Acute and Chronic Effects of Isometric Handgrip Exercise on Cardiovascular Variables in Hypertensive Patients: A Systematic Review

 ,
,
Abstract
:1. Introduction
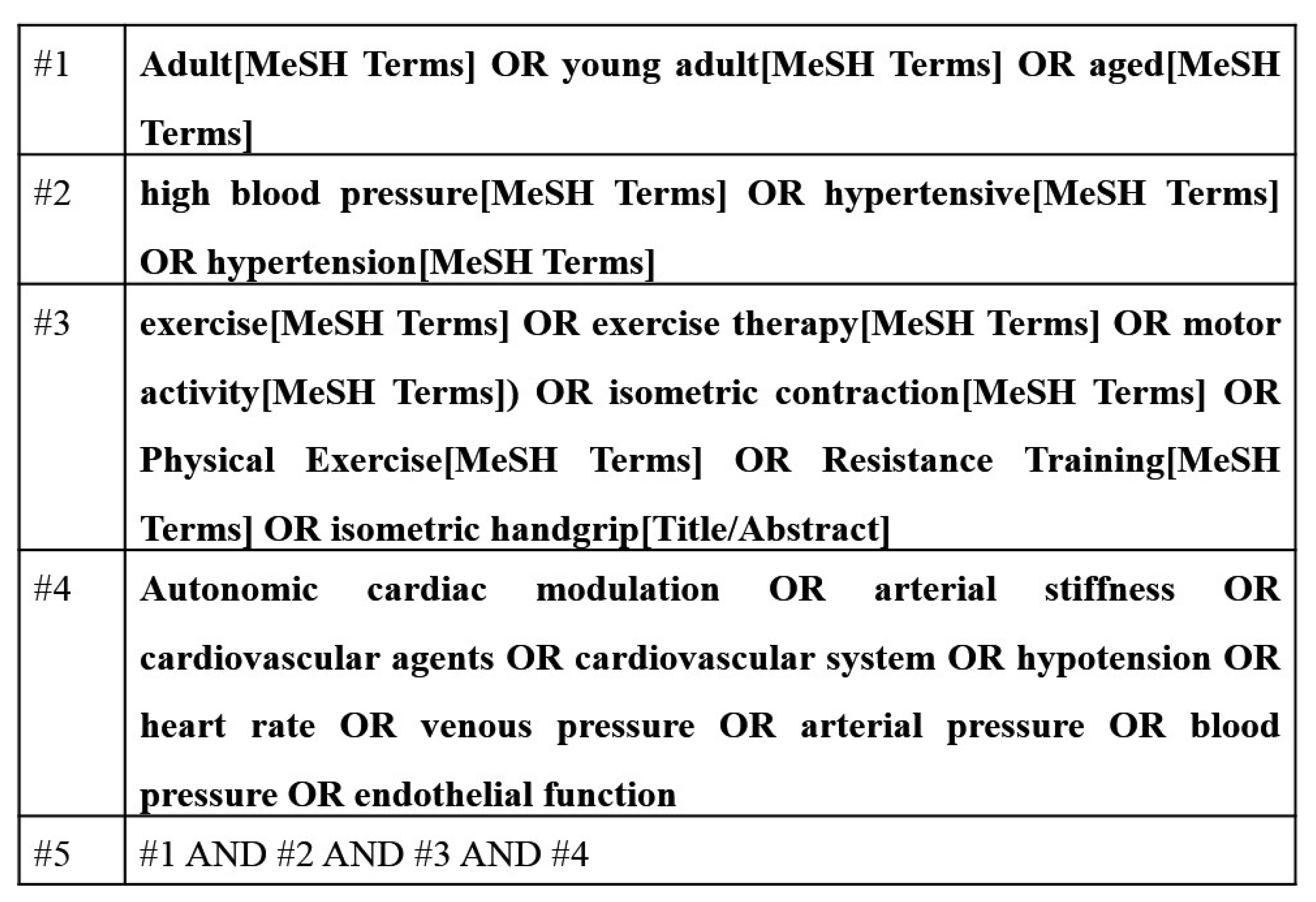
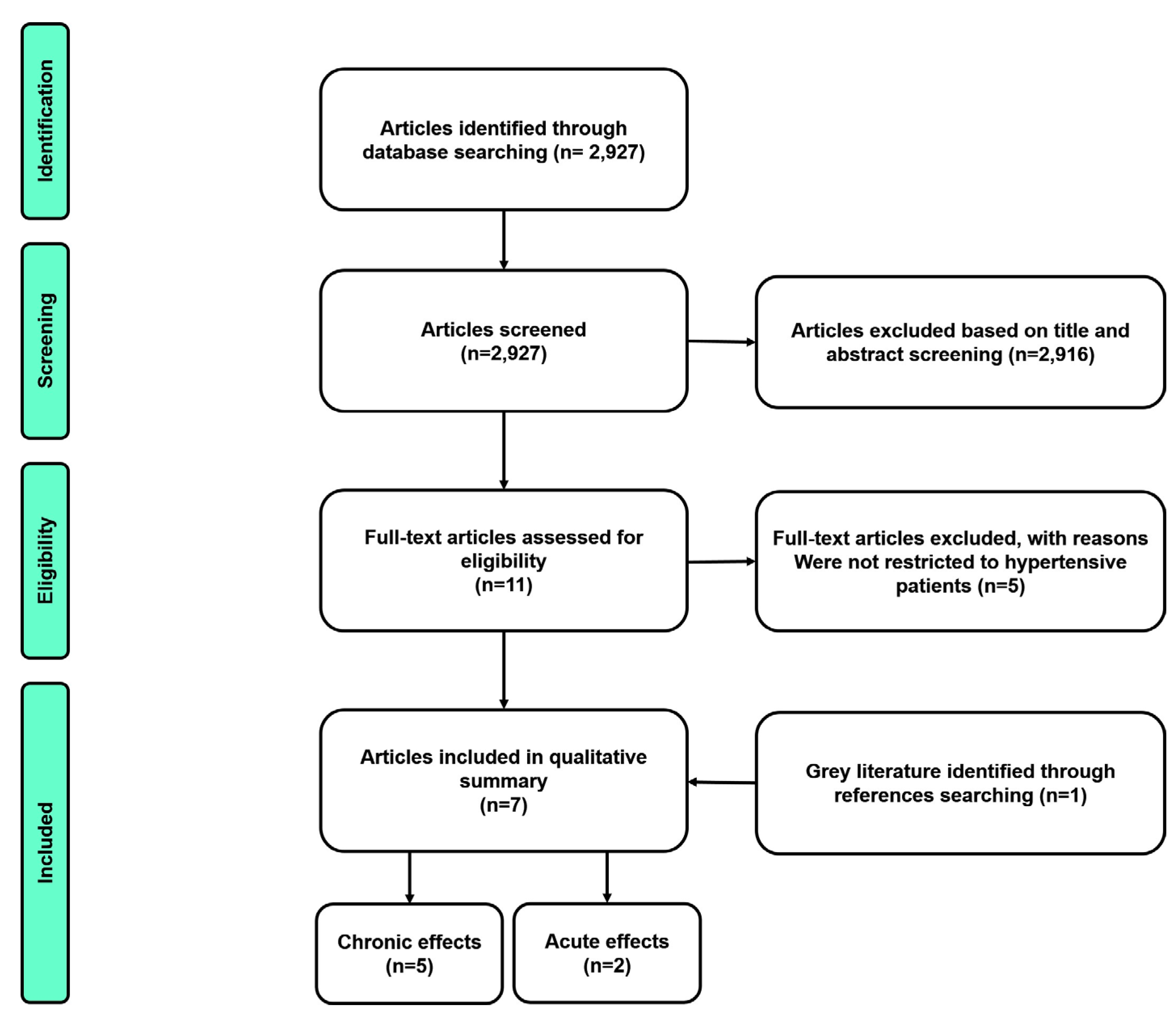
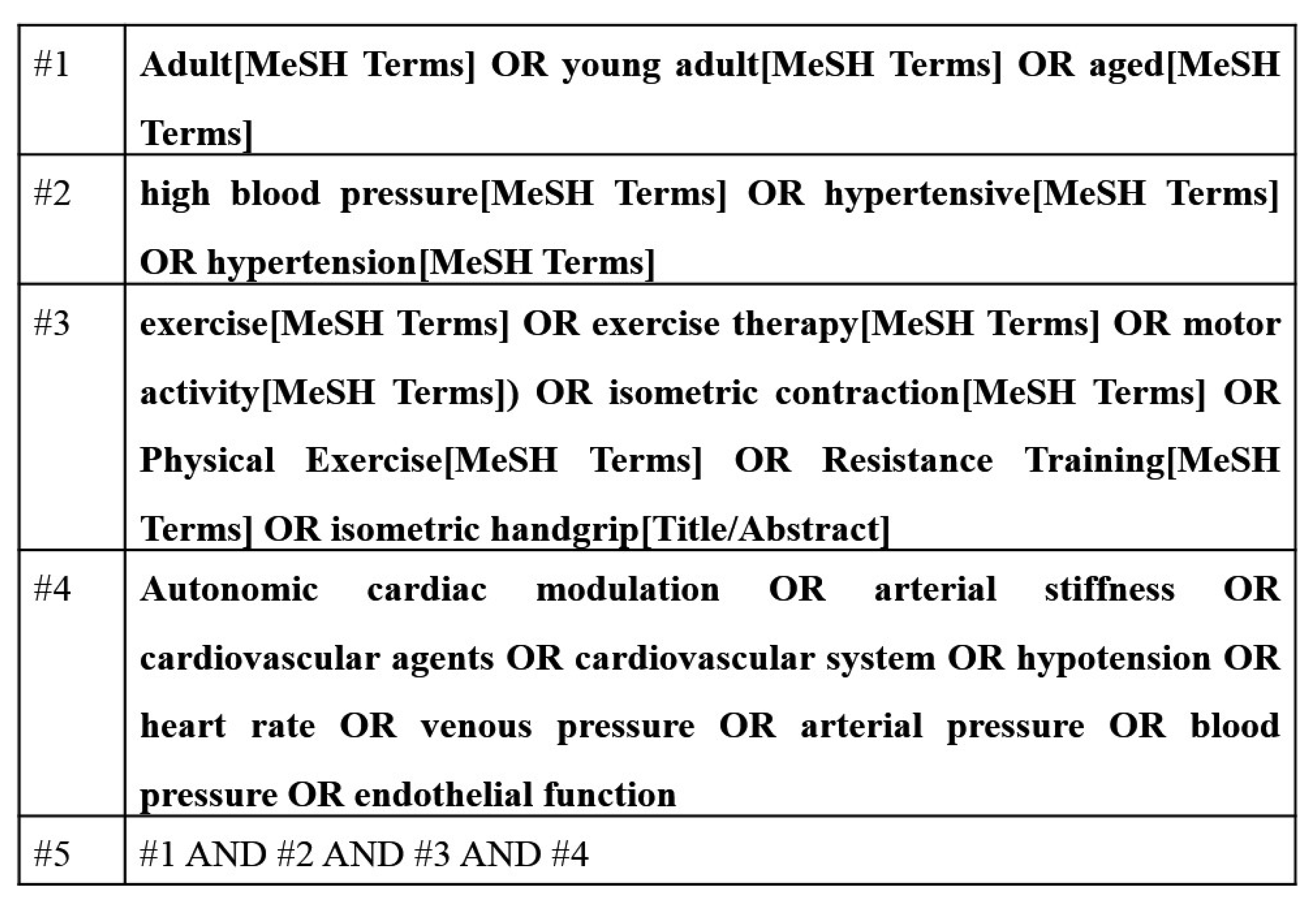
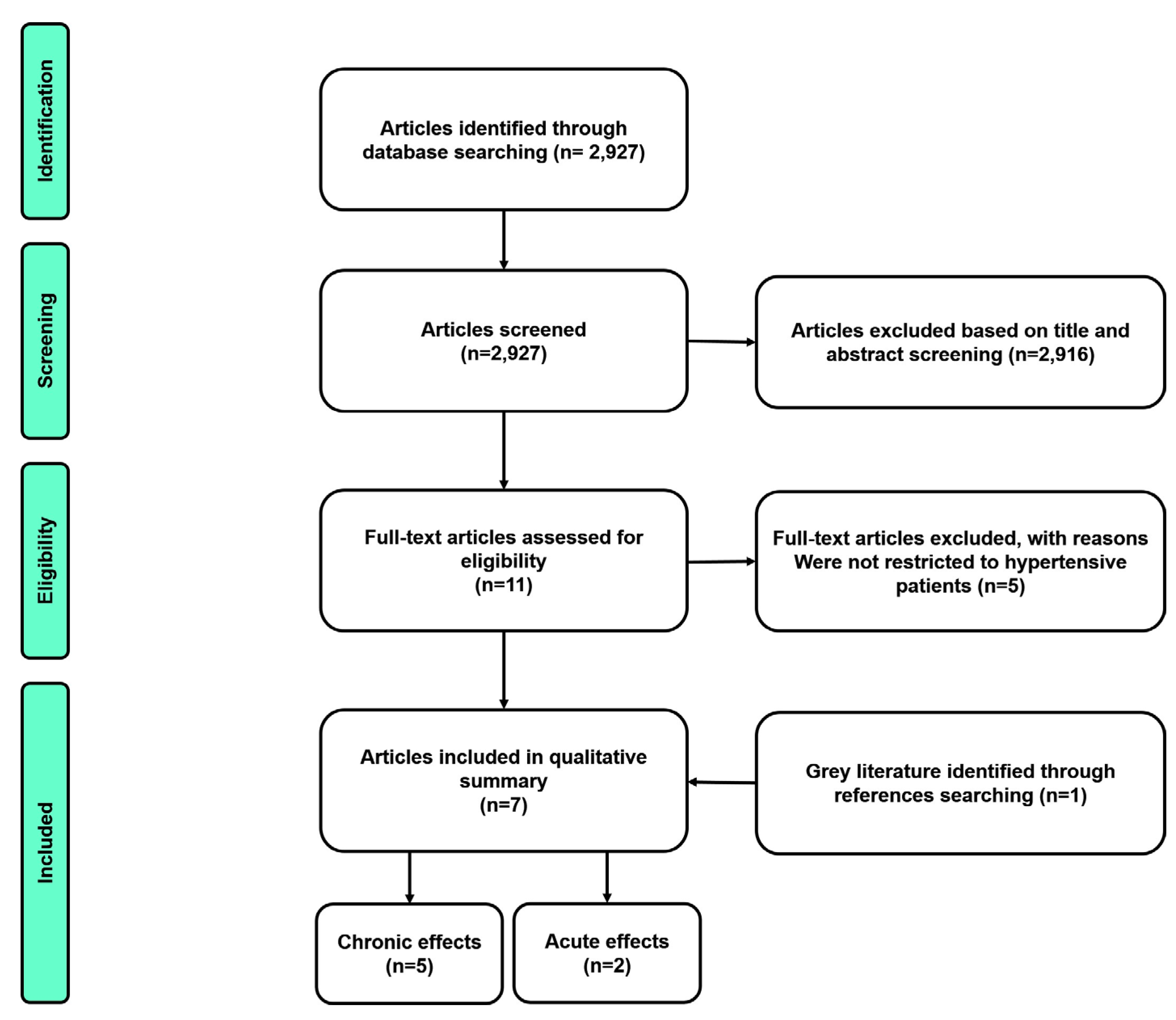
2. Material and Methods
3. Results
4. Discussion
Author Contributions
Conflicts of Interest
References
- Franco, V.; Oparil, S.; Carretero, O.A. Hypertensive therapy: Part I. Circulation 2004, 109, 2953–2958. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H.; Coeckelberghs, E.; Vanhees, L. Impact of resistance training on blood pressure and other cardiovascular risk factors: A meta-analysis of randomized, controlled trials. Hypertension 2011, 58, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S. Isometric handgrip exercise and resting blood pressure: A meta-analysis of randomized controlled trials. J. Hypertens. 2010, 28, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.; Wiles, J.; Swaine, I. Effect of isometric exercise on resting blood pressure: A meta analysis. J. Hum. Hypertens. 2010, 24, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Carlson, D.J.; Dieberg, G.; Hess, N.C.; Millar, P.J.; Smart, N.A. Isometric exercise training for blood pressure management: A systematic review and meta-analysis. Mayo Clin. Proc. 2014, 89, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Inder, J.D.; Carlson, D.J.; Dieberg, G.; McFarlane, J.R.; Hess, N.C.; Smart, N.A. Isometric exercise training for blood pressure management: A systematic review and meta-analysis to optimize benefit. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2015, 39, 88–94. [Google Scholar] [CrossRef] [PubMed]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/esc guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [PubMed]
- Jin, Y.Z.; Yan, S.; Yuan, W.X. Effect of isometric handgrip training on resting blood pressure in adults: A meta-analysis of randomized controlled trials. J. Sports Med. Phys. Fit. 2017, 57, 154–160. [Google Scholar]
- Brook, R.D.; Appel, L.J.; Rubenfire, M.; Ogedegbe, G.; Bisognano, J.D.; Elliott, W.J.; Fuchs, F.D.; Hughes, J.W.; Lackland, D.T.; Staffileno, B.A.; et al. Beyond medications and diet: Alternative approaches to lowering blood pressure: A scientific statement from the American heart association. Hypertension 2013, 61, 1360–1383. [Google Scholar] [CrossRef] [PubMed]
- Moreira, S.R.; Cucato, G.G.; Terra, D.F.; Ritti-Dias, R.M. Acute blood pressure changes are related to chronic effects of resistance exercise in medicated hypertensives elderly women. Clin. Physiol. Funct. Imaging 2014, 36, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Nobrega, A.C. The subacute effects of exercise: Concept, characteristics, and