World-Wide Variation in Incidence of Staphylococcus aureus Associated Ventilator-Associated Pneumonia: A Meta-Regression


1
Rural Health Academic Center, Melbourne Medical School, University of Melbourne, Ballarat, VIC 3350, Australia
2
Division of Internal Medicine, Ballarat Health Services, Ballarat, VIC 3350, Australia
Microorganisms 2018, 6(1), 18; https://doi.org/10.3390/microorganisms6010018
Submission received: 19 January 2018
/
Revised: 13 February 2018
/
Accepted: 25 February 2018
/
Published: 27 February 2018
(This article belongs to the Special Issue Staphylococcus aureus Infection and Antimicrobial Resistance)
Abstract
:Staphylococcus aureus (S. aureus) is a common Ventilator-Associated Pneumonia (VAP) isolate. The objective here is to define the extent and possible reasons for geographic variation in the incidences of S. aureus-associated VAP, MRSA-VAP and overall VAP. A meta-regression model of S. aureus-associated VAP incidence per 1000 Mechanical Ventilation Days (MVD) was undertaken using random effects methods among publications obtained from a search of the English language literature. This model incorporated group level factors such as admission to a trauma ICU, year of publication and use of bronchoscopic sampling towards VAP diagnosis. The search identified 133 publications from seven worldwide regions published over three decades. The summary S. aureus-associated VAP incidence was 4.5 (3.9–5.3) per 1000 MVD. The highest S. aureus-associated VAP incidence is amongst reports from the Mediterranean (mean; 95% confidence interval; 6.1; 4.1–8.5) versus that from Asian ICUs (2.1; 1.5–3.0). The incidence of S. aureus-associated VAP varies by up to three-fold (for the lowest versus highest incidence) among seven geographic regions worldwide, whereas the incidence of VAP varies by less than two-fold. Admission to a trauma unit is the most important group level correlate for S. aureus-associated VAP.
1. Introduction
Ventilator-Associated Pneumonia (VAP) in association with Staphylococcus aureus has been reported from over 100 intensive care units (ICU) worldwide [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133]. In two series drawn predominantly from ICUs in The United States of America and Europe, S. aureus accounted for 20% [134] and 22% [135] of bronchoscopically-documented cases of VAP.
Whether VAP is associated with an increase in attributable mortality may depend on the infecting organism [8,12,115,135]. There may be a specific mortality risk for ventilator-associated pneumonia in association with S. aureus infections in the ICU, although this may be influenced by associated resistance to methicillin [136,137].
There is a worldwide variation in the microbial aetiologies of VAP and other ICU-acquired infections [1,2,3,4,5,6,8,115,130,131,132,133,134,135,136,137,138,139,140]. For example, the incidence of Acinetobacter-associated VAP varies five-fold among reports from ICUs from various geographic regions around the world [139].
The objective here is to define the extent of geographic variation in the incidence of VAP associated with S. aureus within the published literature versus the variation in the incidences associated with VAP overall and with MRSA-VAP. An additional aim is to explore the degree to which any variation may be explainable by other study-related factors, such as mode of VAP diagnosis or admission for trauma [67], using meta-regression methods.
2. Methods
Because this analysis was based on a literature survey, institutional review board approval was not required.
The literature search and analytic approach used here has been adapted from one used previously [139]. In brief, an electronic search of PubMed, the Cochrane database and Google Scholar for systematic reviews containing potentially eligible studies was done using the following search terms: “ventilator-associated pneumonia”, “mechanical ventilation”, “intensive care unit”. The study inclusion criteria were as follows; a listing of S. aureus among the VAP isolates, reporting in the English language and reports for which a VAP incidence could be estimated using the number of Mechanical Ventilation Days (MVD) as the denominator. A hand search was undertaken for additional studies not identified within systematic reviews.
Studies that were restricted to eligible patients within randomized controlled trials were not included as these generally limit inclusion to patients meeting specific eligibility criteria. However, studies that were undertaken without patient restriction within the context of process improvement for the purpose of general infection prevention were retained in the model and designated ‘intervention period’ studies. Studies that were limited to paediatric, burns [141] or haemato-oncology ICUs were excluded.
The S. aureus-associated VAP incidence is defined as the number of patients with VAP having S. aureus isolated from respiratory sampling per 1000 MVD. Where necessary, the numerator was derived as the number of patients with VAP multiplied by the proportion of VAP isolates that were S. aureus. This approximation allows for VAP patients with multiple isolates. In addition, the following were also extracted where available: the number of ICU patients surveyed, the overall incidence of VAP per 1000 mechanically ventilated days, whether the mode of diagnosis of VAP required bronchoscopic sampling and whether the ICU was a trauma ICU (defined as more than 50% of patient admissions being for trauma).
The assignment of countries to near neighbour groupings was solely determined in relation to geographic proximity without regard to political, economic or other considerations. It was not always clear as to the dates to which each survey applied. For convenience and for uniformity, the year of publication rather than the year of the study has been used as a covariate in the meta-regression models and the figures. Meta-regression models of VAP overall, S. aureus-associated VAP and MRSA-VAP were undertaken using the relevant inverse of the variance for each as the study weighting. Because heterogeneity is to be expected both within and between regions, a random effects method was used in deriving summary estimates. The following predictor variables were used without pre-selection in the regression model: the geographic region, whether bronchoscopic sampling was used in the diagnosis of VAP, trauma ICU, year of publication and whether an infection prevention intervention was in place. All factors were entered into the regression models without any pre-selection step. For the purpose of the meta-regression models, the groups from multinational studies and those from studies that were ungrouped were collapsed into a single group, and this composite group was used as the reference group.
Availability of Data and Materials
The datasets supporting the conclusions of this article are included within the article and its additional file.
3. Results
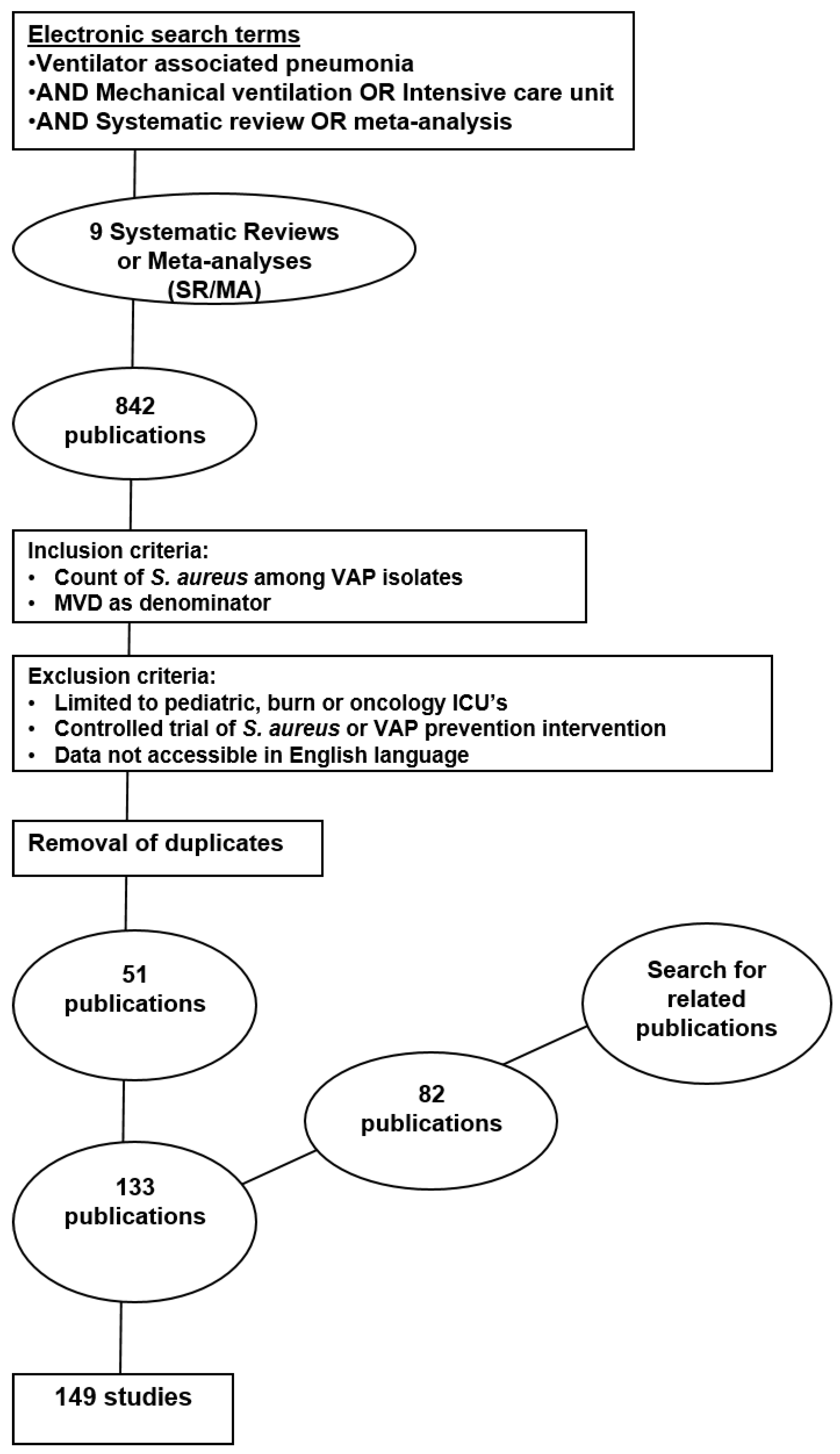
The search identified 149 study groups contained in 133 publications published between 1986 and 2018 [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133]. Of the 133 publications found, 51 had and 82 had not been cited within one of eight systematic reviews identified by the search [142,143,144,145,146,147,148,149] (Figure 1). Fifteen publications provided more than one study. The studies are detailed in Table S1 (see the additional file). The studies were classified by geographic region as detailed in Table 1. There were 17 multinational ICU surveys from six publications that were derived from ICUs that had been anonymized by originating country in these publications.
There were 21 studies that reported for trauma ICU populations. While none of the studies were undertaken in an ICU subject to a known outbreak, there were nine studies undertaken in the context of an infection control intervention. The use of bronchoscopic sampling in the diagnosis of VAP was unequal among the seven regions being used in more than half of the studies from Northern Europe and the Mediterranean versus less than half of studies elsewhere (p < 0.001; chi-square = 27.13, 6 df).
