Defining Multidrug Resistance of Gram-Negative Bacteria in the Dutch–German Border Region—Impact of National Guidelines

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Number of Antibiograms and Patients
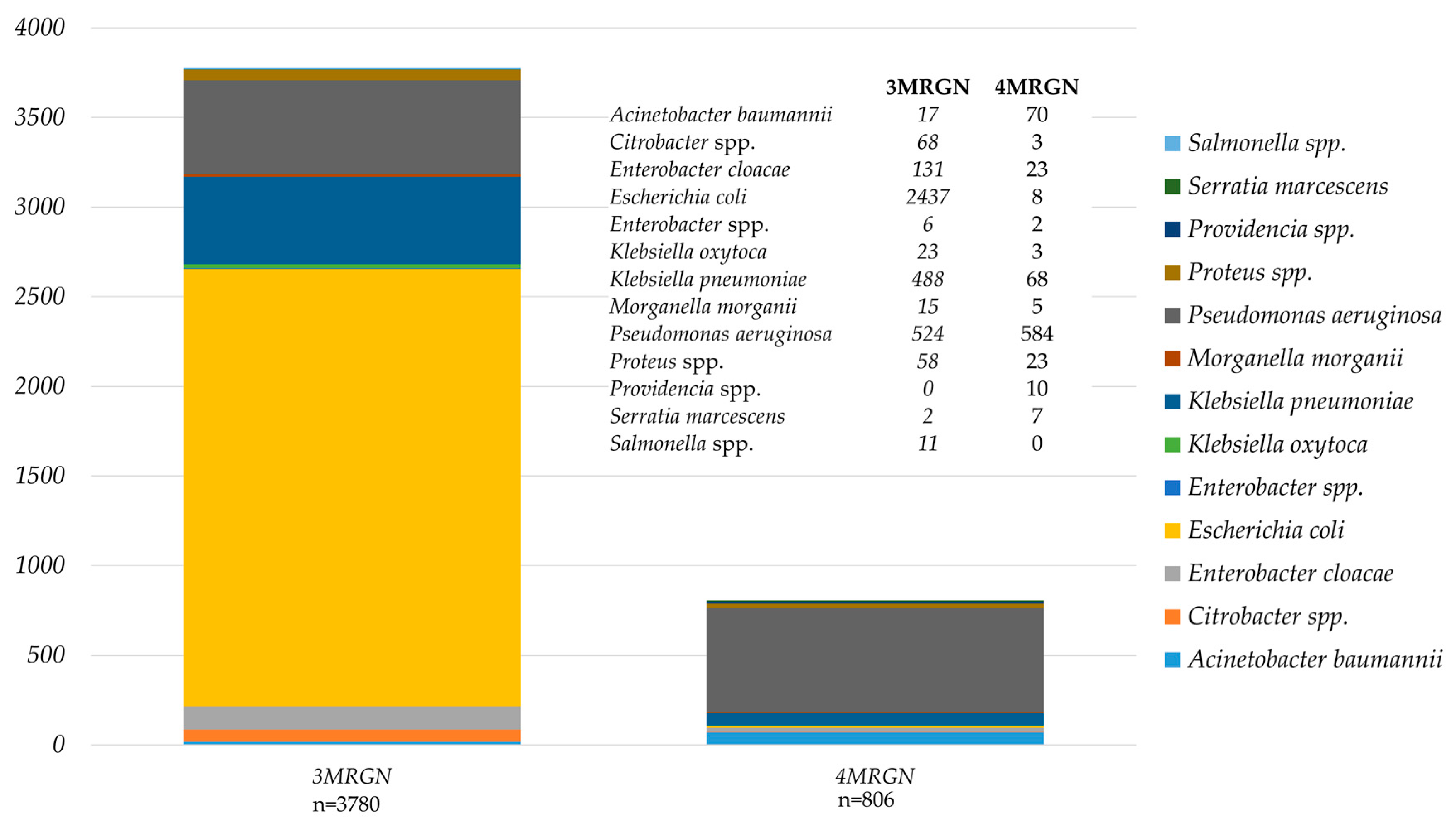
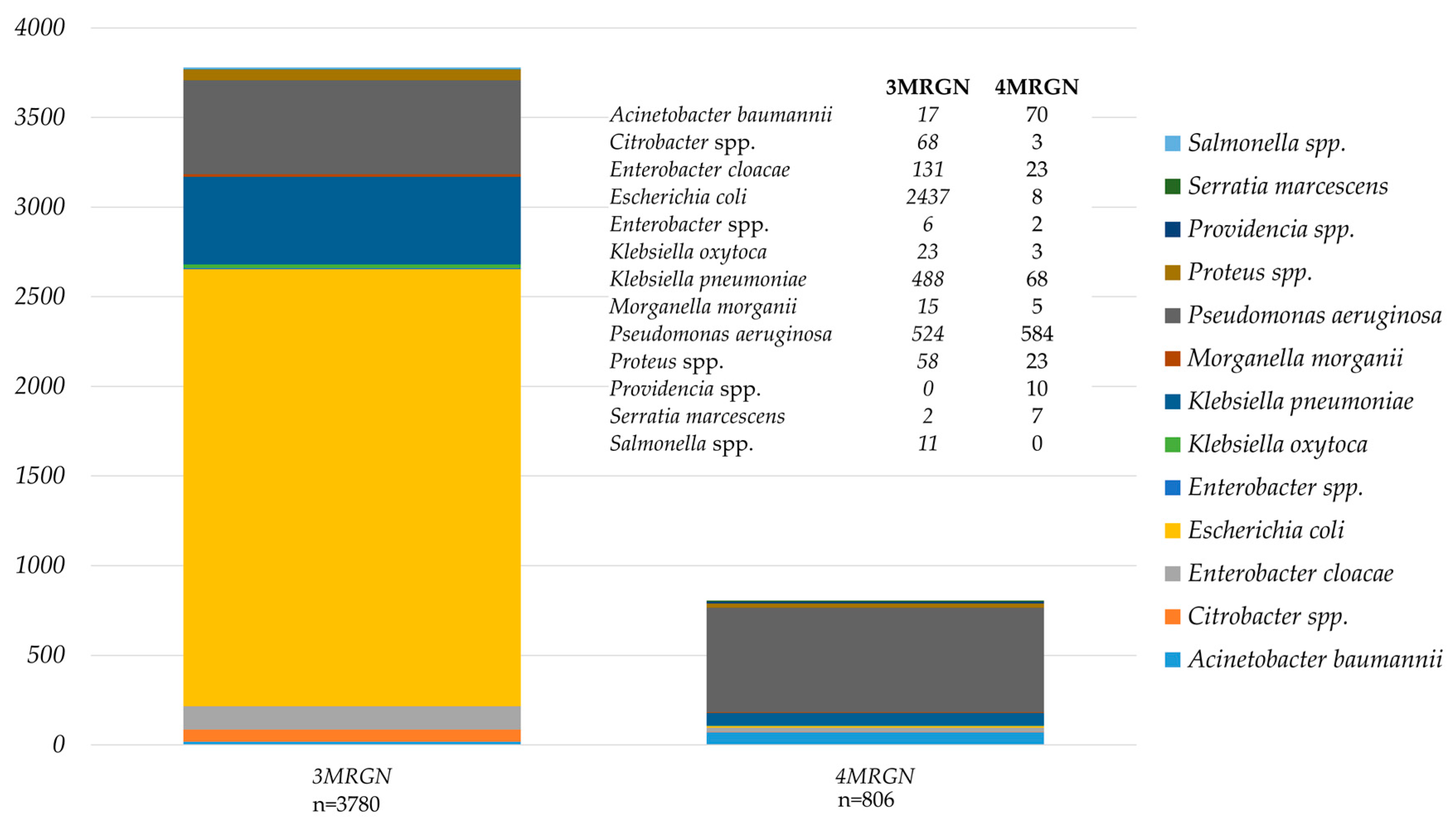
3.2. Results of MRGN and BRMO Classification
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Magiorakos, A.P.; Burns, K.; Rodríguez Baño, J.; Borg, M.; Daikos, G.; Dumpis, U.; Lucet, J.C.; Moro, M.L.; Tacconelli, E.; Simonsen, G.S.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control 2017, 6, 113. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. EARS-Net Resistance Data for 2016. Available online: http://atlas.ecdc.europa.eu/public/index.aspx (accessed on 15 December 2017).
