Community Knowledge about Tuberculosis and Perception about Tuberculosis-Associated Stigma in Pakistan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Sampling Approach
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Approval
3. Results
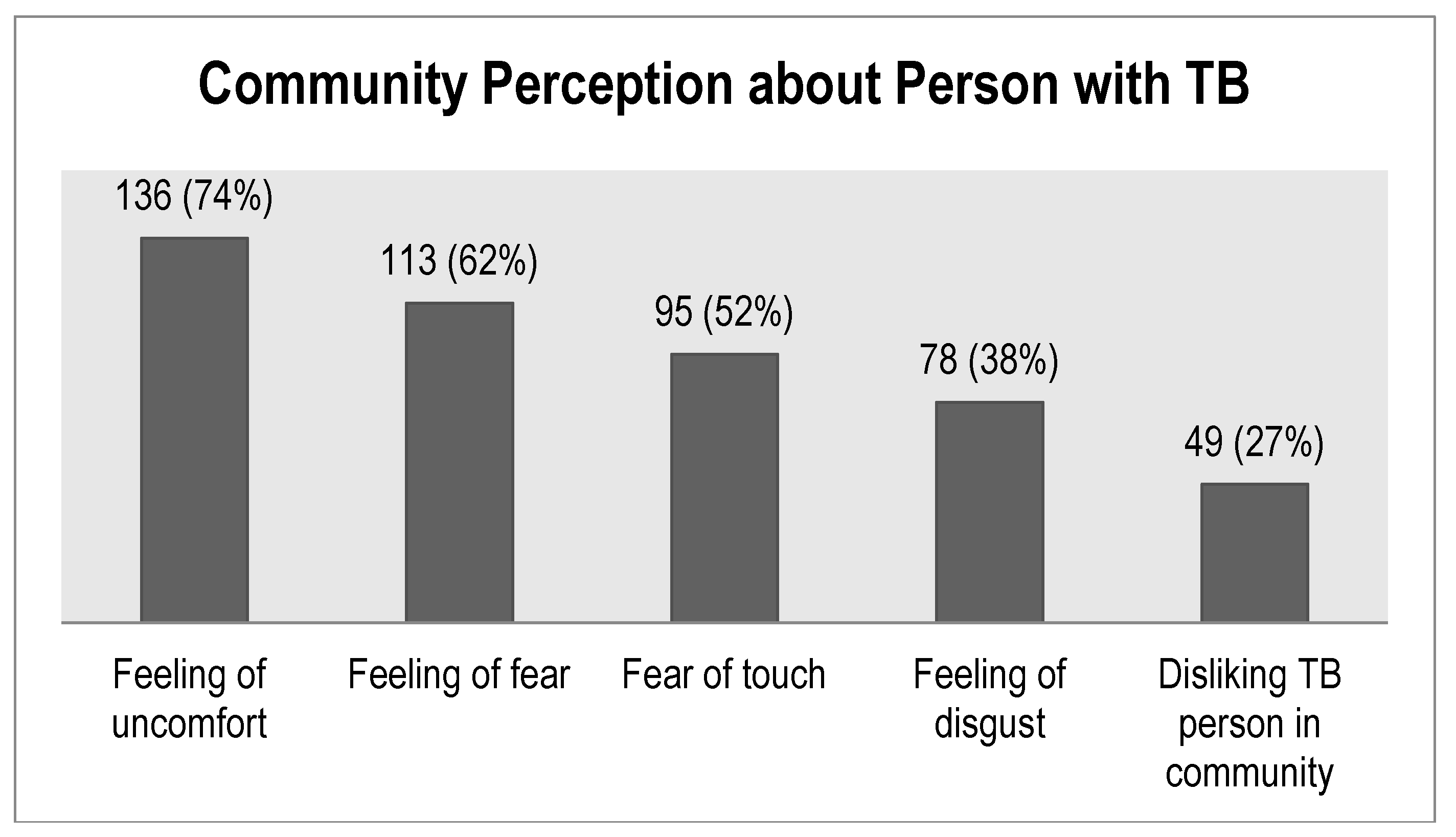
4. Community Perceptions about Tuberculosis
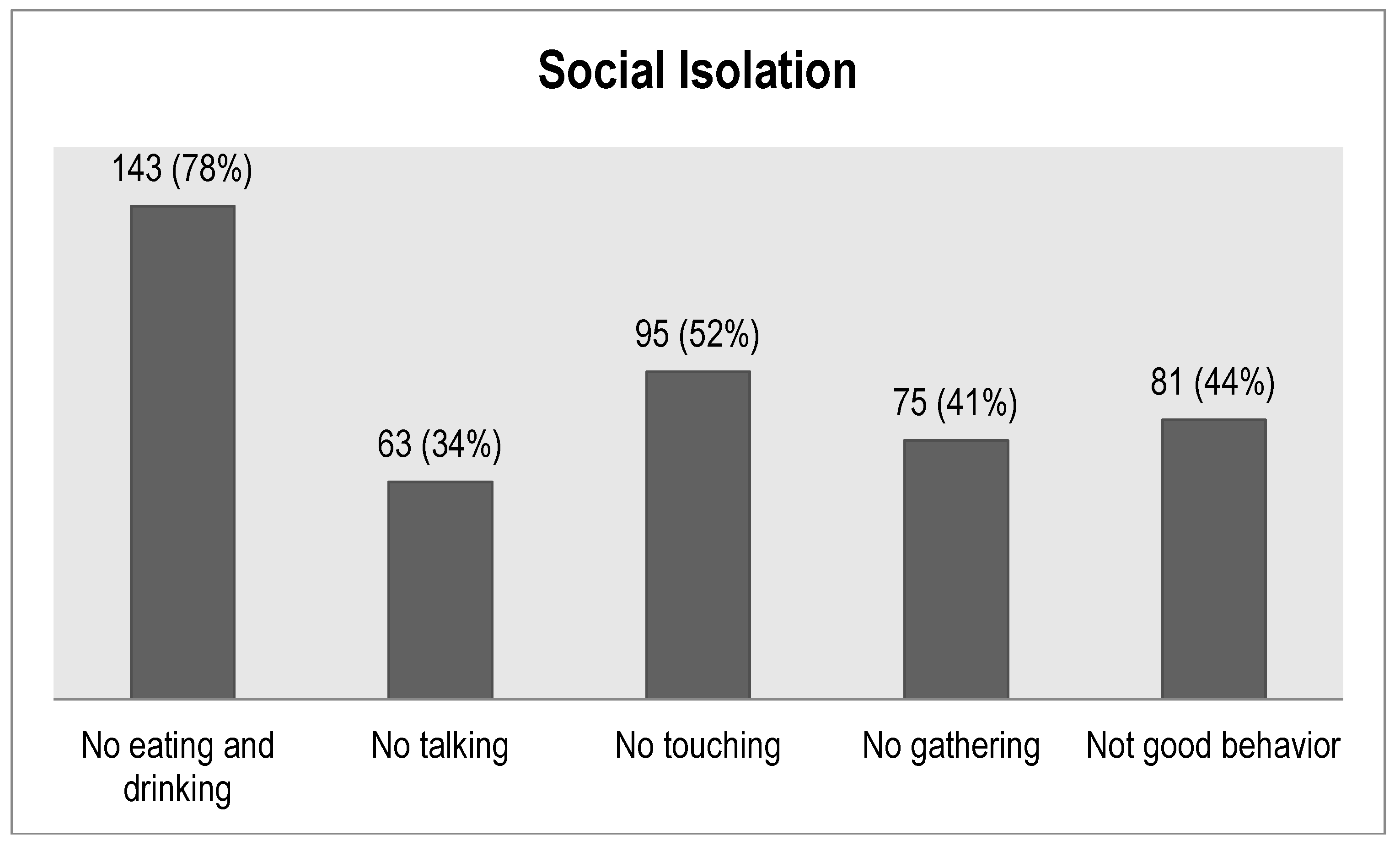
5. Social Isolation
6. Gender Perspectives Regarding Tuberculosis
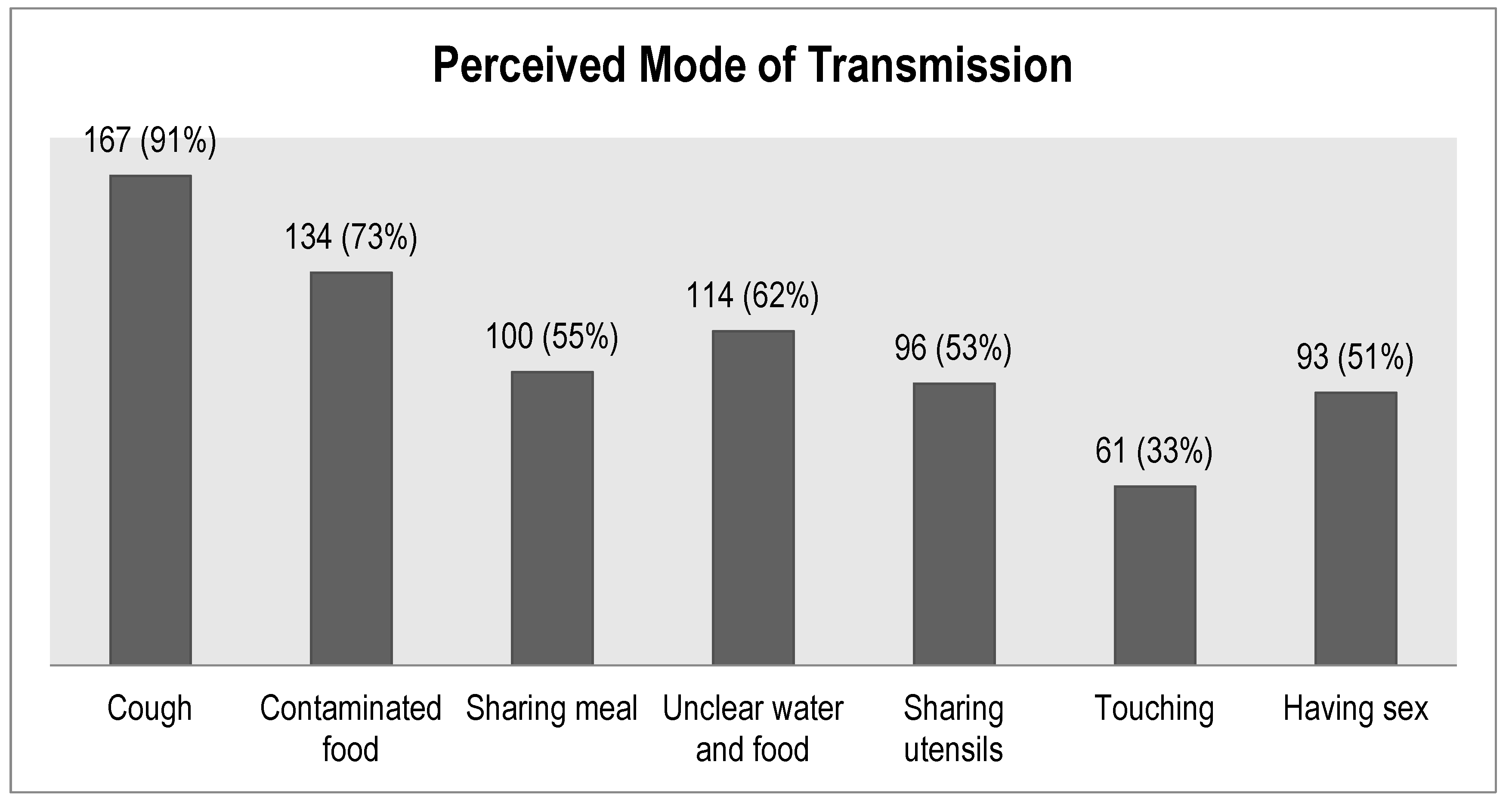
7. Knowledge about Tuberculosis
8. Factors Associated with Stigma
9. Discussion
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
Data Availability
References
- World Health Organization. Global Tuberculosis Report 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Ali, S.S.; Rabbani, F.; Siddiqui, U.N.; Zaidi, A.H.; Sophie, A.; Virani, S.J.; Younus, N.A. Tuberculosis: Do we know enough? A study of patients and their families in an outpatient hospital setting in Karachi, Pakistan. Int. J. Tuberc. Lung Dis. 2003, 7, 1052–1058. [Google Scholar] [PubMed]
- Williams, G.; Alarcon, E.; Jittimanee, S.; Walusimbi, M.; Sebak, M.; Berga, E.; Villa, T.S. Best Practice for the Care of Patients with Tuberculosis; A Guide for Low Income Countries; International Union against Tuberculosis and Lung Disease: Paris, France, 2007. [Google Scholar]
- Baral, S.C.; Karki, D.K.; Newell, J.N. Causes of stigma and discrimination associated with tuberculosis in Nepal: A qualitative study. BMC Public Health 2007, 2, 211. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Walley, J.; Newell, J.; Imdad, N. Tuberculosis in Pakistan: Socio-cultural constraints and opportunities in treatment. Soc. Sci. Med. 2000, 50, 247–254. [Google Scholar] [CrossRef]
- Hoa, N.P.; Thorson, A.E.; Long, N.H.; Diwan, V.K. Knowledge of tuberculosis and associated health-seeking behavior among rural Vietnamese adults with a cough for at least three weeks. Scand. J. Public Health 2003, 62, 59–65. [Google Scholar]
- Parker, R.; Aggleton, P. HIV and AIDS-related stigma and discrimination: A conceptual framework and implications for action. Soc. Sci. Med. 2003, 57, 13–24. [Google Scholar] [CrossRef]
