Decision-Making Behaviour under the Mental Health Act 1983 and Its Impact on Mental Health Tribunals: An English Perspective


School of Law, University of Manchester, Manchester, M13 9PL, UK
Laws 2018, 7(2), 12; https://doi.org/10.3390/laws7020012
Submission received: 21 February 2018
/
Revised: 19 March 2018
/
Accepted: 20 March 2018
/
Published: 24 March 2018
(This article belongs to the Special Issue Concerns, Contradictions and Reality of Mental Health Law)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:In England and Wales, the Mental Health Act 1983 (MHA 1983) provides the legal framework which governs decisions made concerning the care and treatment of those suffering from mental disorders, where they may pose a risk to themselves or others. The perspective of the patient and the care provider may conflict and can be a source of tension and challenge within mental health law. Through access to a mental health tribunal, patients are offered the apparatus to review and challenge their detention. With detention rates under the mental health legislation rising exponentially, this is having a knock-on effect upon tribunal application numbers. As there is a legal requirement to review all cases of individuals detained under the MHA 1983, understanding the key drivers for this increase in detention is essential in order to understand how to better manage both detention rates and the upsurge in tribunal caseloads. With the increase in overall activity, mental health tribunal workloads present significant practical challenges and has downstream cost implications.
Keywords:
detention; caseload; mental health tribunal; Mental Health Act 1983; decision-making; risk; costs1. Introduction
Mental illness costs the UK economy £100 billion a year (Johnson 2016; McCrone et al. 2008). In 2012, the Her Majesty’s (HM) Government spent £126 billion on health (HM Treasury 2011, p. 3), and pledged to spend a further £400 million on psychological therapies and mental health care provision for children and young people (Department of Health 2011, p. 41). Mental health needs remain acute and have garnered further political support in recent years. Following the 2017 Autumn budget £6.3 billion of extra National Health Service (NHS) funding was announced, of which £2.8 billion will be poured into day-to-day health services and £3.5 billion in new buildings and equipment (HM Treasury 2017). However, none of this promised funding has been ringfenced and concerns remain that mental health will see little additional funding.
The funding landscape is important when considering how the mental health legislation is deployed when responding to serious mental health support needs. In England and Wales, the Mental Health Act (MHA) 1983 provides the legal framework which governs decisions made concerning the care and treatment of those suffering from mental disorder where they may pose a risk to themselves or others (Department of Health 2015). The legislation sets out the circumstances when mental health professionals can make decisions about detention and/or treatment without the patient’s consent. The legislation is tasked with providing a system of checks and balances, ensuring robust and justifiable decisions are made and the patient’s interests are well served. While the legislation does this, situated at its heart is the need to protect others from potential harm. Getting the balance right remains a primary, though sometimes difficult, goal.
Getting to the right decision is crucial and has become more so since the Human Rights Act 1998, which requires UK compliance with the European Convention in Human Rights. Articles 3, 5, 6, and 8 play a central role within mental health. Article 3 provides the right not to be subjected to torture or to inhuman and degrading treatment or punishment. Article 5 provides a right to liberty and security except on defined and discrete grounds. Article 6 provides a right to a fair and public hearing that is both timely and independent. Article 8 provides a right to respect for private and family life unless interference is justified as a proportionate response to a legitimate reason. Detention is allowed under Article 5 European Convention on Human Rights when there is evidence of ‘unsound mind’ and it is this which has so far provided justification for the mental health legislation currently in place. As long as a patient meets the Winterwerp criteria (Winterwerp v The Netherlands (1979) ECHR 4): the patient is of unsound mind; the mental disorder is of a kind or degree warranting confinement; and the mental disorder is persistent, detention will be lawful. However, the United Nations Convention on the Rights of Persons with Disabilities (CRPD), has taken on the mantle of promoting and protecting the human rights of persons with disabilities across the globe. It has sparked a broader global debate about how far existing mental health laws can be reconciled with the CRPD’s key principles, which include freedom from discrimination and autonomy, given the common reliance on all-encompassing concepts, such as ‘mental disorder.’ For example, how can Article 14 of the CRPD, which prohibits detention on the grounds of disability and thus excludes detention solely on the grounds of mental disability, be reconciled with the mental health law frameworks operating within numerous countries that are founded on this detention criteria? For many academics and advocates, the CRPD underscores the argument that forcible detention (and treatment) for a mental disorder is unjustifiable and discriminatory (Szmukler et al. 2014, 2010). It has also been argued that the radical interpretation of the CRPD text by the Committee for the UN Convention on the Rights of Persons with Disabilities may threaten the value the CRPD could bring to bear in the protection of patients’ rights (UN Committee on the Rights of Persons with Disabilities 2014). For example, Freeman et al. (Freeman et al. 2015) argue that requiring health professionals to always ensure informed consent is obtained from people with disabilities before detention and/or treatment could undermine access to needed care and support. Obtaining informed consent is not always possible given an individual’s condition, and as such, sometimes the need for informed consent should be superseded.
The CRPD promotes access to justice as a key component to protect the rights of people with disabilities. This reinforces existing rights reiterated in Winterwerp where guidance concerning the patient’s right to challenge detention was laid down. The detention criteria must be ‘in accordance with a procedure prescribed by law’ and set out in legislation that can be scrutinised in court. Through access to a mental health tribunal, patients are offered the apparatus to review and challenge their detention (MHA 1983, section 66). This right to review was first established under the MHA 1959 and has since been amended and refined with further amendments introduced by the MHA 1983 and the MHA 2007. It is this right to challenge and, specifically, the rising mental health tribunal caseload, that is the focus of this paper.
This paper argues that the increasing mental health tribunal caseload in England and Wales is an inherent consequence of increased detention under the MHA 1983. Detention rates under the mental health legislation have been rising exponentially; a consistent trend over the last decade. This has had a knock-on effect on tribunal applications. The ‘tribunal caseload problem’ has become a policy question which is receiving increased attention from the UK government, largely because of the downstream cost implications. This paper argues that trying to reduce tribunal caseload through structural changes to the mental health tribunal system will not be sufficient to address the problem. Rather, it is necessary to determine the factors that influence initial entry into the mental health system and understand why reliance on the legislation is going up. The reasons behind accelerating formal detention rates under the MHA 1983 are complex, and often multi-factorial. With each patient and their needs being unique, the clinical and social response necessarily reflects this. However, as discussed below, the clinical case for detention is not the only factor influencing decision-making behaviour; limitations and strains elsewhere in the mental health system are compelling clinicians to adopt a broader interpretation of the detention criteria. This is having a marked effect upon overall detention rates.
2. Mental Health Tribunals
In the UK, there are over 70 different tribunals that cover a wide range of areas affecting day-to-day life. Tribunals are independent and typically provide a forum to hear and determine appeals by individuals against an initial governmental decision. Tribunals play a crucial role, for they provide the means by which people in the wider community can access justice with relatively little cost and greater ease. Fundamentally, tribunals provide the necessary adjudicative mechanism to meet the important right of administrative justice: to ensure the legality of decision making, through fair, transparent and independent evaluation and review (The Franks Report 1959, p. 23). The tribunal system has undergone significant reform following the Leggett Review in 2001 (Leggatt Andrew 2001), the White Paper, Transforming Public Services in 2004 (Department of Constitutional Affairs 2004) and the enactment of the Tribunals, Courts and Enforcement Act 2007. Mental health tribunals have been renamed ‘First-tier Tribunals (Mental Health)’ following the 2007 Act and are tasked with reviewing the legality of formal detention and guardianship under the MHA 1983. Their jurisdictional remit is governed by Section 72 of the legislation and it enables them to discharge both civil and forensic patients.
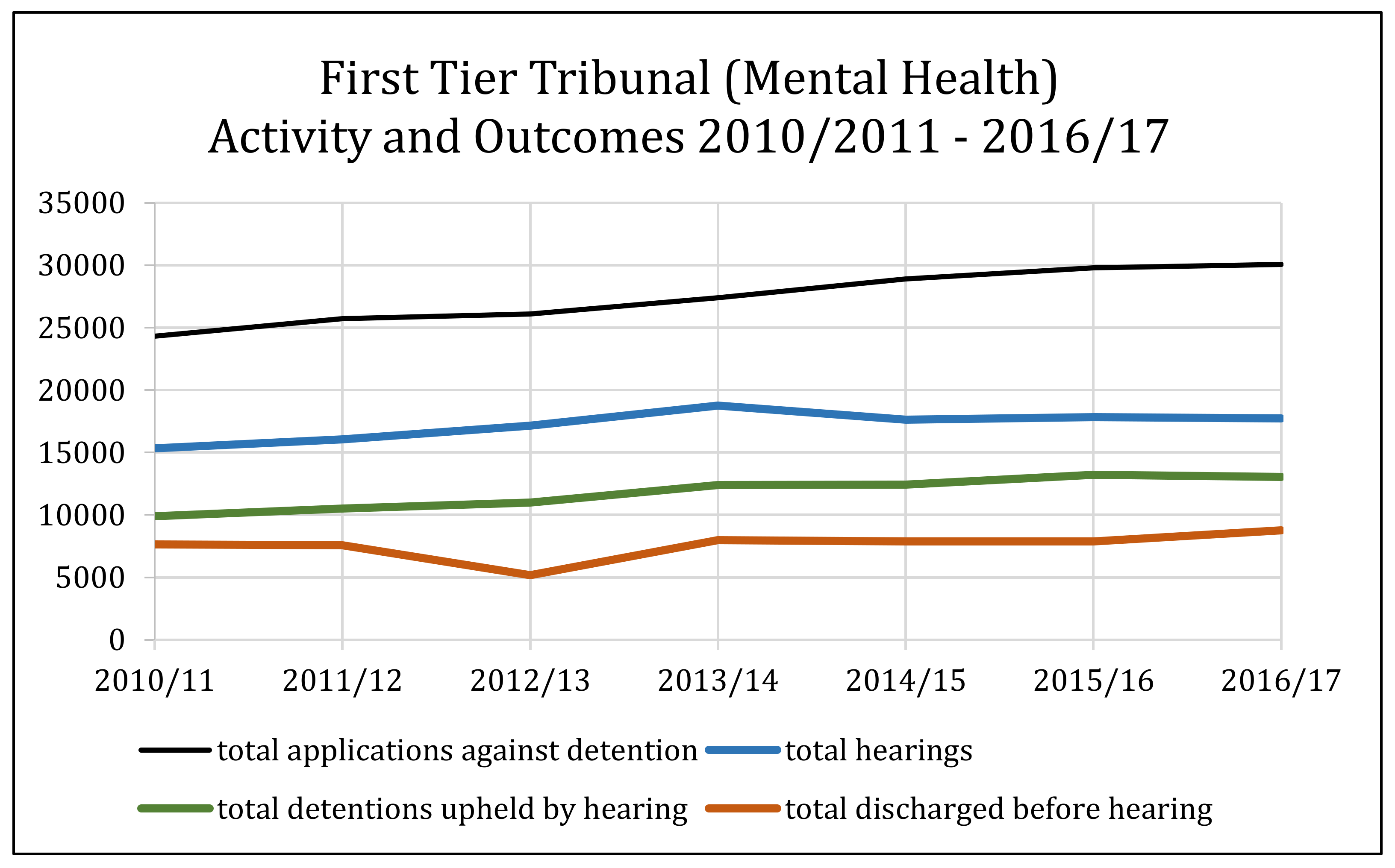
Mental health tribunals have many distinctive characteristics which differ markedly from those of other tribunals (Peay 1989; Perkins 2003a). Unlike many other tribunals, mental health tribunals are dealing with fundamental rights. Its purpose is to undertake a review of an individual’s current detention in a psychiatric hospital under the MHA 1983 and deals directly with the deprivation of an individual’s liberty. Protecting Article 5 ECHR rights to liberty and reinforcing the crucial need for due process when the restriction or removal of liberty is at stake ensures that mental health tribunals act a fundamental safeguard. Data suggests that deprivation of liberty under the MHA 1983 is predominantly deemed justifiable as outlined in Figure 1. In 2016/17, 30,079 applications were made to the mental health tribunal, with 17,744 hearings. Of these hearings, 13,033 detentions were upheld and 8751 patients were discharged before hearing. 73% of hearings resulted in detention being upheld as justified in whole or in part and in the interests of the patient.
Access to and timing of a tribunal hearing depends upon the nature of the detention. A patient can be sectioned under several different parts of the legislation for assessment or to receive treatment for a mental disorder. Part II of the Act deals with the civil commitment provisions. These are the sections that do not involve the criminal law and include Section 2 (for assessment), Section 3 (detention for treatment), Section 4 (emergency detention), and, Sections 5(2) and 5(4) (holding powers). Part III of the Act contains with the forensic sections. They deal with patients who have been involved in criminal proceedings and include Section 35 (remand to hospital for report), Section 36 (remand to hospital for treatment), Section 37 (hospital order), Section 38 (interim hospital order), Section 47 (transfer of sentenced prisoner to hospital), Section 48 (removal to hospital of unsentenced prisoners), Section 47/49 (transfer from prison to hospital with restrictions), Section 48/49 (removal to hospital of other prisoners with restrictions), Section 37/41 (hospital order with restriction) and Section 41 (the conditionally discharged patient). Patients whose detention is subject to restrictions face a different review timeframe to those patients whose detention, whether civil or criminal, is not subject to restrictions. Restrictions refer to Section 41 patients; those detained ‘during her Majesty’s pleasure’; those acquitted on the grounds of insanity, and those found unfit to plead. Only one application to the tribunal can be made during ‘the relevant period’ which, for them, is between six and twelve months of the court disposal and once a year thereafter. The Home Secretary must refer a case if it has not been considered in the previous three years; where a previously ‘unfit to plead’ patient has not made a referral in the first six months; or, where a conditionally discharged patient has been recalled to hospital.
For unrestricted patients, only one application can be made during ‘the relevant period’ which differs depending upon the nature of the patient’s detention or circumstance giving rise to the application. For Section 2, admission for assessment, the application must be made within 14 days of admission. For Section 3, admission for treatment the application must be made within six months of admission. Following renewal of detention, applications to the tribunal can initially take place within the first six months, then every twelve months thereafter. Review following transfer from guardianship to hospital must take place within six months and for hospital orders, review applications can be made between six and twelve months of order and then every twelve months. The tribunal system is placed under particular strain as a result of the tight processing time for Section 2 patients.
Mental health tribunals are concerned with de novo decisions. In other words, the tribunal is not concerned with assessing whether the initial decision made by clinicians to detain an individual under the MHA 1983 is right or wrong. Instead, the tribunal in concerned with assessing a patient on the day of the tribunal hearing, to determine whether continued detention is justified and meets the detention criteria laid down under the MHA or whether discharge is appropriate. The tribunal panel is not required to consider whether a patient had been properly detained in the first place, but rather on whether they are satisfied that the criteria for detention continue to be met. There are two points to note regarding case evidence. First, evidence concerning the initial decision to detain, including the initial evaluation, risk assessment and context surrounding initial entry into the mental health system offer the panel little in terms of conclusive findings. Indeed, even the clinical reports that must be supplied to the tribunal prior to the hearing may not represent the current state of the patient and may serve little purpose beyond demonstrating the patient’s mental health journey since being detained (Practice Direction First-Tier Tribunal Health Education and Social Care Chamber Statements and Reports in Mental Health Cases 2013). Secondly, the oral evidence received by the tribunal on the day of the hearing can consequently vary considerably from the paper evidence. The professional medical, social and nursing oral evidence will have a manifest effect upon the outcome of the hearing on the day. Furthermore, a tribunal hearing also provides an opportunity for supplementary evidence to be presented which may demonstrate a patient’s experience in hospital and attitude towards recovery, such as educational achievement certificates etc. This evidence will not determine whether the legal criteria for detention are met, but does offer the panel a broader more holistic picture of the patient. Indeed, where hearings are heard without the presence of the patient and ‘on the papers,’ the opportunity for a more nuanced evaluation of the evidence is lost.
