Link between Motor Competence and Health Related Fitness in Children and Adolescents


1
Faculdade de Motricidade Humana, Universidade de Lisboa, 1495-688 Lisboa, Portugal
2
Escola Superior de Educação de Lisboa, Instituto Politécnico de Lisboa, 1549-003 Lisboa, Portugal
3
Laboratory of Motor Behavior, CIPER, Faculdade de Motricidade Humana, Universidade de Lisboa, 1549-003 Lisboa, Portugal
4
Departamento de Desporto e Saúde, Universidade de Évora, 7000-803 Évora, Portugal
5
Instituto Politécnico de Viana do Castelo, Escola Superior Desporto e Lazer, 960-529 Melgaço, Portugal
6
Research Center in Sports Sciences Health Sciences and Human Development (CIDESD), 5000-801 Vila Real, Portugal
*
Author to whom correspondence should be addressed.
Sports 2017, 5(2), 41; https://doi.org/10.3390/sports5020041
Submission received: 1 May 2017
/
Revised: 7 June 2017
/
Accepted: 13 June 2017
/
Published: 15 June 2017
(This article belongs to the Special Issue Motor Competence for Health, Exercise and Sports Performance across the Lifespan)
Abstract
:This study examined motor competence (MC) behavior in 6- to 14-year-old children, and investigated the differences in health-related fitness (HRF) between high and low MC groups, according to sex and age. A sample of 564 children (288 males) participated in this study, divided into three age groups (6–8 years; 9–11 years; 12–14 years). Total MC and its three components (stability, locomotor, and manipulative) were assessed with a quantitative instrument. HRF was evaluated using a maximal multistage 20-m shuttle-run test and the handgrip test. Participants were divided into tertiles according to their MC level and high and low MC groups were analyzed. Overall, MC increased across age groups for both sexes, but boys presented better results than girls. The high MC group outperformed their low MC peers in all HRF variables, independent of their age group. Although cardiovascular fitness increased with age for both the high and low MC groups, the differences between these groups were greater in older children compared to younger children, within the study age range. The findings suggest that MC interventions should be considered as an important strategy to enhance HRF, and girls at a young age should be a priority target.
1. Introduction
The overall prevalence of childhood obesity is high [1], and children tend to spend less time and engage less in physical activity (PA) [2] while spending more time on sedentary activities [3]. A theoretical model proposed by Stodden and colleagues (2008) [4] allocates a key role to motor competence (MC) for developing an active and healthy lifestyle, and very recently, several studies provided support for this hypothetical model regarding the effects of MC on the positive developmental trajectories of health [5,6].
MC is used as a global term that includes a wide variety of terms used in literature (i.e., fundamental motor skill or movement, motor proficiency or performance, motor ability and motor coordination), and can be advantageously described as a person’s ability to be proficient in a wide range of motor acts or skills [7] that include locomotor, stability or manipulative movements [1,9].
The strength of the relationship between MC and health-related fitness (HRF), and MC and weight status, is high and increases with time [6]. However, MC and HRF have shown a decline over recent years [10,11,12,13] with approximately 5–8% of school aged children exhibiting motor problems often mentioned as having developmental coordination disorder (DCD) [14,15,16]. This disorder is characterized by poor MC—substantially below that expected for a child’s chronological age and measured intelligence [17]. Moreover, this poor MC renders difficult their involvement in activities of daily living, as well as sports and exercise [18], putting at risk the development of motor competence, health related fitness and health [19]. When investigating the relationship between HRF and MC, body composition can definitely be a confounder. For instance, body mass index is usually positively related to cardiorespiratory fitness [20] and MC [21], while negatively related to strength [22].
Research indicates that low MC children present lower cardiorespiratory fitness and muscle strength, two of the most important determinants of health-related fitness [23]. For example, Cairney, Hay, Faught, Flouris, and Klentrou [24] found that children with low MC (9–14 years) performed on average 17% inferior to their peers on the Progressive Aerobic Cardiovascular Endurance Run (PACER) test. Hands and Larkin [25] also found, using the same test, lower results for the less proficient group (27% lower). Similar results were found using laboratory-based methods. For example, Hands, Larkin, Parker, Straker, and Perry [26] reported a 11% difference between MC groups on cardiorespiratory endurance using the physical working capacity 170 (PWC 170) test. Moreover, longitudinal studies showed that cardiorespiratory fitness differences between motor competence groups (low vs high) tend to remain over time [27,28] or the lower MC group tends to present a much greater decline rate [29]. So, it appears to be increasingly difficult for these children to catch up with their peers. Identical results were found for groups with low MC and muscle strength [30]. In Haga’s research, the group with high MC presented higher performances (21%) at baseline and after 32 months (20%) than the group with low MC.
