Willingness to Participate in a National Precision Medicine Cohort: Attitudes of Chronic Kidney Disease Patients at a Cleveland Public Hospital

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
- Would you be willing to allow your health records and genetic information to be stored in a national biorepository coordinated by the government as a part of their “Precision Medicine Initiative”? If so this information may be available to researchers nationally and internationally with the understanding that your privacy would be protected.
- Would you be willing to install a free phone app that would be able to track your physical activity, measures of your health and location with the understanding that your privacy would be protected?
- Would you be willing to allow the information collected using the phone app (question 2) to be sent to the national coordinating center where it may be shared with researchers nationally and internationally with the understanding that your privacy would be protected?
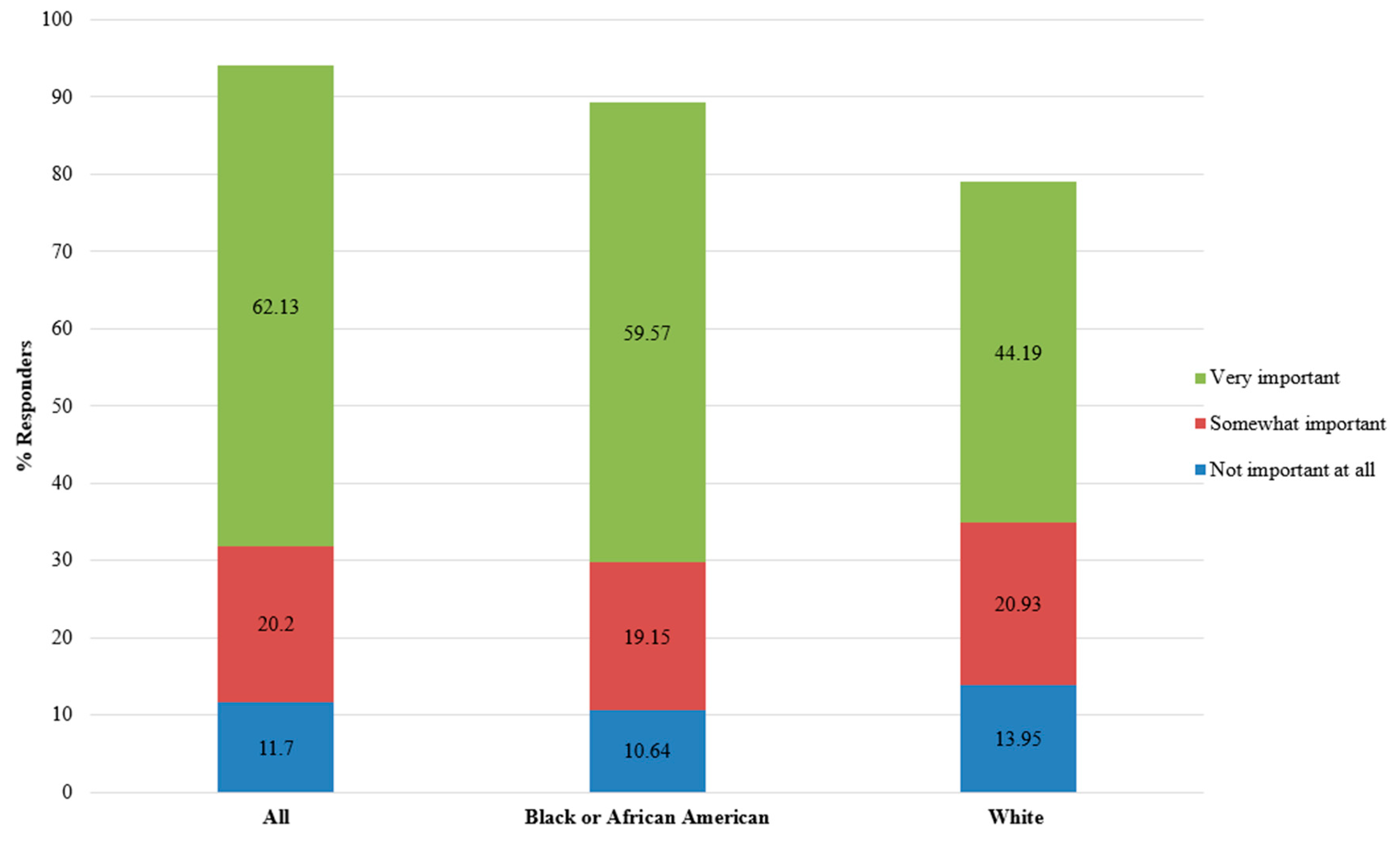
- If you participated in a study that collected your genetic and health information, how important is it to you that you receive results from the study? Circle the number that is closest to how you feel.