- Heijnders, M.; Van Der Meij, S. The fight against stigma: An overview of stigma reduction strategies and interventions. Psychol. Health Med. 2006, 11, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon & Schuster: New York, NY, USA, 1963. [Google Scholar]
- Link, B.; Phelan, J. Conceptualizing stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Smith, R.; Rossetto, K.; Peterson, B.L. A meta-analysis of disclosure of one’s HIV-positive status, stigma and social support. AIDS Care 2008, 20, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Collins, P.Y.; Von-Unger, H.; Armbrister, A. Church ladies, good girls, and locas: Stigma and the intersection of gender, ethnicity, mental illness and sexuality in relation to HIV risk. Soc. Sci. Med. 2008, 67, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Woith, W.M.; Rappleyea, M.L. Emotional representation of tuberculosis with stigma, treatment delay, and medication adherence in Russia. J. Health Psychol. 2016, 21, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, P.G.; Wiens, C.; Smith, W.C. Delay in presentation in the context of local knowledge and attitude towards leprosy—The results of qualitative fieldwork in Paraguay. Int. J. Leprosy Other Mycobact. Dis. 2003, 71, 198–209. [Google Scholar] [CrossRef]
- Piot, P.; Coll Seck, A.M. International response to the HIV/AIDS epidemic: Planning for success. Bull. World Health Organ. 2001, 79, 1106–1112. [Google Scholar] [PubMed]
- Frost, D.M. Social stigma and its consequences for the socially stigmatized. Soc. Personal. Psychol. Compass. 2011, 5, 824–839. [Google Scholar] [CrossRef]
- Mill, J.E.; Edwards, N.; Jackson, R.C.; MacLean, L.; Chaw-Kant, J. Stigmatization as a social control mechanism for persons living with HIV and AIDS. Qual Health Res. 2010, 20, 1469–1483. [Google Scholar] [CrossRef] [PubMed]