Emerging evidence indicates that object control/manipulative skills are more likely to be predictive of HRF in late childhood and early adolescence, while for the early stages of development, locomotor skills may have a more important role [31].
As mentioned above, in recent literature, the differences in HRF related to MC groups are very noticeable. However, and to the best of our knowledge, the instruments used did not assess all MC dimensions: locomotor, stability, and manipulative or object control.
Accordingly, the purpose of the present study was to investigate the differences, according to sex and age, in physical fitness and body composition amongst two groups with differentiated MC (i.e., higher and low MC) using a quantitative instrument [9] with good validity that provides a MC composite from its three theoretical components (i.e., locomotor, stability and manipulative skills) [8]. It is expected that the group with the highest MC group will show better results in HRF, independent of age and sex, in comparison to the group with the lowest MC [27,32].
2. Methods
2.1. Participants
A sample of 564 children (288 males) aged from 6 to 14 years old, with an average age of 10.6 years (SD = 2.40) participated in this study. Children had no motor limitations and were selected from public schools. Two physical education teachers collected all the data for this study over a period of three months during regularly scheduled classes. A local ethics committee ensured that all procedures regarding scientific research involving human beings would be conducted safely. Written informed consent was obtained from the children's parents. Children were asked for verbal assent, while being informed that participation was voluntary and that they could leave the study at any point.
2.2. Measures
Health-related fitness. HRF comprises a number of different components, such as cardiorespiratory fitness, muscle strength, muscle endurance, flexibility, and body composition [26]. In this study, three components of HRF were assessed, namely cardiorespiratory fitness (PACER), upper body strength (handgrip test) and body mass index (BMI). PACER test: This test assessed aerobic capacity by using a progressive shuttle run with an increased cadence. Participants run back and forth across a 20-m course, beginning at a slow pace with increments at every minute. The test finishes when they cannot maintain the pace at the end of two consecutive 20 m laps. The FITNESSGRAM test protocol (for more information see Welk and Meredith, [33]) was used with one modification; to ensure that the participants reached their maximum level and to give proper encouragement, an adult ran with them to pace the rhythm. Handgrip test: This test is often used for assessing muscular fitness in epidemiological studies [23]. Each participant squeezes the dynamometer with maximum isometric effort, maintained for 5 s. The best result after three attempts was recorded as the final score. Body composition: Participant’s height and weight measures were used to calculate the BMI score.
Motor competence. Motor competence was evaluated using the model proposed by Luz and colleagues [9], developed on a sample of Portuguese children. The model is divided into three factors/categories (stability, locomotor and manipulative) with two motor tasks each: Stability tests: (a) Shifting platforms—Moving sideways using two wooden platforms (25 cm × 25 cm × 2 cm with four 3.7 cm feet at the corners). The test begins with the participant standing on one single platform and moving the other from one side to the other (right to left or vice-versa), moving the body to the second platform, and so on for 20 s. Each successful body transfer from one platform to the other is scored with two points (one point for shifting the platform from side to side, one point for moving the body into the platform). Participants were given two trials and only the best score was considered; (b) Lateral jumps—Participants were requested to jump sideways with two feet together over a small wooden beam (60 cm length × 4 cm high × 2 cm width) located in the middle of a rectangular surface (100 cm length × 60 cm width) as fast as possible for 15 s. Each correct jump (two feet together, without touching outside the rectangle, and without stepping in the wooden beam) was scored 1 point and the best score was recorded. Locomotor tests: (a) Shuttle run (SHR)—Children were instructed to run at maximal speed between the starting line and a line placed 10 m away four times (4 × 10 m). They had to pick up a block of wood, run back and place the block beyond the starting line, then repeat it again. The task ended (time stop) when the participants crossed the starting line. The best time of the two trials was recorded; (b) Standing long jump (SLJ)—Participants had to jump with both feet simultaneously as far as possible. Participants were allowed to swing their arms back and forth. The final score was given by the longest (the best of both attempts) distance (in centimetres) between the starting line and the landing position. Manipulative tests: (a) Throwing velocity—Children were requested to throw a ball against a wall at maximum speed using an overarm action with a preparatory balance (one or two steps). A tennis ball (diameter: 6.5 cm; weight: 57 g) and a baseball (diameter: 7.3 cm; weight: 142 g) were used for children between 7 and 10 years old and for 11 years old and older, respectively. Peak velocity was measured in m/s with a velocity radar gun (e.g., Pro II Stalker radar gun). Every participant performed three trials, with the final score being the best result; (b) Kicking velocity—Children were instructed to kick a soccer ball against a wall at maximum speed using a preparatory balance (one or two steps). Three different balls were used, namely a soccer ball nº3 (circumference: 62 cm, weight: 350 g), nº4 (circumference 64 cm, weight: 360 g) and nº5 (circumference 68 cm, weight: 410 g) for children 7–8 years-old, 9–10 years-old and older than 10 years-old, respectively. Ball peak velocity was measured in m/s with a velocity radar gun (e.g., Pro II Stalker radar gun). The final result was obtained through the best performance of three attempts.