Mental health tribunals also differ from other tribunals in that case review can be applied for (Department of Health and Social Care 2013) or can take place automatically. A patient’s case can be heard either on application from the patient or the patient’s nearest relative, on referral from the Secretary of State or, if the mental health tribunal has not reviewed the case within a given period, on referral by hospital managers (automatic review). Under the 1983 Act, Section 68 sets out the provisions for when hospital managers must make a referral (Department of Health 1982, para. 24). Mental health tribunals hearing a case that has been initiated through automatic review must be aware that the patient may still decide to challenge their detention despite the fact that they have not themselves sought case review. Likewise, patients may not be seeking discharge.
Finally, unlike other tribunals, mental health panel hearings are undertaken in-situ, usually in the confines of the hospital where a patient is detained. The (Department of Health 2015, para. 32.33 and 32.34), requires the provision of suitable accommodation for panel hearings to take place. The accommodation should be fit for purpose, private, quiet and clean and be large enough to accommodate all relevant participants of the hearing. Furthermore, the patient should be offered access to a private room to enable them to have separate discussions with their representative (HM Courts and Tribunals Service 2012). Hearings in-situ are a pragmatic response to the particular needs of patients and the practical difficulties of arranging hearings outside of the hospital environment, for example, the challenge around the transit of patients. Yet, hearings in-situ also present problems. The importance of the built environment upon legal proceedings is signaled as a major issue around how legal processes and proceedings are perceived (Mulcahy 2011). It is possible that mental health tribunal hearings may not be seen to be acting as an independent judicial mechanism because they convene within the same space as the detention process. For patients, the ability to separate out the experience of detention, which may have been undertaken unwillingly, and the independent legal case review process, may be difficult. There may also be difficulty in ensuring mental health tribunal panels maintain continuity in their decision making. With hearings taking place up and down the country, separated from other judicial proceedings, the scope for inconsistent application of the law exists. However, the MHA 1983 relies on the decision maker to use discretion when coming to a conclusion and must provide reasons supporting the decision.
3. Detention Rates under the Mental Health Act 1983
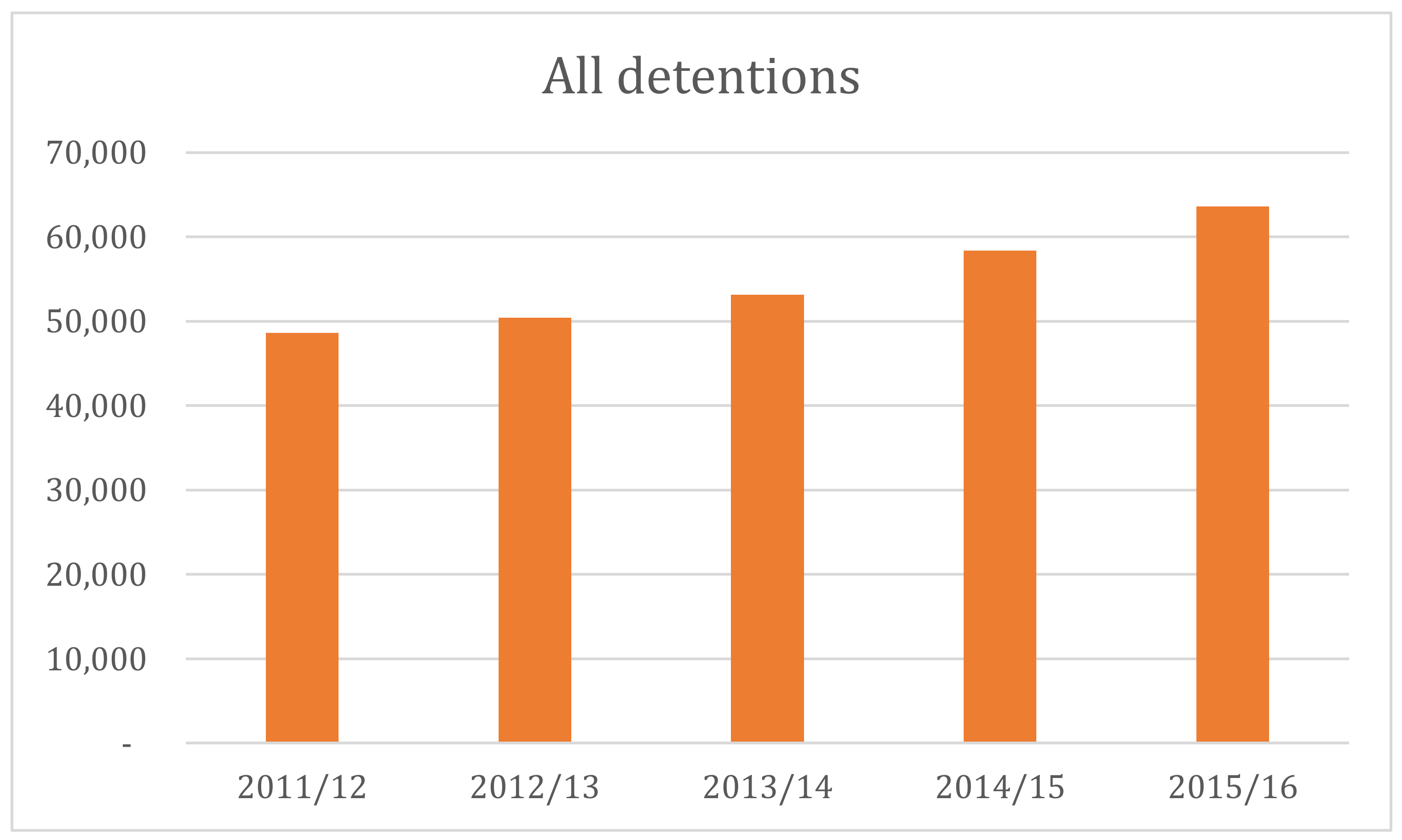
In England and Wales, the number of people detained under the MHA 1983 is rising exponentially—a trend that has been continuing for the last decade. As demonstrated in Figure 2 below, some 63,600 people were detained under the MHA 1983 in 2015/16 compared to 43,400 in 2005/06—an increase of 47%. The 2015/16 detention figure is the highest it has been since 2005/06 when 43,361 detentions were recorded.
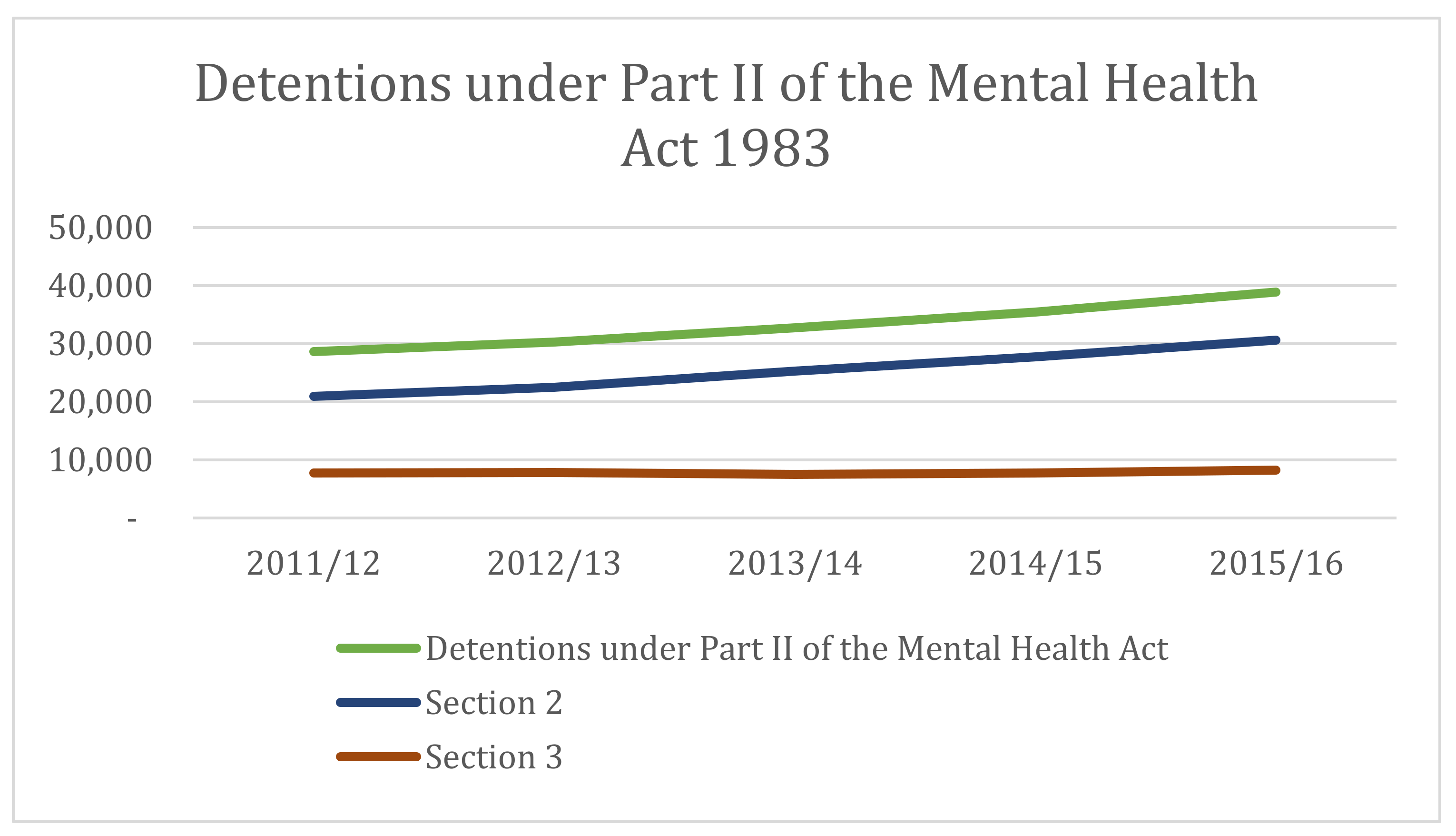
Specifically, detentions under Part II of the MHA 1983, that is Section 2 admission for assessment and Section 3 admission for treatment, have seen particular rises from over 28,500 in 2011/12 to nearly 39,000 in 2015/16 (nearly a 27% increase). For Section 2 detentions alone, there has been a rise of nearly 32% between 2011/12 and 2015/16 (Figure 3 below).
3.1. A System under Strain?
These increases have occurred at a time when both mental health and social care provision continue to experience significant financial challenges. With austerity continuing to bite, mental health provision has not always received the attention it deserves with physical health needs dominating resource allocation. However, mental health conditions account for 23 per cent of the total burden on the NHS, but only 13 per cent of NHS spending is directed towards psychiatric and related services. This under-investment is not new and despite funds being channeled through Primary Care Trusts at a regional level to recognised areas of need prior to the Health and Social Care Act 2012 and now through Clinical Commissioning Groups (CCGs) following the 2012 Act, resource shortfalls continue (Glover-Thomas 2013). Mental health, commonly referred to as the ‘Cinderella’ service, has been struggling under the weight of systemic neglect for a considerable time. Mental health care must compete with all other health and social care needs; many of these present more tangible and positive post-treatment outcomes and can more easily be quantified.
The needs associated with mental ill-health have been explicitly recognised for some time. In 2011, a newly crafted mental health strategy was published, No Health Without Mental Health: A Cross-Government Mental Health Outcomes Strategy for People of All Ages (Department of Health 2011), followed by an implementation framework which sought to reinforce mental health as a key priority. The strategy aimed to provide better mental health for all and to increase the likelihood of recovery, while the implementation framework focused on the provision of strong outcomes monitoring. In the Health and Social Care Act 2012, these mental health objectives were mapped onto the NHS restructuring process. The 2012 Act sought to do this by explicitly recognising that mental ill-health should be given parity alongside other physical health needs.
Despite these efforts to reinforce the need to support mental health provision, mental health continues to experience the effects of low funding and underinvestment compared to its physical health counterparts. Identifying and understanding the source of this underinvestment has proven difficult. CCGs have underinvested in mental health services relative to physical health services. However, the degree of the disparity has largely been obscured by the way spending on mental health conditions is grouped together and reported, unlike spend on physical health care, which is disaggregated by specific conditions. Spending per capita across CCGs varies almost two-fold in relation to underlying need. The social care system is also under sustained and growing pressure, with significant real-terms cuts in spending resulting in a reduction in the number of people accessing publicly funded care (The King’s Fund 2015).
In 2016, the pressure placed upon the NHS was recognised. The provision of universal, high quality healthcare remains a steadfast commitment, but the way in which the NHS operates to meet this requires change to accommodate the modern-day context. In 2016, NHS England published a report, Five Year Forward View for Mental Health (NHS England 2016), which identified key recommendations to improve both the experience of health care and overall outcomes. The report identifies key changes that necessitate a radical rethink around healthcare provision. Notably, a central aspect of the strategy is the recognition that steps need to be taken to respond to increasing inflexibility within the NHS as it impedes health care provision. Artificial barriers within the NHS structure often stymy effective policy and practical implementation, while successful joint working between different facets of the NHS has been hindered.
Modern day mental health care emphasises the view that more people benefit when care is provided in the least restrictive way (Department of Health 2015, p. 22). The more traditional interpretation of this notion focuses upon keeping people out of hospital and in the community as often as possible and providing the support needs required. In practice, this has not always been easy to achieve in terms of providing the levels of community-based support needed. However, understanding that patients are much more likely to have a better outcome if allowed to stay within a familiar home environment while accessing support networks is universally accepted. It is also acknowledged that when patients do have to go to hospital, and require formal detention, the experience is less traumatic and more likely to have a positive outcome when a patient is detained locally (McNicoll 2014).
Data suggests that achieving this is increasingly difficult. Sending people out of area for acute inpatient care as a result of local bed pressures has become a spiraling problem and is having a negative impact upon the way in which mental health care operates and how patients experience their care (NHS Digital 2017). The Mental Health Task Force (Mental Health Taskforce 2016) recommended that round the clock community-based mental health crisis care be made available in all areas across England and adequately resourced intensive home treatment to reinforce the emphasis upon non-inpatient care when appropriate and to reduce increasing reliance on out of area placements (NHS England, 2016). Whether the funding for this will be provided remains to be seen.
3.2. Rising Use of Section 2
One issue that is adding significantly to detention rates is the increased use of Section 2, as seen above in Figure 3. This section authorises the compulsory admission of a patient for the purpose of assessing the patient’s mental condition. Section 2 also allows for medical treatment to follow assessment. Treatment under this section has the same scope as that found under Section 3 and includes nursing, psychological intervention and specialist mental health habilitation, rehabilitation and care (MHA 1983, section 145). However, the power to detain is time limited for up to 28 days. Consequently, Section 2 may be used in practice as a way of providing short-term interim care and treatment.
Section 2 requires admission for assessment may be made in respect of a patient on the grounds that:
- (a)
- he is suffering from mental disorder of a nature or degree which warrants the detention of the patient in a hospital for assessment (or for assessment followed by medical treatment) for at least a limited period; and
- (b)
- he ought to be so detained in the interests of his own health or safety or with a view to the protection of other persons.
In R v. Wilson, ex parte Williamson ([1996], COD 42), the court emphasised the importance of using the appropriate section to detain a patient. Section 2 use should only be for a short duration and for a limited purpose. It should be used to assess a patient’s condition to determine whether treatment would be effective and whether a Section 3 application would be an appropriate next step; yet, the data suggests that Section 2 is being used well beyond these narrow remits.