- Courtwright, A.; Turner, A.N. Tuberculosis and stigmatization: Pathways and interventions. Public Health Rep. 2010, 125 (Suppl. 4), 34–42. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ehiri, J.; Tang, S.; Li, D.; Bian, Y.; Lin, H.; Marshall, C.; Cao, J. Factors associated with patient, and diagnostic delays in Chinese TB patients: A systematic review and meta-analysis. BMC Med. 2013, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Lu, W.; Zhou, Y.; Zhu, L.; Shen, H.; Wang, J. Adherence to anti-tuberculosis treatment among pulmonary tuberculosis patients: A qualitative and quantitative study. BMC Health Serv. Res. 2009, 9, 169. [Google Scholar] [CrossRef]
- Liefooghe, R.; Michiels, N.; Habib, S.; Moran, M.B.; De Muynck, A. Perception and social consequences of tuberculosis: A focus group study of tuberculosis patients in Sialkot, Pakistan. Soc. Sci. Med. 1995, 41, 1685–1692. [Google Scholar] [CrossRef]
- Weiss, M.G.; Ramakrishna, J. Stigma interventions and research for international health. Lancet 2006, 367, 536–538. [Google Scholar] [CrossRef]
- Van Rie, A.; Sengupta, S.; Pungrassami, P.; Balthip, Q.; Choonuan, S.; Kasetjaroen, Y.; Strauss, R.P.; Chongsuvivatwong, V. Measuring stigma associated with tuberculosis and HIV/AIDS in southern Thailand: Exploratory and confirmatory factor analyses of two new scales. Trop. Med. Int. Health 2008, 13, 21–30. [Google Scholar] [CrossRef]
- Van Brakel, W.H. Measuring health-related stigma—A literature review. Psychol. Health Med. 2006, 11, 307–334. [Google Scholar] [CrossRef] [PubMed]
- Freitas, I.M.; Popolin, M.P.; Touso, M.M.; Yamamura, M.; Rodrigues LB, B.; Neto, M.S.; Crispim, J.A.; Arcêncio, R.A. Factors associated with knowledge about tuberculosis and attitudes of relatives of patients with the disease in Ribeirão Preto, São Paulo, Brazil. Revista Brasileira de Epidemiologia 2015, 18, 326–340. [Google Scholar] [CrossRef] [PubMed]
- Tolossa, D.; Medhin, G.; Legesse, M. Community knowledge, attitude and practices towards tuberculosis in Shinile town, Somali regional state, eastern Ethiopia: A cross-sectional study. BMC Public Health 2014, 14, 804. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.A.; Irfan, M.; Zaki, A.; Beg, M.; Rizvi, N. Knowledge, attitude and misconception regarding tuberculosis in Pakistani Patients. J. Pak. Med. Assoc. 2006, 56, 211–214. [Google Scholar] [PubMed]
