The Effectiveness of Hard Martial Arts in People over Forty: An Attempted Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Risk of Bias Assessment
2.3. Data Extraction
2.4. Analysis
3. Results
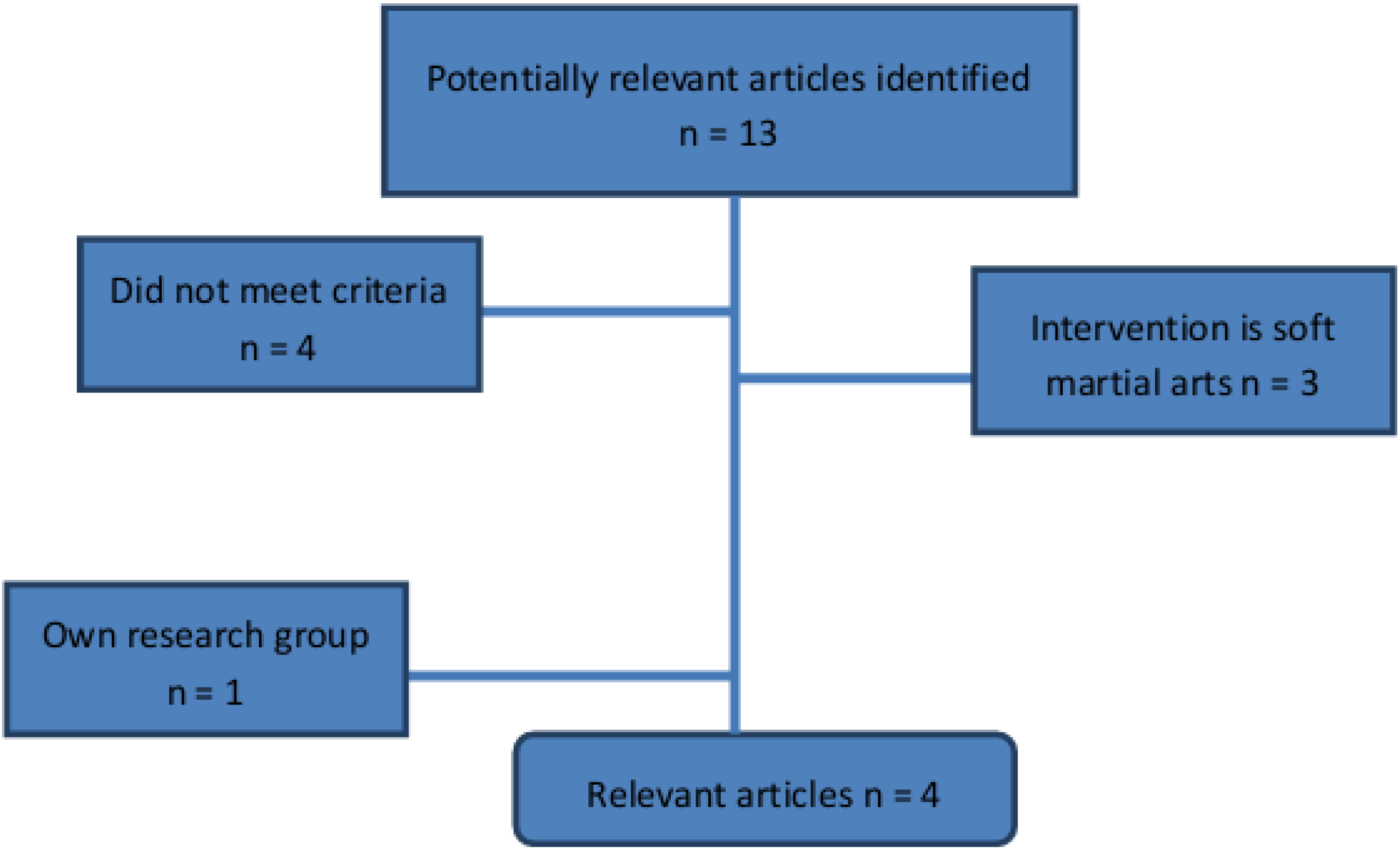
3.1. Search Strategy

3.2. Risk of Bias Assessment

{kind=link}
| Author Year Country | Design | Participants | Intervention | Reported Outcomes | Notes |
|---|---|---|---|---|---|
| Brudnak et al. 2001 [19] Wisconsin, USA | SAI | IG: Community-dwelling volunteers N = 12: ♂/♀ not mentioned Mean age: not mentioned (range: 63–81) RG: - Drop-out: 50%, after first class | IG: Taekwondo 17 weeks once per week, 1 h total 1020 min RG: - | Single leg stance: (s) Sit-and-reach (cm) Pushups (number in 30 s) | Participants measured each other in pairs |
| Cromwell et al. 2007 [9] Texas, USA | CT | IG: Community-dwelling volunteers N = 20: ♂: 3, ♀: 17 Mean age: 73 years (range: 60–83) RG: Community-dwelling volunteers N = 20: ♂: 7, ♀: 13 Mean age: 74 years (range: 59–88) Drop-out: 0 | IG: Taekwondo 11 weeks, twice per week, 1 h total 1320 min RG: normal daily physical activity | Single leg stance (s) Multidirectional reach test (cm) Sit-and-reach (cm) Timed up-and-go (s) Cadence (steps/s) Gait stability ratio (steps/s) Walking velocity (m/s) | |
| Chateau et al. 2010 [19] Canada | SAI | IG: Working 50 years old volunteers N = 15:♂ 15, ♀ 0 Median age: 57 years (range: 51–58) RG: - Drop-out: 7 | IG: Karate 12 months 3 times per week. 1.5 h total: 14040 min RG: - | MOS 36 item Short Form Health Survey Beck Depression Inventory Reaction time (s) Pronation and supination (s and Hz) Finger tapping (s and Hz) Sway path (mm) Sway area (mm2) Sway velocity (mm/s) Effort by ergometric bycicle (units not mentioned) | |
| Jansen et al. 2012 [20] Germany | CT | IG: Community-dwelling volunteers N = 12:♂ 4, ♀ 8 Mean age 74 years (range 69–81) RG1: Community-dwelling volunteers N = 12: ♂ 5, ♀ 7 Mean age 83 years (range 72–93) RG2: N = 12: ♂ 5, ♀ 7 Mean age 75 years (range 67–82) RG3: N = 9: ♂ 1, ♀ 7 8 Mean age 83 years (range 70–89) Drop-out: 15 | IG: Karate-Do 3–6 months 20 training sessions, 1 h total 1200 min RG1: Physical exercise training 20 training sessions, 1h total 1200 min RG2: Cognitive training 20 training sessions, 1h total 1200 min RG3: normal daily physical activity | Number-connection test (min) Number-symbol test (number of correct symbols) Digit-span test (number of span) Figure test (units not mentioned) Block-tapping test (number of blocks) Depression scale (score) |
| Brudnak et al. [18] | Cromwell et al. [9] | Chateau et al. [19] | Jansen et al. [20] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Rating | Points | Rating | Points | Rating | Points | Rating | Points | ||
| 1 | Randomization | No | (0) | No | (0) | No | (0) | No | (0) |
| 2 | Intention to treat analysis | No | (0) | No | (0) | Partly | (1) | Partly | (1) |
