
Narratives of Psychosocial Response to Microtrauma Injury among Long-Distance Runners

Abstract
:1. Introduction
2. Context
- What psychosocial responses do long-distance runners experience surrounding a microtrauma injury?
- What is the chronology of psychosocial experiences associated with microtrauma injuries in long-distance runners?
3. Method
3.1. Participants

{kind=link}
| Pseudonym | Gender | Age | Self-Reported Injury |
|---|---|---|---|
| Logan | Male | 22 | Sciatic nerve; shin splints |
| Anne | Female | 37 | Pulled hamstring/illiotibial band; skin pain |
| Grace | Female | 23 | Achilles tendonitis; stress fracture |
| Caroline * | Female | 22 | Achilles tendonitis; knee patella femoral |
| Jordan | Female | 22 | Pain on inner right foot; illiotibial band |
| Laura | Female | 21 | Patella subluxation (knee) |
| Jane | Female | 19 | Knee pain, Sacroiliac pain |
| Brad | Male | 21 | Separated shoulder; tibia stress fracture |
| Maryn | Female | 25 | Quadriceps strain; pulled gluteus medius |
| Kathryn | Female | 19 | Illiotibial band; blisters |
| Cynthia | Female | 20 | Runner’s knee (right and left); baby fracture |
3.2. Procedure
3.3. Data Analysis
075: P: Um, I’ve talked to my roommate a lot. She’s one of my best friends and I, you know, through talking to her like, I don’t want to, like have a pity party about it.076: so I’ve just kind of, um, come to the realization that, like, I will finish. Like I will probably have to walk some, like I will…it will tack another hour.
4. Results
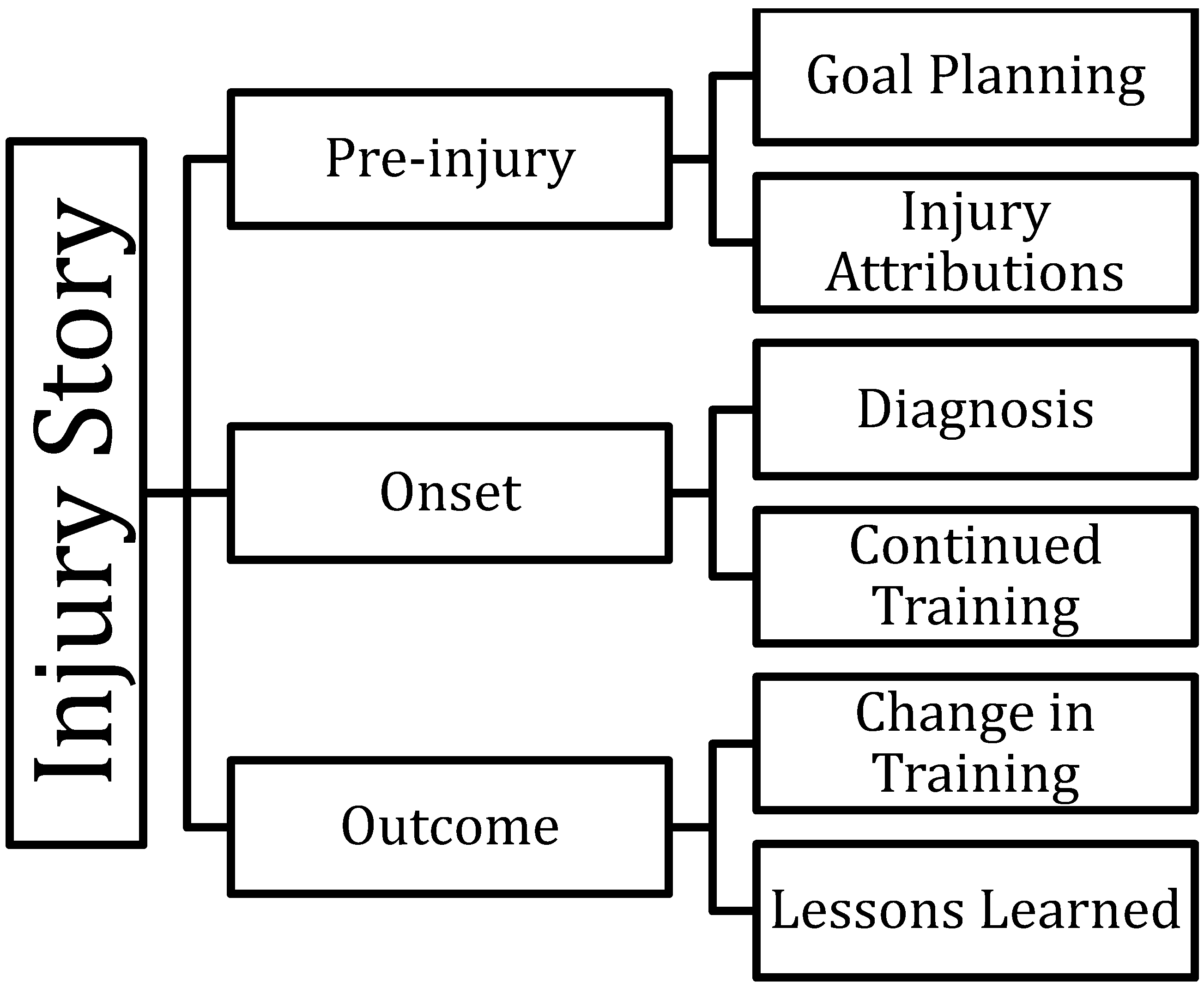
4.2. Research Question 2: Chronology of Experiences
“It [running] was never outside, it was always on a treadmill for that and then I was way over-doing it, because I’d be like… I’d never, kinda of gradually went up, I just like ‘I’m gonna do six miles in the first day’. And that was a bad idea. And I did that for the first two weeks and I was seriously hurting.”
Grace and Laura thought that a change in running conditions, specifically weather conditions, was the cause of their injuries. Participants in the study were primarily from the Midwestern United States and interviews were conducted in the spring after a particularly cold and snowy winter. Participants suggested these harsh running conditions and specifically going from fall running, where the trails and sidewalks were free of ice and snow, to slippery winter conditions contributed to their injury risk. For example, Grace indicated that“Umm, it’s not a big story I guess I was just maybe I was running too much.”
Laura also attributed her injury to winter running conditions, indicating that“I was just doing a run and I had just like, it was like snowy outside and, um, it was icy so I felt my Achilles.”