- What type of results would you like to receive, please check all that apply:
2.2. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Collins, F.S.; Varmus, H. A New Initiative on Precision Medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, J. NIH’s massive health study is off to a slow start. Science 2017, 357, 955. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Concato, J.; Brophy, M.; Fiore, L.; Pyarajan, S.; Breeling, J.; Whitbourne, S.; Deen, J.; Shannon, C.; Humphries, D.; et al. Million Veteran Program: A mega-biobank to study genetic influences on health and disease. J. Clin. Epidemiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Precision Medicine Initiative (PMI) Working Group. The Precision Medicine Initiative Cohort Program—Building a Research Foundation for 21st Century Medicine; Precision Medicine Initiative: Bethesda, MD, USA, 17 September 2015.
- Stein, L.D.; Knoppers, B.M.; Campbell, P.; Getz, G.; Korbel, J.O. Data analysis: Create a cloud commons. Nature 2015, 523, 149–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somiari, S.B.; Somiari, R.I. The Future of Biobanking: A Conceptual Look at How Biobanks Can Respond to the Growing Human Biospecimen Needs of Researchers. In Biobanking in the 21st Century; Karimi-Busheri, F., Ed.; Springer International Publishing: Cham, Switzerland, 2015; pp. 11–27. [Google Scholar]
- Shalowitz, D.I.; Miller, F.G. Communicating the Results of Clinical Research to Participants: Attitudes, Practices, and Future Directions. PLoS Med. 2008, 5, e91. [Google Scholar] [CrossRef] [PubMed]
- Beskow, L.M.; Burke, W.; Fullerton, S.M.; Sharp, R.R. Offering aggregate results to participants in genomic research: Opportunities and challenges. Genet. Med. 2012, 14, 490. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.V.; Ruccione, K.; Wells, R.J.; Long, J.B.; Pelletier, W.; Hooke, M.C.; Pentz, R.D.; Noll, R.B.; Baker, J.N.; O’Leary, M.; et al. Recommendations for the Return of Research Results to Study Participants and Guardians: A Report from the Children’s Oncology Group. J. Clin. Oncol. 2012, 30, 4573–4579. [Google Scholar] [CrossRef] [PubMed]
- Shalowitz, D.I.; Miller, F.G. Disclosing individual results of clinical research: Implications of respect for participants. JAMA 2005, 294, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Oliver Robinson, J.; McGuire, A.L. Return of individual genomic research results: What do consent forms tell participants? Eur. J. Hum. Genet. 2016, 24, 1524. [Google Scholar] [CrossRef] [PubMed]
- Medicaid and CHIP Payment and Access Commission (MACPAC). Profiles of Disproportionate Share Hospitals. MetroHealth Medical Center FactSheet. Washington, DC, USA, March 2017. Available online: https://www.macpac.gov/wp-content/uploads/2017/03/MetroHealth-Medical-Center.pdf (accessed on 15 July 2017).
- United States Census Bureau American FacFinder. 2011–2016 American Community Survey 5-Year Estimates 2016. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml (accessed on 8 May 2018).
- MetroHealth System. Community Health Needs Assessment; MetroHealth System: Cleveland, OH, USA, 2018; Available online: https:/www.metrohealth.org/upload/docs/main/About Us/Community-Health-CHNA-03.23.18_web.pdf (accessed on 8 May 2018).
- Kincaid, J.P.; Fishburne, R.P., Jr.; Rogers, R.L.; Chissom, B.S. Derivation of New Readability Formulas (Automated Readability Index, Fog Count and Flesch Reading Ease Formula) for Navy Enlisted Personnel; University of Central Florida: Orlando, FL, USA, 1975. [Google Scholar]
- Flesch, R.F. A new readability yardstick. J. Appl. Psychol. 1948, 32, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Flesch, R.F. How to Write Plain English: A Book for Lawyers and Consumers; Harper: New York, NY, USA, 1979. [Google Scholar]
- Humes, K.R.; Jones, N.A.; Ramirez, R.R. Overview of Race and Hispanic Origin; Census Bureau: Suitland, MD, USA, March 2011.