| 3 | Blinding assessors | No | (0) | Inadequate | (1) | No | (0) | No | (0) |
| 4 | Blinding participants | No | (0) | No | (0) | No | (0) | No | (0) |
| 5 | Blinding providers | No | (0) | No | (0) | No | (0) | No | (0) |
| 6 | Baseline characteristics | No RG | (0) | No | (0) | No RG | (0) | No, age difference | (0) |
| 7 | Care programs identical | No | (0) | No | (0) | No | (0) | Partly | (1) |
| 8 | Inclusion criteria | Inadequate | (1) | Inadequate | (1) | Clear | (2) | No | (0) |
| 9 | Exclusion criteria | Inadequate | (1) | No | (0) | Clear | (2) | No | (0) |
| 10 | Interventions | Not clear | (0) | Clear | (2) | Clear | (2) | Not clear | (0) |
| 11 | Outcome measures clear | Clear | (2) | Clear | (2) | Inadequate | (1) | Inadequate | (1) |
| 12 | Outcomes appropriately measured | Appropriate | (2) | No | (0) | Appropriate | (2) | Inadequate | (1) |
| 13 | Outcomes useful in daily activities | Adequate | (1) | Adequate | (1) | Adequate | (1) | Adequate | (1) |
| 14 | Surveillance and duration | Inadequate | (1) | Good | (2) | Good | (2) | Inadequate | (1) |
| 15 | Primary outcome defined | Inadequate | (1) | No | (0) | No | (0) | No | (0) |
| 16 | Compliance | Not clear | (0) | Inadequate | (1) | Inadequate | (1) | Clear | (2) |
| 17 | Adverse effects | Not described | (0) | Not described | (0) | Not described | (0) | Not described | (0) |
| 18 | Replicable | Partly | (1) | Partly | (1) | Yes | (2) | Partly | (1) |
| Quality Score | 28% (10/36) | 31% (11/36) | 44% (16/36) | 25% (9/36) | |||||
3.3. Study Characteristics
3.4. Methodological Characteristics
3.5. Outcome Measurements
3.6. Analysis
| Index | |||
|---|---|---|---|
| Group | |||
| Article | Measurement | Pre | Post |
| mean | mean | ||
| Brudnak | Sit-and-reach (cm) | Increase | >8.9 |
| [18] | Pushups (number per 30 s) | Increase | 1.8 |
| Single leg stance (s): Right | Increase | >16 | |
| Left | Increase | 16 |
| Index | Reference | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Group | |||||||||||
| Article | Measurement | Pre | Post | Sign. | Pre | Post | Sign. | Sign. | ||||
| mean | sd | mean | sd | within groups | mean | sd | mean | sd | within groups | between groups | ||
| Cromwell | Single leg stance (s) | 17.0 | 19.4 | 27.2 | 39.4 | Ns | 22.8 | 35.3 | 21.5 | 39.1 | Ns | Ns |
| [9] | Multidirectional reach test (cm) | |||||||||||
| Front | 23.4 | 7.8 | 27.0 | 8.5 | Ns | 23.8 | 3.3 | 23.1 | 7.0 | Ns | Ns | |
| Back | 20.7 | 5.6 | 24.1 | 4.9 | <0.05 | 21.5 | 4.8 | 21.8 | 6.4 | Ns | Ns | |
| Right | 15.0 | 4.8 | 19.2 | 6.2 | <0.05 | 14.8 | 4.3 | 14.9 | 4.6 | Ns | Ns | |
| Left | 14.3 | 5.6 | 18.8 | 8.8 | <0.05 | 13.7 | 4.8 | 15.3 | 5.1 | Ns | Ns | |
| Sit-and-reach (cm) | 18.9 | 7.9 | 21.0 | 7.0 | <0.05 | 20.9 | 8.3 | 19.8 | 8.1 | Ns | Ns | |
| Timed up-and-go (s) | 9.5 | 1.7 | 8.6 | 2.1 | <0.05 | 11.3 | 2.7 | 10.9 | 2.9 | Ns | <0.05 | |
