“Self-Employed” in Caregivinghood: The Contribution of Swedish Informal Caregivers’ Environmental and Contextual Resistance Resources and Deficits

Abstract
:
1. Introduction
1.1. Background
1.2. The Aim of the Study
1.3. The Theoretical Framework
1.4. Caregiving by Informal Caregivers
1.5. The Current State of Research on Caregiving
1.6. Salutogenesis and Caregiving Research
1.7. Salutogenesis among Caregivers to Adult Swedes—Quantitative Designs
1.8. Salutogenesis among Caregivers to Adults—Qualitative or Mixed Designs
2. Materials and Methods
2.1. Participants and Recruitment Process
2.2. Data Collection
2.3. Interview
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. Generalized Resistance Resources, GRRs
Being in Empowering Surroundings
3.2. Caregiving in Enabling Surroundings
It [moving] was an ordeal … but the older ladies living here are really nice to talk to … we’ve got barbeques, play card-games … just outside in our garden it’s really social … I really talk a lot more here than back home! … [A]partments are disability adapted... can pop down to do my shopping, no problem! … [T]hey have got these carts on wheels … just bring it up in the elevator! (CG, 19)
3.3. Caregiving in Relative Ease
3.4. Having Access to Appropriate Support
They [home helpers] think I’m very good … [to] take care of him the way I do. [It] facilitates their work when they have a lot to do in the mornings … [They] don’t have to care for him, only put on his clothing, everything is laid out for them … [They] take him up and put him in his chair … [I] receive a lot of praise [laughs]. (CG 19)
The support I get is good; they’ve told me that if I need more, I’ll just call, so I know that I can if I need more help. [Interviewer: Does that sense of security help you manage?] Yes, it’s comforting to have home nursing. I can talk to her [homecare nurse] if something’s bothering me. (CG 18)
3.5. Generalized Resistance Deficits, GRDs
Struggling in Impeding Surroundings
3.6. Caregiving in Hampering Surroundings
It’s an ordeal … I have to order transport … to carry her down the stairs since here’s no lift … to go through that to get a breath of air … or to visit … It’s sort of not worth it because you have to book when you need assistance in again and sometimes she needs to go earlier, loo or something, and I have to reschedule and they can’t get there in time … you really should be able to go when you need to! (CG 16)
3.7. Being Presupposed to Act and Behave in a Way Expected by Others
She behaved strangely … thought she’d had a small stroke … but they didn’t listen to me at the hospital … had their minds set it was a urinary infection … sent her home by lunchtime … we sent her back at five and finally they listened to me. (CG 30)
When [my husband] goes to the doctor, he’s told him that he’s not to tell me about his conditions. When I ask [the doctor], he just refers to [husband’s] integrity and doesn’t tell me. REALLY! I think doctors should be obligated to tell the one who’s providing care! Especially since [my husband] SAYS he doesn’t remember what the doctor said. (CG 3)
I should have some medication … called down and they said, “just pop down and collect them” and down I went and there was NO medication. Then it happened again. I ordered and they said I could pick them up. NOTHING. They weren’t there! [They] hadn’t even ordered it! I find this utterly disrespectful. (CG 31)
It doesn’t make a heck of a difference where you are, you always hear the same “well we’re always wondering how long you’ll manage”. [I’ll be] damned if that’s any of their business! Not one damned bit!” (CG 30)
3.8. Lacking Access to Appropriate Support
[Interviewer: Are you allowed to accompany your husband?] Are you completely mad!! In that case he would have had to be so sick that he couldn’t sit in a car from point A to B!!! It’s completely hysterical! If he’s to take this service to town I’m supposed to take a bus or a car to meet him down there for such as shopping because he can’t move around in the shops by himself, can he? If I’m to do this, we may as well take the car! And these regulations, they only grant him six months and then he’s got to get a doctor’s certificate again. How can people who decide this be so ignorant concerning different functional limitations that they don’t understand that a person who is 77 years old and have had several strokes will not be healed in six months! It’s outrageous! (CG 4)