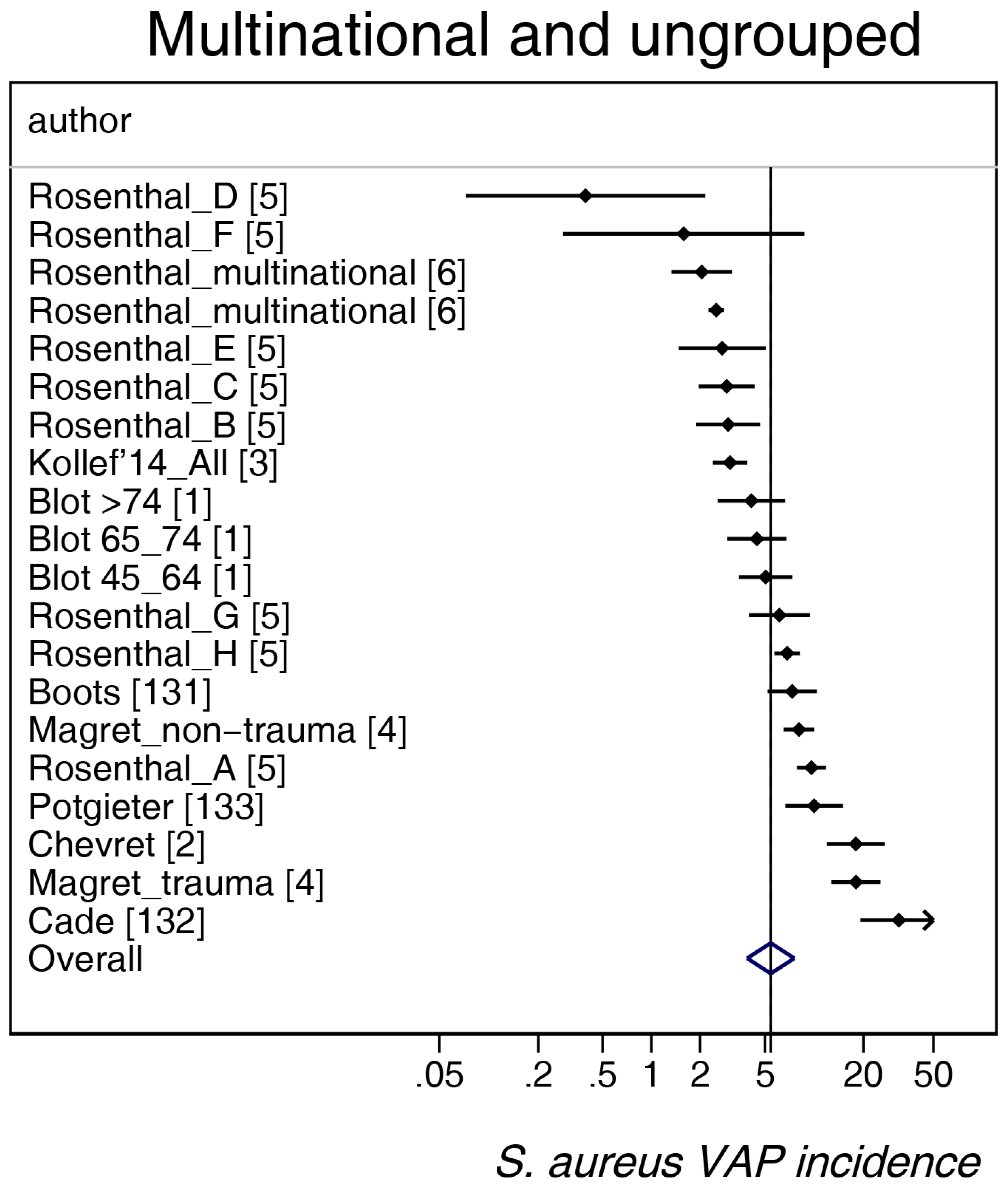
The study-specific S. aureus-associated VAP incidence is displayed by regions (Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6) and collectively with all studies together (Figure 7 and Figure 8). The incidence of MRSA-VAP are displayed by year of publication (Figure S1) and collectively by country (Figure 9). Over all 162 groups, the summary incidence of VAP was 21.3 (18.9–23.8) per 1000 MVD (Figure S2) and 17.1 (14.0–20.6) per 100 patients. The summary S. aureus-associated VAP incidence was 4.5 (3.9–5.3) per 1000 MVD and 3.4 (2.6–4.5) per 100 patients. The numbers of MRSA VAPs were reported for 55 studies, and the summary was 2.2 (1.6–3.1) per 1000 MVD.
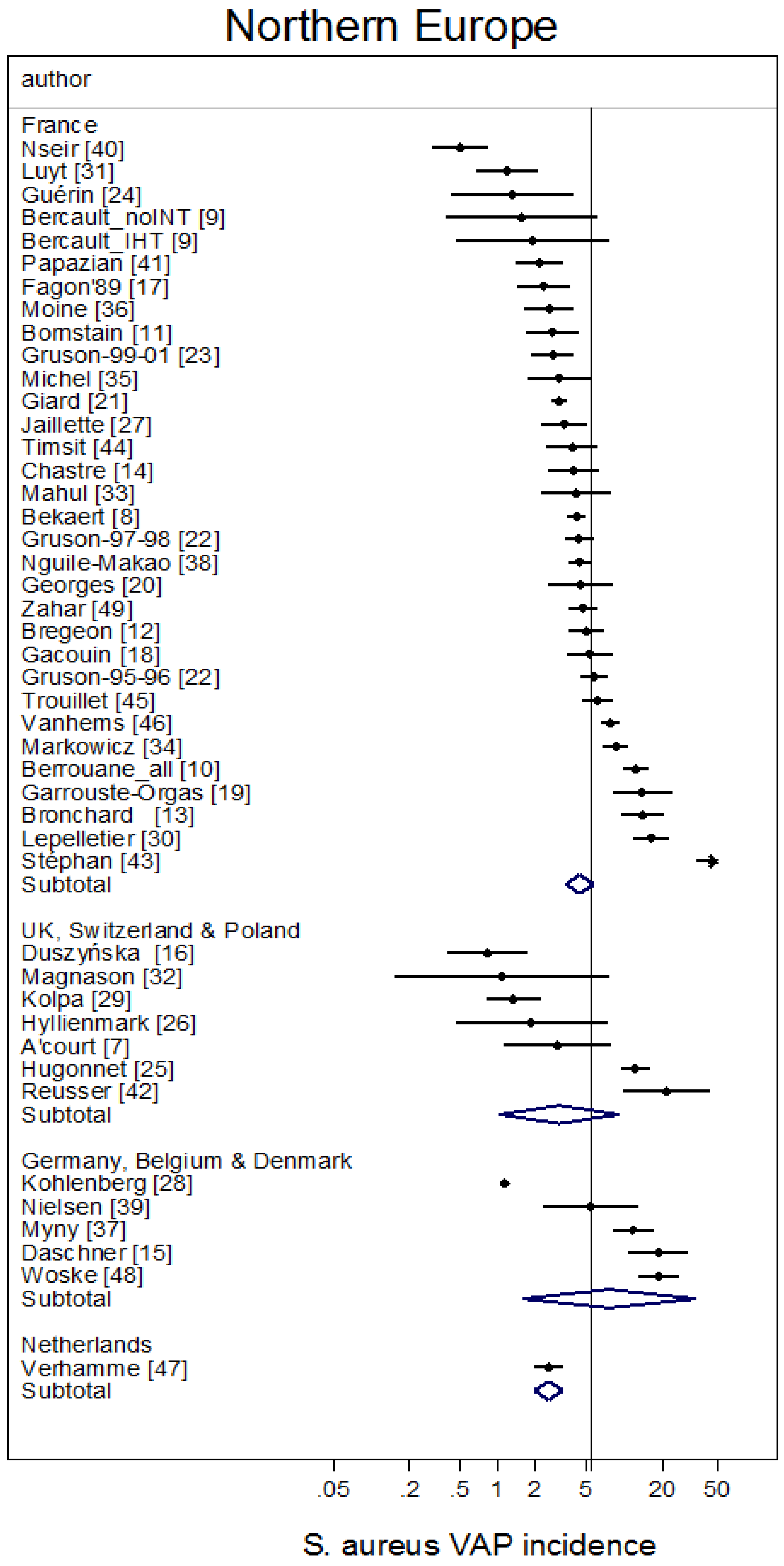
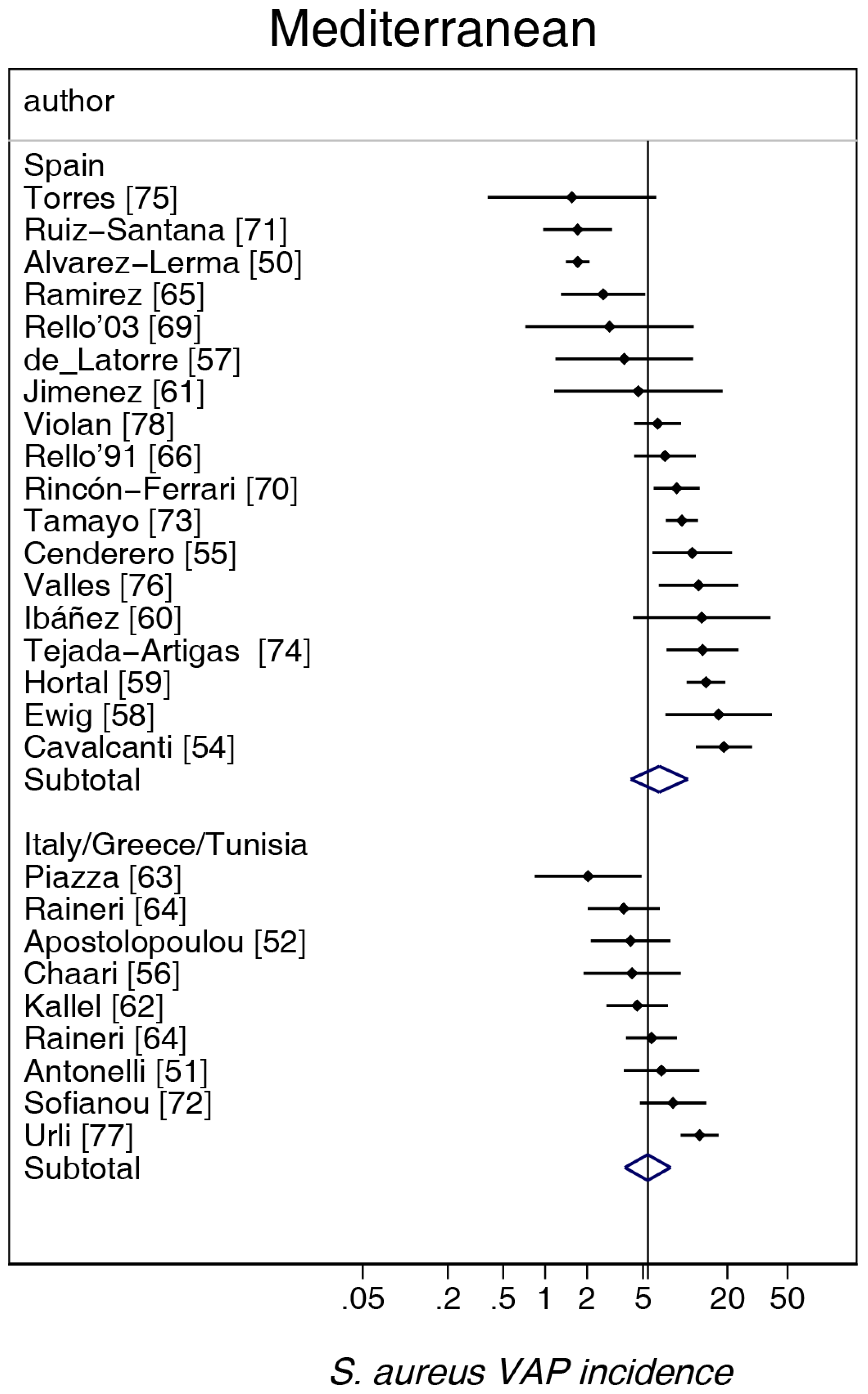
The highest and lowest S. aureus-associated VAP incidences were amongst reports from Mediterranean versus Asian ICUs, respectively. By contrast, the highest and lowest incidences of VAP overall were amongst reports from Mediterranean versus Northern European ICUs, respectively. The incidence of MRSA VAP was lowest within reports from Northern European ICUs (Table 1).