| Cadence (steps/s) | 2.1 | 0.2 | 2.2 | 0.4 | Ns | 2.0 | 0.2 | 2.0 | 0.2 | Ns | <0.05 | |
| Gait stability ratio (steps/m) | 2.4 | 0.5 | 2.0 | 0.4 | <0.05 | 2.4 | 0.7 | 2.4 | 0.5 | Ns | Ns | |
| Walking velocity (m/s) | 0.9 | 0.2 | 1.1 | 0.3 | <0.05 | 0.9 | 0.2 | 0.9 | 0.2 | Ns | Ns |
| Article | Measurement | Pre | 6 months | 12 months | Sign. pre vs. | Sign. pre vs. | |||
|---|---|---|---|---|---|---|---|---|---|
| sd | sd | sd | |||||||
| Chateau | Physical score | 29.8 | 1.1 | Nm | Nm | 34.7 | 1.1 | Nm | 0.01 |
| [19] | Mental score | 50.9 | 1.3 | Nm | Nm | 50.2 | 1.3 | Nm | 0.67 |
| Physical functioning (score) | 81.9 | 1.9 | Nm | Nm | 88.0 | 1,9 | Nm | 0.02 | |
| Physical status (score) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | ||
| Body pain (score) | 69.9 | 2.2 | Nm | Nm | 84.5 | 2.4 | Nm | 0.04 | |
| General health (score) | 13.9 | 0.7 | Nm | Nm | 16.4 | 0.7 | Nm | 0.01 | |
| Vitality (score) | 61.0 | 1.6 | Nm | Nm | 69.12 | 1.6 | Nm | <0.01 | |
| Social functioning (score) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 0.77 | |
| Emotional status (score) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 0.50 | |
| Mental health (score) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 0.95 | |
| Reaction time (s) Right | 0.23 | 0.01 | 0.23 | 0.01 | 0.23 | 0.01 | 0.71 | 0.86 | |
| Left | 0.20 | 0.01 | 0.23 | 0.01 | 0.24 | 0.01 | 0.01 | 0.01 | |
| Pronation and supination | |||||||||
| Precision (s) Right | 0.01 | 0.02 | −0.02 | 0.02 | −0.26 | 0.02 | 0.04 | 0.11 | |
| Left | −0.03 | 0.02 | −0.04 | 0.02 | −0.36 | 0.02 | 0.41 | 0.66 | |
| Regularity Right | 0.06 | 0.01 | 0.06 | 0.01 | 0.06 | 0.01 | 0.37 | 0.96 | |
| Left | 0.05 | 0.01 | 0.05 | 0.01 | 0.05 | 0.01 | 0.15 | 0.82 | |
| Maximum (Hz) Right | 5.43 | 0.32 | 6.07 | 0.30 | 6.10 | 0.32 | <0.01 | 0.04 | |
| Left | 5.07 | 0.24 | 5.85 | 0.23 | 5.88 | 0.26 | <0.01 | <0.01 | |
| Finger tapping | |||||||||
| Precision (s) Right | −0.09 | 0.01 | −0.06 | 0.01 | −0.06 | 0.01 | 0.01 | 0.10 | |
| Left | −0.09 | 0.01 | −0.06 | 0.01 | −0.06 | 0.02 | 0.09 | 0.28 | |
| Regularity Right | 0.09 | 0.01 | 0.06 | 0.01 | 0.06 | 0.01 | 0.03 | 0.08 | |
| Left | 0.07 | 0.01 | 0.07 | 0.01 | 0.08 | 0.01 | 0.49 | 0.42 | |
| Maximum Right | 6.72 | 0.27 | 6.35 | 0.27 | 6.23 | 0.30 | 0.27 | 0.24 | |
| Left | 6.09 | 0.39 | 6.98 | 0.39 | 6.85 | 0.43 | 0.10 | 0.21 | |
| Mean sway Eyes (mm) open | 5.6 | 0.5 | 6.0 | 0.5 | 6.1 | 0.5 | 0.36 | 0.36 | |
| Closed | 6.71 | 0.6 | 5.9 | 0.6 | 5.9 | 0.6 | 0.05 | 0.19 | |
| Transversal sway (mm) Open | 3.0 | 0.2 | 3.1 | 0.2 | 3.1 | 0.2 | 0.46 | 0.57 | |
| Closed | 3.9 | 0.4 | 3.4 | 0.3 | 3.3 | 0.4 | 0.10 | 0.17 | |
| Sagittal sway (mm) Open | 4.1 | 0.5 | 4.4 | 0.5 | 4.6 | 0.5 | 0.43 | 0.40 | |
| Closed | 4.6 | 0.5 | 4.1 | 0.4 | 4.2 | 0.5 | 0.12 | 0.40 | |
| Sway area (mm2) Open | 316.6 | 40.0 | 315.2 | 38.6 | 321.3 | 0.8 | 0.96 | 0.80 | |
| Closed | 507.9 | 87.5 | 404.9 | 84.1 | 399.2 | 89.3 | 0.09 | 0.22 | |