- Bustamante, C.D.; De La Vega, F.M.; Burchard, E.G. Genomics for the world. Nature 2011, 475, 163–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldenberg, A.J.; Marshall, P.A.; Sharp, R.R. Next-generation disadvantages: Identifying potential barriers to integrating genomics into underserved medical settings. Pers. Med. 2013, 10, 623–625. [Google Scholar] [CrossRef] [PubMed]
- Khoury, M.J.; Gwinn, M.; Yoon, P.W.; Dowling, N.; Moore, C.A.; Bradley, L. The continuum of translation research in genomic medicine: How can we accelerate the appropriate integration of human genome discoveries into health care and disease prevention? Genet. Med. 2007, 9, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Hindorff, L.A.; Bonham, V.L.; Brody, L.C.; Ginoza, M.E.C.; Hutter, C.M.; Manolio, T.A.; Green, E.D. Prioritizing diversity in human genomics research. Nat. Rev. Genet. 2018, 19, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Sankar, P.L.; Parker, L.S. The Precision Medicine Initiative’s All of Us Research Program: An agenda for research on its ethical, legal, and social issues. Genet. Med. 2017, 19, 743–750. [Google Scholar] [CrossRef] [PubMed]
- McQuillan, G.M.; Porter, K.S.; Agelli, M.; Kington, R. Consent for genetic research in a general population: The NHANES experience. Genet. Med. 2003, 5, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuillan, G.M.; Pan, Q.; Porter, K.S. Consent for genetic research in a general population: An update on the National Health and Nutrition Examination Survey experience. Genet. Med. 2006, 8, 354–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuillan, G.M.; Porter, K.S. Consent for future genetic research: The NHANES experience in 2007–2008. IRB Ethics Hum. Res. 2011, 33, 9–14. [Google Scholar]
- Kaufman, D.; Murphy, J.; Erby, L.; Hudson, K.; Scott, J. Veterans’ attitudes regarding a database for genomic research. Genet. Med. 2009, 11, 329. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.; Murphy, J.; Scott, J.; Hudson, K. Subjects matter: A survey of public opinions about a large genetic cohort study. Genet. Med. 2008, 10, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.J.; Baker, R.; Milner, L.C.; Devaney, S.; Hudson, K.L. A Survey of U.S Adults’ Opinions about Conduct of a Nationwide Precision Medicine Initiative® Cohort Study of Genes and Environment. PLoS ONE 2016, 11, e0160461. [Google Scholar] [CrossRef]
- Sanderson, S.C.; Brothers, K.B.; Mercaldo, N.D.; Clayton, E.W.; Antommaria, A.H.M.; Aufox, S.A.; Brilliant, M.H.; Campos, D.; Carrell, D.S.; Connolly, J.; et al. Public Attitudes toward Consent and Data Sharing in Biobank Research: A Large Multi-site Experimental Survey in the US. Am. J. Hum. Genet. 2017, 100, 414–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, J.; Scott, J.; Kaufman, D.; Geller, G.; LeRoy, L.; Hudson, K. Public expectations for return of results from large-cohort genetic research. Am. J. Bioeth. 2008, 8, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Ormond, K.E.; Cirino, A.L.; Helenowski, I.B.; Chisholm, R.L.; Wolf, W.A. Assessing the understanding of biobank participants. Am. J. Med. Genet. Part A 2009, 149A, 188–198. [Google Scholar] [CrossRef] [PubMed]
- McCarty, C.A.; Fuchs, M.J.; Lamb, A.; Conway, P. How Do Patients Respond to Genetic Testing for Age-related Macular Degeneration? Optom. Vis. Sci. 2018, 95, 166–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kullo, I.J.; Haddad, R.; Prows, C.A.; Holm, I.; Sanderson, S.C.; Garrison, N.A.; Sharp, R.R.; Smith, M.E.; Kuivaniemi, H.; Bottinger, E.P.; et al. Return of results in the genomic medicine projects of the eMERGE network. Front. Genet. 2014. [Google Scholar] [CrossRef] [PubMed]
- Landry, L.; Nielsen, D.E.; Carere, D.A.; Roberts, J.S.; Green, R.C. Racial minority group interest in direct-to-consumer genetic testing: Findings from the PGen study. J. Community Genet. 2017, 8, 293–301. [Google Scholar] [CrossRef] [PubMed]
- McCarty, C.A.; Nair, A.; Austin, D.M.; Giampietro, P.F. Informed Consent and Subject Motivation to Participate in a Large, Population-Based Genomics Study: The Marshfield Clinic Personalized Medicine Research Project. Public Health Genom. 2007, 10, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Reporter ACSC. Cleveland, OH. 2016. Available online: https://censusreporter.org/profiles/16000US3916000-cleveland-oh/ (accessed on 9 May 2018).