“the only thing that was kinda like different from my normal running is that we were running in snow so it was kinda slushy so that’s kinda how my injury happened.”
Others worried about having their injury get better or at least being able to control their symptoms prior to the time or a race. Specifically, many participants in this study were concerned about being able to complete their first marathon. Participants noted some degree of pressure associated with training for a specific, time-sensitive running goal. Participants indicated these running goals were inflexible and may have contributed to their overtraining or change in training. For example, Logan noted that he chose to run every day rather than taking any rest days because he was trying to complete a marathon in his goal of under three hours. He reported that he thought this contributed to his injury.“stress because I can’t afford to take any time off of the running.”
She continued to seek out information about IT band issues, but looked online.“I talked to [my coach]… I told him what was going on and, like, umm, I told him I thought it was an IT band issue and he agreed with me and he just said take it easy.”
This information she received informed her use of a foam roller in treatment of her injury. Additionally, many participants noted engaging in icing, stretching, or physical therapy-type exercises in order to treat their injury or at least minimize the discomfort they were experiencing. Specifically, Laura, who was one of the few participants to see a physical therapist, explained that her physical therapist instructed her on how to tape her knee as well as what exercises to do. This instruction allowed her to care for her injury independently.“I remember that Monday night,” she said, “umm, I read online about foam rollers and like how you can foam roll it [IT band] out and a lot of people like who have IT band issues they’ll get a foam roller and it like works magic.”
Kathryn indicated that she continued to run despite her injury, saying,“Like, if I’m told I can’t run, that’s just not going to work.”
However, they did note decreasing or changing their running in order to deal with the injury while increasing cross-training activities such as biking or using the elliptical. Logan, in his explanation of why he did not take much time off, said,“I never took more than like one or two days off from running. I tried to stick with it because I figured it would be harder if I just stopped then went back to it.”
Jordan noted modifying her running in order to deal with her injury. Specifically, she said,“One day I felt pain so I took a few days off and then I did it, I ran again, and I still felt pain but I could push through it.”