Standardized scores were calculated for each task and then stability, locomotor, and manipulative categories were calculated through the sum of the t-scores of the two representative tasks. Given the nature of the task (in sec), the SHR result-scores were inverted. As mentioned above, the MC evaluation should include tasks covering stability, locomotor and manipulative categories [8]; thus, total MC was calculated from the mean of the three categories’ outcomes (t-scores).
All participants were evaluated in groups of five, with all five completing each test trial before the next attempt (to minimize the effects of fatigue), and in the same task order. The stability tasks were performed first, followed by the locomotor tasks and, lastly, the manipulative tasks. A proficient movement was demonstrated and one opportunity to try each task was provided to all participants. Motivational feedback was given, but the results of the tasks were not commented on.
2.3. Data Analysis
All variables were delineated according to age (6–8 years; 9–11 years; 12–14 years), and sex. Health related fitness variables were furthermore divided according to MC level (tertile groups). Previous researchers used similar procedures [34,35] and because the intent was to contrast groups with high and low MC, participants with intermediate scores (i.e., middle tertile) were excluded from this analysis [26]. A multivariate analysis of covariance (MANCOVA) using pacer and handgrip strength as multivariate dependent variables was conducted for each sex separately, testing for age and MC effects on HRF and controlling for BMI. Univariate between group analyses was used to further understand the main effects results of the multivariate HRF variable, and Bonferroni post hoc pairwise comparisons were performed when needed. SPSS 20 was used for all statistical analyses with a p < 0.05 as the level of statistical significance.
3. Results
Descriptive statistics for PACER, handgrip, BMI, MC and the three components of MC for each age group, divided by sex, are displayed in Table 1.
The results revealed on average, an overall increase in MC as well as in all MC components with age development. Moreover, boys generally outperformed girls in all MC variables (except in the middle age group for the stability component).
The MANCOVA results for boys revealed a significant main effect for MC groups (Wilks’ λ = 0.506, F (2182) = 88.95, p < 0.001, η2p = 0.49); and for age groups (Wilks’ λ = 0.343, F (4364) = 64.40 p < 0.001, η2p = 0.41). Girls also displayed a significant main effect for MC groups (Wilks’ λ = 0.623, F (2175) = 52.87 p < 0.001, η2p = 0.38); and for age groups (Wilks’ λ = 0.345, F (4350) = 61.45 p < 0.001, η2p = 0.41). BMI was found to be a significant covariate in both analyses of boys and girls.
According to the MANCOVA results, independent of BMI, the more proficient MC group consistently displayed better HRF results, and HRF results increased with age, for both sexes and MC groups.