There are several reasons for the increased use of Section 2. The provision is thought to assist with access to mental health services. The availability of beds has decreased and bed shortages are resulting in delayed admission. With bed occupancy rates in inpatient facilities being well above recommended levels, use of voluntary admission as a preferred method of entering the mental health system is being hampered by scarce resources. Where a patient is deemed in need of care in hospital, resort to civil commitment may be the quickest means of opening up services. The bed occupancy data for all mental health overnight beds was largely stable throughout 2017, though demonstrated a significant overall decline. Across England there is were just over 18,000 beds available. In 2015/16 mental health beds for overnight use were in the region of 22,500 as depicted in Figure 4 below. This accounted for a 20% drop in available beds between 2015 and 2017. In 2001, 34,214 overnight beds were available for use. This represents a 47% reduction of mental health beds since 2001.
Mental health inpatient bed occupancy is frequently well above recommended levels. Community care facilities and services, particularly crisis resolution and home treatment teams that often deal with acute care needs, struggle to provide sufficient levels of support to compensate for bed scarcity. This is creating intense pressure on both hospital and community services and is having a negative impact on safety and quality of care (Care Quality Commission 2016). Furthermore, the lack of available local beds is leading to higher numbers of out-of-area placements for inpatients. When beds are unavailable locally patients are being transferred to facilities outside their area.
In 2012/13 over 4% of adult emergency admissions were out of area (Care Quality Commission 2016). ‘Out of area’ placement occurs when a placement for acute mental health in-patient care is needed by a patient, yet no beds are available in the usual local network of services. When this occurs, a placement is found ‘out of area.’ In some areas, reliance upon out of area beds is particularly widespread and has meant journeys of more than 300 miles for some patients. Moving patients out of their area and away from family and support networks has been found to have a negative impact upon the patient’s experience (McNicoll 2014). For patients with a bed on an acute ward, the environment may not always be safe or therapeutic, or conducive to recovery. While for those waiting for a bed because of bed shortages, any lack of early intervention or crisis care support may worsen their health forcing a decision to move them out of area in order to secure a bed.
Another key area of concern believed to be directly impacting upon formal detention rates is the role of inequalities and cognitive bias in decision making. Data from 2016/17 outlined in Figure 5 below, illustrates that people within a broad Black ethnic group were more likely to be detained under the MHA 1983, with those from the Black Caribbean group having the highest rate of detention of all ethnic groups. Work is currently being undertaken to understand why these differential rates of detention are taking place (Mental Health Act: independent review, due to report Autumn 2018).
3.3. Declining Community Support and Its Impact
A further factor that has influenced the increasing use of the civil commitment procedures under Part II of the MHA 1983 is the decline in contact patients experience when in the community (Care Quality Commission 2016). Evidence supports the view that a key component of a successful community care experience is the presence of strong family and social networks for the individual concerned (Glover 1999; Allmark et al. 2013). Lintern’s work suggests that with less support in the community, the safety net such services provide is often inadequate to meet needs (Lintern 2012). Keeping patients out of acute crisis becomes increasingly difficult and a factor in the rising numbers of detentions. With real term cuts in funding by the NHS on mental health, access to care outside of acute provision has become more difficult (McNicoll 2015; Lintern 2014; Care Quality Commission 2015). For example, assertive outreach provision as part of a traditional Community Mental Health Team’s arsenal has suffered significant funding cuts over the last few years (The King’s Fund 2015; Firn et al. 2013).
Without sufficient funding to support community-based care, accessing services for patients has required greater reliance on formal hospital detention provisions. However, the inpatient data suggests that entry into the mental health system for many continues to be through Section 2. Unless the criteria for Section 3 admission for treatment are met, most patients will be discharged within 28 days. For many patients, this brief window of time is enough to stabilise their condition and allow for continued good health in the community. However, for others, as the Care Quality Commission suggest in its report—Monitoring the Mental Health Act in 2015/16 (Care Quality Commission 2016), increasing detention rates may have been affected by the rise of revolving door patient numbers. These are patients who often experience repeated involuntarily hospitalisations. However, trying to determine the extent to which inpatient data includes revolving door patients is difficult. The data is not sufficiently nuanced; it does not demarcate the nature of the admission, past psychiatric history and community care experience. Constructing an accurate representation of patients entering the mental health system under the MHA 1983 is therefore problematic.
Revolving door patients have been an ongoing problem. Community Treatment Orders (CTOs), introduced under the MHA 2007, were an attempt to respond to the challenges presented by this patient population. However, further questions have been raised about the potential correlation between rising detention rates and the introduction of CTOs. Whether Parliament should introduce a regime of supervised community treatment in England and Wales was a long-standing question, beginning with the decision in R v Hallstrom, ex p W ([1985] 3 All E R 775). The CTO (also known as ‘Supervised Community Treatment’, or SCT) authorises community-based supervision of compulsory patients following their discharge from hospital (MHA 1983, section 17A-17G). A patient discharged onto a CTO must comply with the conditions of the order or face recall to hospital (MHA 1983, section 17B(3)(a)).
Arguments against CTOs have largely centred on civil liberties, public protection and the professional legitimacy of care and treatment providers (Dawson 2005). It appears that as long as ‘the practice is properly regulated, its criteria, procedures, and powers are clearly specified by law, it makes proper use of medical expertise, and it applies in a proportionate manner’ (Dawson 2010) supervised community treatment will not violate a patient’s human rights (L v Sweden (App No 1080/84); Johnson v UK (1997) 27 EHRR 296; Bartlett et al. 2007; Richardson 2008). Yet, this position remains a contested one with some arguing that the CRPD now limits any justification there might have been for managing mental health conditions differently from that of other medical conditions (for example, Minkowitz 2007). The strongest argument in favour of CTOs holds that it serves as a mechanism for a continuous system of care allowing effective transition between hospital and community care (K v Craig [1998] UKHL 54). This framework for long-term community care was thought to reinforce rights and responsibilities (Romans et al. 2004) for both users and providers of this service (Swanson et al. 1997).
Despite the anticipated benefits associated with CTOs, evidence suggests that these have yet to materialise. The result of the Oxford Community Treatment Order Evaluation Trial (OCTET) (Burns et al. 2008; Rugkåsa et al. 2015), undertaken in 2012 suggests that CTOs have not reduced the rate of readmission to hospital as compared with the use of Section 17 leave. In 2011/12, there were 4220 CTOs in operation. By 2015/16 this was 4361 (NHS Digital 2011). The early expectation was that CTO use would gradually increase over time assuming that these community-based provisions would enable a formal shift away from in-patient mental health care. The impact assessment for the MHA 2007 projected NHS savings of approximately £34 million per year by 2014–2015 assuming that 10% of Section 3 admissions would instead be placed under supervised community treatment. The data tells us that the expectation around patterns of decision making behaviour have not changed radically with detention figures continuing to rise.
3.4. The Cheshire West Effect (and Other Cases)
The Supreme Court in P v Cheshire West and Chester Council; P & Q v Surrey County Council ([2014] UKSC 19 (‘Cheshire West’)) clarified an ‘acid test’ for what constitutes a ‘deprivation of liberty.’ The outcome of this case has significantly lowered the threshold for the engagement of Article 5 ECHR. The acid test states that an individual is deprived of their liberty for the purposes of Article 5 ECHR if they: lack the capacity to consent to their care/treatment arrangements; are under continuous supervision and control; and are not free to leave. All three elements must be present for the acid test to be met.
This case raised several fundamental questions around the concept of physical liberty and what is needed to both protect this and ensure detention is legitimate. A vital question addressed by the cases was whether the concept of physical liberty protected by Article 5 is the same for everyone, regardless of whether or not they are mentally or physically impaired. Linked to this was a second question, around what the essence of deprivation of liberty was, and what could be permissible and non-permissible deprivations of liberty under Article 5. In determining whether the acid test was met, the court held that it was irrelevant if the person concerned complied or simply did not object. Furthermore, the relative normality of the placement was irrelevant as was the reason or purpose behind a particular placement. Key to this policy driven decision was the recognition that the position of extremely vulnerable people needs to be subject to independent periodic checks.
The ruling in Cheshire West has had significant practical implications. Data published by the Health and Social Care Information Centre (HSCIC) confirmed that, following the Supreme Court judgment, in the first year, Deprivation of Liberty orders (DoLS) applications rose approximately ten-fold. In 2013/14 there were approximately 13,700 applications. In 2014/15 there were 137,540. Of these, 62,645 applications were completed by local authorities during the year, almost five times as many as in 2013–2014. In a Written Ministerial Statement (Dineage 2018) by Health Minister, Caroline Dinenage, it has been confirmed that the Government is largely in agreement with the Liberty Protection Safeguards model proposed by the Law Commission in 2017 (Law Commission 2017) and will bring forward legislation to provide greater protection for some of the most vulnerable people in our society, when parliamentary time allows. The Cheshire West decision, significantly widened the numbers of vulnerable people considered to be deprived of their liberty and the Liberty Protection Safeguards model is thought likely to offer a solution to the problems caused by the failing Deprivation of Liberty Safeguards. This model sets out rules designed to ensure that people that lack the capacity to consent, such as those with dementia or learning disabilities, are protected when deprived of their liberty in a hospital or care home. In the longer term, law reform will hopefully help to distinguish individuals allowing better and more tailored care and will clarify for clinicians the steps that need to be taken to protect the rights of their patients. It is hoped that the knock-on effect will be that the MHA 1983 is not relied on and will reduce overall detention rates. In the meantime, the immediate increase in applications has had a number of repercussions. The extra activity for health and care providers was significant: increases in the number of DoLS authorisations prepared and submitted, higher Court of Protection applications and local authority teams were required to respond to more requests to assess authorisations and where appropriate, authorise any deprivation of liberty. The significant increase in requests for authorisations, resulted in many local authorities left struggling to process these within the legal time limit.
For mental health patients, the repercussions of Cheshire West have also been keenly felt. The broader impact of the decision has reinforced a cautionary approach to be adopted by clinicians. Section 131 MHA allows the informal treatment of patients with their consent (this does not allow deprivation of liberty—HL v UK 45508/99). Looking at the data regarding informal patient numbers, a stark shift is evident following the Cheshire West decision. The number of informal patients in psychiatric facilities reduced while formal detentions increased. In 2008/09, there were 75,843 informal patients, while there were 30,913 formally detained patients. By 2014/15, the balance between these two categories of patient had shifted considerably, with 51,196 informal patients and 54,225 formal patients (Office for National Statistics 2015). This suggests that post-Cheshire West health and social care providers and decision-makers may be much more sensitive now to the risk of unauthorised deprivation of liberties and this has consequently had a knock-on effect upon formal detention rates.
The impact of ‘risk’ as a more nebulous construct has also been felt in recent years in the mental health care field (see, Hood et al. 2001). Historically, risk has always featured prominently in mental health care (Laing 2000). Following the MHA 2007, risk assessment and management have become the explicit concerns of the civil commitment process. It reflected policy-makers concerns that ‘the safety of both the individual patient and the public are of key importance in determining the question of whether compulsory powers should be imposed’ and that this was not sufficiently the focus of the mental health legislation prior to the 2007 Act amendments. For that reason, ‘concerns of risk [began to take]…precedence’ (HM Government 2000).
Mental health decision-makers must seek to achieve a balance between their patients’ personal freedoms, their health needs and the public’s safety. Risk provides a mechanism (albeit a problematic one) with which decision-makers may achieve this balance, by deploying the compulsory powers under the MHA when a patient’s level of risk becomes so great that he/she poses a threat to either him/herself or others. The standards which the compulsory criteria require are ambiguous. Decision-makers enjoy a wide discretion to interpret relevant factors according to their professional judgment. Sections 2(2)(b) and 3(2)(b) presume that decision-makers will assess a patient’s level of risk. Risk is an open-ended construct for decision-makers to assess and interpret according to their professional judgment and experience (Glover-Thomas 2011).
Rose argues that the language of risk seems ‘all-pervasive’ in contemporary mental health practice (Rose 1998). This is unsurprising: risk determines the nature, duration and extent of a patient’s engagement with the mental health services. Similarly, a patient’s risk profile determines the nature, duration and extent of his/her supervision in the community. Yet mental health decision-making has always entailed an element of risk assessment (Castel 1991). Successive legislative frameworks have reflected this practical reality, albeit in a fairly oblique manner. Consequently, a patient’s risk either to him/herself or others always plays a significant part in the decision to engage the civil commitment procedures (MHA Code of Practice, para. 4.6–4.7). While soft law, such as the Code of Practice and generic NHS Trust Clinical Risk Assessment Tools, provide some guidance, what constitutes a risk to a patient’s health or safety or to others is a matter for decision-makers alone. How reliable, valid and professionally rigorous risk assessments are remains open to question (Grann 2005). Bartlett contends that some decision-makers may find themselves operating in a system driven by personal experience with a fairly ad hoc system of interviewing and determination (Bartlett 2010; Langan and Lindow 2004).
Therefore, concerns around risk in terms of understanding what it is, how to assess it and manage it accurately and effectively remain a central feature of mental health care practice. Behavioural responses to this have also been shaped by external influences, of which the Cheshire West case is one. Two further cases involving the assessment of suicide risk have also had an impact upon risk and its management regarding clinical decision-making. In Savage v. South Essex Partnership NHS Foundation Trust ([2008] UKHL 74) failures to take reasonable precautions to protect the lives of patients with suicidal thoughts was found to have been violated under Article 2 ECHR. In Rabone v. Pennine Care NHS Foundation Trust ([2012] UKSC 2) the Court held that the operational duty (LCB v United Kingdom [1998] ECHR 108; Osman v United Kingdom (1998) 29 EHRR 245) to protect life could be owed to informal psychiatric patients as well as formally detained patients under the MHA 1983 (Allen 2013) as long as there has been ‘an assumption of responsibility by the State for the individual’s welfare and safety (including by the exercise of control)’ (Rabone v. Pennine Care NHS Foundation Trust, p. 22). The European Court also agreed that the duty could be owed to an informal patient (Reynolds v. United Kingdom (2012) 55 EHRR 35).
The practical impact of these cases is noteworthy. Health services must ensure high professional standards are met and effective systems of work are in place (Powell V United Kingdom (2000) 30 EHRR CD 362). The recognition of the operational duty to protect the life of a specific individual in cases of suicide risk where it is known or should have been known that there was a ‘real and immediate risk of suicide’ (Re: Officer L [2007] UKHL 36) has reinforced the obligation placed upon health care professionals. Given the acknowledged difficulty surrounding accurate risk assessment (Heilbrun 1997) an issue that was highlighted in Rabone, both Savage and Rabone present significant implications for public bodies who assume responsibility of vulnerable people.
The effect of Cheshire West, Savage and Rabone has led to greater sensitivity to risk and the potential repercussions should something go wrong. When there is doubt or uncertainty, it is now more likely the civil commitment provisions in the MHA 1983 will be seen as the best option and use of informal hospitalisation will be less attractive.
3.5. The Rise in Section 136 Use
Police in England and Wales are provided under Section 136 of the MHA 1983 with powers to remove a person to a place of safety or to keep a person in an existing place of safety where it is believed the person needs to be examined by a doctor and interviewed by an AMHP. Following the recent changes to Section 136 MHA 1983 by the Policing and Crime Act 2017, police powers now go beyond taking a person from a public place and can now be used anywhere that is not that person’s private home. Police are required to make an assessment of individuals who appear to be suffering from symptoms of mental illness. The purpose of any Section 136 assessment is to determine whether a person ought to be detained in hospital under the MHA.