Finally, he got rehabilitation in [another municipality]; it took him one hour to get there and then physiotherapy one hour and one hour home but … the Taxi sort of went around to several community centres to drop people off so he got motion sickness and it took him hours to get home and when he did he was exhausted … now I drive him. (CG 4)
4. Discussion
SRRs/GRRs and SRDs/GRDs Described by Swedish Informal Caregivers
5. Methodological Considerations
6. Implications for Research and Practice
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European Commission. Long-Term Care for the Elderly. Provisions and Providers in 33 European Countries; European Commission: Luxembourg, 2012. [Google Scholar]
- Mackenzie, A.; Greenwood, N. Positive experiences of caregiving in stroke: A systematic review. Disabil. Rehabil. 2012, 34, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Lindström, B.; Eriksson, M. The salutogenic approach to the making of HiAP/Healthy Public Policy: Illustrated by a case study. Glob. Health Promot. 2009, 16, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Zarit, S.H.; Reamy, A.M. Future directions in family and professionala caregiving for elderly. Gerontology 2013, 59, 152–158. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Ottawa Charter for Health Promotion: An International Conference on Health Promotion, the Move Towards a New Public Health, November 17–21 1986; World Health Organization: Geneva, Switzerland, 1986. [Google Scholar]
- United Nations. Implementation of the International Plan of Action on Ageing and related activities. In ANNEX The United Nations Principles for Older Persons. To Add Life to the Years That Have Been Added to Life; A/res/46/91, 74th Plenary Meeting; United Nations: New York, NY, USA, 1991. [Google Scholar]
- European Commission. European Charter of Rights and Responsibilities of Older People in Need of Long-Term Care and Assistance; EUSTaCEA Project, under Daphne III Programme; Accompanying Guide; European Commission: Luxembourg, 2010. [Google Scholar]
- World Health Organization (WHO). Active Ageing: A Policy Framework; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- World Health Organization (WHO). Resolution Strengthening Active and Healthy Aging; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Koelen, M.; Eriksson, M.; Cattan, M. Older People, Sense of Coherence and Community. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: New York, NY, USA, 2016; pp. 137–149. [Google Scholar]
- Centers for Disease Control and Prevention. Healthy Places Terminology. Retrieved 27 February 2017. Available online: https://www.cdc.gov/healthyplaces/terminology.htm (accesed on 27 February 2017).
- Council of Europe. Resolution ResAP (2001) 1 on the Introduction of the Principles of Universal Design into Curricula of All Occupations Working on the Built Environment; Council of Europe: Strasbourg, France, 2001. [Google Scholar]
- Eriksson, M.; Lindström, B. A salutogenic interpretation of the Ottawa Charter. Health Promot. Int. 2008, 23, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Antonovsky, A. Health, Stress and Coping; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- Antonovsky, A.; Sourani, T. Family sense of coherence and family adaptation. J. Marriage Fam. 1988, 50, 79–92. [Google Scholar] [CrossRef]
- Antonovsky, A. Complexity, conflict, chaos, coherence, coercion and civility. Soc. Sci. Med. 1993, 37, 969–981. [Google Scholar] [CrossRef]
- Janssen, B.M.; Van Regenmortel, T.; Abma, T.A. Balancing Risk Prevention and Health Promotion: Towards a Harmonizing Approach in Care for Older People in the Community. Health Care Anal. 2014, 22, 82–102. [Google Scholar] [CrossRef] [PubMed]
