1. Introduction
The subject of this paper is a digital device for use in those times and places where health professionals and Aboriginal patients and their families are struggling to go on together in generating plans and collective proceedings to achieve healthier Aboriginal individuals, families, and communities. The device is an iPad or generic custom-designed touch screen application that shows interactive biomedical images, animations and models. We propose that this application will differ from other similar applications in that it will not embed any explicit health messages (it is not didactic); it will not privilege the biomedical model of the human body and its functioning; it will not contain any microscopic scale imagery, and will contain few sequential arrays of images. The device will depend entirely upon users in conversation for its navigational logic and focus first on aspects of the healthy body, only later introducing pathology in leading up to images of the experience of chronic disease and its treatment. The design of the device is inspired by Yolŋu principles of communication that we have gradually learned through our participation in other health related projects. In this paper we first elaborate what we understand those principles of communication to be in telling stories of the contexts in which we learned them. Then in our final section we explain how these principles are expressed in the design of the Touch Pad Body. However, we need to be clear in beginning, that this device has reached the concept protoype stage only. At this point we have been unable to secure funding to actually build the device.
2. Knowledge and Agreement Making in Arnhem Land
The Yolŋu Aboriginal people of northeast Arnhem Land, Australia have a long tradition of theorizing about knowledge production, conflict resolution and agreement making [
1,
2,
3]. When bilingual education was introduced to three major Yolŋu schools in the early 1970s, a long process of mobilizing ancestral theory to inform curriculum and pedagogy began. As a young teacher in 1973 Michael was already a keen language learner when invited to become a teacher linguist, and to work with Yolŋu knowledge authorities on research and literature production. Helen became involved in 1987 when she found herself working with the Yirrkala School community as under a program of “Aboriginalisation” of the school supported by both the Yolngu elders and the Department of Education. In particular, as a university lecturer in mathematics education she was involved in “both ways” or “Garma Maths” curriculum development. Over the succeeding 40 years, we have been involved in collaborative research and consultancy work which has extended the reach of Yolŋu practices into much other work—including law, housing [
4], financial literacy [
5], water management [
6], community gardening [
7], and digital knowledge work [
8]. The particularly difficult process of devising a digital “interrupting tool” to embed these agreement making practices into the world of remote Aboriginal health is the subject of this paper.
The curriculum instituted by Yolŋu community elders at the Yirrkala Community School was given the name of
garma. In Yolŋu languages,
garma refers to an open public ceremonial space where people from different tribal and totemic lineages come together to produce a collaborative performance and celebration of history, and a collective agreement on ways forward, here and now. The
garma “describes the format where a Yolŋu learning environment begins” [
9]. The
garma (like Aboriginal education and transdisciplinary research) actually depends on identifying, respecting and maintaining differences, working collaboratively, coming to agreement, and building agreed ways of knowing and going ahead together [
10,
11].
All garma performances start off with an issue, be it a funeral or an initiation or maybe the return of a sacred object to its maker’s descendants. They all entail a common purpose, and a claim of authority. While each group has a large repertoire of songs, dances, gestures, paintings and paraphernalia which can be presented alongside others who share parts of ancestral histories, journeys and totems, they collaborate to choose carefully which songs (dances, names, gestures, paintings, totemic objects) will be shared in this particular located garma, and how, while playing out with other clans their collective history, they will also enact their own distinctive perspective with their own authority in the work around this particular issue, here and now. Having the right people in the right space together under the right authority is always critical to the work of making agreement. Any individual, no matter how specialist, how expert, cannot decide the best way forward alone. This robust Yolŋu epistemology keeps resurfacing in our work. Here, we tell of three distinct research projects from which the conception of the touch pad digital device draws inspiration.
3. Sharing the True Stories
By the 1990s, many Yolŋu who had been curriculum activists in Yolŋu schools were becoming active in other research fields. This work involved a woman who was in her own right a Yolŋu knowledge authority, an experienced Yolŋu educator and linguist, who had had to move from her remote island home to the city of Darwin for dialysis. She became involved in advocacy for better communication between medical practitioners and their renal patients. As a linguist I (the first author) was invited to help with a research project aimed at identifying and rectifying common causes of miscommunication [
12]. Yolŋu medical patients, especially those with serious chronic diseases, were often suspicious that they weren’t being told the true story about their illness. They were also convinced that their own stories were not being taken seriously by the medical staff. While she was only one of a large group of mostly white Australian researchers, this senior Yolŋu woman convinced us pretty early to call the whole project “Sharing the True Stories” (STTS). She flatly repudiated the simplistic conduit metaphor [
13] which sustained the illusion (so common in western understandings of communication) that messages are somehow passed from one person to another as if along a conduit.