Meta-regression models of VAP incidence, S. aureus-associated VAP and MRSA-VAP incidence are presented in Table 2. In the meta-regression model for VAP incidence overall and for S. aureus-associated VAP incidence, origins from a trauma ICU, but not mode of diagnosis using bronchoscopic sampling were significant correlates. In these models, origin from a Northern European study was significantly associated with lower incidences of VAP overall and MRSA-VAP, but not S. aureus VAP. In none of the three models was the year of publication significantly associated with incidence. However, a closer examination revealed an interaction in that a decline in S. aureus-associated VAP (Figure 8) and MRSA-VAP (see the additional file: Figure S2) incidences over the years was apparent for reports from non-trauma ICUs, but not for trauma ICUs (p = 0.001).
4. Discussion
This is a survey of the incidences of VAP overall, S. aureus-associated VAP and MRSA-VAP among over 100 published studies using meta-analysis. The incidences of S. aureus-associated VAP and MRSA-VAP each vary by up to three-fold for the lowest versus highest incidence region among seven geographic regions worldwide, whereas the incidence of VAP varies by less than two-fold.
This variation in incidence among seven broad multinational regions is partly explainable by a limited number of group level factors. Of note, in the meta-regression models, trauma is more strongly correlated with S. aureus-associated VAP than was the case for the incidence of VAP overall or MRSA-VAP. A decline in the incidences of S. aureus-associated VAP and MRSA-VAP in association with year of publication is apparent only for reports originating from non-trauma ICUs.
The less than three-fold variation in S. aureus-associated VAP contrasts with the greater than five-fold variation in Acinetobacter-associated VAP incidence observed in an analysis of mostly the same studies as included here [139].
The findings here reinforce and further characterize previous observations in four multi-national surveys [1,3,5,140]. Rello et al. surveyed ICUs in the following four regions: Paris, Barcelona, Montevideo and Seville, and likewise found less variation between the sites in S. aureus-associated VAP than was the case for Acinetobacter-associated VAP [141]. Another multi-national prospective 24-month survey [5] was conducted across 55 ICUs of 46 hospitals in Argentina, Brazil, Colombia, India, Mexico, Morocco, Peru and Turkey. This anonymized survey also found less variation in S. aureus-associated VAP than was the case for Acinetobacter-associated VAP. This survey found an overall rate of VAP of 24.1 per 1000 MV days with S. aureus accounting for between 13 and 53% of VAP isolates amongst the eight anonymized countries [5].
Kollef et al. prospectively surveyed VAP among 1873 mechanically-ventilated patients in 56 ICUs from 11 countries in the following four regions: Europe, United States, Latin America and the Asia-pacific region [3]. This survey [3] found that the incidence per 100 patients of VAP overall, S. aureus VAP and MRSA-VAP among all 56 ICUs was 293/1873 (15.6%), 65/1873 (3.5%) and 27/1873 (1.4%), respectively. This compares to incidence proportions for VAP overall and S. aureus VAP found here being 17.1 (14.0–20.6), 3.4 (2.6–4.5) and 1.95 (1.14–3.3), respectively. Interestingly, these investigators found that the incidence of VAP overall, but not the incidence of P. aeruginosa VAP varied among the four broadly-defined worldwide regions. In this study [3], the incidences of S. aureus VAP and MRSA-VAP were each only reported in aggregate.
Finally, a survey of 27 European ICUs found a summary VAP incidence of 18.3 per 1000 MVD and that the dominant nosocomial pneumonia isolate varied among the nine European countries in the survey [1,138]. S. aureus was the dominant pneumonia isolate in Spain, France, Belgium and Ireland [1,138].
The extent to which any possible variation in VAP microbiology between regions is explainable by group level factors is difficult to establish in studies that are either short term or single centre. However, the findings here that admissions for trauma, but not bronchoscopic sampling undertaken as part of VAP diagnosis are significant factors towards S. aureus VAP are in line with findings reported from single centre studies [150,151].
With a literature survey, a considerable convenience is that the data are readily available, and the meta-regression methods for analysing these types of data are established. A random effects meta-regression methods is used as previously to enable the imprecision associated with each individual study estimate to be incorporated in the derivation of both the summary estimates and in the meta-regression models [139,152]. This is the major advantage of a meta-analysis in comparison to a simple narrative review. Estimates with random effects are more conservative (i.e., wider 95% confidence limits) than with fixed effects. This analytic approach enables an appreciation of the contextual influences of study-specific factors that would not be apparent within a single centre study examined in isolation.
There are several limitations to this analysis of the literature. Of particular note, this is not a systematic review, and the analysis is limited to English language articles. This is an analysis at the group level and therefore is unable to take account of patient-specific risk factors for S. aureus-associated VAP. For example, the duration of mechanical ventilation and usage of empiric antibiotic therapy are important VAP determinants at the level of the individual patient that cannot be explored at the group level of analysis. To include patient level information within a meta-analysis would require an individual patient data meta-analysis.
A further limitation relating to the survey of MRSA-VAP is that in some reports, MRSA-VAP may not have been reported as a consequence of being rare in that specific location. Hence, this reporting bias may lead to under-representation of zero counts. Moreover, the analysis is unable to account for strain type differences underlying the variation in both S. aureus VAP incidence and also in MRSA-VAP incidence. The ‘intervention periods’ studies include a broad range of interventions. Their inclusion is to indicate the influence relative to other group level associates on the incidences. However, the methodology used here is not appropriate for the evaluation of the effectiveness of infection control interventions. Randomised controlled trials were not included here for two reasons. Firstly, the populations of these studies usually are a small sub-group that meets specific inclusion criteria. Moreover, there is the potential for a contextual effect in the presence of any such intervention within an ICU on the incidence of VAP overall [152], and more so in relation to the potential contextual effect of prevention interventions on S. aureus-associated VAP [151,152,153].
As with any multi-national survey, a range of definitions was applied in the diagnosis of VAP among the studies here, and standardisation was not possible. The classification of studies into those that did versus did not use bronchoscopic sampling towards VAP diagnosis was a simplifying compromise.
The grouping of countries into near neighbour groupings is somewhat arbitrary. This grouping may conceal important variations within each of the regions. Country and even regional groupings could be confounded by other variables such as infection control practices, prevalence of antibiotic use and standards of care for patients receiving mechanical ventilation, which are not able to be considered in the analysis here. Indeed, even the imperative to publish may differ in different countries. The influence of publication bias is difficult to estimate.
5. Conclusions
There is a variation of up to three-fold in S. aureus-associated VAP and MRSA-VAP among published reports from seven broad geographic regions worldwide. This variation exceeds the variation in incidence of VAP overall. For MRSA-VAP incidence, there is a complex interaction between the year of publication and admission for trauma.
Supplementary Materials
The following are available online at https://www.mdpi.com/2076-2607/6/1/18/s1. Table S1: Listing of studies reporting S aureus VAP & MRSA-VAP. Figure S1: MRSA-VAP incidence (per 1000 MV days) versus year of study publication. Figure S2: A scatter plot of VAP overall incidence worldwide.
Supplementary File 1Funding