- Viney, K.A.; Johnson, P.; Tagaro, M.; Fanai, S.; Linh, N.N.; Kelly, P.; Harley, D.; Sleigh, A. Tuberculosis patients’ knowledge and beliefs about tuberculosis: A mixed methods study from the Pacific Island nation of Vanuatu. BMC Public Health 2014, 14, 467. [Google Scholar] [CrossRef] [PubMed]
- Getahun, H.; Aragaw, D. Tuberculosis in rural northwest Ethiopia: Community perspective. Ethiop. Med. J. 2001, 39, 283–291. [Google Scholar] [PubMed]
- Singh, M.M.; Bano, T.; Pagare, D.; Sharma, N.; Devi, R.; Mehra, M. Knowledge and attitude towards tuberculosis in a slum community of Delhi. J. Commun. Dis. 2002, 34, 203–214. [Google Scholar]
- Sommerland, N.; Wouters, E.; Mitchell, E.M.H.; Ngicho, M.; Redwood, L.; Masquillier, C.; van Hoorn, R.; van den Hof, S.; Van Rie, A. Evidence-based interventions to reduce tuberculosis stigma: A systematic review. Int. J. Tuberc. Lung Dis. 2017, 21, S81–S86. [Google Scholar] [CrossRef]
- Balogun, M.; Sekoni, A.; Meloni, S.T.; Odukoya, O.; Onajole, A.; Longe-Peters, O.; Ogunsola, F.; Kanki, P.J. Trained community volunteers improve tuberculosis knowledge and attitudes among adults in a periurban community in Southwest Nigeria. Am. J. Trop. Med. Hyg. 2015, 92, 625–632. [Google Scholar] [CrossRef]
- Croft, R.P.; Croft, R.A. Knowledge, attitude and practice regarding leprosy and tuberculosis in Bangladesh. Lepr. Rev. 1999, 70, 34–42. [Google Scholar] [CrossRef]
- Demissie, M.; Getahun, H.; Lindtjorn, B. Community tuberculosis care through ‘TB clubs’ in rural North Ethiopia. Soc. Sci. Med. 2003, 56, 2009–2018. [Google Scholar] [CrossRef]
- Smith, M. Stigma. Adv. Psychiatr. Treat. 2002, 8, 317–325. [Google Scholar] [CrossRef]