We were required to rethink communication as the building of shared understandings, and as the research project developed we were often amused and bemused at how often the non-Aboriginal researchers and workers on the renal floor reverted to the conduit metaphor when describing their work and their frustrations to us. Through her own quiet contributions to the project, this authoritative woman, speaking out of her experiences as a Yolŋu patient, showed us the key role of narratives and of conversations which we were later to take with us into the work of designing digital resources. One key outcome of the project deriving from the Yolŋu theory of communication was increased attention to all the work which is done outside of the clinical encounter, leading us to move away from the clinical encounter as the key locus of information sharing and agreement making. The burden of communication in the clinical encounter—even with an interpreter, is intolerable. While we worked to improve the work of engagement of interpreters, we also concentrated on other things not immediately obvious as relevant to communication.
For example, a major outcome implemented in Stage 2 of the STTS project involved group meetings around clinical encounters. Honest good-faith agreement upon often quite unusual, specific ways forward for a particular patient involved something of a garma: a meeting together of as many different experts as possible, nephrologists, dietitians, renal nurses, general practitioners, social workers, as well as husbands, mothers, children friends, other patients from the same language group. Moreover, as our senior Yolŋu colleague pointed out, the configurations of people and spaces, charts and instruments also contribute to the garma, as does, of course, the patient, the real expert on the body in question.
Almost unbeknownst to us, the Yolŋu researchers were leading us to understand and undertake health communication in different ways, and these different ways needed to be taken seriously and understood and acted upon collectively, if we were to make a lasting difference to patient and community outcomes. (How those productive advances instituted in the renal unit were ultimately slowly worn down by bureaucratic demands must be the subject of another paper.) We were not at the stage of concentrating on developing a more general theory of health literacy, but are focusing on particular sites where health literacy comes into play (see below). However, our first step had been to engage an Yolŋu epistemology.
4. Healthy Breathing and Heart
Our digital device emerged also from outside the careful Yolŋu analysis of agreement making. We were invited some years later by a senior thoracic surgeon from a large southern teaching hospital, to help him review a suite of disparate digital resources which had been produced to inform people about ‘healthy breathing and hearts’. He had hundreds of images and animations which he showed to a sometimes bored, sometimes startled, sometimes fascinated and animated, often irritated group of senior bilingual Yolŋu consultants over several days. His aim was to produce the perfect health literacy tool to inform Aboriginal patients whose first language is not English, and who may not be comfortable talking about intimate bodily things in an unfamiliar tongue, about lungs, hearts, circulation and of course, smoking [
14]. There were a few problems. From the beginning there were many images, particularly those which showed microscopic details which were simply incomprehensible. I could see that the taken for granted conventions for representing movement, scale, and three dimensionality, for example, in our western graphic traditions were often not coming across at all. It never occurred to the Yolŋu consultants, always looking for a chance to build shared understandings in good faith, to say they had no idea what they were looking at. Like patients in the Sharing the True Stories research, when they didn’t understand something they smiled and nodded agreeably in the face of authority, waiting for something to make sense. What did make sense to them was the top-down disciplinary nature of much of what they were asked to review. It seemed to be blaming them and others for making bad life decisions without ever giving them a chance to contribute their own opinions. It was hard for them to have a reasonable conversation with the thoracic surgeon, despite him being gentle, generous and deeply concerned about Indigenous health. He was completely disconcerted that the photos of diseased organs were offensive, and to hear how wrong it is to say to a patient that there is a chance that the lump they have presented could be a cancer. That is an offensive way to talk. The doctor should say “If you are worried about that lump, we can do some tests and find out what’s going on there”. How conversations produce symptoms was quite lost on the doctor who didn’t understand the ways in which collective Aboriginal performances produce new possible worlds. We must therefore be careful how we perform in a collective agreement making episode.
The outcome of the consultancy was, alas, further production of another top down disciplinary digital resource, but that is another story. The conversations we had around how to talk to the owner of an Aboriginal body led us still further towards a culturally sensitive technology.