- Mittelmark, M.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. (Eds.) The Handbook of Salutogenesis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Eriksson, M.; Lindström, B. Antonovsky’s Sense of Coherence Scale and the relation with health: A systematic review. J. Epidemiol. Commun. Health 2006, 60, 376–381. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.L. Self-identifying as a caregiver: Exploring the positioning process. J. Aging Stud. 2007, 21, 165–174. [Google Scholar] [CrossRef]
- Goodman, C. Research on the informal carer: A selected literature review. J. Adv. Nurs. 1986, 11, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Kinney, I.M.; Stephens, M.A.P. Hassels and uplifts of giving care to a family member with dementia. Psychol. Aging 1989, 4, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef]
- Stephens, M.A.P.; Kinney, J.M.; Norris, V.K.; Ritchie, S.W.; Grotz, R.C. Stressful situations in caregiving: Relations between caregiver coping and well-being. Pscyhol. Aging 1988, 3, 208–209. [Google Scholar] [CrossRef]
- Acton, G.J.; Kang, J. Interventions to reduce the burden of caregiving for an adult with dementia: A meta-analysis. Res. Nurs. Health 2001, 24, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Green, A.; Koschera, A. Meta-analysis of psychosocial interventions for caregivers of people with dementia. J. Am. Geriatr. Soc. 2003, 51, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Cooke, D.D.; McNally, L.; Mulligan, T.; Harrison, J.G.; Newman, S.P. Psychosocial interventions for caregivers of people with dementia: A systematic review. Aging Ment. Health 2001, 5, 120–135. [Google Scholar] [CrossRef] [PubMed]
- Deeken, J.F.; Taylor, K.L.; Mangan, P.; Yabroff, K.R.; Ingham, J.M. Care of the caregivers: A review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J. Pain Symptom Manag. 2003, 26, 922–953. [Google Scholar] [CrossRef]
- Cohen, C.A.; Colantonio, A.; Vernich, L. Positive aspects of caregiving: Rounding out the caregiver experience. Int. J. Geriatr. Psychiatry 2002, 17, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.K. Concepts in caregiver research. J. Nurs. Scholarsh. 2003, 35, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Kramer, B.J. Gain in the caregiving experience: Where are we? What next? Gerontologist 1997, 37, 218–232. [Google Scholar] [CrossRef]
- Louderback, P. What’s happening. Elder Care: A positive approacah to caregiving. J. Am. Acad. Nurse Pract. 2000, 12, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Moss, M.; Kleban, M.H.; Glicksman, A.; Rovine, M. A two-factor model of caregiving appraisal and psychological well-being. J. Gerontol. 1991, 46, 181–189. [Google Scholar] [CrossRef]
- Yamamoto-Mitani, N.; Ishigaki, K.; Kuniyoshi, M.; Kawahara-Maekawa, M.; Hayashi, K.; Hasegawa, K.; Sugishita, C. Subjective quality of life and positive appraisal of care among Japanese caregivers of older adults. Qual. Life Res. 2004, 13, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Kinney, J.; Stephens, M.; Franks, M.; Norris, V. Stresses and satisfactions of family caregivers to older stroke patients. J. Appl. Gerontol. 1995, 14, 3–21. [Google Scholar] [CrossRef]
- Nijboer, C.; Tempelaar, B.; Tiemestra, M.; Sanderman, R.; Van den Bos, C. Measuring both negative and positive reactions to giving care to cancer patients: Psychometric qualities of the caregiver reaction assessment. Soc. Sci. Med. 1999, 48, 1259–1269. [Google Scholar] [CrossRef]
- Rapp, S.R.; Chao, D. Appraisals of strain and gain: Effects on psychological wellbeing of caregivers of dementia patients. Aging Ment. Health 2000, 4, 142–147. [Google Scholar] [CrossRef]
- Ayres, L. Narratives of family caregiving: The process of making meaning. Res. Nurs. Health 2000, 23, 424–434. [Google Scholar] [CrossRef]
- Ayres, L. Narratives of family caregiving: Four story types. Res. Nurs. Health 2000, 23, 359–371. [Google Scholar] [CrossRef]
- Farran, C.; Keane-Hagerty, E.; Salloway, S.; Kupferer, S.; Wilken, C. Finding meaning: An alternative paradigm for Alheimer’s disease family caregivers. Gerontologist 1991, 31, 483–489. [Google Scholar] [CrossRef]