clinical implications. Exerc. Sport Sci. Rev. 2005, 33, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; La Gerche, A.; Coombes, J.S. Exercise and cardiovascular risk in patients with hypertension. Am. J. Hypertens. 2015, 28, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: Testex. Int. J. Evid. Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Porro, T.; Colombo, F.; Azzola, F.L.; Orlandi, L.; Merati, M.G.; Libretti, A. Diurnal blood pressure variability in essential hypertension and vascular reactivity to isometric stress. J. Hum. Hypertens. 1995, 9, 329–335. [Google Scholar] [PubMed]
- Araujo, C.G.; Duarte, C.V.; Goncalves Fde, A.; Medeiros, H.B.; Lemos, F.A.; Gouvea, A.L. Hemodynamic responses to an isometric handgrip training protocol. Arq. Bras. Cardiol. 2011, 97, 413–419. [Google Scholar] [PubMed]
- Olher, R.R.; Bocalini, D.S.; Bacurau, R.F.; Rodriguez, D.; Figueira, A., Jr.; Pontes, F.L., Jr.; Navarro, F.; Simoes, H.G.; Araujo, R.C.; Moraes, M.R. Isometric handgrip does not elicit cardiovascular overload or post-exercise hypotension in hypertensive older women. Clin. Interv. Aging 2013, 8, 649–655. [Google Scholar]
- Carlson, D.J.; Inder, J.; Palanisamy, S.K.; McFarlane, J.R.; Dieberg, G.; Smart, N.A. The efficacy of isometric resistance training utilizing handgrip exercise for blood pressure management: A randomized trial. Medicine 2016, 95, e5791. [Google Scholar] [CrossRef] [PubMed]