5. Redefining Health Literacy
In the third research project we were asked with our Yolŋu colleagues, to evaluate needs for health literacy, health communication and interpreters in east Arnhem Land. In the East Arnhem Region Aboriginal Client Health Education (EARACHE) project, we interviewed over 50 community members from five different communities in their own languages, and held extensive discussion with another 50 health professionals [
15]. We found many different roles and job titles—infant health workers, general practitioners, Aboriginal health workers, mental health workers, community health workers, ear health,
etc.) and a vast array of health communication resources—digital and on paper—were mostly unused. This was seen against the background of several distinct languages and several distinct cultures,
i.e., Aboriginal community life, the culture of small clinic health service delivery, and plural government bureaucracies. The people we interviewed were tired of researchers coming to troubleshoot the system, tired of the overwhelming and increasingly differentiated health work force, and tired of the top-down disciplinary health literacy messages. However, we also heard so many stories of unusual, highly productive collaborations across boundaries of professional responsibility and across the boundaries of culture which were invisible from above, unsupported, but carried out through long conversations with commitment and good faith and good results.
Good health literacy, we concluded, especially in this remote Aboriginal context of extended family and community living, is better understood not so much as what the individual client knows about biomedicine, but rather the productive working together of the people and resources which generate shared understandings and agreement. It involves good access to clear information, and honest respectful discussion and agreement making across the divide between providers and consumers. Health literacy is not so much a knowledge problem as a structural problem so there are structural solutions. We began to talk of “systemic health literacy”. Present attempts to improve Aboriginal health communication practices and “health literacy” tend to utilize a top-down policy approach which seem to blame the client for irresponsible life choices and ways, and/or front line workers for poor delivery. Yet health professionals, clients and families were often using their discretion to create good open collaborative ways of working together. How could we support this work?
We came to understand “policy” as the cumulative effect of the individual decisions made by front line workers producing slow but effective and evidence-based bottom-up changes to practice [
16]. We found Aboriginal and non-Aboriginal people discerning what is working on the ground, supporting it, having conversations around difficult decisions about chronic diseases, and making informed decisions together. We also found that resources that contain health messages seldom stimulated these productive conversations which promote new productive collaborations across the boundaries between health professionals, service users and their families. On the contrary, they actually tended to entrench definitions, roles and attitudes rather than modify them.
So in the EARACHE project we sought to develop strategies consistent with the knowledge and agreement practices we had developed with our Yolŋu co-researchers in STTS. Aboriginal clients have strong ideas and practices of embodiment and well being which might be quite different from those in other constructions, say of policy makers or health professionals or interpreters. Received views of agency in the rhetoric around health literacy infect our ability to offer alternative strategies for improved practices. We attend to the agency of these health communication resources.
6. The Touch Pad Interrupting Tool
A collective approach to dealing with the problems of the moment allows us to remain respectful of both government and Aboriginal community members and the participants in their worlds—even though they may be quite different. A collective approach allows us to avoid assuming the salience of the biomedical model, as well as the individualism of western ethics and political philosophies. There are many good health literacy resources out there, and we will encourage their use, but we propose a different sort of object which we have designed in the process of the HBH research project.
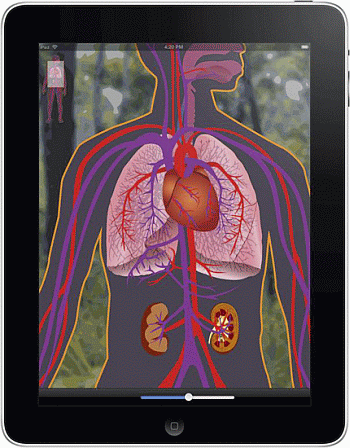
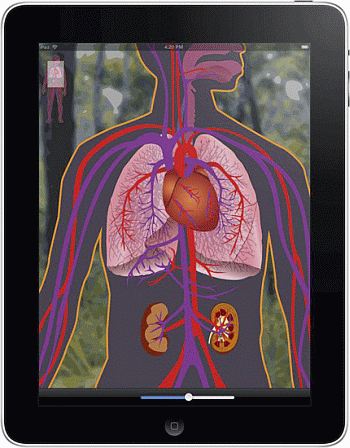
We propose a radically different resource, a user-friendly touch-pad animation of a diagrammed human body which has no message, no sequence. It is manipulable, zoomable, transparent, three dimensional, detailed in particular areas (heart, lungs, kidneys, liver, pancreas, ears). Such bodily structures are familiar to patients and their families and to health professionals, albeit in different ways. The diagramming of the Touch-pad Body de-emphasises biomedical details and assumptions. It stimulates conversation—in any language or mixture of languages. The conversations which the interactive diagram generates will not be unlike the conversations through which it is iteratively developed. Designed collaboratively, its development and its use will be coterminous. Which parts it shows and which it conceals, its genders and its pathologies will all be designed and developed collaboratively so it emerges as a body which is both Aboriginal and biomedical emergent in exchange in particular times and places.