- Creamers, A.L.; de Laat, M.M.; Kapata, N.; Gerrets, R.; Klipstein-Grobusch, K.; Grobusch, M.P. Assessing the consequences of stigma for tuberculosis patients in urban Zambia. PLoS ONE 2015, 10, e0119861. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Yan, S.; Tong, Y.; Peng, X.; Yang, T.; Lu, Z.; Gong, Y. Status of tuberculosis-related stigma and associated factors: A cross-sectional study in central China. Trop. Med. Int. Health 2018, 23, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Boccia, D.; Hargreaves, J.; De Stavola, B.L.; Fielding, K.; Schaap, A.; Godfrey-Faussett, P.; Ayles, H. The association between household socioeconomic position and prevalent tuberculosis in Zambia: A case-control study. PLoS ONE 2011, 6, e20824. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, L.; Akande, T.; Shankar, A.V.; McIntire, K.N.; Gounder, C.R.; Gupta, A.; Yang, W.T. Gender-related barriers and delays in accessing tuberculosis diagnostic and treatment services: A systematic review of qualitative studies. Tuberc. Res. Treat. 2014, 2014, 215059. [Google Scholar] [CrossRef]
- Ganapathy, S.; Thomas, B.E.; Jawahar, M.S.; Selvi, K.J.; Sivasubramaniam Weiss, M. Perceptions of gender and tuberculosis in a south Indian urban community. Indian J. Tuberc. 2008, 51, 9–14. [Google Scholar]
- Onifade, D.A.; Bayer, A.M.; Montoya, R.; Haro, M.; Alva, J.; Franco, J.; Sosa, R.; Valiente, B.; Valera, E.; Ford, C.M.; et al. Gender-related factors influencing tuberculosis control in shantytowns: A qualitative study. BMC Public Health 2010, 10, 381. [Google Scholar] [CrossRef]
- Atre, S.; Kudale, A.; Morankar, S.; Gosoniu, D.; Weiss, M.G. Gender and community views of stigma and tuberculosis in rural Maharashtra, India. Glob. Public Health 2011, 6, 56–71. [Google Scholar] [CrossRef]
- Mason, P.H.; Roy, A.; Spillane, J.; Singh, P. Social, historical and cultural dimensions of tuberculosis. J. Biosoc. Sci. 2016, 48, 206–232. [Google Scholar] [CrossRef] [PubMed]
- Mason, P.H.; Degeling, C.; Denholm, J. Sociocultural dimensions of tuberculosis: An overview of key concepts. Int. J. Tuberc. Lung Dis. 2015, 19, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Abebe, G.; Deribew, A.; Apers, L.; Woldemichael, K.; Shiffa, J.; Testaye, M.; Abdissa, A.; Deribie, F.; Jira, C.; Bezabih, M.; et al. Knowledge, health seeking behavior and perceived stigma towards tuberculosis among tuberculosis suspects in a rural community in Southwest Ethiopia. PLoS ONE 2010, 5, e13339. [Google Scholar] [CrossRef] [PubMed]