| Sway velocity (mm/s) Open | 11.4 | 0.9 | 10.6 | 0.9 | 10.5 | 0.9 | 0.16 | 0.33 | |
| Closed | 17.5 | 1.9 | 14.4 | 1.8 | 14.4 | 1.9 | 0.02 | 0.01 | |
| Sway intensity (mm) Open | 4.4 | 0.3 | 4.4 | 0.3 | 4.4 | 0.3 | 0.97 | 0.93 | |
| Closed | 6.2 | 0.5 | 5.4 | 0.5 | 5.4 | 0.5 | 0.01 | 0.04 | |
| Duration of effort (min) | 10.9 | 0.5 | Nm | Nm | 12.2 | 0.6 | Nm | 0.04 | |
| Maximal power developed | 198.0 | 10.0 | 214.8 | 10.2 | 0.01 | 0.01 | |||
| Maximal heart rate (beats/min) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | |
| Individual effort profile | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | |
| Beck depression score | 9.8 | 1.1 | 4.9 | 1.0 | 4.9 | 1.1 | 0.01 | <0.01 |
| Article | Measurement | RG | EG | CT | Karate | Effect of | Effect of | Interaction | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | group | time of testing | |||
| Jansen | Cognitive speed | |||||||||||
| [20] | Number-connection test (s) | 45.51 | 3.8 | 29.72 | 3.45 | 23.83 | 3.28 | 29.31 | 3.41 | 6.31 * | 0.01 | 0.125 |
| Number-symbol test (items) | 26.34 | 2.95 | 41.11 | 2.41 | 41.11 | 2.41 | 35.82 | 2.51 | 4.72 * | 1.56 | 0.86 | |
| Memory performance | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | ||||
| Digit-span test (number) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 1.5 | 0.22 | 1.6 | |
| Figure test (score) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 1.63 | 1.01 | 0.74 | |
| Block-tapping test (number) | Nm | Nm | Nm | Nm | Nm | Nm | Nm | Nm | 1.03 | 1.03 | 0.85 | |
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |||||
| Depression score | 11 | 12.5 | 13.5 | 13 | 10 | 18 | 13 | 8 | 0.81 | 0.84 | 4.12 |
4. Discussion and Conclusions
Author Contributions
Conflicts of Interest
References
- American College of Sports Medicine. Acms’s Resource Manual for Guidelines for Exercise Testing and Prescription, 6th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2001; pp. 57–90. [Google Scholar]
- Kroes, G.; de Greef, M. National initiatives for the promotion of physical activity for older persons in the Netherlands. J. Aging Phys. Act 2000, 8, 431–435. [Google Scholar]
- Lobstein, T.; Rigby, N.; Leach, R. EU platform on diet, physical activity and health. Available online: http://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/iotf_en.pdf (accessed on 15 March 2005).
- Cress, M.E; Buchner, D.M.; Questad, K.A.; Esselman, P.C.; de Lateur, B.J.; Schwartz, R.S.A. Exercise: Effects on physical functional performance in independent older adults. J Gerontol. Med. Sci. 1995, 54A, 242–248. [Google Scholar]
- Buchner, D.; Cress, M.E.; de Lateur, B.J.; Esselman, P.C.; Margherita, A.J.; Price, R.; Wagner, E.H. A comparison of the effects of three types of endurance training on balance and other fall risk factors in older adults. Aging Clin. Exp. Res. 1997, 9, 112–119. [Google Scholar] [CrossRef]