- Allen, N.L.; Karlson, E.W.; Malspeis, S.; Lu, B.; Seidman, C.E.; Lehmann, L.S. Biobank Participants’ Preferences for Disclosure of Genetic Research Results: Perspectives from the Our Genes, Our Health, Our Community Project. Mayo Clin. Proc. 2014, 89, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.I.; Fletcher, A.J.; Sanghani, V.R.; Spainhour, M.; Graham, A.W.; Russell, G.B.; Bailey, J.N.C.; Iltis, A.S.; King, N.M.P. Perceptions regarding Genetic Testing in Populations at Risk for Nephropathy. Am. J. Nephrol. 2013, 38, 453–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Overall | Black or African American | White | Other | |
|---|---|---|---|---|
| Samples size | 103 | 52 | 47 | 4 |
| % Female | 54.40 | 57.69 | 51.06 | 50.00 |
| Mean age, in years (SD) | 61.45 (13.52) | 61.42 (13.02) | 62.38 (13.37) | 50.75 (15.42) |
| 1. Would you be willing to allow your health records and genetic information to be stored in a national biorepository coordinated by the government as a part of their “Precision Medicine Initiative”? If so this information may be available to researchers nationally and internationally with the understanding that your privacy would be protected. | |||
| Response | All Respondents | Black or African American Respondents | White Respondents |
| % Yes (n) | 71.29 (72/101) | 69.23 (36/52) | 71.11 (32/45) |
| 2. Would you be willing to install a free phone app that would be able to track your physical activity, measures of your health and location with the understanding that your privacy would be protected? | |||
| Response | All Respondents | Black or African American Respondents | White Respondents |
| % Yes (n) | 44.66 (46/103) | 46.15 (24/52) | 38.30 (18/47) |
| 3. Would you be willing to allow the information collected using the phone app (question 2) to be sent to the national coordinating center where it may be shared with researchers nationally and internationally with the understanding that your privacy would be protected? | |||
| Response | All Respondents | Black or African American Respondents | White Respondents |
| % Yes (n) | 48.45 (47/97) | 54.00 (27/50) | 37.21 (16/43) |
| Answer Included at Least: | % All Respondents | % Black or African American Respondents | % White Respondents |
|---|---|---|---|
| a | 37.23 | 28.84 | 36.17 |
| b | 67.02 | 59.62 | 59.57 |
| c | 76.60 | 71.15 | 68.09 |
| d | 61.70 | 57.69 | 53.19 |
| e | 10.64 | 9.62 | 10.64 |
| Response Category | % All Respondents | % Black or African American Respondents | % White Respondents |
|---|---|---|---|
| At least summary data | 40.48 | 33.33 | 44.74 |
| Only summary data | 4.76 | 2.38 | 7.89 |
| At least health data | 73.81 | 71.43 | 73.68 |
| Only health data | 3.57 | 2.38 | 2.63 |
| At least genetic data | 90.48 | 92.86 | 89.47 |
| Only genetic data | 20.24 | 26.19 | 15.79 |
| At least data on self | 95.24 | 97.62 | 92.11 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cooke Bailey, J.N.; Crawford, D.C.; Goldenberg, A.; Slaven, A.; Pencak, J.; Schachere, M.; Bush, W.S.; Sedor, J.R.; O’Toole, J.F. Willingness to Participate in a National Precision Medicine Cohort: Attitudes of Chronic Kidney Disease Patients at a Cleveland Public Hospital. J. Pers. Med. 2018, 8, 21. https://doi.org/10.3390/jpm8030021
Cooke Bailey JN, Crawford DC, Goldenberg A, Slaven A, Pencak J, Schachere M, Bush WS, Sedor JR, O’Toole JF. Willingness to Participate in a National Precision Medicine Cohort: Attitudes of Chronic Kidney Disease Patients at a Cleveland Public Hospital. Journal of Personalized Medicine. 2018; 8(3):21. https://doi.org/10.3390/jpm8030021
Chicago/Turabian StyleCooke Bailey, Jessica N., Dana C. Crawford, Aaron Goldenberg, Anne Slaven, Julie Pencak, Marleen Schachere, William S. Bush, John R. Sedor, and John F. O’Toole. 2018. "Willingness to Participate in a National Precision Medicine Cohort: Attitudes of Chronic Kidney Disease Patients at a Cleveland Public Hospital" Journal of Personalized Medicine 8, no. 3: 21. https://doi.org/10.3390/jpm8030021