This research was supported by the Australian Government Department of Health and Ageing through the Rural Clinical Training and Support (RCTS) program. The funding agency had no role in the preparation of the manuscript, nor its approval for submission.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blot, S.; Koulenti, D.; Dimopoulos, G.; Martin, C.; Komnos, A.; Krueger, W.A.; Spina, G.; Armaganidis, A.; Rello, J.; EU-VAP Study Investigators. Prevalence, risk factors, and mortality for ventilator-associated pneumonia in middle-aged, old, and very old critically ill patients. Crit. Care Med. 2014, 42, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Chevret, S.; Hemmer, M.; Carlet, J.; Langer, M. Incidence and risk factors of pneumonia acquired in intensive care units. Results from a multicenter prospective study on 996 patients. European Cooperative Group on Nosocomial Pneumonia. Intensive Care Med. 1993, 19, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Chastre, J.; Fagon, J.Y.; François, B.; Niederman, M.S.; Rello, J.; Torres, A.; Vincent, J.L.; Wunderink, R.G.; Go, K.W.; et al. Global prospective epidemiologic and surveillance study of ventilator-associated pneumonia due to Pseudomonas aeruginosa. Crit. Care Med. 2014, 42, 2178–2187. [Google Scholar] [CrossRef] [PubMed]
- Magret, M.; Amaya-Villar, R.; Garnacho, J.; Lisboa, T.; Diaz, E.; DeWaele, J.; Deja, M.; Manno, E.; Rello, J.; et al. Ventilator-associated pneumonia in trauma patients is associated with lower mortality: Results from EU-VAP study. J. Trauma Acute Care Surg. 2010, 69, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, V.D.; Maki, D.G.; Salomao, R.; Moreno, C.A.; Mehta, Y.; Higuera, F.; Cuellar, L.E.; Arikan, O.A.; Abouqal, R.; Leblebicioglu, H. Device-associated nosocomial infections in 55 intensive care units of 8 developing countries. Ann. Intern. Med. 2006, 145, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, V.D.; Rodrigues, C.; Madani, N.; Mitrev, Z.; Ye, G.; Salomao, R.; Ulger, F.; Guanche-Garcell, H.; Kanj, S.S.; Cuéllar, L.E.; et al. Effectiveness of a multidimensional approach for prevention of ventilator-associated pneumonia in adult intensive care units from 14 developing countries of four continents: Findings of the International Nosocomial Infection Control Consortium. Crit. Care Med. 2012, 40, 3121–3128. [Google Scholar] [CrossRef] [PubMed]
- A’court, C.H.; Garrard, C.S.; Crook, D.; Bowler, I.; Conlon, C.; Peto, T.; Anderson, E. Microbiological lung surveillance in mechanically ventilated patients, using non-directed bronchial lavage and quantitative culture. Q. J. Med. 1993, 86, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Bekaert, M.; Timsit, J.F.; Vansteelandt, S.; Depuydt, P.; Vésin, A.; Garrouste-Orgeas, M.; Decruyenaere, J.; Clec’h, C.; Azoulay, E.; Benoit, D. Attributable mortality of ventilator-associated pneumonia: A reappraisal using causal analysis. Am. J. Respir. Crit. Care Med. 2011, 184, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Bercault, N.; Wolf, M.; Runge, I.; Fleury, J.C.; Boulain, T. Intrahospital transport of critically ill ventilated patients: A risk factor for ventilator-associated pneumonia—A matched cohort study. Crit. Care Med. 2005, 33, 2471–2478. [Google Scholar] [CrossRef] [PubMed]
- Berrouane, Y.; Daudenthun, I.; Riegel, B.; Emery, M.N.; Martin, G.; Krivosic, R.; Grandbastien, B. Early onset pneumonia in neurosurgical intensive care unit patients. J. Hosp. Infect. 1998, 40, 275–280. [Google Scholar] [CrossRef]
- Bornstain, C.; Azoulay, E.; De Lassence, A.; Cohen, Y.; Costa, M.A.; Mourvillier, B.; Descorps-Declere, A.; Garrouste-Orgeas, M.; Thuong, M.; Schlemmer, B.; et al. Sedation, sucralfate, and antibiotic use are potential means for protection against early-onset ventilator-associated pneumonia. Clin. Infect. Dis. 2004, 38, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Bregeon, F.; Papazian, L.; Visconti, A.; Gregoire, R.; Thirion, X.; Gouin, F. Relationship of microbiologic diagnostic criteria to morbidity and mortality in patients with ventilator-associated pneumonia. JAMA 1997, 277, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Bronchard, R.; Albaladejo, P.; Brezac, G.; Geffroy, A.; Seince, P.F.; Morris, W.; Branger, C.; Marty, J. Early onset pneumonia: Risk factors and consequences in head trauma patients. Anesthesiologists 2004, 100, 234–239. [Google Scholar] [CrossRef]
- Chastre, J.; Trouillet, J.L.; Vuagnat, A.; Joly-Guillou, M.L.; Clavier, H.; Dombret, M.C.; Gibert, C. Nosocomial pneumonia in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1998, 157, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Daschner, F.; Kappstein, I.; Schuster, F.; Scholz, R.; Bauer, E.; Jooβens, D.; Just, H. Influence of disposable (‘Conchapak’) and reusable humidifying systems on the incidence of ventilation pneumonia. J. Hosp. Infect. 1988, 11, 161–168. [Google Scholar] [CrossRef]
- Duszyńska, W.; Rosenthal, V.D.; Dragan, B.; Węgrzyn, P.; Mazur, A.; Wojtyra, P.; Tomala, A.; Kübler, A. Ventilator-associated pneumonia monitoring according to the INICC project at one centre. Anaesthesiol. Intensive Ther. 2015, 47, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Fagon, J.Y.; Chastre, J.; Domart, Y.; Trouillet, J.L.; Pierre, J.; Darne, C.; Gibert, C. Nosocomial pneumonia in patients receiving continuous mechanical ventilation. Prospective analysis of 52 episodes with use of a protected specimen brush and quantitative culture techniques. Am. Rev. Respir. Dis. 1989, 139, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Gacouin, A.; Barbarot, N.; Camus, C.; Salomon, S.; Isslame, S.; Marque, S.; Lavoué, S.; Donnio, P.Y.; Thomas, R.; Le Tulzo, Y. Late-onset ventilator-associated pneumonia in nontrauma intensive care unit patients. Anesth. Analg. 2009, 109, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Garrouste-Orgeas, M.; Chevret, S.; Arlet, G.; Marie, O.; Rouveau, M.; Popoff, N.; Schlemmer, B. Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients. A prospective study based on genomic DNA analysis. Am. J. Respir. Crit. Care Med. 1997, 156, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Georges, H.; Leroy, O.; Guery, B.; Alfandari, S.; Beaucaire, G. Predisposing factors for nosocomial pneumonia in patients receiving mechanical ventilation and requiring tracheotomy. Chest 2000, 118, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Giard, M.; Lepape, A.; Allaouchiche, B.; Guerin, C.; Lehot, J.J.; Robert, M.O.; Fournier, G.; Jacques, D.; Chassard, D.; Gueugniaud, P.Y.; et al. Early-and late-onset ventilator-associated pneumonia acquired in the intensive care unit: Comparison of risk factors. J. Crit. Care 2008, 23, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Gruson, D.; Hilbert, G.; Vargas, F.; Valentino, R.; Bebear, C.; Allery, A.; Bebear, C.; Gbikpi-benissan, G.E.; Cardinaud, J.P. Rotation and restricted use of antibiotics in a medical intensive care unit: Impact on the incidence of ventilator-associated pneumonia caused by antibiotic-resistant gram-negative bacteria. Am. J. Respir. Crit. Care Med. 2000, 162, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Gruson, D.; Hilbert, G.; Vargas, F.; Valentino, R.; Bui, N.; Pereyre, S.; Bebear, C.; Bebear, C.M.; Gbikpi-Benissan, G. Strategy of antibiotic rotation: Long-term effect on incidence and susceptibilities of Gram-negative bacilli responsible for ventilator-associated pneumonia. Crit. Care Med. 2003, 31, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Guerin, C.; Girard, R.; Chemorin, C.; De Varax, R.; Fournier, G. Facial mask noninvasive mechanical ventilation reduces the incidence of nosocomial pneumonia. Intensive Care Med. 1997, 23, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Hugonnet, S.; Uçkay, I.; Pittet, D. Staffing level: A determinant of late-onset ventilator-associated pneumonia. Crit. Care 2007, 11, R80. [Google Scholar] [CrossRef] [PubMed]
- Hyllienmark, P.; Gardlund, B.; Persson, J.O.; Ekdahl, K. Nosocomial pneumonia in the ICU: A prospective cohort study. Scand. J. Infect. Dis. 2007, 39, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Jaillette, E.; Nseir, S. Relationship between inhaled β2-agonists and ventilator-associated pneumonia: A cohort study. Crit. Care Med. 2011, 39, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, A.; Schwab, F.; Behnke, M.; Geffers, C.; Gastmeier, P. Pneumonia associated with invasive and noninvasive ventilation: An analysis of the German nosocomial infection surveillance system database. Intensive Care Med. 2010, 36, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Kolpa, M.; Walaszek, M.; Gniadek, A.; Wolak, Z.; Dobros, W. Incidence, Microbiological Profile and Risk Factors of Healthcare-Associated Infections in Intensive Care Units: A 10 Year Observation in a Provincial Hospital in Southern Poland. Int. J. Environ. Res. Public Health 2018, 15, 112. [Google Scholar] [CrossRef] [PubMed]
