Internet Res. 2008, 10, e51. [Google Scholar] [CrossRef]
- Peterson, A.V.; Kealey, K.A.; Mann, S.L.; Marek, P.M.; Ludman, E.J.; Liu, J.; Bricker, J.B. Group-randomized trial of a proactive, personalized telephone counseling intervention for adolescent smoking cessation. J. Natl. Cancer Inst. 2009, 101, 1378–1392. [Google Scholar] [CrossRef]
- Strecher, V.J.; Marcus, A.; Bishop, K.; Fleisher, L.; Stengle, W.; Levinson, A.; Fairclough, D.L.; Wolfe, P.; Morra, M.; Davis, S. A randomized controlled trial of multiple tailored messages for smoking cessation among callers to the cancer information service. J. Health Commun. 2005, 10, 105–118. [Google Scholar]
- Akter, S.; Ray, P. mHealth—An ultimate platform to serve the unserved. Yearb Med Inform 2010, 2010, 94–100. [Google Scholar] [CrossRef]
- Whittaker, R.; Maddison, R.; McRobbie, H.; Bullen, C.; Denny, S.; Dorey, E.; Ellis-Pegler, M.; van Rooyen, J.; Rodgers, A. A multimedia mobile phone-based youth smoking cessation intervention: findings from content development and piloting studies. J. Med. Internet Res. 2008, 10, e49. [Google Scholar] [CrossRef]
- Luxton, D.D.; McCann, R.A.; Bush, N.E.; Mishkind, M.C.; Reger, G.M. mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 2011, 42, 505–512. [Google Scholar] [CrossRef]
- Abroms, L.C.; Padmanabhan, N.; Thaweethai, L.; Phillips, T. iPhone apps for smoking cessation: a content analysis. Am. J. Prev. Med. 2011, 40, 279–285. [Google Scholar]
- Baumeister, R.F. Yielding to temptation: Self-control failure, impulsive purchasing, and consumer behavior. J. Consum. Res. 2002, 28, 670–676. [Google Scholar] [CrossRef]
- Ghorai, K.; Jahan, S.; Ray, P.; Chylinski, M. Mobile Phone Including Smart Phone based Persuasive System Design for controlling Hypertension and Diabetes in Bangladesh. In Proceedings of the 24th Australasian Conference on Information Systems PSD for Prevention of HTN and T2D in Bangladesh, Melbourne, Australia, 4–6 December 2013.
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ghorai, K.; Akter, S.; Khatun, F.; Ray, P. mHealth for Smoking Cessation Programs: A Systematic Review. J. Pers. Med. 2014, 4, 412-423. https://doi.org/10.3390/jpm4030412
Ghorai K, Akter S, Khatun F, Ray P. mHealth for Smoking Cessation Programs: A Systematic Review. Journal of Personalized Medicine. 2014; 4(3):412-423. https://doi.org/10.3390/jpm4030412
Chicago/Turabian StyleGhorai, Koel, Shahriar Akter, Fatema Khatun, and Pradeep Ray. 2014. "mHealth for Smoking Cessation Programs: A Systematic Review" Journal of Personalized Medicine 4, no. 3: 412-423. https://doi.org/10.3390/jpm4030412