- Albiger, B.; Glasner, C.; Struelens, M.J.; Grundmann, H.; Monnet, D.L. European Survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE) Working Group. Carbapenemase-producing Enterobacteriaceae in Europe: Assessment by national experts from 38 countries, May 2015. Euro Surveill. 2015, 20, 30062. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.; Voss, A.; Köck, R.; Sinha, B.; Rossen, J.W.; Kaase, M.; Mielke, M.; Daniels-Haardt, I.; Jurke, A.; Hendrix, R.; et al. Cross-border comparison of the Dutch and German guidelines on multidrug-resistant Gram-negative microorganisms. Antimicrob. Resist. Infect. Control 2015, 4, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO). Hygienemaßnahmen bei Infektionen oder Besiedlung mit multiresistenten gramnegativen Stäbchen. Bundesgesundheitsbl 2012, 55, 1311–1354. [Google Scholar]
- Werkgroep Infectiepreventie. BRMO (Bijzonder Resistente Micro-Organismen)—Ziekenhuizen. Available online: http://www.rivm.nl/dsresource?objectid=b6b99580-44e2-4b9c-8183-52871e61764f&type=org&disposition=inline (accessed on 17 December 2017).
- Mellmann, A.; Bletz, S.; Böking, T.; Kipp, F.; Becker, K.; Schultes, A.; Prior, K.; Harmsen, D. Real-Time Genome Sequencing of Resistant Bacteria Provides Precision Infection Control in an Institutional Setting. J. Clin. Microbiol. 2016, 54, 2874–2881. [Google Scholar] [CrossRef] [PubMed]
- Kluytmans-van den Bergh, M.F.Q.; van Mens, S.P.; Haverkate, M.R.; Bootsma, M.C.J.; Kluytmans, J.A.J.W.; Bonten, M.J.M.; SoM Study Group. Quantifying Hospital-Acquired Carriage of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae among Patients in Dutch Hospitals. Infect. Control Hosp. Epidemiol. 2018, 39, 32–39. [Google Scholar] [CrossRef] [PubMed]
- SWAB. NethMap 2017—Consumption of Antimicrobial Agents and Antimicrobial Resistance among Medically Important Bacteria in The Netherlands in 2016. Available online: http://www.swab.nl (accessed on 17 December 2017).
- Paul-Ehrlich Gesellschaft (PEG). Bundesamt für Verbraucherschutz und Lebensmittelsicherheit, GERMAP 2015—Antibiotika-Resistenz und –Verbrauch. Available online: http://www.p-e-g.org/econtext/germap (accessed on 17 December 2017).
- Kaase, M. Bericht des Nationalen Referenzzentrums (NRZ) für gramnegative Krankenhauserreger. Epidemiol. Bull. 2016, 2, 11–14. [Google Scholar]

{kind=link}
| Bacteria | Categories 1 | Classification | ||||
|---|---|---|---|---|---|---|
| I | II | III | IV | 3MRGN 5 | 4MRGN 5 | |
| Enterobacteriaceae 2 | PIP | TAX | CIP | IMI 3 or MER or CARB | Resistance to three of four categories | Resistance to four of four categories or to category IV alone |
| P. aeruginosa | PIP | TAZ and FEM | CIP | IMI and MER | Resistance to three of four categories | Resistance to four of four categories |
| A. baumannii | PIP 4 | TAZ 4 | CIP | IMI or MER or CARB | Resistance to three of four categories | Resistance to four of four categories or to category IV alone |
| Bacteria | Categories 1 | ||||||
|---|---|---|---|---|---|---|---|
| ESBL | CARB 1 | FQ | AM | PIP | TAZ | SXT | |
| Enterobacteriaceae 2 | BRMO 3 | BRMO | BRMO: Resistance to FQ and AM 2 | - | - | ||
| P. aeruginosa | - | BRMO: Resistance to ≥3 categories: CARB 1, FQ; AM; PIP; TAZ | - | ||||
| A. baumannii | - | BRMO | BRMO: Resistance to FQ and AM 2 | - | - | ||
| S. maltophilia | - | - | - | BRMO | |||
| Dutch Classification | German Classification | ||||
|---|---|---|---|---|---|