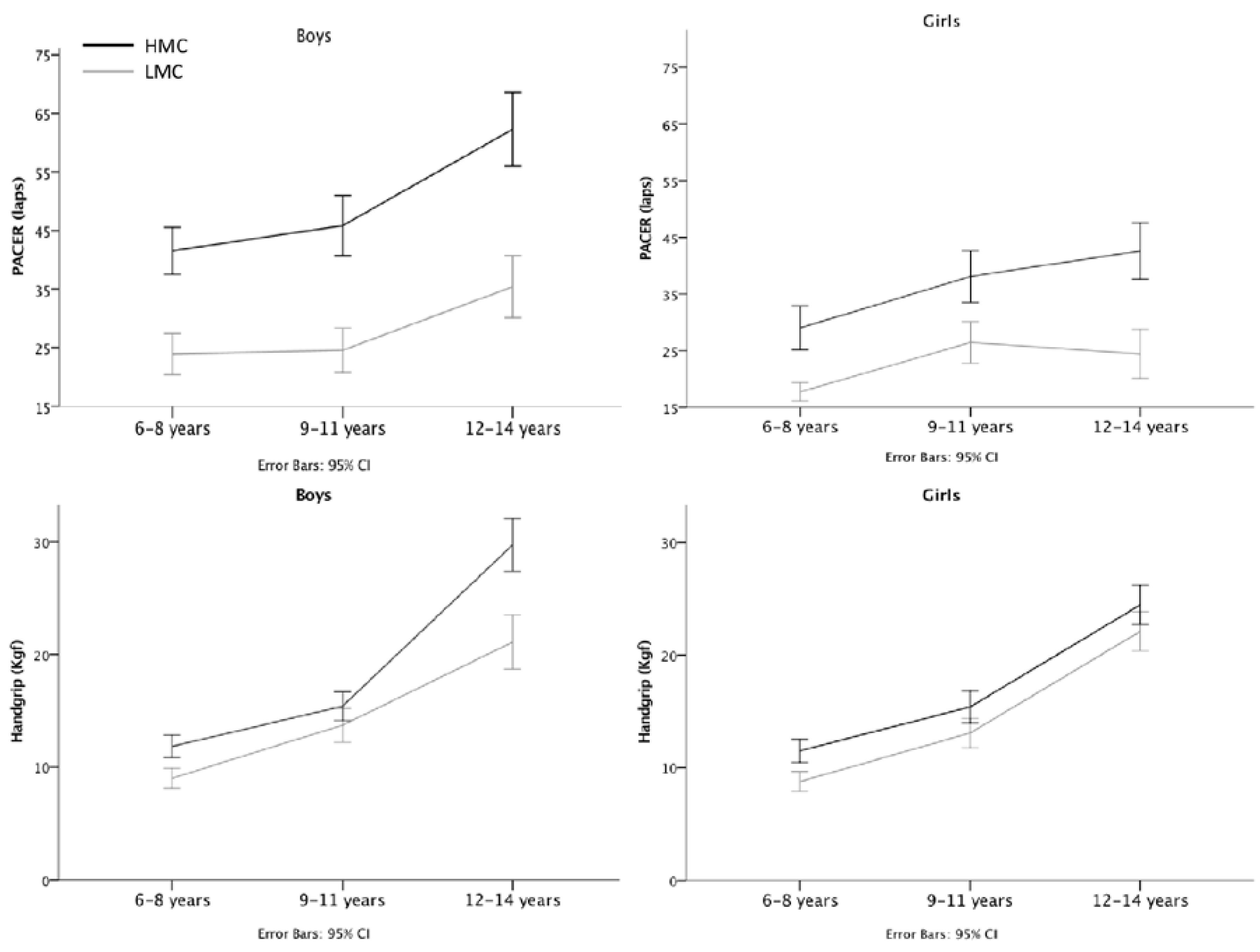
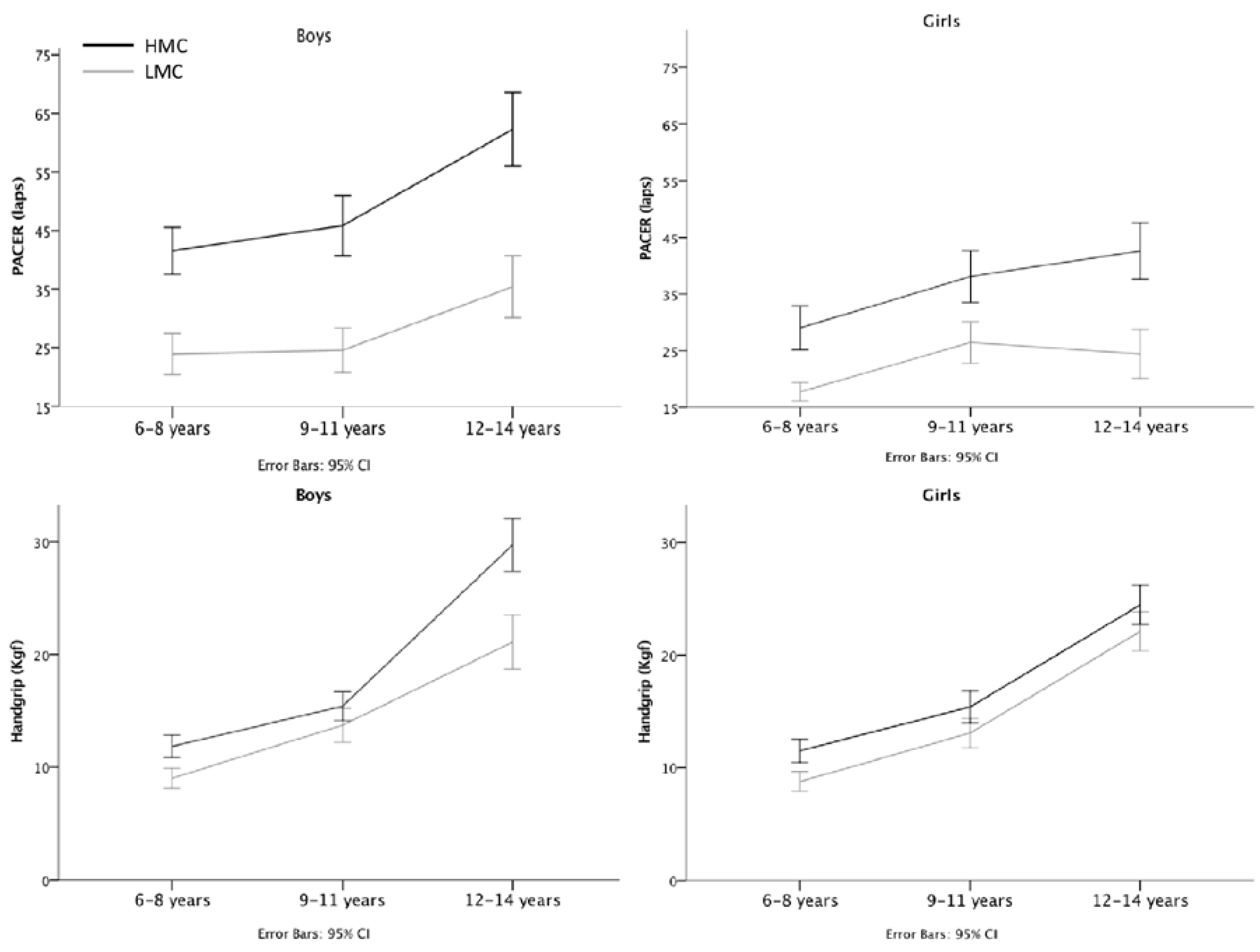
To further clarify the results, univariate main effects for each HRF variable were examined for both sexes (see Figure 1). Boys displayed a significant main effect for the MC proficiency group for both PACER [F (1183) = 114.7; p < 0.001; η2p = 0.39], and handgrip [F (1183) = 86.9; p < 0.001; η2p = 0.32]; and significant main effects for age groups [PACER − F (2183) = 43.4; p < 0.001; η2p = 0.32; Handgrip − F (2183) = 149.1; p < 0.001; η2p = 0.62]. A significant interaction effect between age and MC groups was also found for both HRF variables [PACER − F (2183) = 3.1; p = 0.045; η2p = 0.03; Handgrip − F (2183) = 9.8; p < 0.001; η2p = 0.10]. Girls exhibited similar results to boys in the MC [PACER − F (1176) = 54.7; p < 0.001; η2p = 0.24; Handgrip − F (1176) = 43.7; p < 0.001; η2p = 0.209), and age groups main effects [PACER − F (2176) = 32.2; p < 0.001; η2p = 0.27; Handgrip − F (2176) = 119.8; p < 0.001; η2p = 0.58], but no interaction effect was found.
4. Discussion
In this study, we have investigated the effect of MC on the HRF of children divided into three age groups (6–8 years; 9–11 years; 12–14 years). Global results revealed that boys always outperformed girls, probably as a result of biological sex related differences and a stronger social support system and motivation towards physical activities for boys [36].
Overall MANCOVA results revealed a large effect [37] of MC levels on the multivariate HRF constituted by cardiorespiratory fitness and handgrip, regardless of weight status (BMI). Furthermore, the MC groups explained the HRF variance in about 38% for girls and 49% for boys. An effect of age was also observed, with HRF increasing across age groups, and similar explained variance (41%) for boys and girls. These results clearly show that distinct levels of motor competence are associated with distinct HRF characteristics that can be interpreted as the divergent pathways (positive and negative) described in the Stodden et al. [4] model. It is well established that children with high MC spend more time doing physical activities [38], and participating in sports [27], having more opportunities to improve their HRF. Even if our data is not longitudinal, the described effect remains regardless of age, sex, and BMI values.