- Lepelletier, D.; Roquilly, A.; Mahe, P.J.; Loutrel, O.; Champin, P.; Corvec, S.; Naux, E.; Pinaud, M.; Lejus, C.; Asehnoune, K. Retrospective analysis of the risk factors and pathogens associated with early-onset ventilator-associated pneumonia in surgical-ICU head-trauma patients. J. Neurosurg. Anesthesiol. 2010, 22, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Luyt, C.E.; Guérin, V.; Combes, A.; Trouillet, J.L.; Ayed, S.B.; Bernard, M.; Gibert, C.; Chastre, J. Procalcitonin kinetics as a prognostic marker of ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Magnason, S.; Kristinsson, K.G.; Stefansson, T.; Erlendsdottir, H.; Jonsdottir, K.; Kristjansson, M.; Gudmundsson, S. Risk factors and outcome in ICU-acquired infections. Acta Anaesthesiol. Scand. 2008, 52, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Mahul, P.; Auboyer, C.; Jospe, R.; Ros, A.; Guerin, C.; el Khouri, Z.; Galliez, M.; Dumont, A.; Gaudin, O. Prevention of nosocomial pneumonia in intubated patients respective role of mechanical subglottic secretions drainage and stress ulcer prophylaxis. Intensive Care Med. 1992, 18, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Markowicz, P.; Wolff, M.; Djedaini, K.; Cohen, Y.; Chastre, J.; Delclaux, C. Multicenter prospective study of ventilator-associated pneumonia during acute respiratory distress syndrome. Incidence, prognosis, and risk factors. Am. J. Respir. Crit. Care Med. 2000, 161, 1942–1948. [Google Scholar] [CrossRef] [PubMed]
- Michel, F.; Franceschini, B.; Berger, P.; Arnal, J.M.; Gainnier, M.; Sainty, J.M.; Papazian, L. Early antibiotic treatment for BAL-confirmed ventilator-associated pneumonia: A role for routine endotracheal aspirate cultures. Chest 2005, 127, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Moine, P.; Timsit, J.F.; De Lassence, A.; Troché, G.; Fosse, J.P.; Alberti, C.; Cohen, Y. Mortality associated with late-onset pneumonia in the intensive care unit: Results of a multi-center cohort study. Intensive Care Med. 2002, 28, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Myny, D.; Depuydt, P.; Colardyn, F.; Blot, S. Ventilator-associated pneumonia in a tertiary care ICU analysis of risk factors for acquisition and mortality. Acta Clin. Belg. 2005, 60, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Nguile-Makao, M.; Zahar, J.R.; Français, A.; Tabah, A.; Garrouste-Orgeas, M.; Allaouchiche, B.; Goldgran-Toledano, D.; Azoulay, E.; Adrie, C.; Jamali, S.; et al. Attributable mortality of ventilator-associated pneumonia: Respective impact of main characteristics at ICU admission and VAP onset using conditional logistic regression and multi-state models. Intensive Care Med. 2010, 36, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.L.; Røder, B.; Magnussen, P.; Engquist, A.; Frimodt-møller, N. Nosocomial pneumonia in an intensive care unit in a Danish university hospital: Incidence, mortality and etiology. Scand. J. Infect. Dis. 1992, 24, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Nseir, S.; Di Pompeo, C.; Soubrier, S.; Cavestri, B.; Jozefowicz, E.; Saulnier, F.; Durocher, A. Impact of ventilator-associated pneumonia on outcome in patients with COPD. Chest 2005, 128, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Bregeon, F.; Thirion, X.; Gregoire, R.; Saux, P.; Denis, J.P.; Perin, G.; Charrel, J.; Dumon, J.F.; Affray, J.P.; et al. Effect of ventilator-associated pneumonia on mortality and morbidity. Am. J. Respir. Crit. Care Med. 1996, 154, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Reusser, P.; Zimmerli, W.; Scheidegger, D.; Marbet, G.A.; Buser, M.; Gyr, K. Role of gastric colonization in nosocomial infections and endotoxemia: A prospective study in neurosurgical patients on mechanical ventilation. J. Infect. Dis. 1989, 160, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Stéphan, F.; Mabrouk, N.; Decailliot, F.; Delclaux, C.; Legrand, P. Ventilator-associated pneumonia leading to acute lung injury after trauma: Importance of Haemophilus influenzae. Anesthesiology 2006, 104, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.F.; Chevret, S.; Valcke, J.; Misset, B.; Renaud, B.; Goldstein, F.W.; Vaury, P.; Carlet, J. Mortality of nosocomial pneumonia in ventilated patients: Influence of diagnostic tools. Am. J. Respir. Crit. Care Med. 1996, 154, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Trouillet, J.L.; Chastre, J.; Vuagnat, A.; Joly-Guillou, M.L.; Combaux, D.; Dombret, M.C.; Gibert, C. Ventilator-associated pneumonia caused by potentially drug-resistant bacteria. Am. J. Respir. Crit. Care Med. 1998, 157, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Vanhems, P.; Bénet, T.; Voirin, N.; Januel, J.M.; Lepape, A.; Allaouchiche, B.; Argaud, L.; Chassard, D.; Guérin, C. Early-onset ventilator-associated pneumonia incidence in intensive care units: A surveillance-based study. BMC Infect. Dis. 2011, 11, 236. [Google Scholar] [CrossRef] [PubMed]
- Verhamme, K.M.; De Coster, W.; De Roo, L.; De Beenhouwer, H.; Nollet, G.; Verbeke, J.; Demeyer, I.; Jordens, P. Pathogens in early-onset and late-onset intensive care unit–acquired pneumonia. Infect. Control Hosp. Epidemiol. 2007, 28, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Woske, H.J.; Röding, T.; Schulz, I.; Lode, H. Ventilator-associated pneumonia in a surgical intensive care unit Epidemiology, etiology and comparison of three bronchoscopic methods for microbiological specimen sampling. Crit. Care 2001, 5, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Zahar, J.R.; Nguile-Makao, M.; Français, A.; Schwebel, C.; Garrouste-Orgeas, M.; Goldgran-Toledano, D.; Azoulay, E.; Thuong, M.; Jamali, S.; Cohen, Y.; et al. Predicting the risk of documented ventilator-associated pneumonia for benchmarking: Construction and validation of a score. Crit. Care Med. 2009, 37, 2545–2551. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lerma, F. ICU-acquired Pneumonia Study Group. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. Intensive Care Med. 1996, 22, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Moro, M.L.; Capelli, O.; De Blasi, R.A.; D’Errico, R.R.; Conti, G.; Bufi, M.; Gasparetto, A. Risk factors for early onset pneumonia in trauma patients. Chest 1994, 105, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulou, E.; Bakakos, P.; Katostaras, T.; Gregorakos, L. Incidence and risk factors for ventilator-associated pneumonia in 4 multidisciplinary intensive care units in Athens, Greece. Respir. Care 2003, 48, 681–688. [Google Scholar] [PubMed]
- Bouza, E.; Pérez, A.; Muñoz, P.; Perez, M.J.; Rincón, C.; Sánchez, C.; Martín-Rabadán, P.; Riesgo, M.; Cardiovascular Infection Study Group. Ventilator-associated pneumonia after heart surgery: A prospective analysis and the value of surveillance. Crit. Care Med. 2003, 31, 1964–1970. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, M.; Ferrer, M.; Ferrer, R.; Morforte, R.; Garnacho, A.; Torres, A. Risk and prognostic factors of ventilator-associated pneumonia in trauma patients. Crit. Care Med. 2006, 34, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Cendrero, J.A.; Solé-Violán, J.; Benitez, A.B.; Catalán, J.N.; Fernández, J.A.; Santana, P.S.; de Castro, F.R. Role of different routes of tracheal colonization in the development of pneumonia in patients receiving mechanical ventilation. Chest 1999, 116, 462–470. [Google Scholar] [CrossRef]
- Chaari, A.; El Habib, M.; Ghdhoun, H.; Algia, N.B.; Chtara, K.; Hamida, C.B.; Chelly, H.; Bahloul, M.; Bouaziz, M. Does low-dose hydrocortisone therapy prevent ventilator-associated pneumonia in trauma patients? Am. J. Ther. 2015, 22, 22–28. [Google Scholar] [CrossRef] [PubMed]
- De Latorre, F.J.; Pont, T.; Ferrer, A.; Rosselló, J.; Palomar, M.; Planas, M. Pattern of tracheal colonization during echanical ventilation. Am. J. Respir. Crit. Care Med. 1995, 152, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Ewig, S.; Torres, A.; El-Ebiary, M.; Fàbregas, N.; Hernandez, C.; Gonzalez, J.; Nicolas, J.M.; Soto, L. Bacterial colonization patterns in mechanically ventilated patients with traumatic and medical head injury. Incidence, risk factors, and association with ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 1999, 159, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Hortal, J.; Giannella, M.; Pérez, M.J.; Barrio, J.M.; Desco, M.; Bouza, E.; Muñoz, P. Incidence and risk factors for ventilator-associated pneumonia after major heart surgery. Intensive Care Med. 2009, 35, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, J.; Peñafiel, A.; Marsé, P.; Jordá, R.; Raurich, J.M.; Mata, F. Incidence of gastroesophageal reflux and aspiration in mechanically ventilated patients using small-bore nasogastric tubes. J. Parenter. Enter. Nutr. 2000, 24, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, P.A.; Torres, A.; Rodríguez-Roisin, R.O.; Aznar, R.; Gatell, J.M.; Agusti-Vidal, A. Incidence and etiology of pneumonia acquired during mechanical ventilation. Crit. Care Med. 1989, 17, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Kallel, H.; Chelly, H.; Bahloul, M.; Ksibi, H.; Dammak, H.; Chaari, A.; Hamida, C.B.; Rekik, N.; Bouaziz, M. The effect of ventilator-associated pneumonia on the prognosis of head trauma patients. J. Trauma Acute Care Surg. 2005, 59, 705–710. [Google Scholar]