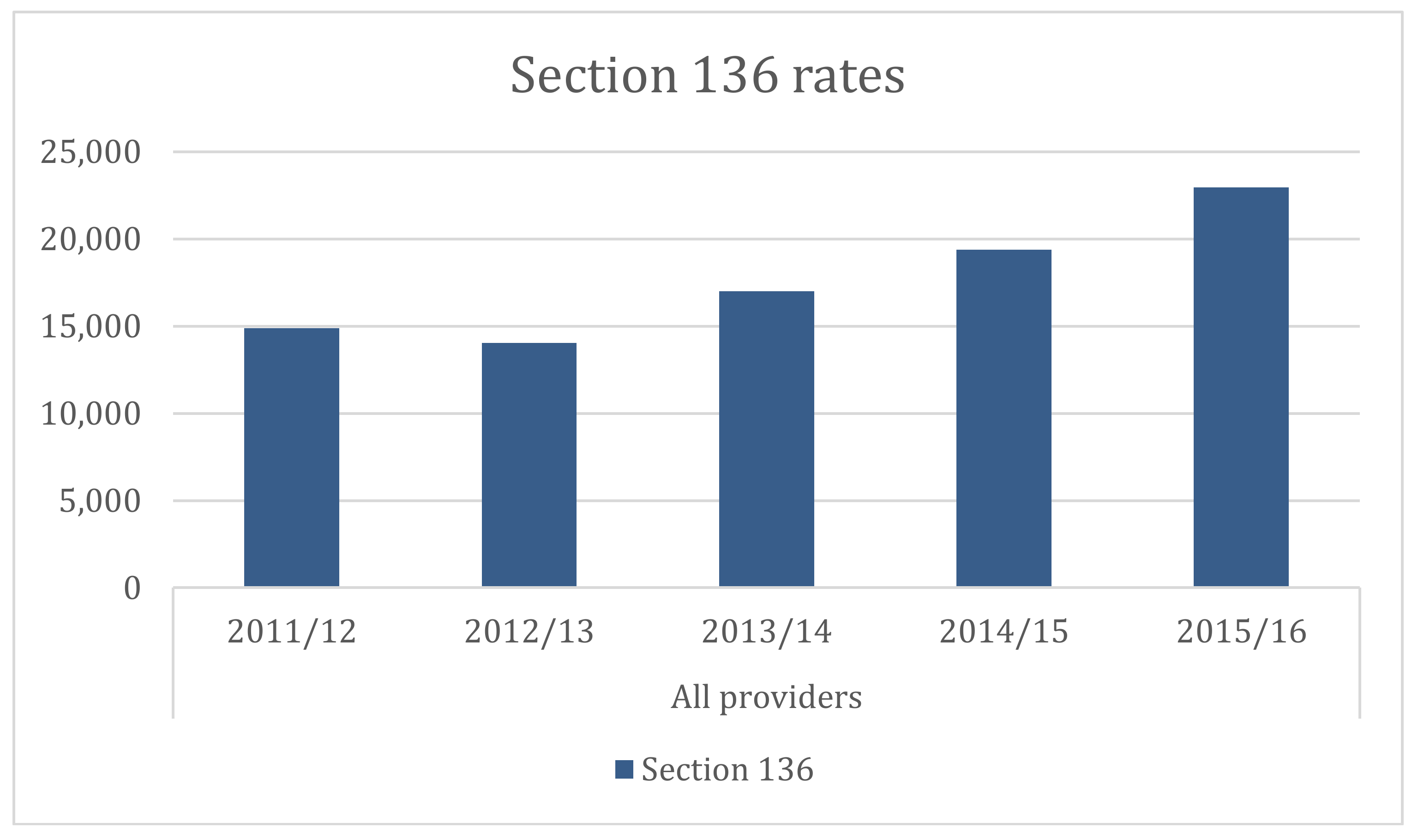
Although there is a presumption that use of the MHA should be a last resort, a shift in the use of Section 136 by the police is apparent, as denoted in Figure 6 below.
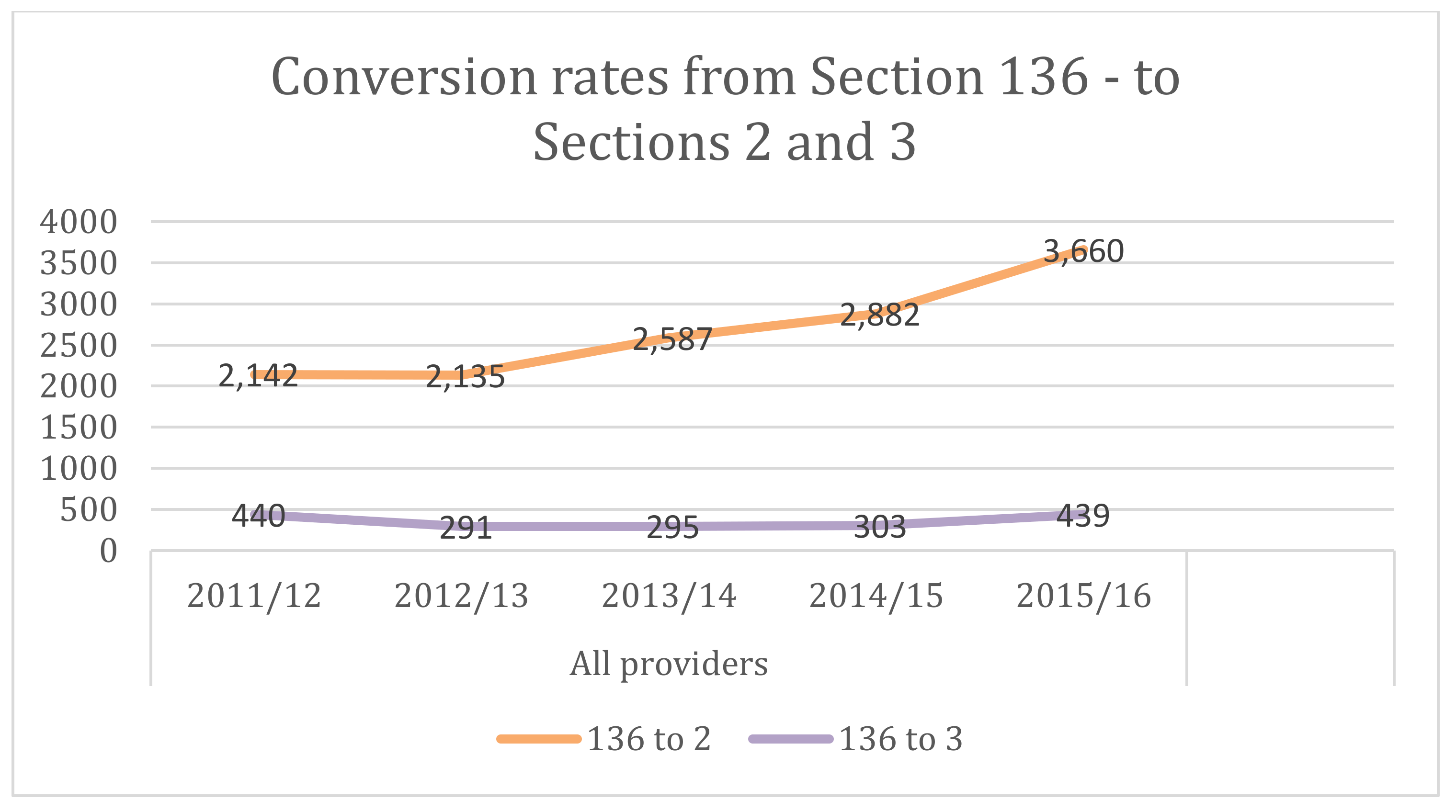
More notably, the shift in Section 136 reliance has impacted on conversion rates. With the presumption that Section 136 should only ever be used if no other avenues were available, conversion rates from Section 136 to Section 2 and Section 3 were once high. Since the early 2000s, conversion rates were in the region of 85% suggesting that the police were primarily putting people on a Section 136 who warranted informal admission to hospital. Individuals that were taken out of a public place by the police were highly likely to need mental health support. However, the Cheshire West decision has since discouraged use of the informal patient status under Section 131 and has had a knock-on effect upon Sections 2 and 3 figures. Since 2014, conversion rates from Section 136 to both Section 2 (29% increase since 2014) and Section 3 (32% increase since 2014) have risen. However, drawing a firm conclusion that the Cheshire West decision has had a marked and direct effect on conversion rates is difficult given the presence of multi-factorial drivers, though it has certainly played a significant role.
The data outlined in Figure 7 above suggests a number of things. First, the use of Section 136 has gone up as has the conversion rate from Section 136 to Sections 2 and 3. Therefore, there is a direct bearing upon overall detention figures and consequently tribunal receipts. Second, evidence suggest that revolving door patients are being identified by police and Section 136 is being used. Third, the Care Quality Commission’s concern that community-based services are becoming increasingly fragmented (Care Quality Commission 2015) with more gaps forming in service provision may be requiring greater input by the police. Finally, concerns around patients either not being able to access mental health services when they need it or being discharged too quickly because of overstretched acute care services, may be leading to more vulnerable people on the streets which the police are having to identify and support (Borschmann et al. 2010). This data provides a useful insight into the fragile nature of the contemporary mental health system in England and Wales and the impact of this on mental health tribunal activity.
3.6. Can Detention Rates Be Reduced?
Several things might relieve some of the pressure on the system. Reducing reliance on Section 2 would significantly free up the mental health care system and create space in the corresponding review process. As discussed above, several factors influence the heavy use of Section 2. Some of these factors, such as the rising use of Section 136, have arisen because of broader policy and funding changes to the mental health system and so are not easily fixed. Ensuring that Section 2 is used only for mental health assessment purposes would reduce the availability of the section for a considerable number of patients. Strengthening the MHA Code of Practice might be an initial way forward. Likewise, the practical demands placed on clinicians wishing to detain a patient under Section 3 could also be modified to enable access to care via Section 3 possible. Currently, it is necessary to identify inpatient facilities for patients to be detained under Section 3. Given tight budgets and fluid resources, it is not always possible to do this.
Clinicians often detain individuals under Section 2 to allow breathing space for inpatient beds to then be sourced. The impact of this is twofold. Patients are not placed on the appropriate care pathway that their condition demands, and the deployment of Section 2 instead of Section 3 instigates two review processes instead of one. The tribunal system is taken up by patients that would have been better served by appropriate sectioning in the first instance. However, problems around resources require more than one step system fixes.
While gaps remain elsewhere in the mental health and social care system, it is unlikely that a more literal interpretation of Section 2 admission criteria would necessarily help. Those not admitted under Section 2 (as they do not just require assessment) but for whom services are not available for them under Section 3, may simply find themselves picked up elsewhere in the system, such as under Section 136. Better communication, local joint protocols and joint working in terms of procurement and delivery between different agencies and stakeholders would be beneficial (Glover-Thomas and Barr 2008).
4. Mental Health Tribunal Caseloads
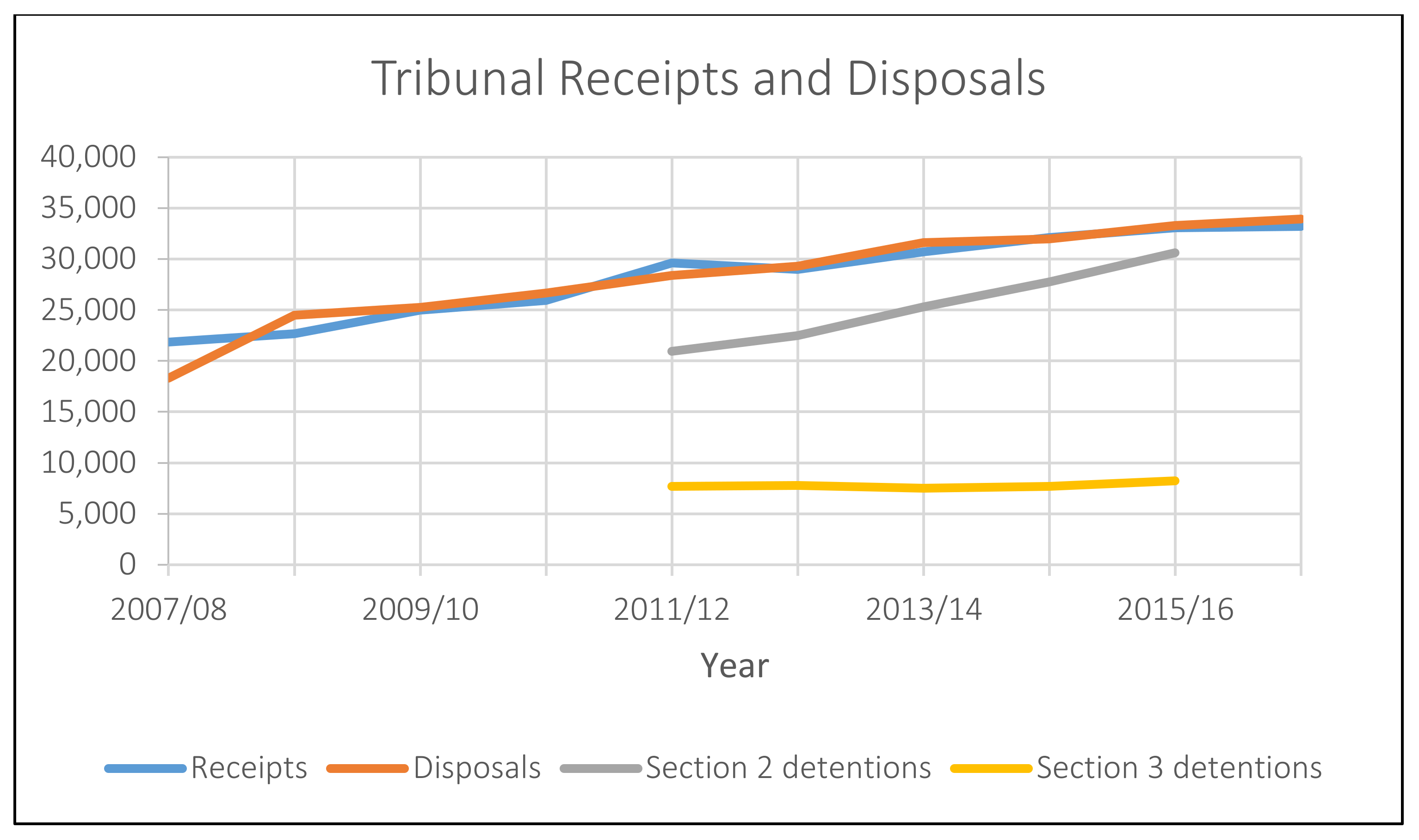
The upsurge in inpatient detention under the MHA 1983, has clear and direct implications for tribunal caseloads. Between 2007/8 and 2016/17, tribunal receipts (received applications by the tribunal) increased from nearly 22,000 to over 33,000 receipts—a rise of over 33% (Figure 8 below).
Section 2 cases have increased by around 32%, though this also reflects the rising volume of Section 2 detentions (a rise of nearly 32% between 2011/12 and 2015/16) (Care Quality Commission 2016, p. 51). Looking at data published by the Care Quality Commission, Section 2 related tribunal activity increased overall between 2014/15 and 2015/16. Section 2 applications increased from 9729 in 2014/15 to 10,093 in 2015/16, while hearings increased by over 7%. Section 2 discharges made by tribunals dropped by approximately 1.5% over the same period (Care Quality Commission 2015, p. 68).
Increased tribunal workloads present significant practical challenges. Section 2 review applications, in particular, have raised specific problems. Hearings must be listed within 7 days of application, and undertaken within 14 days of the date of admission. With the pressure on time and mounting demands to make effective and efficient decisions, the increasing number of Section 2 applications have meant that mental health tribunals have had to manage this while maintaining standards. Ensuring effective decision-making may be affected by the level of information, data and supporting documentation available at the hearing. The short timeframe to prepare a case may result in the quality and depth of the accompanying responsible authority reports being compromised (Practice Direction First-Tier Tribunal Health Education and Social Care Chamber Statements and Reports in Mental Health Cases 2013). There may have been insufficient time for the clinical team to be in a position where a judgement can be made about the patient’s current mental state. Treatment options may not have had enough time to provide an indicative picture of potential success. For many cases, writing a report about a patient for whom the clinical team still knows little will be difficult. Added to this is the often-chronic demands for reports to be produced quickly and at short notice. With insufficient information, projected treatment outcomes unknown and little time for the patient to settle, both the clinical team and tribunal panel are faced with a decision-making situation that is fraught with difficulty and necessarily encourages a cautious approach. For the tribunal system, increased caseloads also mean more judicial sittings and increased demand on limited judicial resources.