- Cameron, I.D.; Gillespie, L.D.; Robertson, M.C.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Josephson, K.R. The epidemiology of falls and syncope. Clin. Geriatr. Med. 2002, 18, 141–158. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelber, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Cromwell, R.L.; Meyers, P.M.; Meyers, P.E.; Newton, R.A. Taekwondo: An effective exercise for improving balance and walking ability in older adults. J. Gerontol.: Med. Sci. 2007, 62A, 641–646. [Google Scholar]
- Gauchard, G.C.; Gangloff, P.; Jeandel, C.; Perrin, P.P. Influence of regular proprioceptive and bioenergetic physical activities on balance control in elderly women. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 846–850. [Google Scholar] [CrossRef]
- Corcoran, J.; Farkas, E.; Sobel, S. The Original Martial Arts Encyclopedia: Tradition, History, Pioneers; Pro-Action Publications: Los Angeles, CA, USA, 1993. [Google Scholar]
- Alexandrov, A.; Frolov, A.A.; Massion, J. Biomechanical analysis of movement strategies in human forward trunk bending. I. Modeling. Biol. Cybern. 2001, 84, 425–434. [Google Scholar] [CrossRef]
- Fong, SS.; Ng, G.Y. Does taekwondo training improve physical fitness? Phys. Ther. Sport 2011, 12, 100–106. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Li, Y.; Devault, C.N.; van Oteghen, S. Effects of extended tai chi intervention on balance and selected motor functions of the elderly. Am. J. Chin. Med. 2007, 35, 383–391. [Google Scholar] [CrossRef]
- Pons van Dijk, G.; Lenssen, A.F.; Leffers, P.; Kingma, H.; Lodder, J. Taekwondo training improves balance in volunteers over forty. Front. Aging Neurosci. 2013, 5, 10. [Google Scholar] [CrossRef]
- Douris, P.; Chinan, A.; Gomez, M.; Aw, A.; Steffens, D.; Weiss, S. Fitness levels of middle aged martial art practicioners. Br. J. Sports Med. 2004, 38, 143–147. [Google Scholar] [CrossRef]
- Brudnak, M.A.; Dundero, D.; van Hecke, F.M. Are the “hard” martial arts, such as the korean martial art, taekwon-do, of benefit to senior citizens? Med. Hypotheses 2002, 59, 485–491. [Google Scholar] [CrossRef]
- Chateau-Degat, M.-L.; Papouin, G.; Saint-Val, P.; Lopez, A. Effect of adapted karate training on quality of life and body balance in 50-year-old men. Open Access J. Sports Med. 2010, 1, 143–150. [Google Scholar]
- Jansen, P.; Dahmen-Zimmer, K. Effects of cognitive, motor, and karate training on cognitive functioning and emotional well-being of elderly people. Front. Psychol. 2012, 3, 40. [Google Scholar] [CrossRef] [Green Version]
- Leplege, A.; Ecosse, E.; Pouchot, J.; Coste, J.; Perneger, T. Le questionnaire MOS SF-36: Manuel de L’itilisateur et Guide de L’interpretation des Scores; Editions Estem: Paris, France, 2001. [Google Scholar]
- Pons van Dijk, G.; Leffers, P.; Lodder, J. Feasibility, safety and subjective experience of a one-year WTF-Taekwondo training course for middle-aged volunteers: The Sekwondo study. Gazz. Med. Ital. Arch. Sci. Med. 2013, 172, 433–441. [Google Scholar]