- Farran, C.; Miller, B.H.; Kaufman, J.E.; Donner, E.; Fogg, L. Finding meaning through caregiving: Development of an instrument for family caregivers to persons with Alzheimer’s disease. J. Clin. Psychol. 1999, 55, 1107–1125. [Google Scholar] [CrossRef]
- Kramer, B.J. Expanding the conceptualization of caregiver coping: The importance of relationship-focused coping strategies. Gerontologist 1993, 35, 340–348. [Google Scholar] [CrossRef]
- Van Puymbroeck, M.; Rittman, M.R. Quality-of-life predictors for caregivers at 1 and 6 months poststroke: Results of path analysis. J. Rehabil. Res. Dev. 2005, 42, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Ekwall, A.K. Informal Caregiving at Old Age. Content, Coping, Difficulties and Satisfaction. Ph.D. Thesis, Lund University, Lund, Sweden, 2004. [Google Scholar]
- Milberg, A.; Strang, P. Meaningfulness in palliative home care: An interview study of dying cancer patients’ next of kin. Palliat. Support. Care 2003, 1, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Mok, E.; Chan, F.; Chan, V.; Yeung, E. Perception of empowerment by family caregivers of patients with a terminal illness in Hong Kong. Int. J. Palliat. Nurs. 2002, 8, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Waldrop, D.P.; Rinfrette, E.S. Can short hospice enrolment be long enough? Comparing the perspectives of hospice professionals and family caregivers. Palliat. Support. Care 2009, 7, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Chumbler, N.R.; Rittman, M.R.; Wu, S.S. Associations in sense of coherence and depression in caregivers of stroke survivors across 2 years. J. Behav. Health Serv. Res. 2008, 35, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Forsberg-Wärleby, G.; Möller, A.; Blomstrand, C. Spouses of first-ever stroke victims: Sense of coherence in the first phase after stroke. J. Rehabil. Med. 2002, 34, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, I.; Axelsson, K.; Gustafson, Y.; Lundman, B.; Norberg, A. Well-being, sense of coherence, and burnout in stroke victims and spouses during the first few months after stroke. Scand. J. Caring Sci. 2001, 15, 203–214. [Google Scholar] [CrossRef] [PubMed]
- O’Connel, B.; Baker, L. Managing as carers of stroke survivors: Strategies from the field. Int. J. Nurs. Pract. 2004, 11, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Gosman-Hedström, G.; Dahlin-Ivanoff, S. “Mastering an unpredictable everyday life after stroke”—Older women’s experiences of caring and living with their partners. Scand. J. Caring Sci. 2012, 26, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Luk, W.S.-C. The home care experience as perceived by caregivers of Chinese dialysis patients. Int. J. Nurs. Stud. 2002, 39, 269–277. [Google Scholar] [CrossRef]
- Saunders, M.M. Perspectives from family caregivers receiving home nursing support: Findings from a qualitative study of home care patients with heart failure. Home Healthc. Nurse 2012, 30, 82–90. [Google Scholar] [PubMed]
- Cheung, J.; Hocking, P. Caring as worrying: The experience of spousal carers. J. Adv. Nurs. 2004, 47, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Topcu, G.; Buchanan, H.; Aubeeluck, A.; Garip, G. Caregiving in multiple sclerosis and quality of life: A meta-synthesis of qualitative research. Psychol. Health 2016, 31, 693–710. [Google Scholar] [CrossRef] [PubMed]
- Rollero, C. The experience of men caring for a partner with Multiple Sclerosis. J. Nurs. Scholarsh. 2016. [Google Scholar] [CrossRef] [PubMed]
- Lethin, C.; Renom-Guiteras, A.; Zwakhalen, S.; Soto-Martin, M.; Saks, K.; Zabalegui, A.; Challis, D.J.; Nilsson, C.; Karlsson, S. Psychological well-being over time among informal caregivers caring for persons with dementia living at home. Aging Ment. Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Galvin, M.; Corr, B.; Madden, C.; Mays, I.; McQuillan, R.; Timonen, V.; Staines, A.; Hardiman, O. Caregiving in ALS—A mixed methods approach to the study of burden. BMC Palliat. Care 2016, 15, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.B.; Long, S.O. Husbands and sons in the United States and Japan: Cultural expectations and caregiving experiences. J. Aging Stud. 1999, 13, 241–267. [Google Scholar] [CrossRef]