- Badrov, M.B.; Horton, S.; Millar, P.J.; McGowan, C.L. Cardiovascular stress reactivity tasks successfully predict the hypotensive response of isometric handgrip training in hypertensives. Psychophysiology 2013, 50, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Stiller-Moldovan, C.; Kenno, K.; McGowan, C.L. Effects of isometric handgrip training on blood pressure (resting and 24 h ambulatory) and heart rate variability in medicated hypertensive patients. Blood Press. Monit. 2012, 17, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Peters, P.G.; Alessio, H.M.; Hagerman, A.E.; Ashton, T.; Nagy, S.; Wiley, R.L. Short-term isometric exercise reduces systolic blood pressure in hypertensive adults: Possible role of reactive oxygen species. Int. J. Cardiol. 2006, 110, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.C.; McCartney, N.; Kamath, M.V.; Wiley, R.L. Isometric training lowers resting blood pressure and modulates autonomic control. Med. Sci. Sports Exerc. 2003, 35, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Millar, P.J.; Bray, S.R.; McGowan, C.L.; MacDonald, M.J.; McCartney, N. Effects of isometric handgrip training among people medicated for hypertension: A multilevel analysis. Blood Press. Monit. 2007, 12, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, E.B.; Liao, D.; Chambless, L.E.; Prineas, R.J.; Evans, G.W.; Heiss, G. Hypertension, blood pressure, and heart rate variability: The atherosclerosis risk in communities (ARIC) study. Hypertension 2003, 42, 1106–1111. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author (year) | Session/Groups | Age (Years) | Baseline SBP | Baseline DBP | N | Sex | R | Duration of Hypertension | Medicine | Quality Score (%) * |
|---|---|---|---|---|---|---|---|---|---|---|
| ACUTE STUDIES | ||||||||||
| Olher et al., (2013) [19] | HS e CS | 64 ± 1 | 121 ± 7 | 72 ± 6 | 12 | Female | Yes | NI | βb, ACE, Diu, ARB and CCB | 7 (100.0) |
| Porro et al., (1995) [17] | HS | 43 ± 3 | Ndip—144 ± 3 Dip—134 ± 3 | Ndip—96 ± 3 Dip—91 ± 3 | 50 | Both | NA | NI | NI | 3 (42.9) |
| CHRONIC STDUIES | ||||||||||
| Carlson et al., (2016) [20] | GC GT | CG—54 ± 8 TG—52 ± 8 | CG—128 ± 15 TG—136 ± 12 | CG—74 ± 9 TG—77 ± 7 | CG—20 TG—20 | Both | Yes | NI | ACE, Diu, ARB, CCB, αAA and unmedicated | 10 (66.7) |
| Badrov et al., (2013) [21] | GC GT | CG—63 ± 9 TG—65 ± 7 | CG—130 ± 17 TG—129 ± 16 | CG—73 ± 12 TG—72 ± 9 | CG—12 TG—12 | Both | Yes | ≥4 months | ACE, Diu, CCB, and unmedicated | 13 (86.7) |
| Stiller-Moldovan et al., (2012) [22] | CG TG | CG—63 ± 6 TG—60 ± 8 | CG—118 ± 14 TG—114 ± 13 | CG—68 ± 4 TG—61 ± 12 | CG—9 TG—11 | Both | Yes | >4 months | βb, ACE, Diu, ARB and CCB | 10 (66.7) |
| Peters et al., (2006) [23] | TG | 52 ± 5 | 146 ± 11 | 90 ± 7 | 10 | Both | NA | >6 months | NI | 6 (40.0) |