Moreover, when each HRF variable (i.e., PACER and handgrip) was analyzed, we found a significant interaction between age and MC groups in boys, meaning that MC groups tend to become more different on cardiovascular fitness and handgrip with age (Figure 1 and Table 1) in boys, while in girls the gap remained stable. Previous works found similar results for cardiovascular fitness [27,28,30], and handgrip in the younger age group [27]. Longitudinal studies confirmed that children with low MC are unlikely to catch up to their peers in time [27,28,30].
The novelty of this research lies in the way that MC was measured. This research used a new instrument with good validity [9] that allows the assessment of MC using all three components (i.e., locomotor, stability and manipulative skills) proposed by the Gallahue et al. [8] framework.
Longitudinal and interventional studies are needed to better understand these complex relationships and their changes across age groups. The absence of maturational information was also a limitation to our conclusions. Biological maturation influences all variables, mostly during the transition from childhood to adolescence; so, future studies should consider including an assessment of the children’s biological maturation. Although other variables (e.g., vertical jump) can be used to measure muscular strength, the handgrip task is a simple assessment method and is related to both maximal upper and lower body strength [39].
Although the cross-sectional design of the study makes it impossible to indicate the causality direction between MC and HRF, two very distinct HRF trajectories emerge from the age-related data analysis. This conclusion is even stronger because all results were controlled for BMI confounding effects. Body mass index is usually positively related to cardiorespiratory fitness [20] and MC [21], while negatively related to strength [22]. Using participants’ BMI as a covariate in the analysis removed the potential confounder effect of BMI, showing the true relationship between MC and HRF.
Our results lead to a conclusion that may be of paramount importance to promote the development of MC from an early age in order to decrease the possibility that children will develop negative trajectories of MC and health-related fitness, also avoiding health and social problems that derive from being overweight and obesity [32].
Acknowledgments
The authors gratefully acknowledge all the schools and families who participated in this study and would like to thank Jamie Moody for the helpful comments during the writing of the manuscript. This research was funded by the Foundation for Science and Technology (Portugal) I&D 472 (UID/DTP/00447/2013).
Author Contributions
C.L. and L.P.R. conceived and designed the experiments; C.L. and G.A. performed the experiments; C.L., R.C. and L.P.R. analyzed the data; G.A. contributed reagents/materials/analysis tools. All authors wrote the paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Low, S.; Chin, M.C.; Deurenberg-Yap, M. Review on epidemic of obesity. Ann. Acad. Med. Singap. 2009, 38, 57–65. [Google Scholar] [PubMed]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.R.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence Based Physical Activity for School-age Youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.; Santos, R.; Pereira, B.; Lopes, V.P. Associations between sedentary behavior and motor coordination in children. Am. J. Hum. Biol. 2012, 24, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Cattuzzo, M.T.; Dos Santos Henrique, R.; Ré, A.H.N.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sport Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; D’Hondt, E.; Bourgois, J.; Vaeyens, R.; Philippaerts, R.M.; Lenoir, M. Motor competence assessment in children: Convergent and discriminant validity between the BOT-2 Short Form and KTK testing batteries. Res. Dev. Disabil. 2014, 35, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- Gallahue, D.; Ozmun, J.; Goodway, J. Understanding Motor Development: Infants, Children, Adolescents, Adults, 7th ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Luz, C.; Rodrigues, L.P.; Almeida, G.; Cordovil, R. Development and validation of a model of motor competence in children and adolescents. J. Sci. Med. Sport 2016, 19, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Catley, M.J.; Tomkinson, G.R. Normative health-related fitness values for children: Analysis of 85347 test results on 9–17-year-old Australians since 1985. Br. J. Sports Med. 2013, 47, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Barnett, L.; Espinel, P.; Okely, A.D. Thirteen-year trends in child and adolescent fundamental movement skills: 1997–2010. Med. Sci. Sports Exerc. 2013, 45, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Olds, T.S. Secular changes in aerobic fitness test performance of Australasian children and adolescents. Med. Sport Sci. 2007, 50, 168–182. [Google Scholar] [PubMed]
- Vandorpe, B.; Vandendriessche, J.; Lefevre, J.; Pion, J.; Vaeyens, R.; Matthys, S.; Philippaerts, R.; Lenoir, M. The KörperkoordinationsTest für Kinder: Reference values and suitability for 6–12-year-old children in Flanders. Scand. J. Med. Sci. Sports 2011, 21, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Cermak, S.A.; Larkin, D. Developmental Coordination Disorder; Delmar Thomson Learning: Albany, NY, USA, 2002. [Google Scholar]