- Yamamoto-Mitani, N.; Wallhagen, M.I. Pursuit of psychological well-being (ikigai) and the evolution of self-understanding in the context of caregiving in Japan. Cult. Med. Psychiatry 2002, 26, 399–417. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-Y. The effect of health promotion counselling to family caregivers. Public Health Nurs. 1999, 16, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Potgieter, J.C.; Heyns, P.M. Caring for a spouse with Alzheimer’s disease: Stressors and strengths. S. Afr. J. Psychol. 2006, 36, 547–563. [Google Scholar] [CrossRef]
- Pretorius, C.; Walker, S.; Heyns, M. Sense of coherence amongst male caregivers in dementia. Dementia 2009, 8, 79–94. [Google Scholar] [CrossRef]
- Prince, M.; Graham, N.; Brodaty, H.; Rimmer, E.; Varghese, M.; Chiu, H.; Acosta, D.; Scazufca, M. Alzheimer Disease International’s 10/66 Dementia Research Group—One model for action research in developing countries. Int. J. Geriatr. Psychiatry 2004, 19, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Kirsi, T.; Hervonen, A.; Jylhä, M. A man’s gotta do what a man’s gotta do: Husbands as caregivers to their demented wives: A discourse analysis approach. J. Aging Stud. 2000, 2, 153–169. [Google Scholar] [CrossRef]
- Morgan, T.; William, L.A.; Trussardi, G.; Gott, M. Gender and family caregiving at the end-of-life in the context of old age: A systematic review. Palliat. Med. 2016, 30, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Kramer, B.J. Marital history and the prior relationship as predictors of positive and negative outcomes among wife caregivers. Fam. Relat. 1993, 42, 367–375. [Google Scholar] [CrossRef]
- Riberio, O.; Constanca, P. Older male carers and the positive aspects of care. Ageing Soc. 2008, 28, 165–183. [Google Scholar] [CrossRef]
- Russel, R. In sickness and in health. A qualitative study of elderly men who care for wives with dementia. J. Aging Stud. 2001, 15, 351–367. [Google Scholar]
- Calasanti, T.; Bowen, M.E. Spousal caregiving and crossing gender boundaries: Maintaining gendered identities. J. Aging Stud. 2006, 20, 253–263. [Google Scholar] [CrossRef]
- Lewis, R.D. The impact of the marital relationship on the experience of caring for an elderly spouse with dementia. Ageing Soc. 1998, 18, 209–231. [Google Scholar] [CrossRef]
- Romoren, T.I. The carer career of son and daughter primary carers of their very old parents in Norway. Ageing Soc. 2003, 23, 471–485. [Google Scholar] [CrossRef]
- Eriksson, M. Unravelling the Mystery of Salutogenesis: The Evidence Base of the Salutogenic Research as Measured by Antonovsky’s Sense of Coherence Scale. Ph.D. Thesis, Åbo Akademi University Vasa, Turku, Finland, 2007. [Google Scholar]
- Coe, R.M.; Romeis, J.C.; Tang, B.; Wolinsky, F.D. Correlates of a measure of coping in older veterans: A preliminary report. J. Commun. Health 1990, 15, 287–296. [Google Scholar] [CrossRef]
- Sagy, S.; Antonovsky, A. Coping with retirement: Does the sense of coherence matter less in the kibbutz? Int. J. Health Sci. 1990, 1, 233–242. [Google Scholar]
- Wells, Y.D.; Kendig, H.L. Health and wellbeing of spouse caregivers and the widowed. Gerontologist 1997, 37, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Coe, R.M.; Miller, D.K.; Flaherty, J. Sense of coherence and perception of caregiving burden. Behav. Health Aging 1992, 2, 93–99. [Google Scholar]
- Andrén, S.; Elmståhl, S. Family caregivers’ subjective experiences of satisfaction in dementia care: Aspects of burden, subjective health and sense of coherence. Scand. J. Caring Sci. 2005, 19, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Andrén, S.; Elmståhl, S. The relationship between caregiver burden, caregivers’ perceived health and their sense of coherence in caring for elders with dementia. J. Clin. Nurs. 2008, 17, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Kristensson, A.E.; Rahm Hallberg, I. The association between caregiving satisfaction, difficulties and coping among older family caregivers. J. Clin. Nurs. 2007, 16, 832–844. [Google Scholar]