- Tsang, T.W.; Kohn, M.; Chow, C.M.; Singh, M.F. Health benefits of kung fu: A systematic review. J. Sports Sci. 2008, 26, 1249–1267. [Google Scholar]
Appendixes
| Item | Points | Rating |
|---|---|---|
| 2 | Method did not allow disclosure of assignment |
| 1 | Small but possible chance of disclosure of assignment or unclear | |
| 0 | Quasi-randomized or open list/tables | |
| 2 | Drop outs well described and accounted for in analysis |
| 1 | Drop outs described and analysis is not possible | |
| 0 | No mention, inadequate mention or obvious differences and no adjustment | |
| 2 | Effective action taken to blind assessors |
| 1 | Small or moderate chance of unblinding of assessors | |
| 0 | Not mentioned or not possible | |
| 2 | Effective action taken to blind participants |
| 1 | Small or moderate chance of unblinding of participants | |
| 0 | Not possible or not mentioned, or possible but not done | |
| 2 | Effective action taken to blind intervention providers |
| 1 | Small or moderate chance of unblinding of intervention providers | |
| 0 | Not possible or not mentioned, or possible but not done | |
| 2 | Good comparability of groups, or confounding adequately adjusted for in analysis |
| 1 | Confounding small; mentioned but not adjusted for | |
| 0 | Large potential for confounding, or not discussed | |
| 2 | Care programs clearly identical |
| 1 | Clear but trivial differences | |
| 0 | Not mentioned or clear and important differences in care programs | |
| 2 | Clearly defined |
| 1 | Inadequately defined | |
| 0 | Not defined | |
| 2 | Clearly defined |
| 1 | Inadequately defined | |
| 0 | Not defined | |
| 2 | Clearly defined interventions are applied with a standardized protocol |
| 1 | Clearly defined interventions are applied but the application protocol is not standardized | |
| 0 | Intervention and/or application protocol are poorly or not defined | |
| 2 | Clearly defined |
| 1 | Inadequately defined | |
| 0 | Not defined | |
| 2 | Appropriately measured |
| 1 | Inadequately measured | |
| 0 | Not defined | |
| 2 | Optimal |
| 1 | Adequate | |
| 0 | Not defined, not adequate | |
| 2 | Active surveillance and appropriate duration |
| 1 | Active surveillance, but inadequate duration | |
| 0 | Surveillance not active or not defined | |
| 2 | Yes |
| 1 | Point estimates, but no measures of variability presented | |
| 0 | Vague descriptions | |
| 2 | Compliance well described and accounted for in analysis |
| 1 | Compliance well described but differences between groups not accounted for in analysis | |
| 0 | Compliance unclear | |
| 2 | Well described |
| 1 | Poorly described | |
| 0 | Not described | |
| 2 | Yes |
| 1 | Partly | |
| 0 | No |
| Category | ||
|---|---|---|
| Design | Type of study design | RCT, Controlled Trial, uncontrolled Trial, cohort; cross-section |