The increased use of detention powers by hospitals and increased tribunal caseloads has downstream cost implications especially for the Ministry of Justice. Normally, one would expect that an increased caseload would result in delays before tribunals. This has not occurred in the context of mental health tribunals, though adjournments remain a common feature. The timeliness of cases has remained relatively static and has shown improvement during the period in which caseloads have increased. In 2013, the average timeliness of cases was as follows: 1 week for Section 2 cases; 13 weeks for restricted patients; and 8 weeks for non-restricted patients (July 2013 Tribunal Statistics Quarterly). Restricted patients are those subject to special restrictions set out in Section 41 MHA 1983—leave under Section 17, transfer under Section 19, and discharge under Section 23 cannot take place without the consent of the Ministry of Justice; whereas decisions regarding non-restricted patients are not subject to Ministry of Justice oversight and approval. The additional restrictions associated with restricted patients necessarily add time to the review process. In 2017, the average timeliness was: 1 week for Section 2 cases; 12 weeks for restricted patients; and 6 weeks for non-restricted patients (July 2017 Tribunal Statistics Quarterly).
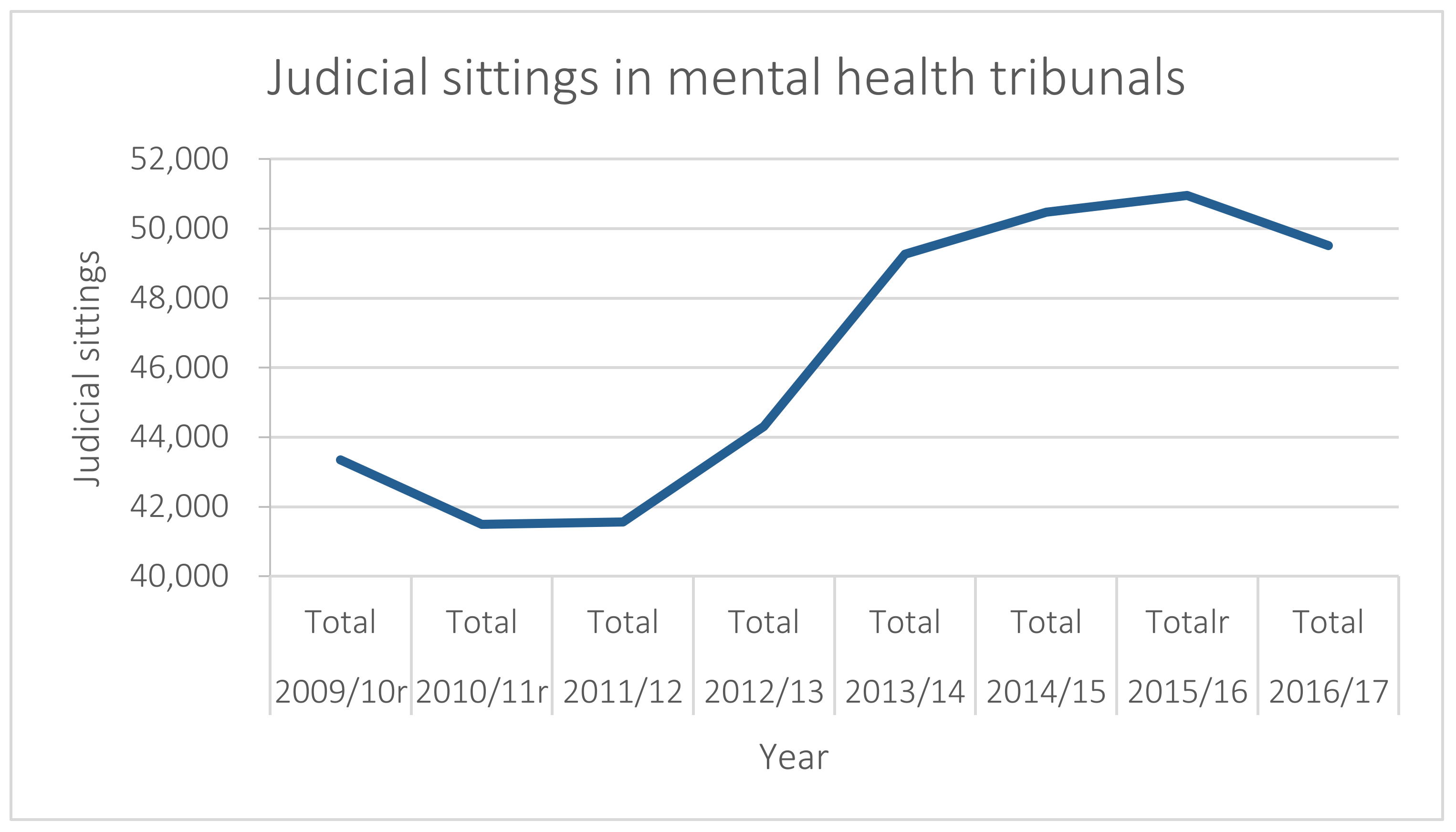
What has changed has been increased judicial sittings to cope with the caseload. As Figure 9 below demonstrates, the number of judicial sittings in mental health tribunals increased from 41,500 sittings in 2010/11 to 50,953 sittings in 2015/16. The increase in judicial sittings has been necessary to ensure that cases are heard and decided in a timely way. One consequence of increased judicial sittings is that the Ministry of Justice, as the responsible government department, will have borne the additional costs of such sittings.
4.1. The Patient Voice
A related challenge concerns the need to ensure that patients can have their voice heard. One of the key values that informs the work of tribunals is the use of fair procedures by which affected people can participate in decision-making. Achieving this in practice in the mental health context poses various difficulties. Nonetheless, despite the practical constraints mental health tribunals sometimes face, a 2011 report by the Care Quality Commission, Patients’ experiences of the First-tier Tribunal (Mental Health) (Care Quality Commission 2011), suggests that the tribunal process provides patients with a number of helpful opportunities. Importantly, patients can have their voice heard. Such an observation can be interpreted in a number of ways. The hearing provides an opportunity for the patient’s case to be reviewed and for them to speak about their experiences. On the other hand, the mental health care system should be able to offer a patient a voice throughout the experience. Patient collaboration is recognised as offering the most therapeutic approach to care in most clinical settings; better patient engagement is achieved through partnership and this requires patients to be fully involved in the process (Coulter and Jo 2007). For many patients, discharge from hospital may not be the goal, but a tribunal hearing provides a forum to scrutinise the patient’s progress, consider next steps and evaluate the patient’s continuing needs. Importantly, the tribunal hearing acts as a protective mechanism to safeguard the patient.
4.2. The Role of Independent Mental Health Advocacy
Following the introduction of Independent Mental Health Advocates (IMHAs) under the MHA 2007, access to some form of independent legal support and representation has been strong. The Care Quality Commission observed that most detained patients knew that they were entitled to legal support both in terms of providing legal advice and representing them during tribunal hearings (Care Quality Commission 2011). However, easily accessing support and high quality legal provision may not necessarily be a universal experience by patients, where many rely on hospital referrals for lawyers (WHO 2003). There is currently no research on this and it is an area which should be examined more closely. IMHAs, however, offer a valuable bridge between the patient, lawyers and the clinical environment (Newbigging et al. 2015). The lack of information regarding a patient’s detention status, their rights and the tribunal process has previously been recognised as a major concern (Care Quality Commission 2011). The use of independent advocacy may offer an effective response to this by increasing patient self-determination (Eades 2018) and providing a mechanism to support patients in presenting a more holistic picture of their current state of health (Freckleton 2003), though again, mapping IMHA presence nationally would be a valuable step. The role of an advocate is to act as a conduit for patients to enable them to promote their own voices (Ridley et al. 2015) express their wishes and to facilitate participation (Henderson and Pochin 2001). However, despite the valuable contributions made by IMHAs, practical limitations remain (Department of Health 2012). Difficulties with funding continuity experienced by many different organisations providing independent advocacy services prevent individual advocates from building rapport with patients over the longer term. The benefits of advocacy require sufficient time and certainty to enable trust and confidence to flourish.
4.3. Mental Health Tribunal Delays
Although increased tribunals sittings have been implemented to respond to increasing tribunal caseloads, patients still experience delays. Despite the valuable role of the mental health tribunal, some significant system problems exist which negatively impact on the patient experience. Delays which are often a result of adjournment are particularly problematic. Where some detained patients must be seen quickly, for example, Section 2 patients, others are forced to wait creating further bottlenecks. Delays in the process contribute to many negative patient experiences, leading to additional distress and anxiety. This is not a new problem, though it has been exacerbated by the rise in detention rates across the various commitment provisions in the MHA 1983 (Blumenthal and Wessely 1994). In 2002, it was found in the case of R v Mental Health Review Tribunal and Secretary of State for Health, ex parte KB and 6 Others ([2002] EWHC 639 (Admin)) that delays in mental health tribunal hearings breached patient rights to timely reviews under Article 5 ECHR. In this case, the individuals concerned had all experienced repeated adjournments. The strain on the mental health tribunal system around this time emerged following policy shifts around funding patterns and practice changes. Patients were being placed in smaller units rather than large hospitals and this had had a knock-on effect in terms of the number of tribunals that needed to convene and the frequency in which they met. At the time of this case, shortages in consultant psychiatrists sitting on tribunal panels was noted as a factor that influenced the opportunities to arrange tribunal hearings. Although the practical challenges facing the tribunal system at the time were acknowledged, delays were deemed unjustified and detrimental to the patient. Delays were found to breach Article 5(4) of the ECHR. The delays reflected systemic inadequacies and inefficiencies in the administration of the tribunal system. Furthermore, patients were being denied their absolute right to a speedy hearing which the state was obliged to provide. In an effort to reduce delays and counter the effect of rising caseloads, judicial sittings have risen to cope with the increased demand but to ensure cases are heard quickly and in a timely fashion, tribunal costs have and continue to go up.
4.4. Other Challenges
Other challenges with the hearing process exist which can impact negatively upon both the patient experience and the efficiency of the tribunal system. For example, the pre-hearing medical examination has been subject to some discussion over its value, the process and its independence. Details of the pre-hearing medical examination of the patient is laid down in rule 34 of the Tribunal Procedure Rules (The Tribunal Procedure Rules 2008). The medical member of the tribunal panel will conduct a pre-hearing examination of the patient in all Section 2 cases, unless the patient objects and share findings with the other panel members before the hearing. For other patients, the examination will take place if the tribunal is informed 14 days before and in writing that an examination is desired or the tribunal has directed that there should be an examination. Medical examinations should normally occur where a patient fails to attend the hearing. For patients that have had a pre-hearing medical examination, the experience has not always been helpful. Raised levels of anxiety and fear are quite common. The MHA 1983 Code of Practice notes that ‘[h]ospital managers must ensure that the medical examiner can see patients who are in hospital in private, where this is safe and practicable’ (Department of Health 2015, para. 12.23). Yet, examinations are sometimes rushed, not always carried out in private and often inconsistently undertaken with different approaches and emphases being used by different medical panel members. Questions have been raised regarding the value of the examination, given the recognised limits of the process, and the influence of it on the hearing outcome (for example, Wexler 1992; Winick 1997).
Tensions and constraints face mental health tribunals in daily practice. The rise in tribunal caseload has resulted in a form of ‘crisis management’. Despite these practical challenges, the value of the tribunal process for patients is recognised; a benefit that patients particularly gain from when hearings are well organised and directed effectively by panel members. The inextricable link between the entry of patients into the mental health system and tribunal caseload is clear. There is no ‘quick fix’ approach to reducing tribunal caseload, but instead relies upon a multi-agency approach to accommodate the complexity of the problem.
5. Next Steps for Mental Health Tribunals
The Ministry of Justice’s Transforming Justice paper (Ministry of Justice 2016) sets out a far-reaching plan for court reform with technology and innovation as its heart. Although mental health tribunals are not currently the focus of this reform programme, the paper notes that there is ‘potential to extend…[these proposals to]…other areas such as Mental Health’ (Ministry of Justice 2016, p. 15). The expectation is that use of technology will improve access to justice, providing tools to help people understand what their rights are and how to protect them. Beside this, robust case management systems are to be put in place with the intention of improving efficiency. Ambitious plans such as these hold the key to significant gains in system management, however, it is recognised elsewhere that challenges are also possible (Thomas and Tomlinson 2016).
Scope for technology in the mental health tribunal system is evident and may have a valuable impact in overcoming some of the practical difficulties experienced by panels and patients on a regular basis. For patients, with the help of legal representatives and/or IMHAs, online support could improve patient experiences. One of the concerns noted by the Care Quality Commission (Care Quality Commission 2011) was that patients did not always have the information they needed both in terms of how the detention process worked, what their rights were and how they could initiate the review process. The introduction of IMHAs has made considerable inroads into responding to this concern; access to online support would be valuable and would reinforce the position of the patient within the relationship. Use of technology could also greatly assist in the evidence gathering process, the hearing itself and follow-up.
Despite the benefits that may come from greater use of technology, there is a need to be mindful of the particular vulnerability of individuals being formally detained and being seen by mental health tribunals. There is a clear tension between the focus on efficiency and ensuring legal safeguards and protections are maintained. There is recognition among mental health tribunal judges in the UK that greater use of technology could offer a sensible avenue for overcoming difficulties, whether in relation to evidence collation or assisting with a patient’s active presence within a hearing. However, resort to technology, such as video-link or Skype usage for hearings, remains anecdotal with currently no research available to demonstrate the level of use and reliance on technology, its value or the challenges technology poses in this context. This issue is particularly evident when examining the question of whether cases should be decided after an oral hearing or solely on the papers. Studies examining other tribunals systems have considered the debate (Thomas 2017). Oral hearings offer the tribunal the benefit of meeting the patient. In addition to the medical reports and other paper evidence supplied as part of the hearing process, the tribunal panel have an opportunity to hear direct evidence given by the patient themselves. The informal and inquisitorial nature of the tribunal also enables the panel to ask questions and assist the patient allowing evidence to be drawn out from the patient that might be important. Indeed, mental health tribunal proceedings are often likened to a case review (Perkins 2003b). Hearing a case on the papers loses much of this exchange. A tribunal will only be able to base a decision on the paper evidence submitted and there will be no opportunity to interrogate this evidence further. Within mental health, paper hearings without the patient present do take place. For example, in 2016/17, out of 4645 applications against CTOs, 520 of those were undertaken on the papers only. Taking account of the withdrawn applications, this figure represents nearly 14% of the hearings undertaken during this period (Tribunal Secretariat 2016/17). Paper hearings do aid timeliness and assist with the goal of driving up efficiency. However, as Thomas observes, oral appeals are more commonly allowed compared to those heard on the papers. ‘Looking at these data, it is apparent that appellants who opt for oral appeals experience higher success rates than those appellants whose appeals are determined on the papers’ (Thomas 2017).
In order to respond to the challenge of increasing mental health tribunal caseloads, it is important to ensure reforms are informed by evidence. More research, consultation and use of pilots are essential. Building on the research undertaken by the Care Quality Commission on patient experience of the tribunal system would also be valuable. Detailed mapping and evaluation of the role and impact of IMHAs to date and the potential expansion of the role as a bridge between the care and legal system would also offer significant insight.