- Guidroz, K.; Berger, M.T. A Conversation with Founding Scholars of Intersectionality: Kimberle Crenshaw, Nira Yuval-Davis, and Michelle Fine. In The Intersectional Approach: Transforming the Academy Through Race, Class & Gender; Berger, M.T., Guidroz, K., Eds.; The University of North Carolina Press: Chapel Hill, NC, USA, 2009. [Google Scholar]
- Hankivsky, O. Women’s health, men’s health, and gender and health: Implications of intersectionality. Soc. Sci. Med. 2012, 74, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Final Report of the Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- McCall, L. Introduction. In The Intersectional Approach: Transforming the Academy Through Race, Class & Gender; Berger, M.T., Guidroz, K., Eds.; The University of North Carolina Press: Chapel Hill, NC, USA, 2009. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Variables | Number (Percentage) |
|---|---|---|
| Sex | Male | 134 (73) |
| Female | 49 (27) | |
| Age (years) | Early working age (15–24) | 31 (17) |
| Prime working age (25–35) | 66 (36) | |
| Prime working age (36–54) | 68 (37) | |
| Mature working age (55–64) | 13 (7) | |
| Elderly (≥65) | 5 (3) | |
| Mean Age (SD) | 37 (±12) | |
| Years of Education | Illiterate | 52 (28) |
| Till primary (1–5) | 32 (18) | |
| 6–8 | 27 (15) | |
| 9–12 | 14 (8) | |
| 13–16 | 58 (32) | |
| Occupation | Unemployed | 4 (2) |
| Housewife | 28 (15) | |
| Student | 16 (9) | |
| Laborer | 55 (30) | |
| Small scale business owner | 17 (9) | |
| Business (or landlord) | 18 (10) | |
| Government employee | 3 (2) | |
| Private sector employee | 42 (23) | |
| Religion | Muslim | 167 (91) |
| Christian | 1 (0.5) | |
| Hindu | 15 (8.5) | |
| Location | Urban | 127 (69) |
| Rural | 56 (31) | |
| Province | Punjab | 93 (51) |
| Sindh | 57 (31) | |
| Khyber Pakhtunkhwa | 12 (7) | |
| Balochistan | 21 (11) | |
| Total | 183 | |