| Method of group allocation | Random number table; computer random number generator; coin toss | |
| Blinding of group allocation | Therapist and/or patient; sealed envelopes | |
| Duration of follow-up period | ||
| Power sample size calculation | sample size needed for adequate statistical power | |
| Subject selection | Setting | |
| Country | ||
| Year of study | ||
| Inclusion and exclusion criteria | ||
| Planned interventions | Description of experimental intervention | Type of martial arts; description of content of training sessions |
| Description of reference intervention | ||
| Time per intervention session | ||
| Frequency intervention sessions | ||
| Duration of intervention period | ||
| Total number of interventions | ||
| Cumulative training time in study | ||
| Outcome definition | All collected outcomes variables | Units of measurement, upper and lower limits of ordinal scales |
| Measurements | ||
| Time points of collected data | ||
| Adverse effects | ||
| Subjects per group | Number of subjects | |
| Ethnicity | Proportions | |
| Age | Mean and SD; median; range | |
| Gender | Proportions | |
| Socio-demographic characteristics | ||
| Co-morbidity | ||
| Reported results per group | Outcome measures | Proportions; means and SD; medians; ranges |
| Intention to treat analysis | ||
| Cumulative training time | ||
| Loss to follow-up | ||
| Summary of all outcome measurements | ||
| Adverse events | ||
| Data analysis | Type of analysis | Intention to treat; per protocol analysis |
| Estimates of effect measures | RR, (OR), AR, NNT, difference of means; CI’s and/or p-values | |
| Subgroup analysis | Differences of effect measures between subgroups | |
| Drop outs | Drop out, lost to follow-up, missing data, crossover | |
| Limitations | Internal validity | Research question free from bias, methodology |
| Confounding | Differences in baseline characteristics | |
| Concerns about external validity | Appropriate research question, generalizability/applicability of findings | |
| Main conclusions according to authors | ||
| Miscellaneous | Source of funding | |
| Year of publication | ||
| Miscellaneous comments from authors |
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pons van Dijk, G.; Leffers, P.; Lodder, J. The Effectiveness of Hard Martial Arts in People over Forty: An Attempted Systematic Review. Societies 2014, 4, 161-179. https://doi.org/10.3390/soc4020161
Pons van Dijk G, Leffers P, Lodder J. The Effectiveness of Hard Martial Arts in People over Forty: An Attempted Systematic Review. Societies. 2014; 4(2):161-179. https://doi.org/10.3390/soc4020161
Chicago/Turabian StylePons van Dijk, Gaby, Pieter Leffers, and Jan Lodder. 2014. "The Effectiveness of Hard Martial Arts in People over Forty: An Attempted Systematic Review" Societies 4, no. 2: 161-179. https://doi.org/10.3390/soc4020161