Improving efficiency within the mental health tribunal system is not an easy task. This is largely because the tribunal system cannot be viewed separately. Tribunal caseloads are directly linked to initial decisions to detain under the MHA 1983. Mental health tribunals review all cases whereas in other tribunal contexts, such as immigration and social security, the appellant must decide whether or not to appeal. While detention rates (under all relevant provisions) are high and getting higher, the impact will be felt by mental health tribunals. Looking forward, it is important to understand better why greater reliance is being placed upon the MHA, and what, if anything can be done to resolve this. Undertaking empirical research into this is essential.
Acknowledgments
The research underpinning this article was facilitated with a Research Support Grant from the University of Manchester and financial and administrative support from the UK Administrative Justice Institute.
Conflicts of Interest
The authors declare no conflict of interest.
References and Notes
- Allen, Neil. 2013. The right to life in a suicidal state. International Journal of Law and Psychiatry 36: 350–57. [Google Scholar] [CrossRef] [PubMed]
- Allmark, Peter, Baxter Susan, Goyder Elizabeth, Guillaume Louise, and Crofton-Martin Gerard. 2013. Assessing the health benefits of advice services: Using research evidence and logic model methods to explore complex pathways. Health & Social Care in the Community 21: 59–68. [Google Scholar]
- Bartlett, Peter. 2010. Civil Confinement. In Principles of Mental Health Law. Edited by Jean McHale and Judy Laing. Oxford: OUP. [Google Scholar]
- Bartlett, Peter, Thorold Oliver, and Lewis Oliver. 2007. Mental Disability and the European Convention on Human Rights. Leiden: Martinus Nijhoff. [Google Scholar]
- Blumenthal, Stephen, and Simon Wessely. 1994. The pattern of delays in Mental Health Review Tribunals. Psychiatric Bulletin 18: 398–400. [Google Scholar] [CrossRef]
- Borschmann, Rohan D., Steven Gillard, Kati Turner, Mary Chambers, and Ann O’Brien. 2010. Section 136 of the Mental Health Act: A new literature review. Medicine, Science and the Law 50: 34–39. [Google Scholar] [CrossRef] [PubMed]
- Burns, Tom, Rugkasa Jorun, and Molodynshi Andrew. 2008. The Oxford Community Treatment Order Evaluation Trial (OCTET). Royal College of Psychiatrists 32: 400. [Google Scholar] [CrossRef]
- Care Quality Commission. 2011. Patients’ Experiences of the First-Tier Tribunal (Mental Health) Report of a Joint Pilot Project of the Administrative Justice and Tribunals Council and the Care Quality Commission. London: CQC. [Google Scholar]
- Care Quality Commission. 2015. Right Here Right Now: People’s Experiences of Help, Care and Support during a Mental Health Crisis. London: CQC. [Google Scholar]
- Care Quality Commission. 2016. Monitoring the Mental Health Act in 2015/16. London: CQC. [Google Scholar]
- Castel, Robert. 1991. From Dangerousness to Risk. In The Foucault Effect: Studies in Governmentality. Edited by Burchell Graham, Gordon Colin and Miller Peter. Chicago: The University of Chicago Press. [Google Scholar]
- Coulter, Angela, and Ellins Jo. 2007. Effectiveness of strategies for informing, educating, and involving patients. British Medical Journal 335: 24–27. [Google Scholar] [CrossRef] [PubMed]
- Dawson, John. 2005. Community Treatment Orders: International Comparisons. Dunedin: Otago University Print. [Google Scholar]
- Dawson, John. 2010. Supervised Community Treatment Orders. In Principles of Mental Health Law and Policy. Edited by Jean McHale and Judy Laing. Oxford: OUP. [Google Scholar]
- Department of Constitutional Affairs. 2004. Transforming Public Services: Complaints, Redress and Tribunals; Cmnd.6243; London: TSO.
- Department of Health. 1982. White Paper on Reform of Mental Health Legislation; London: TSO, Cmnd 8405.
- Department of Health. 2011. No Health without Mental Health: A Cross-Government Mental Health Outcomes Strategy for People of All Age; London: HM Government/Department of Health.
- Department of Health. 2012. Post-Legislative Assessment of the Mental Health Act 2007: Memorandum to the Health Committee of the House of Commons; London: TSO, Cm 8408.
- Department of Health. 2015. Mental Health Act Code of Practice; London: Department of Health.
- Department of Health, and Social Care. 2013. Section 67 of the Mental Health Act 1983 References by the Secretary of State for Health to the First-tier Tribunal; London: TSO.
- Dineage, Caroline. 2018. Final Government Response to the Law Commission’s Review of Deprivation of Liberty Safeguards and Mental Capacity; Written Ministerial Statement, HCWS542; London: Houses of Parliament, March 14.
- Eades, Susan. 2018. Impact evaluation of an Independent Mental Health Advocacy (IMHA) service in a high secure hospital: A co-produced survey measuring self-reported changes to patient self-determination. Mental Health and Social Inclusion 22: 53–60. [Google Scholar] [CrossRef]
- Firn, Mike, Keelyjo Hindhaugh, Dieneke Hubbeling, Gwyn Davies, Ben Jones, and Sarah White. 2013. A dismantling study of assertive outreach services: Comparing activity and outcomes following replacement with the FACT model. Social Psychiatry and Psychiatric Epidemiology 48: 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Freckleton, Ian. 2003. Mental Health Review Tribunal Decision-making: A Therapeutic Jurisprudence Lens. Psychiatry, Psychology and Law 10: 44–62. [Google Scholar] [CrossRef]
- Freeman, Melvin, Kolappa Kavitha, Caldas de Almeida Jose Miguel, Kleinman Arthur, Makhashvili Nino, Phakathi Sifiso, Saraceno Benedetto, and Thornicroft Graham. 2015. Reversing hard won victories in the name of human rights: A critique of the General Comment on Article 12 of the UN Convention on the Rights of Persons with Disabilities. Lancet Psychiatry 2: 844–50. [Google Scholar] [CrossRef]
- Glover, Nicola. 1999. Mental health and housing: A crisis on the streets? Journal of Social Welfare and Family Law 21: 327–37. [Google Scholar] [CrossRef]
- Glover-Thomas, Nicola. 2011. The Age of Risk: Risk Perception and Determination following the Mental Health Act 2007. Medical Law Review 19: 581–605. [Google Scholar] [CrossRef] [PubMed]
- Glover-Thomas, Nicola. 2013. The Health and Social Care Act 2012: The emergence of equal treatment for mental health care or another false dawn? Medical Law International 13: 279–97. [Google Scholar] [CrossRef] [PubMed]
- Glover-Thomas, Nicola, and Warren Barr. 2008. Re-examining the Benefits of Charitable Involvement in Housing the Mentally Vulnerable. Northern Ireland Legal Quarterly 59: 177–200. [Google Scholar]
- Grann, Martin. 2005. Psychiatric Risk Assessment Methods: Are Violent Acts Predictable? A Systematic Review (Summary and Conclusions); SBU Report No 175; Stockholm: Swedish Council on Health Technology Assessment.
- Heilbrun, Kirk. 1997. Prediction Versus Management Models Relevant to Risk Assessment: The Importance of Legal Decision-Making Context. Law and Human Behavior 21: 347–59. [Google Scholar] [CrossRef] [PubMed]
- Henderson, Rick, and Mike Pochin. 2001. A Right Result? Advocacy, Justice and Empowerment. Bristol: The Policy Press. [Google Scholar]
- HM Courts, and Tribunals Service. 2012. First-Tier Tribunal Health, Education and Social Care Chamber Mental Health jurisdiction: Room Specification Recommendations for Tribunal Hearings; London: TSO.
- HM Courts, and Tribunals Service. 2013. Practice Direction First-Tier Tribunal Health Education and Social Care Chamber Statements and Reports in HMCTS. Mental Health Cases; London: HMCTS. Available online: https://www.judiciary.gov.uk/publications/practice-direction-first-tier-tribunal-health-education-and-social-care-chamber-statements-and-reports-in-mental-health-cases/ (accessed on 5 February 2018).
- HM Government. 2000. Reforming the Mental Health Act: Part I: The New Legal Framework; London: TSO, Cm 5016-I.
- HM Treasury. 2011. Budget; London: TSO.
- HM Treasury. 2017. Autumn Budget 2017 NHS Spending. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/661432/NHS_spending.pdf (accessed on 12 February 2018).
- HL v UK 45508/99.
- Hood, Christopher, Rothstein Henry, and Baldwin Robert. 2001. The Government of Risk Understanding Risk Regulation Regimes. Oxford: OUP. [Google Scholar]
- Johnson v UK (1997) 27 EHRR 296.
- Johnson, Sarah. 2016. The cost of mental illness. The Guardian, May 17. [Google Scholar]
- K v Craig [1998] UKHL 54.
- L v Sweden (App No 1080/84).
- Laing, Judy. 2000. Rights versus Risk? Reform of the Mental Health Act 1983. Medical Law Review 8: 210–50. [Google Scholar] [CrossRef] [PubMed]
- Langan, Joan, and Vivien Lindow. 2004. Living with Risk: Mental Health Service-User Involvement in Risk Assessment and Management. York: Joseph Rowntree Foundation. [Google Scholar]
- Law Commission. 2017. Mental Capacity and Deprivation of Liberty (Law Com No 372); London: TSO.
- Leggatt, Andrew. 2001. Tribunals for Users: One System, One Service. London: TSO. [Google Scholar]
- Lintern, Shaun. 2012. Mental health charity funding falls as demand grows. Health Service Journal, May 31. [Google Scholar]
- Lintern, Shaun. 2014. Analysis reveals mental health trust funding cuts. Health Service Journal, August 14. [Google Scholar]
- McCrone, Paul, Dhanasiri S. Sujith, Patel Anita, Knapp Martin, and Lawton-Smith Simon. 2008. Paying the Price: The Cost of Mental Health Care in England to 2016. London: The King’s Fund. [Google Scholar]
- McNicoll, Andy. 2014. Rise in mental health patients sent out-of-area for beds. Community Care, May 6. [Google Scholar]
- McNicoll, Andy. 2015. Mental health trust funding down 8% from 2010 despite coalition’s drive for parity of esteem. Community Care, March 20. [Google Scholar]
- Ministry of Justice. 2016. Transforming Our Justice System by the Lord Chancellor, the Lord Chief Justice and the Senior President of Tribunals; London: TSO.
- Ministry of Justice. 2017. Tribunals and Gender Recognition Certificate Statistics Quarterly—July to September 2017; London: Ministry of Justice.
- Minkowitz, Tina. 2007. The United Nationals Convention of the Rights of Persons with Disabilities and the Right to Be Free from Nonconsensual Psychiatric Interventions. Syracuse Journal of International Law and Commerce 34: 405–28. [Google Scholar]
- Mulcahy, Linda. 2011. Legal Architecture. Oxford: Routledge. [Google Scholar]
- Newbigging, Karen, Julie Ridley, Mick Mckeown, Karen Machin, and Konstantina Poursanidou. 2015. When you haven’t got much of a voice’: An evaluation of the quality of Independent Mental Health Advocate (IMHA) services in England. Health and Social Care in the Community 23: 313–24. [Google Scholar] [CrossRef] [PubMed]
- NHS Digital. 2011. Inpatients Formally Detained in Hospitals Under the Mental Health Act 1983 and Patients Subject to Supervised Community Treatment—England, 2010–2011, Annual figures. London: TSO. [Google Scholar]
- NHS Digital. 2017. Out of Area Placements in Mental Health Services Data Quality Statement 2017. London: TSO. [Google Scholar]
- P v Cheshire West and Chester Council; P & Q v Surrey County Council [2014] UKSC 19.
- Peay, Jill. 1989. Tribunals on Trial: A Study of Decision-Making under the Mental Health Act 1983. Gloucestershire: Clarendon Press. [Google Scholar]
- Perkins, Elizabeth. 2003. Decision-Making in Mental Health Review Tribunals. London: Policy Studies Institute. [Google Scholar]
- Perkins, Elizabeth. 2003. A New Tribunal? Psychiatry Psychology and Law 10: 113–21. [Google Scholar] [CrossRef]
- Powell V United Kingdom (2000) 30 EHRR CD 362.
- Practice Direction First-Tier Tribunal Health Education and Social Care Chamber Statements and Reports in Mental Health Cases; 2013 October. Available online: https://www.judiciary.gov.uk/publications/practice-direction-first-tier-tribunal-health-education-and-social-care-chamber-statements-and-reports-in-mental-health-cases/ (accessed on 2 February 2018).
- R v Hallstrom, ex p W [1985] 3 All E R 775.
- R v Mental Health Review Tribunal and Secretary of State for Health, ex parte KB and 6 Others [2002] EWHC 639 (Admin).
- R v. Wilson, ex parte Williamson [1996], COD 42.
- Rabone v. Pennine Care NHS Foundation Trust [2012] UKSC 2.
- Re: Officer L [2007] UKHL 36.
- Reynolds v. United Kingdom (2012) 55 EHRR 35.
- Richardson, Genevra. 2008. Coercion and Human Rights: A European Perspective. Journal of Mental Health 17: 245–54. [Google Scholar] [CrossRef]
- Ridley, Julie, Karen Newbigging, Mick McKeown, June Sadd, Karen Machin, Kaaren Cruse, Stephanie De La Haye, Laura Able, and Konstantina Poursanidou. 2015. Independent Mental Health Advocacy—The Right to Be Heard: Context, Values and Good Practice. London: Jessica Kingsley Publishers. [Google Scholar]
- Romans, Sarah, Dawson John, Mullen Richard, and Gibbs Anita. 2004. How Mental Health Clinicians View Community Treatment Orders: A National New Zealand Survey. ANZ Journal of Psychiatry 38: 836–41. [Google Scholar] [CrossRef] [PubMed]
- Rose, Nikolas. 1998. Governing Risky Individuals: The Role of Psychiatry in New Regimes of Control. Psychiatry, Psychology and Law 5: 177–95. [Google Scholar] [CrossRef]
- Rugkåsa, Jorun, Molodynski Andrew, Yeeles Ksenija, Montes M. Vazquez, and Visser Claire. 2015. Community treatment orders: Clinical and social outcomes, and a subgroup analysis from the OCTET RCT. Acta Psychiatrica Scandinavica 131: 321–29. [Google Scholar] [CrossRef] [PubMed]
- Savage v. South Essex Partnership NHS Foundation Trust [2008] UKHL 74.
- Swanson, Jeffrey, Linda K. George, Barbara J. Burns, Randy Borum, Virginia Aldige Hiday, and Wagner H. Ryan. 1997. Interpreting the Effectiveness of Outpatient Commitment: A Conceptual Model. Journal of American Ac Psychiatry and Law 25: 5–16. [Google Scholar]
- Szmukler, George, Rowena Daw, and John Dawson. 2010. A model law fusing incapacity and mental health legislation. Special Issue. Journal of Mental Health Law, 9–22. [Google Scholar] [CrossRef]
- Szmukler, George, Rowena Daw, and Felicity Callard. 2014. Mental health law and the UN Convention on the Rights of Persons with Disabilities. International Journal of Law and Psychiatry 37: 245–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Franks Report. 1959. Report of the Committee on Administrative Tribunals and Enquiries. London: TSO, Cmnd: 218. [Google Scholar]
- The King’s Fund. 2015. Briefing—Mental Health under Pressure. London: The King’s Fund. [Google Scholar]
- The Mental Health Taskforce. 2016. The Five Year Forward View for Mental Health a Report from the Independent Mental Health Taskforce to the NHS in England. London: TSO. [Google Scholar]
- The Tribunal Procedure Rules. 2008. The Tribunal Procedure (First-tier Tribunal) (Health, Education and Social Care Chamber) Rules 2008. (2008 No. 2699 (L. 16) PART 4 CHAPTER 1 Rule 34; London: Ministry of Justice.