Brad indicated that he was in the taper phase of his marathon training when his injury occurred and therefore he was less concerned about taking time off as compared to during other times in his training.“I haven’t felt good since like the injury but like I’ve really learned how to deal with it and like, umm, on our runs I would just like slow down.”
“I reduced my mileage,” he said, “I originally planned on doing for those two weeks just because I wanted to let it rest and let it recover but I didn’t want to just completely stop training so I still ran at least once a week.”
“I think that would have been a big difference would be if I couldn’t do anything active, it would have meant a lot more, but I could still do something active with both those injuries so it didn’t pull me out of physical activity all together so I think that made a big difference.”
“It’s [cross-training workouts developed by her coach] been really helpful to being feeling like I still have a little bit of control of, like maintaining fitness and stuff like. So, doing workouts, that helped me cope with it a little.”
Other participants noted they took a substantial break from running after their goal or deadline. Therefore, the outcome phase, for some, was not until after they had completed their goal race and had taken a break from running.“I haven’t felt good since like the injury but like I’ve really learned how to deal with it and like on our runs I would just like slow down.”
Brad also learned a lesson about overtraining, indicating the injury“I’m more cautious, I would say. I don’t go out and do seven miles after seven miles after seven miles anymore.”
Jane also indicated how important it was to take care of your body. Specifically she said, “Like, I want to be healthy so bad. Um, I definitely respect it [her body] more. Like you have to take care of your body”.“kind of taught me that I was maybe overtraining a little bit. I was running prior to that [the injury] and just kept building up on it and at some point I figured something would happen, but I kind of hoped it would be later.”
She added that,“freak out right off the bat, like umm I guess I was really concerned with the outcome, like am I going to be able to reach my goal, like is this going to prevent me from actually doing the marathon, so I was quick to jump to the worst case scenario.”
Laura noted that she learned that she could deal with more than she thought, specifically she said,“I don’t know, I jumped to conclusions then I realized I need to relax about this so I guess just not panicking and not assuming the worst.”
She also said,“One thing that it [the injury] taught me is like I can push through pain a lot better than I thought I could.”
Jane indicated that“It also helped me to just work through an obstacle because, I don’t know, I hadn’t really had a lot of obstacles I’ve had to work around, especially in exercise.”
Upon reflecting on their injury experience when telling their injuries stories, participants generally indicated continued positive feelings about running despite their injuries. Jane, who was training to complete a marathon, reflected that completing the marathon would mean more to her now because of her injury.“I definitely think that I’ve become tougher.”

5. Discussion
Limitations
6. Future Directions
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lun, V.; Meeuwisse, W.H.; Stergiou, P.; Stefanyshyn, D. Relation between running injury and static lower limb alignment in recreational runners. Brit. J. Sport Med. 2004, 38, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.S.; Grossman, H.Y. Psychological effects of running loss on consistent runners. Percept. Motor Skill. 1988, 66, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Wiese-Bjornstal, D.M.; Smith, A.M.; Shaffer, S.M.; Morrey, M.A. An integrated model of response to sport injury: Psychological and sociological dynamics. J. Appl. Sport Psychol. 1998, 10, 46–69. [Google Scholar] [CrossRef]
- Wiese-Bjornstal, D.M. Psychology and socioculture affect injury risk, response, and recovery in high-intensity athletes: A consensus statement. Scand. J. Med. Sci. Sports 2010, 20, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Flint, F.A. Integrating sport psychology and sports medicine in research: The dilemmas. J. Appl. Sport Psychol. 1998, 10, 83–102. [Google Scholar] [CrossRef]