- Gillberg, C.; Kadesjö, B. Why bother about clumsiness? The implications of having developmental coordination disorder (DCD). Neural Plast. 2003, 10, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Barnhart, R.C.; Davenport, M.J.; Epps, S.B.; Nordquist, V.M. Developmental Coordination Disorder. Phys. Ther. 2003, 83, 722–731. [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Cairney, J.; Hay, J.A.; Faught, B.E.; Wade, T.J.; Corna, L.; Flouris, A. Developmental coordination disorder, generalized self-efficacy toward physical activity, and participation in organized and free play activities. J. Pediatr. 2005, 147, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Bouffard, M.; Watkinson, E.J.; Thompson, L.P.; Causgrove Dunn, J.L.; Romanow, S.K.E. A test of the activity deficit hypothesis with children with movement difficulties. Adapt. Phys. Act. Q. 1996, 13, 61–73. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J. Physical activity , physical fitness , and overweight in children and adolescents: Evidence from epidemiologic studies. Med. Intensiva (Eng. Ed.) 2013, 60, 458–469. [Google Scholar] [CrossRef]
- Lopes, V.P.; Stodden, D.F.; Bianchi, M.M.; Maia, J.A.; Rodrigues, L.P. Correlation between BMI and motor coordination in children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The Health Benefits of Muscular Fitness for Children and Adolescents: A Systematic Review and Meta-Analysis. Sport Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cairney, J.; Hay, J.A.; Faught, B.E.; Flouris, A.; Klentrou, P. Developmental coordination disorder and cardiorespiratory fitness in children. Pediatr. Exerc. Sci. 2007, 19, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Hands, B.; Larkin, D. Physical fitness differences in children with and without motor learning difficulties. Eur. J. Spec. Needs Educ. 2006, 21, 447–456. [Google Scholar] [CrossRef]
- Hands, B.; Larkin, D.; Parker, H.; Straker, L.; Perry, M. The relationship among physical activity, motor competence and health-related fitness in 14-year-old adolescents. Scand. J. Med. Sci. Sports 2009, 19, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Deprez, D.; Pion, J.; Tallir, I.B.; D’Hondt, E.; Vaeyens, R.; Lenoir, M.; Philippaerts, R.M. Changes in physical fitness and sports participation among children with different levels of motor competence: A 2-year longitudinal study. Pediatr. Exerc. Sci. 2014, 26, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Hands, B. Changes in motor skill and fitness measures among children with high and low motor competence: A five-year longitudinal study. J. Sci. Med. Sport 2008, 11, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Cairney, J.; Hay, J.; Veldhuizen, S.; Faught, B.E. Trajectories of cardiorespiratory fitness in children with and without developmental coordination disorder: A longitudinal analysis. Br. J. Sports Med. 2011, 45, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Haga, M. Physical fitness in children with high motor competence is different from that in children with low motor competence. Phys. Ther. 2009, 89, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Gao, Z.; Goodway, J.D.; Langendorfer, S.J. Dynamic Relationships between Motor Skill Competence and Health-Related Fitness in Youth. Pediatr. Exerc. Sci. 2014, 26, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.P.; Stodden, D.F.; Lopes, V.P. Developmental pathways of change in fitness and motor competence are related to overweight and obesity status at the end of primary school. J. Sci. Med. Sport 2015, 19, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Meredith, M.D. FITNESSGRAM/ACTIVITYGRAM Reference Guide; Welk, G.J., Meredith, M.D., Eds.; The Cooper Institute: Dalas, TX, USA, 2008. [Google Scholar]
- Duncan, M.J.; Bryant, E.; Stodden, D.; Duncan, M.J.; Bryant, E.; Stodden, D.; Duncan, M.J. Low fundamental movement skill proficiency is associated with high BMI and body fatness in girls but not boys aged 6–11 years old fatness in girls but not boys aged 6–11 years old. J. Sports Sci. 2016, 1–7. [Google Scholar] [CrossRef]
- Williams, H.G.; Pfeiffer, K.A.; O’Neill, J.R.; Dowda, M.; McIver, K.L.; Brown, W.H.; Pate, R.R. Motor skill performance and physical activity in preschool children. Obesity (Silver Spring) 2008, 16, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Kourtessis, T.; Tsougou, E.; Maheridou, M.; Tsigilis, N.; Psalti, M.; Kioumourtzoglou, E. Developmental coordination disorder in early childhood—A preliminary epidemiological study in greek schools. Int. J. Med. 2008, 1, 95–99. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988; p. 567. [Google Scholar]
- Barnett, L.M.; van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood Motor Skill Proficiency as a Predictor of Adolescent Physical Activity. J. Adolesc. Heal. 2009, 44, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Milliken, L.A.; Faigenbaum, A.D.; Loud, R.L.; Westcott, W.L. Correlates of upper and lower body muscular strength in children. J. Strength Cond. Res. 2008, 22, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Means and 95%CI for all HRF variables in both genders. HMC—high motor competence; LMC—low motor competence.