- Thomas, Robert. 2017. Oral and paper tribunal appeals, and the online future. London: UKAJI. [Google Scholar]
- Thomas, Robert, and Joe Tomlinson. 2016. New ESRC Report Launched: Current Issues in Administrative Justice: Examining Administrative Review, Better Initial Decisions, and Tribunal Reform. London: UKAJI. [Google Scholar]
- United Nations Committee on the Rights of Persons with Disabilities. 2014. General Comment No 1: Article 12: Equal Recognition before the Law. Geneva: OHCHR, (CRPD/C/GC/1). [Google Scholar]
- Wexler, David. 1992. Justice, mental health, and therapeutic jurisprudence. Cleveland State Law Review 40: 517–26. [Google Scholar]
- WHO. 2003. Advocacy for Mental Health. Geneva: World Health Organization. [Google Scholar]
- Winick, Brian. 1997. Coercion and mental health treatment. Denver University Law Review 74: 1145–68. [Google Scholar] [PubMed]
- Winterwerp v The Netherlands (1979) ECHR 4.
Figure 1.
This chart shows the total number of applications to the mental health tribunal in England; the total number of detentions upheld by the tribunal; the total number of hearings and total patient discharges before the tribunal hearing between 2010 and 2017. Source: Tribunal Secretariat, 2017.
Figure 1.
This chart shows the total number of applications to the mental health tribunal in England; the total number of detentions upheld by the tribunal; the total number of hearings and total patient discharges before the tribunal hearing between 2010 and 2017. Source: Tribunal Secretariat, 2017.
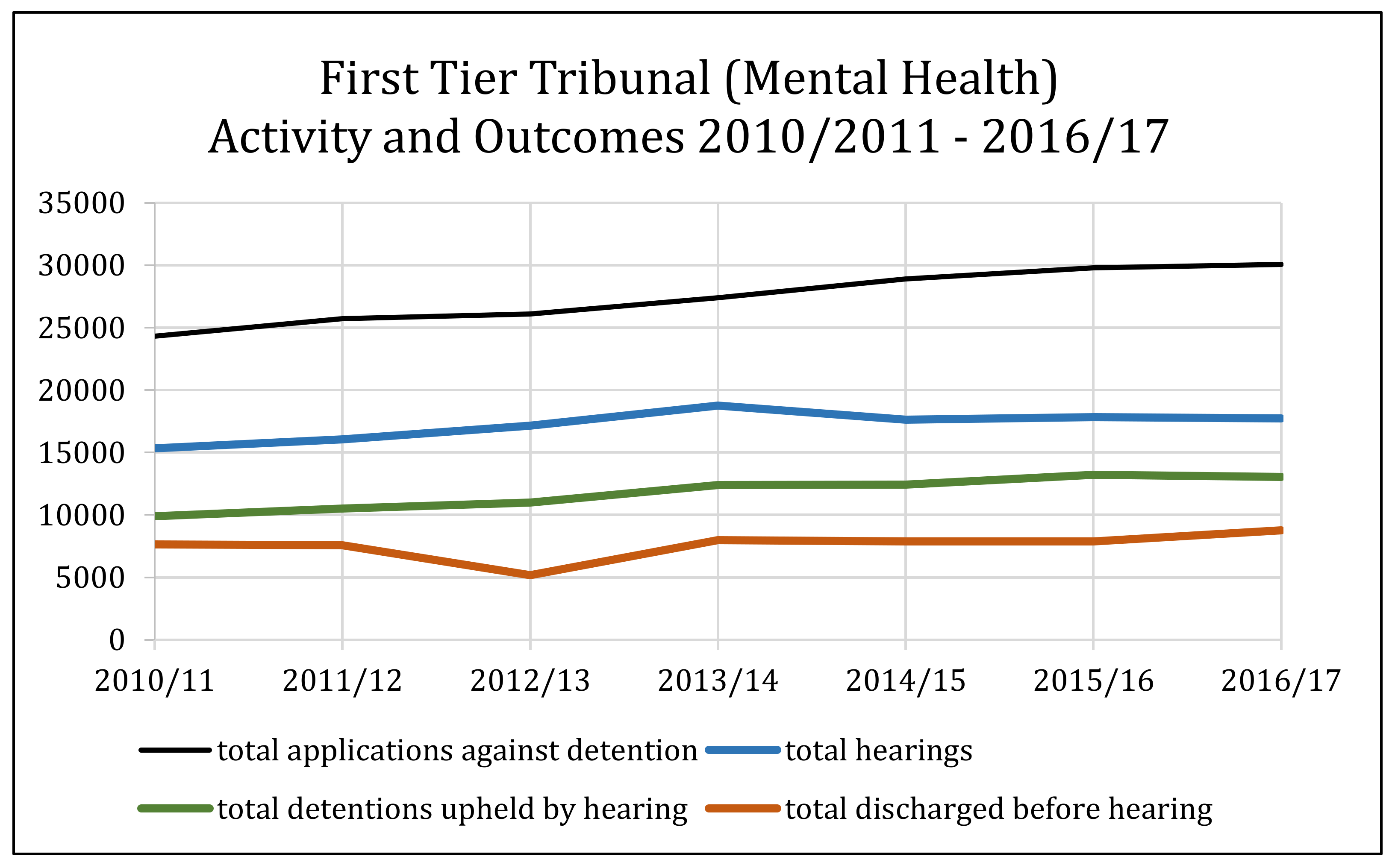
Figure 2.
This chart shows the overall number of all detentions under the Mental Health Act 1983 in England and Wales from 2011–2016. Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
Figure 2.
This chart shows the overall number of all detentions under the Mental Health Act 1983 in England and Wales from 2011–2016. Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
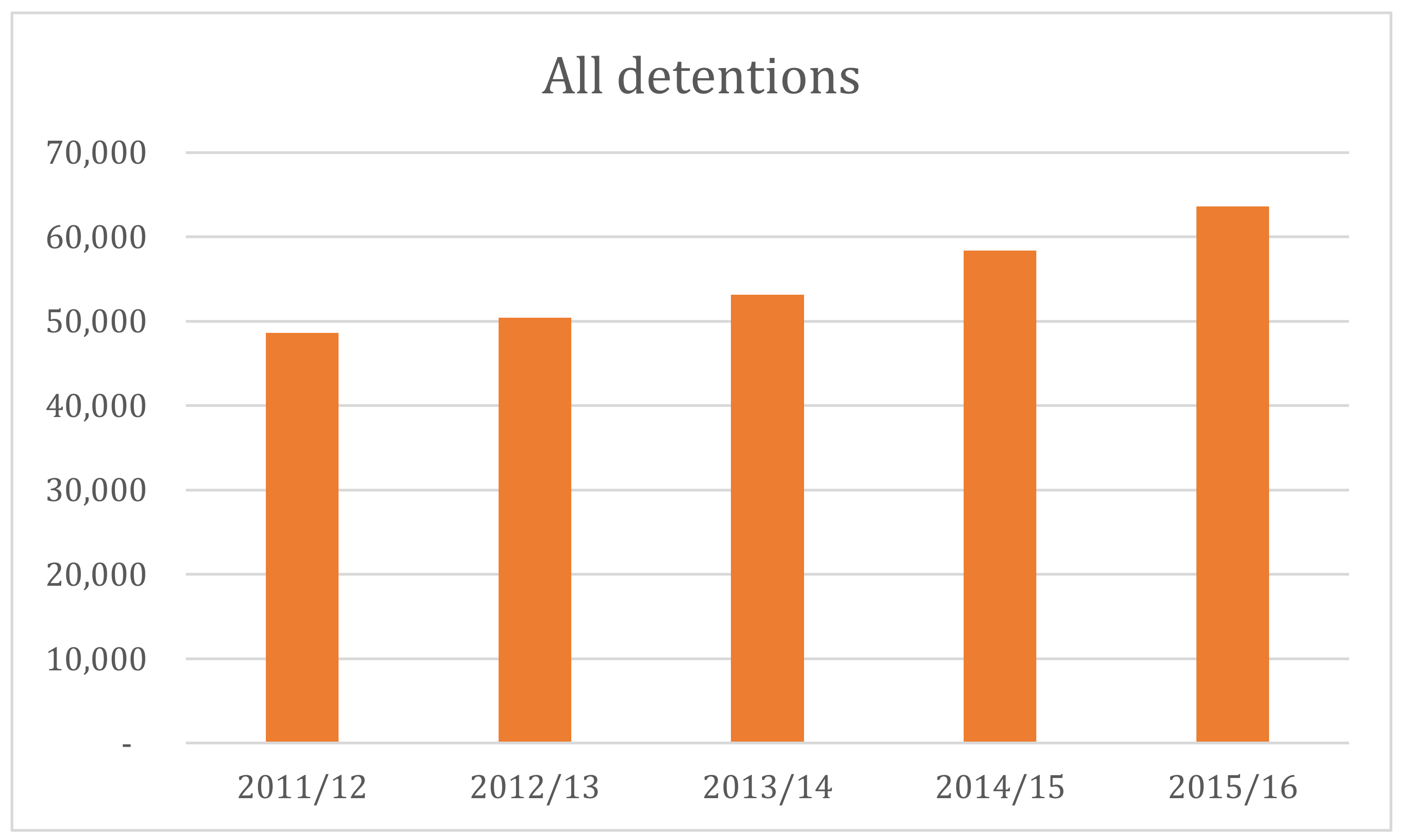
Figure 3.
This chart shows all detentions under Part II of the Mental Health Act 1983 between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
Figure 3.
This chart shows all detentions under Part II of the Mental Health Act 1983 between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
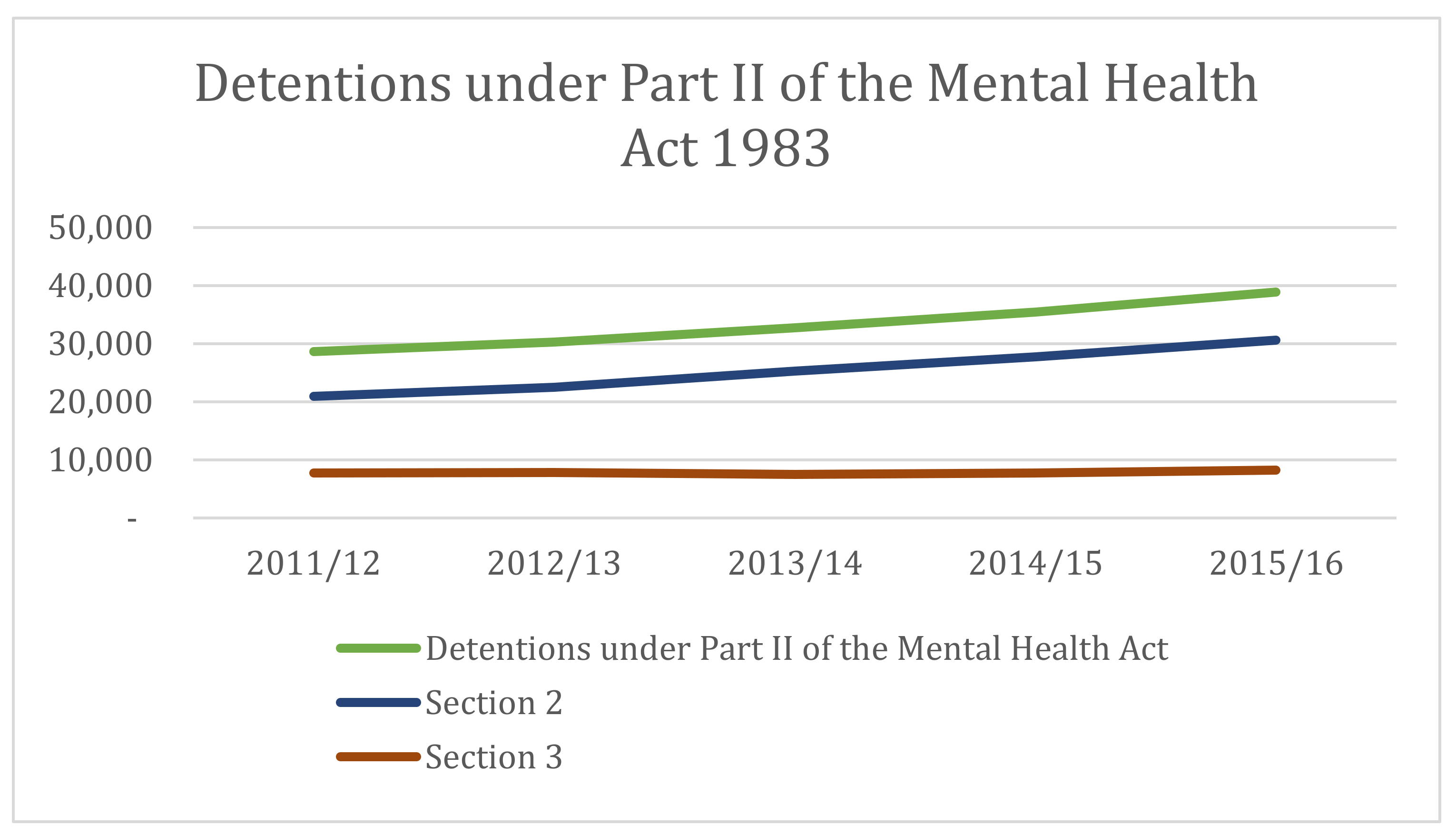
Figure 4.
This chart shows the number of overnight beds for mental illness across England between 2010 and 2018. Source: NHS England, Average Daily Available and Occupied Beds Timeseries 2010/11—2017/18, NHS England: Unify2 data collection—KH03, November 23 2017.
Figure 4.
This chart shows the number of overnight beds for mental illness across England between 2010 and 2018. Source: NHS England, Average Daily Available and Occupied Beds Timeseries 2010/11—2017/18, NHS England: Unify2 data collection—KH03, November 23 2017.
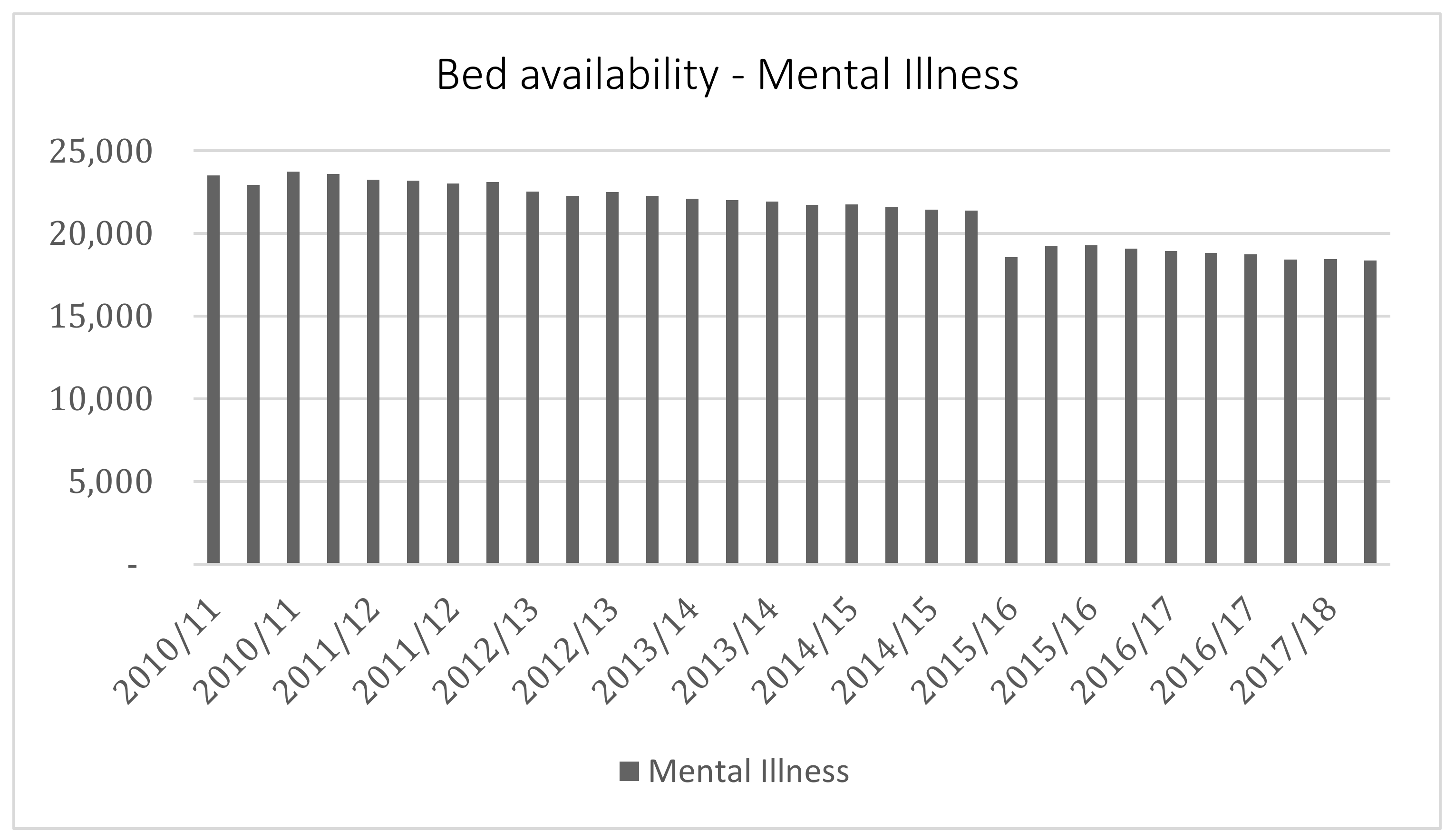
Figure 5.