- Van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.A.; Koes, B.W. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Brit. J. Sport Med. 2007, 41, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Wasley, D.; Lox, C.L. Self-esteem and coping responses of athletes with acute versus chronic injuries. Percept. Motor Skill 1998, 86, 1402. [Google Scholar] [CrossRef] [PubMed]
- Henert, S.E. Exploring Injured Athletes’ Ratings of Social Support and Use of Coping Strategies as a Function of Injury Type and Gender over the Course of Rehabilitation. Ph.D. dissertation, University of Minnesota, Minneapolis, MN, USA, 2000. [Google Scholar]
- Bianco, T. Social support and recovery from sport injury: Elite skiers share their experiences. Res. Q. Exercise Sport 2001, 72, 376–388. [Google Scholar] [CrossRef] [PubMed]
- Brock, S.C.; Kleiber, D.A. Narrative in medicine: The stories of elite college athletes’ career-ending injuries. Qual. Health Res. 1994, 4, 411–430. [Google Scholar] [CrossRef]
- Podlog, L.; Eklund, R.C. High level athletes’ perceptions of success in returning to sport following injury. Psychol. Sport Exercise 2009, 10, 535–544. [Google Scholar] [CrossRef]
- Tracey, J. The emotional response to the injury and rehabilitation process. J. Appl. Sport Psychol. 2003, 15, 279–293. [Google Scholar] [CrossRef]
- Bleakley, A. Stories as data, data as stories: Making sense of narrative inquiry in clinical education. Med. Educ. 2005, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Lieblich, A.; Tuval-Mashiach, R.; Zilber, T. Narrative Research: Reading, Analysis, and Interpretation; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Bailey, P. The dyspnea-anxiety-dyspnea cycle—COPD patients’ stories of breathlessness: “It’s scary/When you can’t breathe.”. Qual. Health Res. 2004, 14, 760–778. [Google Scholar] [CrossRef] [PubMed]
- Borkan, J.M.; Quirk, M.; Sullivan, M. Finding meaning after the fall: Injury narratives from elderly hip fracture patients. Soc. Sci. Med. 1991, 33, 947–957. [Google Scholar] [CrossRef]
- Patton, M.Q. Qualitative Research and Evaluation Methods; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Eatough, V.; Smith, J. Interpretative phenomenological anaylsis. In The Sage Handbook for Qualitative Research in Psychology; Willig, C., Stainton, W., Eds.; Sage Publications, Inc.: Throusand Oaks, CA, USA, 2008. [Google Scholar]
- Tesch, R. Qualitative Research Analysis Types and Software Tools; Falmer Press: New York, NY, USA, 1990. [Google Scholar]
- Mishler, E.G. The analysis of interview-narratives. In Narrative Psychology: The Storied Nature of Human Conduct; Sarbin, T.R., Ed.; Praeger: New York, NY, USA, 1986; pp. 233–255. [Google Scholar]
- Jevon, S.M.; Johnston, L.H. The perceived knowledge and attitudes of governing body chartered physiotherapists towards the psychological aspects of rehabilitation. Phys. Ther. Sport 2003, 4, 74–81. [Google Scholar] [CrossRef]
- McDonald, S.A.; Hardy, C.J. Affective response patterns of the injured athlete: An exploratory analysis. Sport Psychol. 1990, 4, 261–274. [Google Scholar]
- Walker, N.; Thatcher, J.; Lavallee, D. Psychological responses to injury in competitive sport: A critical review. J. R. Soc. Promo. Health 2007, 127, 174–180. [Google Scholar] [CrossRef]
- Mann, B.J.; William, G.A.; Indelicato, P.A.; O’Neill, D.F.; George, S.Z. A survey of sports medicine physicians regarding psychological issues in patient-athletes. Am. J. Sport Med. 2007, 35, 2140–2147. [Google Scholar] [CrossRef] [PubMed]
- Russell, H.; Tracey, J. What do injured athletes want from their health care professionals? Int. J. Athl. Ther. Train. 2011, 16, 18–21. [Google Scholar]
- Tracey, J. Inside the clinic: Health professionals’ role in their clients’ psychological rehabilitation. J. Sport Rehabil. 2008, 17, 413–431. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russell, H.C.; Wiese-Bjornstal, D.M. Narratives of Psychosocial Response to Microtrauma Injury among Long-Distance Runners. Sports 2015, 3, 159-177. https://doi.org/10.3390/sports3030159
Russell HC, Wiese-Bjornstal DM. Narratives of Psychosocial Response to Microtrauma Injury among Long-Distance Runners. Sports. 2015; 3(3):159-177. https://doi.org/10.3390/sports3030159
Chicago/Turabian StyleRussell, Hayley C., and Diane M. Wiese-Bjornstal. 2015. "Narratives of Psychosocial Response to Microtrauma Injury among Long-Distance Runners" Sports 3, no. 3: 159-177. https://doi.org/10.3390/sports3030159