- Kristensson, A.E.; Sivberg, B.; Rahm Hallberg, I. Older caregivers’ coping strategies and sense of coherence in relation to quality of life. J. Adv. Nurs. 2007, 57, 584–596. [Google Scholar]
- Zhang, J.; Vitaliano, P.P.; Lutgendorf, S.K.; Scanlan, J.M.; Savage, M.V. Sense of coherence buffers relationships of chronic stress with fasting glucose levels. J. Behav. Med. 2001, 24, 33–55. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I. Tribute to Aaron Antonovsky—“What creates health”. Health Promot. Int. 1996, 11, 5–6. [Google Scholar] [CrossRef]
- Milberg, A.; Strang, P. Exploring comprehensibility and manageability in palliative home care: An interview study of dying cancer patients’ informal carers. Psycho-Oncology 2004, 13, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Milberg, A.; Strang, P. What to do when ‘there is nothing more to do’? A study within a salutogenic framework of family members’ experience of palliative home care staff. Psycho-Oncology 2007, 16, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Milberg, A. Family Members’ Experience of Palliative Home Care. Ph.D. Thesis, Linköping University, Linköping, Sweden, 2003. [Google Scholar]
- Wennerberg, M.M.T.; Lundgren, S.M.; Danielson, E. Using the salutogenic approach to unravel informal caregivers’ resources to health: Theory and methodology. Aging Ment. Health 2012, 16, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, M.M.T.; Eriksson, M.; Danielson, E.; Lundgren, S.M. Unravelling Swedish informal caregivers’ Generalised Resistance Resources. Scand. J. Caring Sci. 2016, 30, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, M.M.T.; Eriksson, M.; Lundberg, S.M.; Danielson, E. Unravelling Swedish informal caregivers’ Generalized Resistance Deficits. Scand. J. Caring Sci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Andershed, B.; Ternestedt, B.-M. Involvement of relatives in the care of the dying in different care cultures: Involvement in the dark or in the light? Cancer Nurs. 1998, 21, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Stoltz, P.; Willman, A.; Udén, G. The meaning of support as narrated by family carers for a senior relative at home. Health Res. 2006, 16, 594–610. [Google Scholar] [CrossRef] [PubMed]
- Krevers, B.; Magnusson, H.; Johansson, L.; Öberg, B. (Eds.) The National Survey Report for Sweden. In EUROFAMCARE Consortium Services for Supporting Family Carers of Older Dependent People in Europe: Characteristics, Coverage and Usage; European Union: Brussels, Belgium, 2006. [Google Scholar]
- Benzein, E.G.; Hagberg, M.; Saveman, B.-I. “Being appropriately unusal”: A challenge for nurses in health-promoting conversations with families. Nurs. Inq. 2008, 15, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Hollnagel, H.; Malterud, K. Shifting attention from objective risk factors to patients’ self-assessed health resources: A clinical model for general practice. Fam. Pract. 1995, 12, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Hollnagel, H.; Malterud, K.; Witt, K. Men’s self-assessed personal health resources: Approaching patients’ strong points in general practice. Fam. Pract. 2000, 17, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2007, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Birks, M.; Chapman, Y.; Francis, K. Memoing in qualitative research. Probing data and processes. J. Res. Nurs. 2008, 13, 68–75. [Google Scholar] [CrossRef]
- Sandelowski, M.; Barosso, J. Finding the findings in qualitative studies. J. Nurs. Scholarsh. 2002, 34, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K. Qualitative research: Standards, challenges, and guidelines. Lancet 2001, 358, 483–488. [Google Scholar] [CrossRef]