So how does this device embody the principles of communication we have learned from our Yolŋu colleagues in a number of projects across several years? The device promotes a sharing of the burden, and a continuation of the so called “phatic” elements of communication. This is the work done by such utterances as “Hello. How are you?” It is the work of promoting sociability in which mutually engaging communication can occur. The device in part provides a form of diagrammatic infrastructure to enables that phatic work to continue and importantly to be done on all sides, so that it is not only Aboriginal patients who find themselves doing all the work. However, more substantively, when it comes to human bodies the device works at a level “below” the ontological, and the emergent diagram it provides is not a representation of a determining structure.
As itself an emerging body in the here and now of the clinical encounter—albeit of a very different corporeality than a flesh and blood human body, the diagram will interrupt the presumptions of all contributing parties presuming “neither biomedical certainties, nor Aboriginal certainties about bodies” [
17]. By using the device as a diagram to pilot a conversation around the individual problem of the moment, accepting the constraints of that particular here and now, and not obliged to import and to promote “theories about bodies” formulated in other times and places which may or may not be salient to the issues at hand, the device evades a priori assumptions at work in the working stories of all these different participants (the biomedics, the Aboriginal patients, the social workers, family members,
etc.), which entrench received assumptions, and prevent us from thinking and acting together in new ways.
The Touch-pad body will likely split into various versions, with the possibilities of adding family members and environments, as they suffer when individuals suffer and take part in treatment and healing. Some version may find its way into schools, or to the training of health workers and interpreters [
18]. However, by its very ambiguity, its capacity to absorb contradictions and tread the tight-rope of equivocation it will always open up the opportunity to interrupt the assumptions of strangeness or certitude at work between the Aboriginal and the biomedical.
In the EARACHE project it was clearly impossible for us to recommend any top down structural changes to health literacy projects which would guarantee a direct improvement on the health literacy of 7000 people. However, we did recommend the support of flexible collective ground-level discretion and decision making wherever there is openness and interest to start the conversation going, and to join up existing individuals and services. Our touch-pad body can actively stimulate this work, particularly by making itself an essential, well known public resource, (through making its images available more widely through posters, websites, leaflets, etc.) and by its very ubiquity it could institutionalize collective agreement making over medical issues, marginalize the autocratic practitioners including some of the fly-in fly-out specialists, and cry out for a garma-style setting which activates complex intercultural conversation to generate a unique complex way forward for this medical issue here and now. Moerover, those using it would be part of the collective iterative design, development, implementation and evaluation project. Our device interrupts received notions and entrenched practices by getting as many authoritative people talking about each medical decision in their own way, but together. Our yet unfunded, undeveloped digital device will help this bottom-up change in mutual understanding, agreement making and informed consent to reverberate upwards towards changing policies and practices at higher levels. We look forward to working with this device, when funds are made available to bring it fully to life. There are issues associated with its interventions that can only be dealt with ‘face-to-face’ with the device, so to speak. How can we contrive the routines and the techniques by which agreement over how to build agreement in ways that explicitly involve humans and non-humans actively contributing? In particular where and how might the important principle of informed consent be given its due?
In all this piecemeal work, our digital garma device will promote a new coherence and reflexivity in the ways in which service users and providers approach their work with Aboriginal patients and their families. Real change comes when categories are unsettled, where we have conversations which allow us all to rethink our assumptions and our collective possibilities. Finding new ways of understanding and enhancing health literacy requires using the language and tools available for developing a generative health literacy policy and practice, first of all at the local level. Both Aboriginal people and governments could be “end users” of research, providing an evidence base, which should not be different from making policy change.
7. Conclusions
Yolngu Aboriginal principles of communication have been conveyed in telling stories out of our experiences of participating in health related research projects under the tutelage of senior Aboriginal people, often themselves clients of health delivery services. Acting on this gradually developed understanding of Yolngu experience and expectations of how the clinical experience should proceed, we have worked with designers to develop an electronic communication device that interrupts the normal clinical encounter. The device elicits phatic contributions from both clinical personnel and Aboriginal clients; exchanges that attend to the important work of maintaining the sociability of the encounter. In addition it deflects the precise clinical observations and prescriptions of health professionals away from what is experienced as unwarranted and unacceptable imagined intrusions into actual patient bodies, to instead become expressions of concern for the Touchpad body generated in the encounter, as an intimate, interactive ‘stand-in’ for the patient’s body. This enables, as a subsequent distinct step, informed delicate negotiations over agreement to responsibly accept medical interventions. This device currently exists as a concept prototype as we are yet to secure funds to take the device to a further stage.

{kind=link}
{kind=link}