- Piazza, O.; Iasiello, A.; PapaIanni, C.; De Robertis, E.; Servillo, G.; Rossano, F.; Tufano, R. Incidence of antimicrobial-resistant ventilator-associated pneumonia: An eighteen-month survey. Panminerva Med. 2005, 47, 265–267. [Google Scholar] [PubMed]
- Raineri, E.; Crema, L.; Dal Zoppo, S.; Acquarolo, A.; Pan, A.; Carnevale, G.; Albertario, F.; Candiani, A. Rotation of antimicrobial therapy in the intensive care unit: Impact on incidence of ventilator-associated pneumonia caused by antibiotic-resistant Gram-negative bacteria. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.; Lopez-Ferraz, C.; Gordon, M.; Gimeno, A.; Villarreal, E.; Ruiz, J.; Menendez, R.; Torres, A. From starting mechanical ventilation to ventilator-associated pneumonia, choosing the right moment to start antibiotic treatment. Crit. Care 2016, 20, 169. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Quintana, E.; Ausina, V.; Castella, J.; Luquin, M.; Net, A.; Prats, G. Incidence, etiology, and outcome of nosocomial pneumonia in mechanically ventilated patients. Chest 1991, 100, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Ausina, V.; Castella, J.; Net, A.; Prats, G. Nosocomial respiratory tract infections in multiple trauma patients: Influence of level of consciousness with implications for therapy. Chest 1992, 102, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Sonora, R.; Jubert, P.; Artigas, A.; Rué, M.; Vallés, J. Pneumonia in intubated patients: Role of respiratory airway care. Am. J. Respir. Crit. Care Med. 1996, 154, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Lorente, C.; Diaz, E.; Bodi, M.; Boque, C.; Sandiumenge, A.; Santamaria, J.M. Incidence, etiology, and outcome of nosocomial pneumonia in ICU patients requiring percutaneous tracheotomy for mechanical ventilation. Chest 2003, 124, 2239–2243. [Google Scholar] [CrossRef] [PubMed]
- Rincón-Ferrari, M.D.; Flores-Cordero, J.M.; Leal-Noval, S.R.; Murillo-Cabezas, F.; Cayuelas, A.; Muñoz-Sánchez, M.A.; Sánchez-Olmedo, J.I. Impact of ventilator-associated pneumonia in patients with severe head injury. J. Trauma Acute Care Surg. 2004, 57, 1234–1240. [Google Scholar] [CrossRef]
- Ruiz-Santana, S.E.; García, A.J.; Esteban, A.N.; Guerra, L.; Alvarez, B.E.; Corcia, S.A.; Gudin, J.; Martinez, A.; Quintana, E.; Armengol, S. ICU pneumonias: A multi-institutional study. Crit. Care Med. 1987, 15, 930–932. [Google Scholar] [CrossRef] [PubMed]
- Sofianou, D.C.; Constandinidis, T.C.; Yannacou, M.; Anastasiou, H.; Sofianos, E. Analysis of risk factors for ventilator-associated pneumonia in a multidisciplinary intensive care unit. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Tamayo, E.; Álvarez, F.J.; Martínez-Rafael, B.; Bustamante, J.; Bermejo-Martin, J.F.; Fierro, I.; Eiros, J.M.; Castrodeza, J.; Heredia, M.; Gómez-Herreras, J.I.; et al. Ventilator-associated pneumonia is an important risk factor for mortality after major cardiac surgery. J. Crit. Care 2012, 27, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Artigas, A.T.; Dronda, S.B.; Vallés, E.C.; Marco, J.M.; Usón, M.C.; Figueras, P.; Suarez, F.J.; Hernandez, A. Risk factors for nosocomial pneumonia in critically ill trauma patients. Crit. Care Med. 2001, 29, 304–309. [Google Scholar] [CrossRef]
- Torres, A.; Aznar, R.; Gatell, J.M.; Jiménez, P.; González, J.; Ferrer, A.; Celis, R.; Rodriguez-Roisin, R. Incidence, risk, and prognosis factors of nosocomial pneumonia in mechanically ventilated patients. Am. Rev. Respir. Dis. 1990, 142, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Urli, T.; Perone, G.; Acquarolo, A.; Zappa, S.; Antonini, B.; Candiani, A. Surveillance of infections acquired in intensive care: Usefulness in clinical practice. J. Hosp. Infect. 2002, 52, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Valles, J.; Pobo, A.; Garcia-Esquirol, O.; Mariscal, D.; Real, J.; Fernandez, R. Excess ICU mortality attributable to ventilator-associated pneumonia: The role of early vs. late onset. Intensive Care Med. 2007, 33, 1363. [Google Scholar] [CrossRef] [PubMed]
- Violan, J.S.; Sanchez-Ramirez, C.; Mujica, A.P.; Cendrero, J.C.; Fernandez, J.A.; de Castro, F.R. Impact of nosocomial pneumonia on the outcome of mechanically-ventilated patients. Crit. Care 1998, 2, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Apisarnthanarak, A.; Pinitchai, U.; Thongphubeth, K.; Yuekyen, C.; Warren, D.K.; Zack, J.E.; Warachan, B.; Fraser, V.J. Effectiveness of an educational program to reduce ventilator-associated pneumonia in a tertiary care center in Thailand: A 4-year study. Clin. Infect. Dis. 2007, 45, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Mallick, U.K.; Faruq, M.O.; Ahsan, A.A.; Fatema, K.; Ahmed, F.; Asaduzzaman, M.; Islam, M.; Sultana, A. Spectrum of Early Onset and Late Onset Ventilator Associated Pneumonia (VAP) in a Tertiary Care Hospital of Bangladesh: A Prospective Cohort Study. Bangladesh Crit. Care J. 2015, 3, 9–13. [Google Scholar] [CrossRef]
- Noor, A.; Hussain, S.F. Risk factors associated with development of ventilator-associated pneumonia. J. Coll. Phys. Surg. Pak. 2005, 15, 92–95. [Google Scholar]
- Pawar, M.; Mehta, Y.; Khurana, P.; Chaudhary, A.; Kulkarni, V.; Trehan, N. Ventilator-associated pneumonia: Incidence, risk factors, outcome, and microbiology. J. Cardiothorac. Vasc. Anesth. 2003, 17, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Salahuddin, N.; Zafar, A.; Sukhyani, L.; Rahim, S.; Noor, M.F.; Hussain, K.; Siddiqui, S.; Islam, M.; Husain, S.J. Reducing ventilator-associated pneumonia rates through a staff education programme. J. Hosp. Infect. 2004, 57, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Zhu, S.; Yan, D.; Chen, W.; Chen, R.; Zou, J.; Yan, J.; Zhang, X.; Farmakiotis, D.; Mylonakis, E. Candida spp. airway colonization: A potential risk factor for Acinetobacter baumannii ventilator-associated pneumonia. Sabouraudia 2016, 54, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Hu, B.; Rosenthal, V.D.; Gao, X.; He, L. Device-associated infection rates in 398 intensive care units in Shanghai, China: International Nosocomial Infection Control Consortium (INICC) findings. Int. J. Infect. Dis. 2011, 15, e774–e780. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Hu, B.; Rosenthal, V.D.; Zhang, Y.; Gao, X.; He, L. Impact of a multidimensional approach on ventilator-associated pneumonia rates in a hospital of Shanghai: Findings of the International Nosocomial Infection Control Consortium. J. Crit. Care 2012, 27, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Thongpiyapoom, S.; Narong, M.N.; Suwalak, N.; Jamulitrat, S.; Intaraksa, P.; Boonrat, J.; Kasatpibal, N.; Unahalekhaka, A. Device-associated infections and patterns of antimicrobial resistance in a medical-surgical intensive care unit in a university hospital in Thailand. J. Med. Assoc. Thail. 2004, 87, 819–824. [Google Scholar]
- Xie, D.S.; Xiong, W.; Lai, R.P.; Liu, L.; Gan, X.M.; Wang, X.H.; Wang, M.; Lou, Y.X.; Fu, X.Y.; Wang, H.F.; et al. Ventilator-associated pneumonia in intensive care units in Hubei Province, China: A multicentre prospective cohort survey. J. Hosp. Infect. 2011, 78, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Ertugrul, B.M.; Yildirim, A.; Ay, P.; Oncu, S.; Cagatay, A.; Cakar, N.; Ertekin, C.; Ozsut, H.; Eraksoy, H.; Calangu, S. Ventilator-associated pneumonia in surgical emergency intensive care unit. Saudi Med. J. 2006, 27, 52–57. [Google Scholar] [PubMed]