- Ayres, L.; Kavanaugh, K.; Knafl, K. Within-case and across-case approaches to qualitative data analysis. Qual. Health Res. 2003, 13, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Swedish Council for Research in the Humanities and Social Sciences. Ethical Guidelines for Research in the Humanities and Social Sciences; Codex: Stockholm, Sweden, 2002. [Google Scholar]
- Sagy, S.; Antonovsky, H. The development of the sense of coherence: A retrospective study of early life experiences in the family. J. Aging Hum. Dev. 2000, 51, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Lezwijn, J.; Vaandrager, L.; Naaldenberg, J.; Wagemakers, A.; Koelen, M.; van Woerkum, C. Healthy ageing in a salutogenic way: Building the HP 2.0 framework. Health Soc. Care Commun. 2011, 19, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Riksrevisionen. Stödet till Anhöriga Omsorgsgivare (RiR 2014:9); Summary; Support for Carers; Swedish National Audit Office: Stockholm, Sweden, 2014. [Google Scholar]
- Annerstedt, L.; Elmståhl, S.; Invad, B.; Samuelsson, S.-M. Family caregiving in dementia. An analysis of the caregiver’s burden and the “breaking-point” when home care becomes inadequate. Scand. J. Public Health 2000, 28, 23–31. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Caregiver Characteristics | Wife ( n = 17) | Husband ( n = 9) | Daughter ( n = 6) | Total ( n = 32) |
|---|---|---|---|---|
| Mean age (range) in years | 71 (60–84) | 78 (67–87) | 58 (50–69) | 71 (50–87) |
| Professional nursing experience (mean and range in years) | 9 | 1 | 4 | 14 |
| Care Recipient Characteristics | Women (n = 15) | Men (n = 17) | Total (n = 32) | |
| Mean age (range) in years | Wives 77 (67–86)
Mothers 89 (76–97) | 76 (63–86) | 77 (63–97) | |
| Physical disease and/or impairment requiring assistance None One to two Three or more | 4 7 4 | 1 9 7 | 5 16 11 | |
| Extensive difficulties with communication | 4 | 3 | 7 | |
| Psychological impairment including psychiatric morbidity, excessive anxiety and dementia | 11 | 11 | 22 | |
| Blind, deaf or extensive limitations with sight/hearing | 2 | 5 | 7 | |
| Capability to be alone Never Short periods of time A few hours Always | 1
3 6 6 | 0
3 1 1 | 1
6 7 7 | |
| Contextual Characteristics | ||||
| Place of living | ||||
| Rural area | 3 | 3 | 6 | |
| Urban area | 20 | 6 | 26 | |
| Nature | ||||
| Close by < 300 m | 23 | 2 | 3 | |
| Don’t have time to go out | 2 | 0 | 2 | |
| Doesn’t use nature due to other reasons | 32 | 2 | 3 |
| Comparison | Purpose | Strategy | Product |
|---|---|---|---|
| Within individual caregivers | Identify variation GRRs and GRDs | Close reading of individual interviews and memos | Themes (GRRs and GRDs) |
| Across multiple caregivers | Identify variation around GRRs and GRDs | Data coding and display | Sub-themes (GRRs and GRDs) |
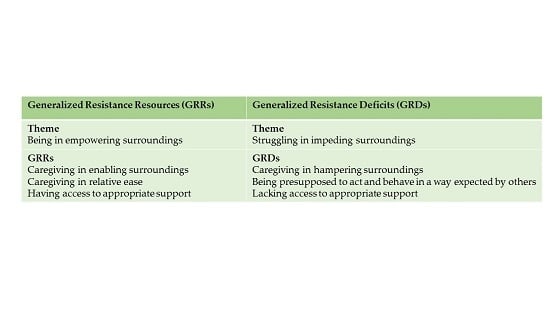
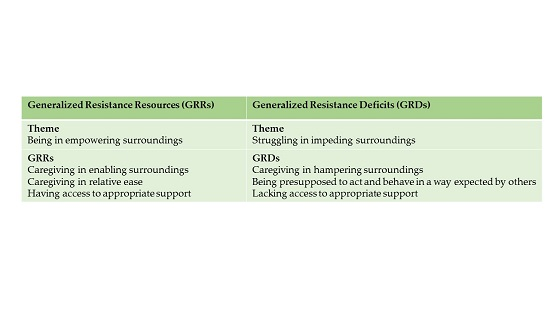
| Generalized Resistance Resources (GRRs) | Generalized Resistance Deficits (GRDs) |
|---|---|
| Theme Being in empowering surroundings | Theme Struggling in impeding surroundings |
| GRRs Caregiving in enabling surroundings Caregiving in relative ease Having access to appropriate support | GRDs Caregiving in hampering surroundings Being presupposed to act and behave in a way expected by others Lacking access to appropriate support |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eriksson, M.; Wennerberg, M.M.T.; Lundgren, S.M.; Danielson, E. “Self-Employed” in Caregivinghood: The Contribution of Swedish Informal Caregivers’ Environmental and Contextual Resistance Resources and Deficits. Societies 2017, 7, 19. https://doi.org/10.3390/soc7030019
Eriksson M, Wennerberg MMT, Lundgren SM, Danielson E. “Self-Employed” in Caregivinghood: The Contribution of Swedish Informal Caregivers’ Environmental and Contextual Resistance Resources and Deficits. Societies. 2017; 7(3):19. https://doi.org/10.3390/soc7030019
Chicago/Turabian StyleEriksson, Monica, Mia M. T. Wennerberg, Solveig M. Lundgren, and Ella Danielson. 2017. "“Self-Employed” in Caregivinghood: The Contribution of Swedish Informal Caregivers’ Environmental and Contextual Resistance Resources and Deficits" Societies 7, no. 3: 19. https://doi.org/10.3390/soc7030019