| Taylor et al., (2003) [24] | CG TG | CG—64 ± 6 TG—69 ± 6 | CG—152 ± 8 TG—156 ± 9 | CG—87 ± 11 TG—82 ± 9 | CG—8 TG—9 | Both | Yes | CG—9.2 years TG—9.4 years | βb, ACE, Diu, CCB, and unmedicated | 11 (11.3) |
| Author (Year) | Session | Variables Analyzed | Exercise Protocol | Assessment Duration | Main Results |
|---|---|---|---|---|---|
| Olher et al., (2013) [19] | HS1, HS2, and CS | SBP, DBP, MBP, HR, and RPP | HS1 = 20 × 10 s; RI NI; 30% MVC. HS2 = 20 × 10 s; RI NI; 50% MVC. | 60 min | HS1, HS2 e SC = → SBP, DBP, MBP, HR, and RPP. |
| Porro et al., (1995) [17] | HS | SVR and CI | 1 × 3 min; 30% MVC | 24 h | Non-dippers = ↑ SVR and CI Dippers = → SVR; ↑ CI |
| Author | Variables Analysed | Training Protocol | Frequency | Duration | Main Results |
|---|---|---|---|---|---|
| Carlson et al., (2016) [20] | SBP, DBP, MBP, and HR | UN arms:4 × 2 min.; 3 min. RI; 30% MVC. | 3 × / weeks | 8 weeks | ↓ SBP, MBP |
| Badrov et al., (2013) [21] | SBP, DBP, MBP, and PP | Alternated arms: 4 × 2 min.; 1 min. RI; 30% MVC. | 3 × / weeks | 10 weeks | ↓ SBP, DBP, MBP, and PP (at rest) ↓ SBP (mental and physical stress) |
| Stiller-Moldovan et al., (2012) [22] | SBP, DBP, MBP (clinic and 24 h), and HRV | Alternated arms: 4 × 2 min.; 1 min. RI; 30% MVC. | 3 × / weeks | 8 weeks | →SBP, DBP, MBP (clinic and 24 h), and → HRV |