| Items of Perceived Stigma Sub-Scale | Status of Stigma for Each Item | |
|---|---|---|
| Present (%) | Absent (%) | |
| Some people may not like to eat and drink with relatives who have TB | 143 (78) | 40 (22) |
| Some people feel uncomfortable about being near those with TB | 136 (74) | 47 (26) |
| If a person has TB, some community members will behave differently towards that person for the rest of his/her life, even if s/he is treated and cured | 81 (44) | 102 (56) |
| Some people do not want those with TB playing with their children | 118 (64) | 65 (36) |
| Some people keep their distance from people with TB | 136 (74) | 47 (26) |
| Some people think that those with TB are disgusting | 70 (38) | 113 (62) |
| Some people do not want to talk to others with TB | 63 (34) | 120 (66) |
| Some people are afraid of those with TB | 113 (62) | 70 (38) |
| Some people try not to touch others with TB | 95 (52) | 88 (48) |
| Some people may not like to eat and drink with friends who have TB | 139 (76) | 44 (24) |
| Some people prefer not to have those with TB living in their community | 49 (27) | 134 (73) |
| Some people think that those with TB, both male and female face same social problems (marriage, job, continuing education, attending social gatherings etc.) | 131 (72) | 52 (28) |
| Some people think that those males with TB face more problems in marriage | 142 (78) | 41 (22) |
| Some people think that those females with TB face more problems in marriage | 157 (86) | 26 (14) |
| Some people think that those females with TB depend economically on their husbands and in-laws and need their cooperation to obtain treatment | 105 (57) | 78 (43) |
| Some people think that a family with TB patient should not allowed to participate in any social function | 75 (41) | 108 (59) |
| Some people think that female TB patient should be sent off to her parent’s house | 38 (21) | 145 (79) |
| Knowledge Variable | Number (%) |
|---|---|
| TB is curable | 159 (87) |
| TB patient also has HIV/AIDS | 45 (25) |
| TB leads to infertility | 54 (30) |
| Emotional stress is a cause of TB | 91 (50) |