- Gursel, G.; Aydogdu, M.; Nadir Ozis, T.; Tasyurek, S. Comparison of the value of initial and serial endotracheal aspirate surveillance cultures in predicting the causative pathogen of ventilator-associated pneumonia. Scand. J. Infect. Dis. 2010, 42, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Chang, R.W.; Lee, B.; Bartlett, F.W. Continuous enteral feeding: A major cause of pneumonia among ventilated intensive care unit patients. J. Parenter. Enter. Nutr. 1990, 14, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Jahani-Sherafat, S.; Razaghi, M.; Rosenthal, V.D.; Tajeddin, E.; Seyedjavadi, S.; Rashidan, M.; Alebouyeh, M.; Rostampour, M.; Haghi, A.; Sayarbayat, M.; et al. Device-associated infection rates and bacterial resistance in six academic teaching hospitals of Iran: Findings from the International Nocosomial Infection Control Consortium (INICC). J. Infect. Public Health 2015, 8, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Kanafani, Z.A.; Kara, L.; Hayek, S.; Kanj, S.S. Ventilator-associated pneumonia at a tertiary-care center in a developing country: Incidence, microbiology, and susceptibility patterns of isolated microorganisms. Infect. Control Hosp. Epidemiol. 2003, 24, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Leblebicioglu, H.; Rosenthal, V.D.; Arıkan, Ö.A.; Özgültekin, A.; Yalcin, A.N.; Koksal, I.; Usluer, G.; Sardan, Y.C.; Ulusoy, S. Device-associated hospital-acquired infection rates in Turkish intensive care units. Findings of the International Nosocomial Infection Control Consortium (INICC). J. Hosp. Infect. 2007, 65, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Leblebicioglu, H.; Yalcin, A.N.; Rosenthal, V.D.; Koksal, I.; Sirmatel, F.; Unal, S.; Turgut, H.; Ozdemir, D.; Ersoz, G.; Uzun, C.; et al. Effectiveness of a multidimensional approach for prevention of ventilator-associated pneumonia in 11 adult intensive care units from 10 cities of Turkey: Findings of the International Nosocomial Infection Control Consortium (INICC). Infection 2013, 41, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Cunningham, G.; Oni, G.A.; Djazmati, W. The incidence and risk factors of ventilator-associated pneumonia in a Riyadh hospital. Infect. Control Hosp. Epidemiol. 2000, 21, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Rezai, M.S.; Bagheri-Nesami, M.; Nikkhah, A.; Bayg, A.H. Incidence, risk factors, and outcome of ventilator-associated Pneumonia in 18 hospitals of Iran. Running title: Ventilator-associated pneumonia in Iran. Int. J. Adv. Biotechnol. Res. 2016, 7, 936–946. [Google Scholar]
- Şimşek, S.; Yurtseven, N.; Gercekogalu, H.; Izgi, F.; Sohtorik, Ü.; Canik, S.; Özler, A. Ventilator-associated pneumonias in a cardiothoracic surgery centre postoperative intensive care unit. J. Hosp. Infect. 2001, 47, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.E.; Hershow, R.C.; Ramirez, C.A.; Weinstein, R.A. Control of nosocomial infections in an intensive care unit in Guatemala City. Clin. Infect. Dis. 1995, 21, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Guanche-Garcell, H.; Morales-Perez, C.; Rosenthal, V.D. Effectiveness of a multidimensional approach for the prevention of ventilator-associated pneumonia in an adult intensive care unit in Cuba: Findings of the International Nosocomial Infection Control Consortium (INICC). J. Infect. Public Health 2013, 6, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, M.M.; Rocco, J.R. Prevalence of ventilator-associated pneumonia in a university hospital and prognosis for the patients affected. J. Bras. Pneumol. 2006, 32, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Jaimes, F.; De La Rosa, G.; Gómez, E.; Múnera, P.; Ramírez, J.; Castrillón, S. Incidence and risk factors for ventilator-associated pneumonia in a developing country Where is the difference? Respir. Med. 2007, 101, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Luna, C.M.; Blanzaco, D.; Niederman, M.S.; Matarucco, W.; Baredes, N.C.; Desmery, P.; Palizas, F.; Menga, G.; Rios, F.; Apezteguia, C. Resolution of ventilator-associated pneumonia: Prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome. Crit. Care Med. 2003, 31, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.A.; Rosenthal, V.D.; Olarte, N.; Gomez, W.V.; Sussmann, O.; Agudelo, J.G.; Rojas, C.; Osorio, L.; Linares, C.; Valderrama, A.; et al. Device-associated infection rate and mortality in intensive care units of 9 Colombian hospitals: Findings of the International Nosocomial Infection Control Consortium. Infect. Control 2006, 27, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Resende, M.M.; Monteiro, S.G.; Callegari, B.; Figueiredo, P.M.; Monteiro, C.R.; Monteiro-Neto, V. Epidemiology and outcomes of ventilator-associated pneumonia in northern Brazil: An analytical descriptive prospective cohort study. BMC Infect. Dis. 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.M.; Neto, C.; Santos, L.R.; Knibel, M.F. Ventilator-associated pneumonia: Epidemiology and impact on the clinical evolution of ICU patients. J. Bras. Pneumol. 2009, 35, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.M.; Meredith, J.W.; Haponik, E.F. Pneumonia in intubated trauma patients. Microbiology and outcomes. Am. J. Respir. Crit. Care Med. 1996, 153, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Bochicchio, G.V.; Joshi, M.; Bochicchio, K.; Tracy, K.; Scalea, T.M. A time-dependent analysis of intensive care unit pneumonia in trauma patients. J. Trauma 2004, 56, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.R.; Levin, A.B.; Clark, K.L. Role of corticosteroids in the development of pneumonia in mechanically ventilated head-trauma victims. Crit. Care Med. 1986, 14, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.; Norwood, S.; Berne, J. Ventilator-associated pneumonia is more common and of less consequence in trauma patients compared with other critically ill patients. J. Trauma Acute Care Surg. 2010, 69, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Craven, D.E.; Kunches, L.M.; Lichtenberg, D.A.; Kollisch, N.R.; Barry, M.A.; Heeren, T.C.; McCabe, W.R. Nosocomial infection and fatality in medical and surgical intensive care unit patients. Arch. Intern. Med. 1988, 148, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Ensminger, S.A.; Wright, R.S.; Baddour, L.M.; Afess, B. Suspected ventilator-associated pneumonia in cardiac patients admitted to the coronary care unit. Mayo Clin. Proc. 2006, 81, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.L.; Zonies, D.H.; Warner, K.J.; Bulger, E.M.; Sharar, S.R.; Maier, R.V.; Cuschieri, J. Timing of intubation and ventilator-associated pneumonia following injury. Arch. Surg. 2010, 145, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- George, D.L.; Falk, P.S.; Wunderink, R.G.; Leeper Jr, K.V.; Meduri, G.U.; Steere, E.L.; Glen Mayhall, C. Epidemiology of ventilator-acquired pneumonia based on protected bronchoscopic sampling. Am. J. Respir. Crit. Care Med. 1998, 158, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Cook, D.J.; Griffith, L.; Keenan, S.P.; Brun-Buisson, C. The attributable morbidity and mortality of ventilator-associated pneumonia in the critically ill patient. Am. J. Respir. Crit. Care Med. 1999, 159, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.H.; Ward, S.; Sherman, G.; Kollef, M.H. A comparative analysis of patients with early-onset vs late-onset nosocomial pneumonia in the ICU setting. Chest 2000, 117, 1434–1442. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.H.; Hill, C.; Fraser, V.; Kollef, M.H. The Occurrence Of Ventilator-associated Pneumonia (vap) In A Community Hospital: Risk Factors And Clinical Outcomes. Chest 2000, 118, 555–561. [Google Scholar]
- Kasuya, Y.; Hargett, J.L.; Lenhardt, R.; Heine, M.F.; Doufas, A.G.; Remmel, K.S.; Ramirez, J.A.; Akça, O. Ventilator-associated pneumonia in critically ill stroke patients: Frequency, risk factors, and outcomes. J. Crit. Care 2011, 26, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H. Ventilator-associated pneumonia. A multivariate analysis. JAMA 1993, 270, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Silver, P.; Murphy, D.M.; Trovillion, E. The effect of late-onset ventilator-associated pneumonia in determining patient mortality. Chest 1995, 108, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Vlasnik, J.O.; Sharpless, L.; Pasque, C.; Murphy, D.; Fraser, V. Scheduled change of antibiotic classes: A strategy to decrease the incidence of ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 1997, 156, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shapiro, S.D.; Von Harz, B.; Prentice, D.; John, R.S.; Silver, P.; Trovillion, E. Patient transport from intensive care increases the risk of developing ventilator-associated pneumonia. Chest 1997, 112, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Koss, W.G.; Khalili, T.M.; Lemus, J.F.; Chelly, M.M. Nosocomial pneumonia is not prevented by protective contact isolation in the surgical intensive care unit. Am. Surg. 2001, 67, 1140. [Google Scholar] [PubMed]