Figure 1.
Means and 95%CI for all HRF variables in both genders. HMC—high motor competence; LMC—low motor competence.

{kind=link}
Table 1.
Means and standard deviations by age group and sex for motor competence (MC) components, health-related fitness (HRF) variables, and HRF variables according to MC groups.
Table 1.
Means and standard deviations by age group and sex for motor competence (MC) components, health-related fitness (HRF) variables, and HRF variables according to MC groups.
| Variables | 6–8 Years | 9–11 Years | 12–14 Years | |||
|---|---|---|---|---|---|---|
| B n = 94 | G n = 90 | B n = 97 | G n = 94 | B n = 97 | G n = 92 | |
| M ± SD | M ± SD | M ± SD | M ± SD | M ± SD | M ± SD | |
| Stability (pts) | 43.5 ± 7.0 | 41.3 ± 7.1 | 49.2 ± 7.6 | 50.8 ± 8.0 | 59.1 ± 8.2 | 55.5 ± 9.1 |
| Locomotor (pts) | 46.3 ± 6.6 | 40.5 ± 7.9 | 50.7 ± 8.0 | 48.6 ± 7.0 | 61.1 ± 8.8 | 52.0 ± 8.3 |
| Manipulative (pts) | 46.0 ± 4.9 | 38.3 ± 4.8 | 53.7 ± 6.0 | 46.2 ± 4.9 | 64.3 ± 8.6 | 50.4 ± 5.6 |
| MC total (pts) | 44.6 ± 5.8 | 38.8 ± 6.2 | 51.4 ± 6.5 | 48.4 ± 6.0 | 62.9 ± 8.2 | 53.0 ± 7.0 |
| BMI (kg/m2) | 17.0 ± 1.9 | 17.4 ± 2.5 | 19.4 ± 3.7 | 18.7 ± 3.4 | 20.3 ± 3.7 | 21.9 ± 4.7 |
| PACER (laps) | 31.8 ± 12.6 | 23.1 ± 9.0 | 35.7 ± 16.0 | 30.9 ± 11.9 | 49.1 ± 19.0 | 32.8 ± 14.6 |
| High MC | 41.5 ± 10.9 | 29.0 ± 10.3 | 45.8 ± 14.3 | 38.1 ± 12.4 | 62.3 ± 17.4 | 42.6 ± 13.6 |
| Low MC | 23.9 ± 9.5 | 17.7 ± 4.4 | 24.6 ± 10.5 | 26.45 ± 9.9 | 35.4 ± 14.7 | 24.4 ± 11.6 |
| Handgrip (Kgf) | 10.4 ± 2.7 | 10.0 ± 2.7 | 14.9 ± 4.1 | 14.6 ± 4.1 | 25.3 ± 7.4 | 22.9 ± 4.7 |
| High MC | 11.8 ± 2.7 | 11.5 ± 2.8 | 15.4 ± 3.6 | 15.4 ± 3.9 | 29.7 ± 6.5 | 24.5 ± 4.8 |
| Low MC | 9.0 ± 2.5 | 8.7 ± 2.4 | 13.7 ± 4.2 | 13.1 ± 3.6 | 21.1 ± 6.6 | 22.1 ± 4.7 |
Notes: B = boys; G = girls; M = mean; SD = standard deviation; BMI—body mass index; PACER—Progressive aerobic cardiovascular endurance run.
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Luz, C.; Cordovil, R.; Almeida, G.; Rodrigues, L.P. Link between Motor Competence and Health Related Fitness in Children and Adolescents. Sports 2017, 5, 41. https://doi.org/10.3390/sports5020041
AMA Style
Luz C, Cordovil R, Almeida G, Rodrigues LP. Link between Motor Competence and Health Related Fitness in Children and Adolescents. Sports. 2017; 5(2):41. https://doi.org/10.3390/sports5020041
Chicago/Turabian StyleLuz, Carlos, Rita Cordovil, Gabriela Almeida, and Luis P. Rodrigues. 2017. "Link between Motor Competence and Health Related Fitness in Children and Adolescents" Sports 5, no. 2: 41. https://doi.org/10.3390/sports5020041
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.