| Peters et al., (2006) [23] | SBP, DBP, MBP, and oxidative stress | Alternated arms: 4 × 45 s; 1 min. RI; 50% MVC. | 3 × /weeks | 6 weeks | ↓ SBP, and oxidative stress → DBP and MBP |
| Taylor et al., (2003) [24] | SBP, DBP, MBP, HRV, and BPV | Alternated arms: 4 × 2 min.; 1 min. RI; 30% MVC. | 3 × / weeks | 10 weeks | ↓ SBP and MBP; →DBP; ↑ HRV and BPV |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farah, B.Q.; Germano-Soares, A.H.; Rodrigues, S.L.C.; Santos, C.X.; Barbosa, S.S.; Vianna, L.C.; Cornelissen, V.A.; Ritti-Dias, R.M. Acute and Chronic Effects of Isometric Handgrip Exercise on Cardiovascular Variables in Hypertensive Patients: A Systematic Review. Sports 2017, 5, 55. https://doi.org/10.3390/sports5030055
Farah BQ, Germano-Soares AH, Rodrigues SLC, Santos CX, Barbosa SS, Vianna LC, Cornelissen VA, Ritti-Dias RM. Acute and Chronic Effects of Isometric Handgrip Exercise on Cardiovascular Variables in Hypertensive Patients: A Systematic Review. Sports. 2017; 5(3):55. https://doi.org/10.3390/sports5030055
Chicago/Turabian StyleFarah, Breno Q., Antônio H. Germano-Soares, Sergio Luiz C. Rodrigues, Camila X. Santos, Sávio S. Barbosa, Lauro C. Vianna, Véronique A. Cornelissen, and Raphael M. Ritti-Dias. 2017. "Acute and Chronic Effects of Isometric Handgrip Exercise on Cardiovascular Variables in Hypertensive Patients: A Systematic Review" Sports 5, no. 3: 55. https://doi.org/10.3390/sports5030055