This chart shows the rates of detention under the Mental Health Act 1983 for different ethnic groups, with the red line on the secondary axis representing a percentage of the total between 2016 and 2017. Sources: Rates of detention (per 100,000) under the MHA 1983 by specific ethnic group in England 2016/17, Mental Health Services Dataset at: http://content.digital.nhs.uk/mhsds.
Figure 5.
This chart shows the rates of detention under the Mental Health Act 1983 for different ethnic groups, with the red line on the secondary axis representing a percentage of the total between 2016 and 2017. Sources: Rates of detention (per 100,000) under the MHA 1983 by specific ethnic group in England 2016/17, Mental Health Services Dataset at: http://content.digital.nhs.uk/mhsds.
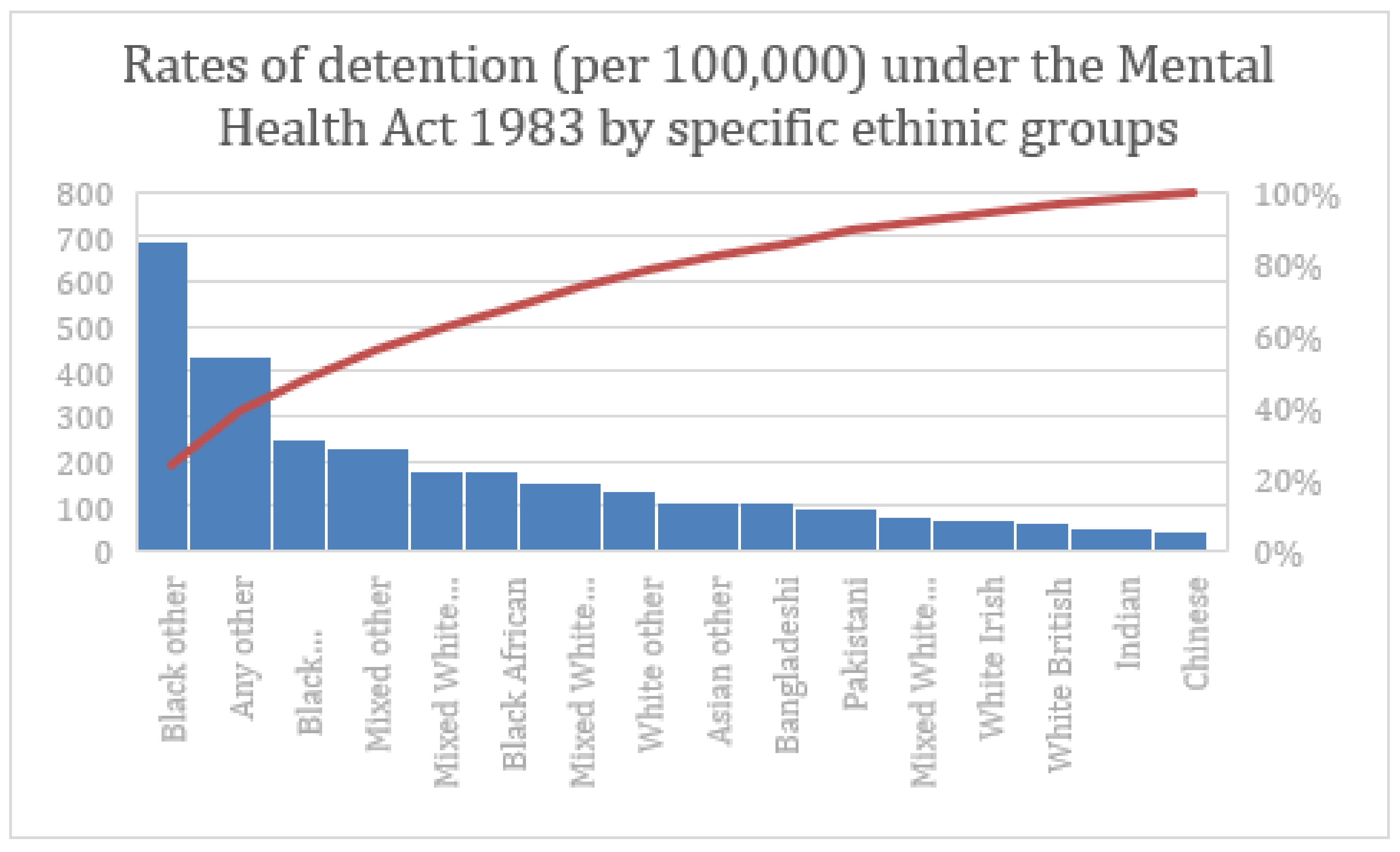
Figure 6.
This chart shows the frequency of section 136 use under the Mental Health Act 1983 in England and Wales between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the MHA 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
Figure 6.
This chart shows the frequency of section 136 use under the Mental Health Act 1983 in England and Wales between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the MHA 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.

Figure 7.
This chart shows the level of conversion between Section 136 and Section 2 and Section 3 of the Mental Health Act 1983 between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the MHA 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
Figure 7.
This chart shows the level of conversion between Section 136 and Section 2 and Section 3 of the Mental Health Act 1983 between 2011 and 2016. Source: NHS Digital, Inpatients formally detained in hospitals under the MHA 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, 30 November 2016.
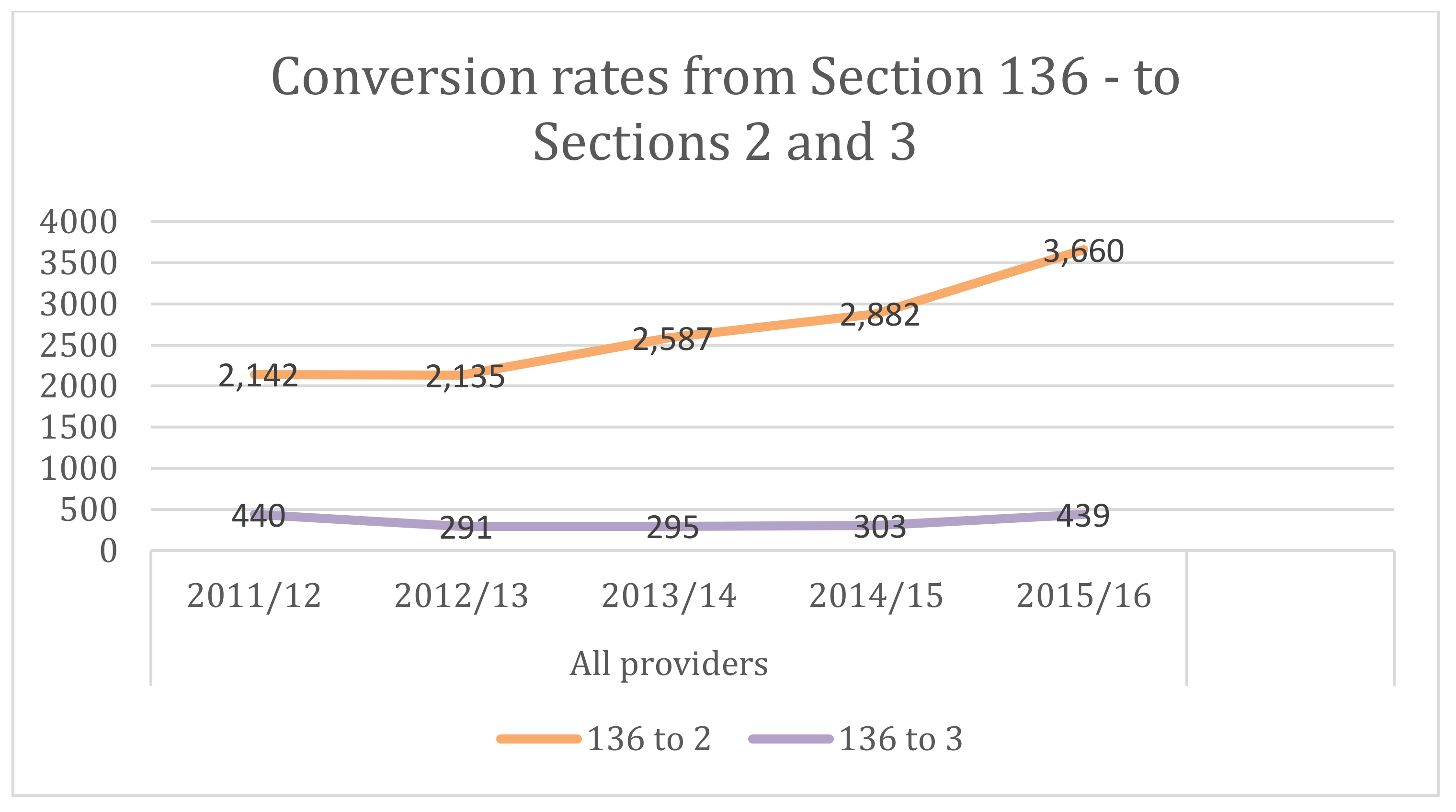
Figure 8.
This chart shows the number of mental health tribunal receipts and disposals in England between 2007 and 2016. Source: Data taken from: Ministry of Justice, Tribunals and gender recognition certificate statistics quarterly—July to September 2017, London, Ministry of Justice, 2017.
Figure 8.
This chart shows the number of mental health tribunal receipts and disposals in England between 2007 and 2016. Source: Data taken from: Ministry of Justice, Tribunals and gender recognition certificate statistics quarterly—July to September 2017, London, Ministry of Justice, 2017.

Figure 9.
This chart shows the number of mental health tribunal sittings between 2009 and 2017. Source: Ministry of Justice, Tribunal Statistics Quarterly June 2017.
Figure 9.
This chart shows the number of mental health tribunal sittings between 2009 and 2017. Source: Ministry of Justice, Tribunal Statistics Quarterly June 2017.
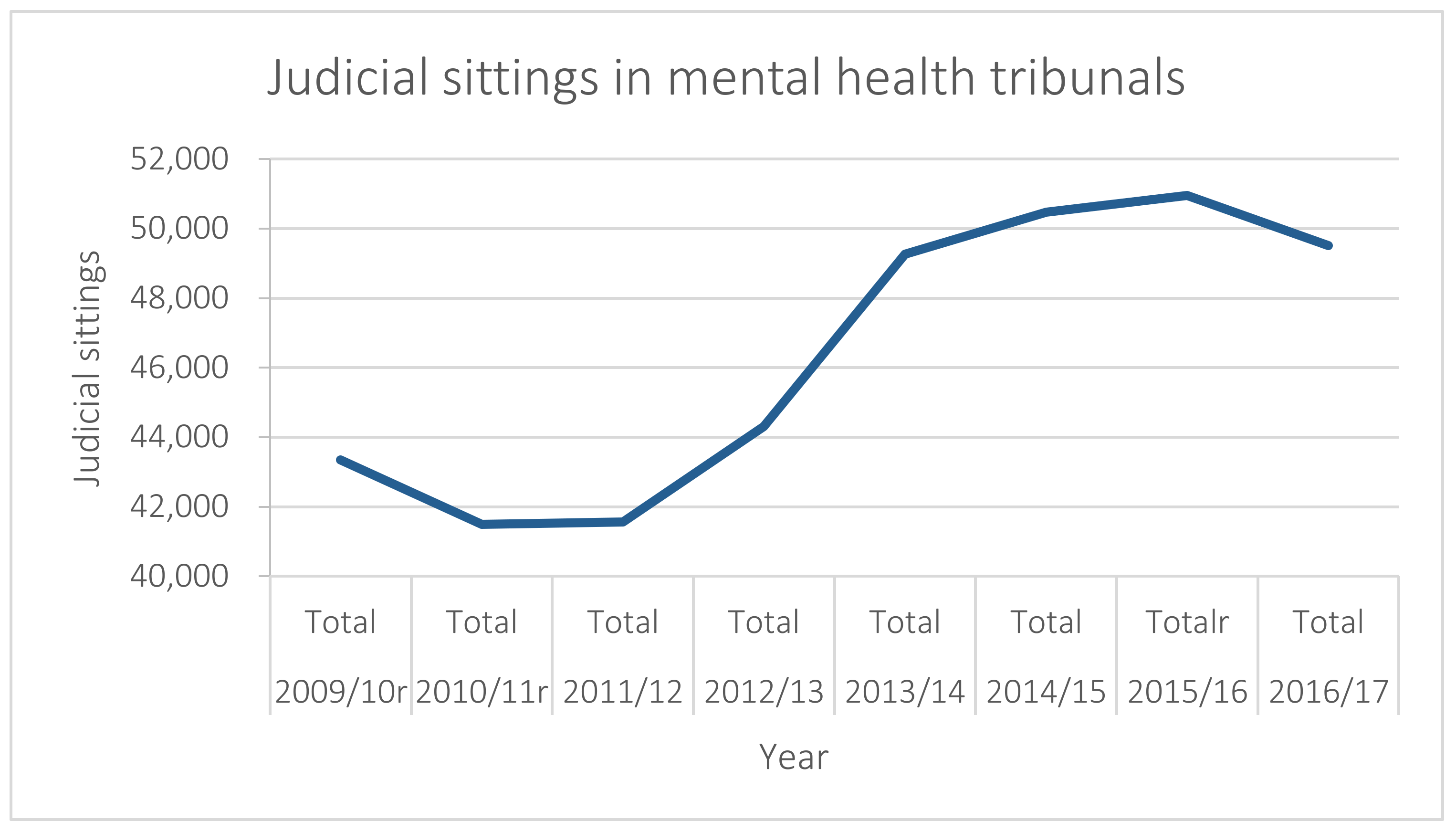
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Glover-Thomas, N. Decision-Making Behaviour under the Mental Health Act 1983 and Its Impact on Mental Health Tribunals: An English Perspective. Laws 2018, 7, 12. https://doi.org/10.3390/laws7020012
AMA Style
Glover-Thomas N. Decision-Making Behaviour under the Mental Health Act 1983 and Its Impact on Mental Health Tribunals: An English Perspective. Laws. 2018; 7(2):12. https://doi.org/10.3390/laws7020012
Chicago/Turabian StyleGlover-Thomas, Nicola. 2018. "Decision-Making Behaviour under the Mental Health Act 1983 and Its Impact on Mental Health Tribunals: An English Perspective" Laws 7, no. 2: 12. https://doi.org/10.3390/laws7020012
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.