| Perceived mode of TB transmission | |
| Contaminated food | 134 (73) |
| Cough | 167 (91) |
| Sharing meal with a person with TB | 100 (55) |
| Unclean water and food | 114 (62) |
| Sharing utensils with a person with TB | 96 (53) |
| Touching a person with TB | 61 (33) |
| Sex with a person with TB | 93 (51) |
| Variable | Stigma Level | Crude Odds Ratio (95% CI) | ||
|---|---|---|---|---|
| High n (%) | Low n (%) | |||
| Sex | Male | 72 (53.7) | 62 (46.3) | 0.82 (0.63, 1.06) |
| Female | 32 (65.3) | 17 (34.7) | 1.33 (0.87, 2.04) | |
| Urban or Rural Location | Urban | 72 (56.7) | 55 (43.3) | 0.99 (0.82, 1.21) |
| Rural | 32 (57.1) | 24 (42.9) | 1.01 (0.65, 1.57) | |
| Education Level | Till grade 5 | 52 (61.9) | 32 (38.1) | 1.2 (0.89, 1.72) |
| Above grade 5 | 52 (52.5) | 47 (47.5) | 0.84 (0.64, 1.10) | |
| Employment Status | Employed | 76 (56.3) | 59 (43.7) | 0.98 (0.82, 1.17) |
| Unemployed | 28 (58.3) | 20 (41.7) | 1.06 (0.65, 1.74) | |
| TB is curable | Yes | 86 (53.4) | 75 (46.6) | 0.87 (0.79, 0.96) |
| No | 18 (81.8) | 4 (18.2) | 3.42 (1.20, 9.70) | |
| TB spreads through cough | Yes | 94 (56.3) | 73 (37.5) | 0.98 (0.89, 1.07) |
| No | 10 (62.5) | 6 (37.5) | 1.27 (0.49, 3.34) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, S.M.; Anjum, N.; Ishaq, M.; Naureen, F.; Noor, A.; Rashid, A.; Abbas, S.M.; Viney, K. Community Knowledge about Tuberculosis and Perception about Tuberculosis-Associated Stigma in Pakistan. Societies 2019, 9, 9. https://doi.org/10.3390/soc9010009
Ali SM, Anjum N, Ishaq M, Naureen F, Noor A, Rashid A, Abbas SM, Viney K. Community Knowledge about Tuberculosis and Perception about Tuberculosis-Associated Stigma in Pakistan. Societies. 2019; 9(1):9. https://doi.org/10.3390/soc9010009
Chicago/Turabian StyleAli, Syed Mustafa, Naveed Anjum, Muhammad Ishaq, Farah Naureen, Arif Noor, Aamna Rashid, Syed Muslim Abbas, and Kerri Viney. 2019. "Community Knowledge about Tuberculosis and Perception about Tuberculosis-Associated Stigma in Pakistan" Societies 9, no. 1: 9. https://doi.org/10.3390/soc9010009