| BRMO 1 | no BRMO 1 | MRGN 1 | no MRGN 1 | p | |
| A. baumannii | 72 | 370 | 87 | 355 | 0.2202 |
| Citrobacter spp. | 79 | 626 | 71 | 634 | 0.5454 |
| E. cloacae | 146 | 972 | 154 | 964 | 0.6641 |
| E. coli | 5270 | 9606 | 2445 | 12,431 | <0.0001 |
| Enterobacter spp. | 8 | 280 | 8 | 280 | 1 |
| Hafnia spp. | 1 | 44 | 0 | 45 | 1 |
| K. oxytoca | 75 | 1885 | 26 | 1934 | 0.0001 |
| K. pneumoniae | 877 | 2578 | 556 | 2899 | <0.0001 |
| Klebsiella spp. | 0 | 17 | 0 | 17 | 1 |
| Morganella spp. | 45 | 226 | 20 | 251 | 0.0015 |
| P. aeruginosa | 788 | 5068 | 1108 | 4748 | <0.0001 |
| Proteus spp. | 257 | 1009 | 81 | 1185 | <0.0001 |
| Providencia spp. | 16 | 33 | 10 | 39 | 0.2526 |
| S. maltophilia | 30 | 471 | 0 | 501 | <0.0001 |
| Salmonella | 95 | 17 | 11 | 101 | <0.0001 |
| S. marcescens | 11 | 770 | 9 | 772 | 0.8219 |
| Serratia spp. | 2 | 43 | 0 | 45 | 0.4944 |
| Total | 7772 | 24,015 | 4586 | 27,201 | <0.0001 |
| MRGN % BRMO 1 | MRGN % BRMO/CARB 2 | BRMO % 3MRGN 3 | BRMO % 4MRGN 3 | BRMO % MRGN (All) 3 | no MDRGNB 4 | no Isolates 5 | |
|---|---|---|---|---|---|---|---|
| Acinetobacter baumannii | 98.6 | 100.0 | 5.9 | 100.0 | 81.6 | 80.1 | 442 |
| Citrobacter spp. | 54.4 | 100.0 | 58.8 | 100.0 | 60.6 | 84.8 | 705 |
| Enterobacter cloacae | 58.2 | 100.0 | 57.3 | 43.5 | 55.2 | 80.8 | 1118 |
| Enterobacter spp. | 12.5 | 100.0 | 16.7 | 0.0 | 12.5 | 94.8 | 288 |
| Escherichia coli | 45.5 | 100.0 | 98.3 | 37.5 | 98.1 | 63.3 | 14,876 |
| Hafnia spp. | 0.0 | 100.0 | 100.0 | 100.0 | 100.0 | 97.8 | 45 |
| Klebsiella oxytoca | 21.3 | 100.0 | 60.9 | 66.7 | 61.5 | 95.7 | 1960 |
| Klebsiella pneumoniae | 61.7 | 100.0 | 99.0 | 85.3 | 97.3 | 74.2 | 3455 |
| Klebsiella spp. | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 17 |
| Morganella spp. | 33.3 | 100.0 | 67.0 | 100.0 | 75.0 | 81.5 | 271 |
| Proteus spp. | 30.0 | 100.0 | 96.6 | 91.3 | 95.1 | 79.4 | 1266 |
| Providencia spp. | 62.5 | 100.0 | 100.0 | 100.0 | 100.0 | 67.3 | 49 |
| Pseudomonas aeruginosa | 92.8 | 100.0 | 34.7 | 94.0 | 66.0 | 80.1 | 5856 |
| Salmonella spp. | 11.6 | 100.0 | 100.0 | 100.0 | 100.0 | 15.2 | 112 |
| Serratia marcescens | 36.4 | 100.0 | 100.0 | 28.6 | 44.4 | 98.0 | 781 |
| Serratia spp. | 0.0 | 100.0 | 100.0 | 100.0 | 100.0 | 95.6 | 45 |
| Stenotrophomonas maltophilia | 0.0 | 100.0 | 100.0 | 100.0 | 100.0 | 94.0 | 501 |
| Legend | ≥75.0% | 25.0–74.9% | <25.0% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köck, R.; Siemer, P.; Esser, J.; Kampmeier, S.; Berends, M.S.; Glasner, C.; Arends, J.P.; Becker, K.; Friedrich, A.W. Defining Multidrug Resistance of Gram-Negative Bacteria in the Dutch–German Border Region—Impact of National Guidelines. Microorganisms 2018, 6, 11. https://doi.org/10.3390/microorganisms6010011
Köck R, Siemer P, Esser J, Kampmeier S, Berends MS, Glasner C, Arends JP, Becker K, Friedrich AW. Defining Multidrug Resistance of Gram-Negative Bacteria in the Dutch–German Border Region—Impact of National Guidelines. Microorganisms. 2018; 6(1):11. https://doi.org/10.3390/microorganisms6010011
Chicago/Turabian StyleKöck, Robin, Philipp Siemer, Jutta Esser, Stefanie Kampmeier, Matthijs S. Berends, Corinna Glasner, Jan P. Arends, Karsten Becker, and Alexander W. Friedrich. 2018. "Defining Multidrug Resistance of Gram-Negative Bacteria in the Dutch–German Border Region—Impact of National Guidelines" Microorganisms 6, no. 1: 11. https://doi.org/10.3390/microorganisms6010011