- Kunac, A.; Sifri, Z.C.; Mohr, A.M.; Horng, H.; Lavery, R.F.; Livingston, D.H. Bacteremia and Ventilator-Associated Pneumonia: A Marker for Contemporaneous Extra-Pulmonic Infection. Surg. Infect. 2014, 15, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Walker, V.; Chen, L.F.; Sexton, D.J.; Anderson, D.J. The epidemiology of ventilator-associated pneumonia in a network of community hospitals: A prospective multicenter study. Infect. Control Hosp. Epidemiol. 2013, 34, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Lowy, F.D.; Carlisle, P.S.; Adams, A.; Feiner, C. The incidence of nosocomial pneumonia following urgent endotracheal intubation. Infect. Control Hosp. Epidemiol. 1987, 8, 245–248. [Google Scholar] [CrossRef]
- Rello, J.; Ollendorf, D.A.; Oster, G.; Vera-Llonch, M.; Bellm, L.; Redman, R.; Kollef, M.H. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 2002, 122, 2115–2121. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.L.; Gibbons, K.J.; Bitzer, L.G.; Dechert, R.E.; Steinberg, S.M.; Flint, L.M. Pneumonia: Incidence, risk factors, and outcome in injured patients. J. Trauma 1991, 31, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Salata, R.A.; Lederman, M.M.; Shlaes, D.M.; Jacobs, M.R.; Eckstein, E.; Tweardy, D.; Toossi, Z.; Chmielewski, R.; Marino, J.; King, C.H. Diagnosis of nosocomial pneumonia in intubated, intensive care unit patients. Am. Rev. Respir. Dis. 1987, 135, 426–432. [Google Scholar] [PubMed]
- Shahin, J.; Bielinski, M.; Guichon, C.; Flemming, C.; Kristof, A.S. Suspected ventilator-associated respiratory infection in severely ill patients: A prospective observational study. Crit. Care 2013, 17, R251. [Google Scholar] [CrossRef] [PubMed]
- Boots, R.J.; Phillips, G.E.; George, N.; Faoagali, J.L. Surveillance culture utility and safety using low-volume blind bronchoalveolar lavage in the diagnosis of ventilator-associated pneumonia. Respirology 2008, 13, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.F.; McOwat, E.; Siganporia, R.; Keighley, C.; Presneill, J.; Sinickas, V. Uncertain relevance of gastric colonization in the seriously ill. Intensive Care Med. 1992, 18, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Potgieter, P.D.; Linton, D.M.; Oliver, S.; Forder, A.A. Nosocomial infections in a respiratory intensive care unit. Crit. Care Med. 1987, 15, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Chastre, J.; Fagon, J.Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Koulenti, D.; Lisboa, T.; Brun-Buisson, C.; Krueger, W.; Macor, A.; Sole-Violan, J.; Diaz, E.; Topeli, A.; DeWaele, J.; Carneiro, A.; et al. Spectrum of practice in the diagnosis of nosocomial pneumonia in patients requiring mechanical ventilation in European intensive care units. Crit. Care Med. 2009, 37, 2360–2369. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shorr, A.; Tabak, Y.P.; Gupta, V.; Liu, L.Z.; Johannes, R.S. Epidemiology and outcomes of healthcare-associated pneumonia. Results from a large US database of culture-positive pneumonia. Chest 2005, 128, 3854–3862. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Torres, A.; Ricart, M.; Valles, J.; Gonzalez, J.; Artigas, A.; Rodriguez-Roisin, R. Ventilator-associated pneumonia by Staphylococcus aureus. Comparison of methicillin-resistant and methicillin-sensitive episodes. Am. J. Respir. Crit. Care Med. 1994, 150, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Koulenti, D.; Tsigou, E.; Rello, J. Nosocomial pneumonia in 27 ICUs in Europe: Perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. World-wide variation in incidence of Acinetobacter associated ventilator-associated pneumonia: A meta-regression. BMC Infect. Dis. 2016, 16, 577. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Sa-Borges, M.; Correa, H.; Leal, S.R.; Baraibar, J. Variations in etiology of ventilator-associated pneumonia across four treatment sites: Implications for antimicrobial prescribing practices. Am. J. Respir. Crit. Care Med. 1999, 160, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. Severe Burns: Pathogenesis and Prevention of Infection. In Recent Clinical Techniques, Results, and Research in Wounds; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Safdar, N.; Dezfulian, C.; Collard, H.R.; Saint, S. Clinical and economic consequences of ventilator-associated pneumonia: A systematic review. Crit. Care Med. 2005, 33, 2184–2193. [Google Scholar] [CrossRef] [PubMed]
- Collard, H.R.; Saint, S.; Matthay, M.A. Prevention of ventilator-associated pneumonia: An evidence-based systematic review. Ann. Intern. Med. 2003, 138, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Melsen, W.G.; Rovers, M.M.; Bonten, M.J. Ventilator-associated pneumonia and mortality: A systematic review of observational studies. Crit. Care Med. 2009, 37, 2709–2718. [Google Scholar] [PubMed]
- Arabi, Y.; Al-Shirawi, N.; Memish, Z.; Anzueto, A. Ventilator-associated pneumonia in adults in developing countries: A systematic review. Int. J. Infect. Dis. 2008, 12, 505–512. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Chen, B.; Li, W.; Yan, J.; Chen, L.; Wang, X.; Xiao, Y. Ventilator-associated pneumonia after cardiac surgery: A meta-analysis and systematic review. J. Thorac. Cardiovasc. Surg. 2014, 148, 3148–3155. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.; Kääriäinen, M.; Kyngäs, H. Effectiveness of educational programmes in preventing ventilator-associated pneumonia: A systematic review. J. Hosp. Infect. 2013, 84, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Zhang, Y.; Yang, Z.; Wang, J.; Jin, A.; Wang, W.; Chen, R.; Zhan, S. Incidence, temporal trend and factors associated with ventilator-associated pneumonia in mainland China: A systematic review and meta-analysis. BMC Infect. Dis. 2017, 17, 468. [Google Scholar] [CrossRef] [PubMed]
- Agrafiotis, M.; Siempos, I.I.; Ntaidou, T.K.; Falagas, M.E. Attributable mortality of ventilator-associated pneumonia: A meta-analysis. Int. J. Tubercul. Lung Dis. 2011, 15, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Ruíz, M.; Torres, A.; Ewig, S.; Marcos, M.A.; Alcón, A.; LLedó, R.; Asenjo, M.A.; Maldonado, A. Noninvasive versus invasive microbial investigation in ventilator-associated pneumonia: Evaluation of outcome. Am. J. Respir. Crit. Care Med. 2000, 162, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. Unusually High Incidences of Staphylococcus aureus Infection within Studies of Ventilator Associated Pneumonia Prevention Using Topical Antibiotics: Benchmarking the Evidence Base. Microorganisms 2018, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. Ventilator Associated Pneumonia prevention methods using topical antibiotics: Herd protection or herd peril? Chest 2014, 146, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. The perfidious effect of topical placebo: A calibration of Staphylococcus aureus Ventilator Associated Pneumonia incidence within Selective Digestive Decontamination (SDD) studies versus the broader evidence base. Antimicrob Agents Chemother. Antimicrob. Agents Chemother. 2013, 57, 4524–4531. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the literature search. MVD, Mechanical Ventilation Days; VAP, Ventilator-Associated Pneumonia; SR/MA, systematic review or meta-analysis.
Figure 1.
Flowchart of the literature search. MVD, Mechanical Ventilation Days; VAP, Ventilator-Associated Pneumonia; SR/MA, systematic review or meta-analysis.
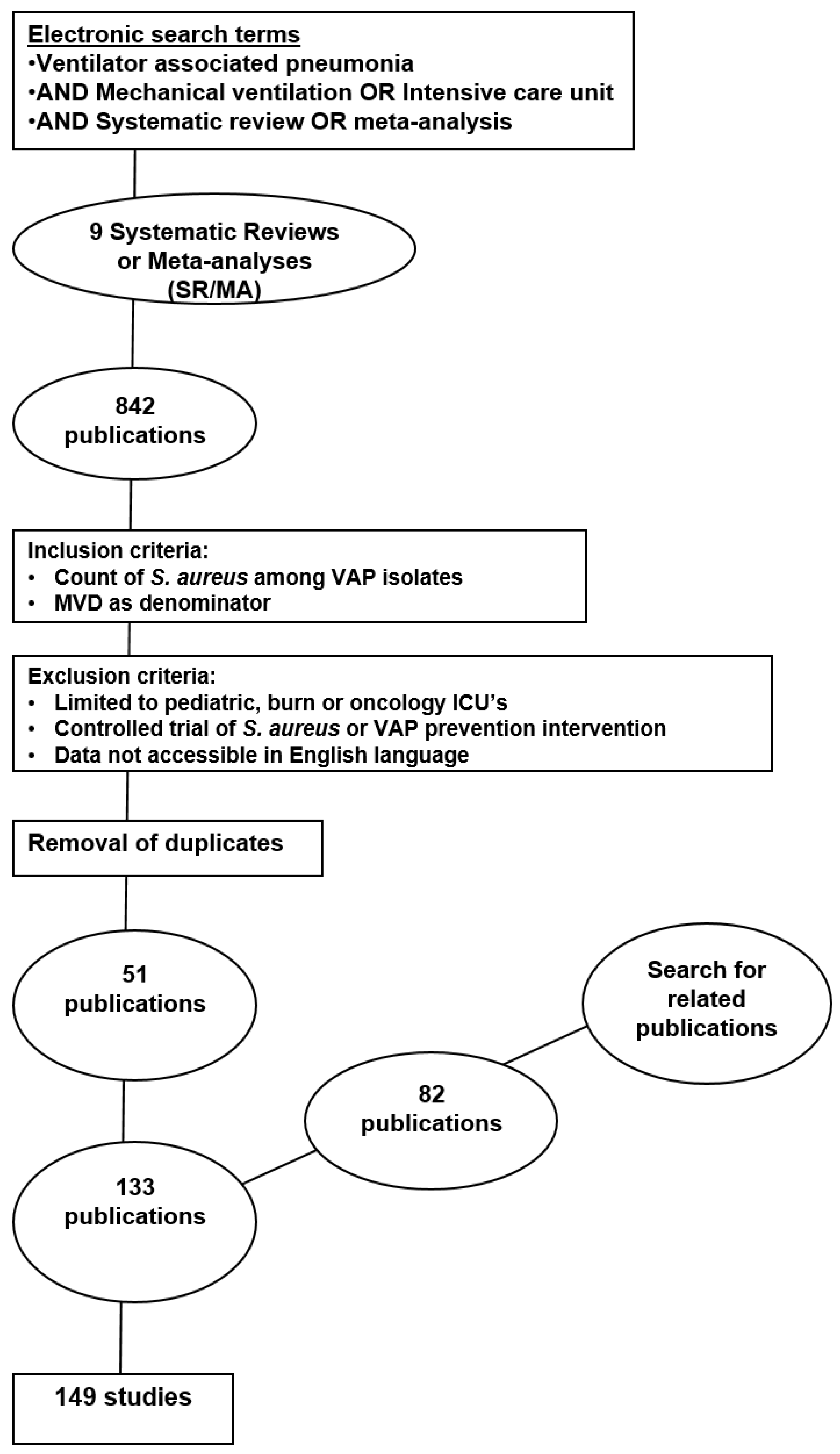
Figure 2.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond, vertical line) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the multinational and ungrouped studies. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
Figure 2.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond, vertical line) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the multinational and ungrouped studies. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
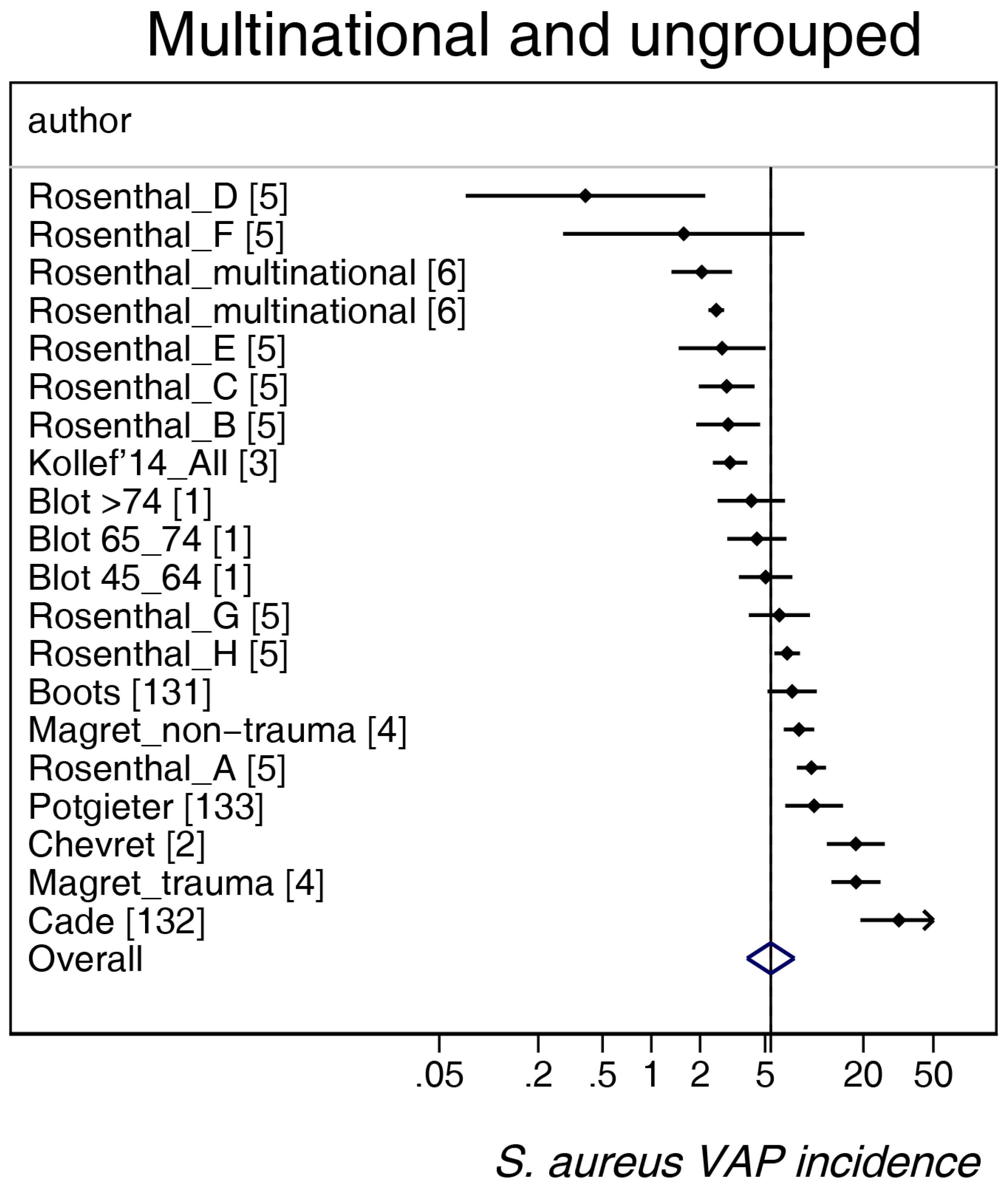
Figure 3.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from Northern European countries. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
Figure 3.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from Northern European countries. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
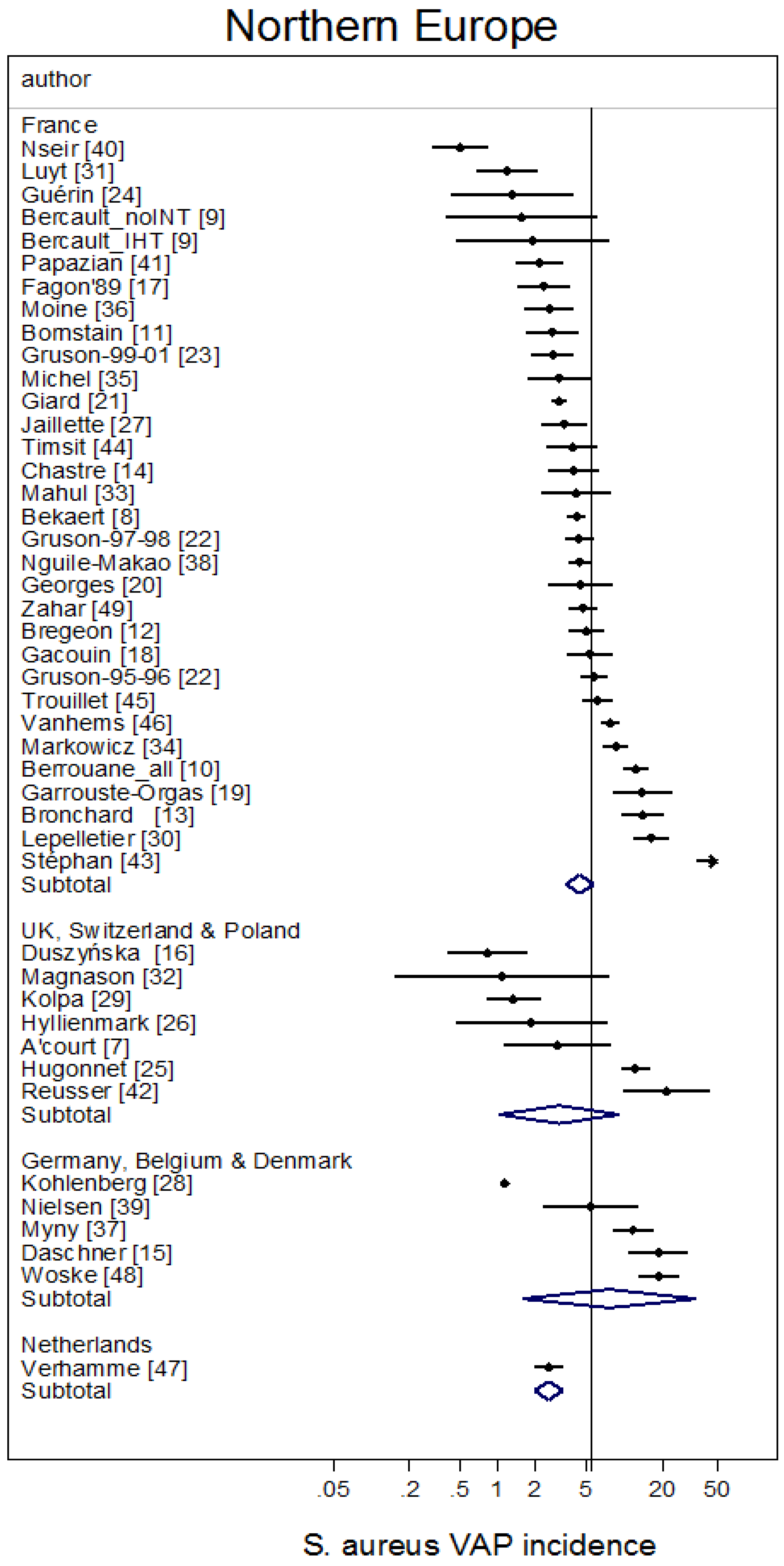
Figure 4.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the Mediterranean studies. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
Figure 4.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the Mediterranean studies. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.

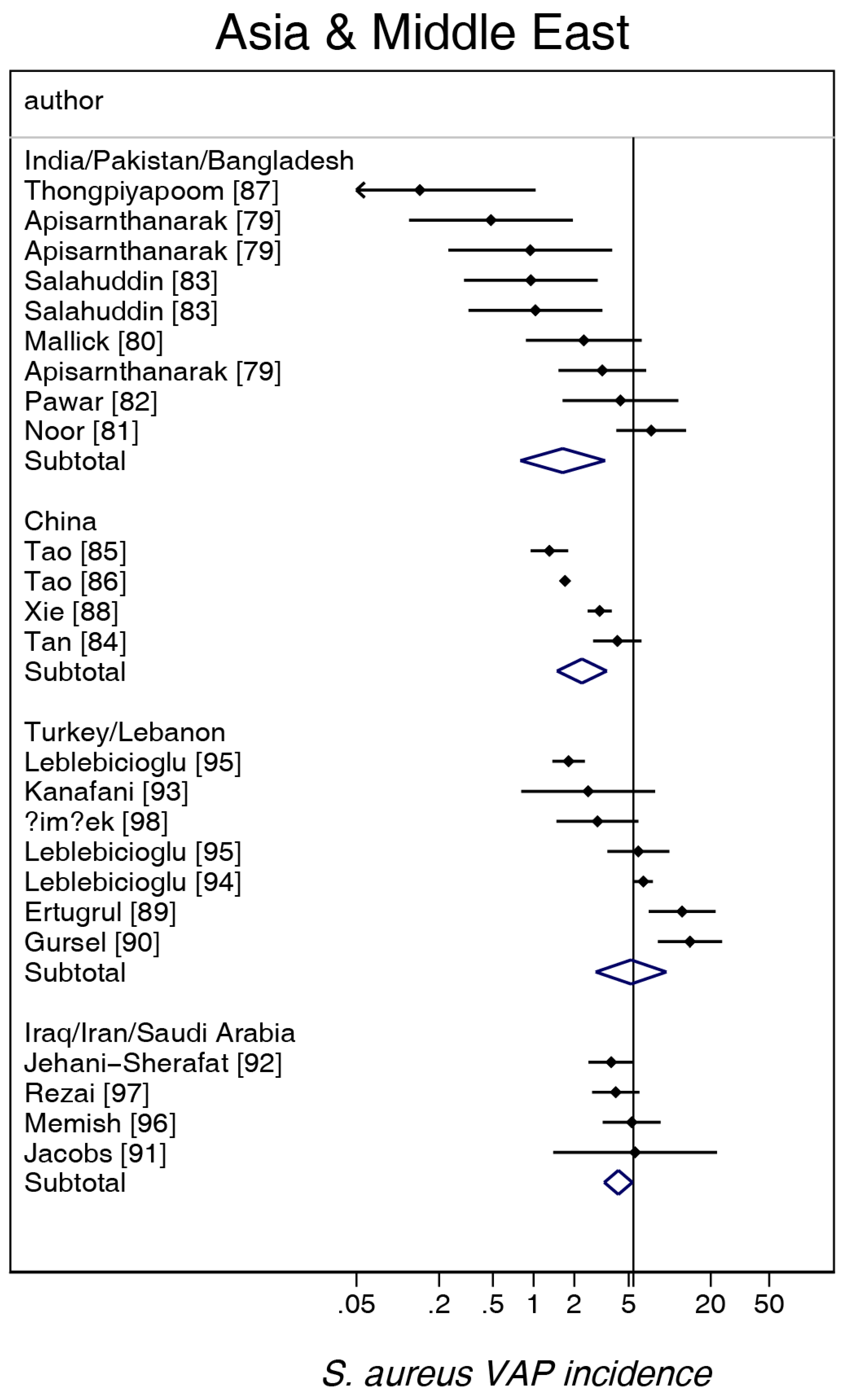
Figure 5.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the studies from Asia and the Middle East. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
Figure 5.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S. aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the studies from Asia and the Middle East. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
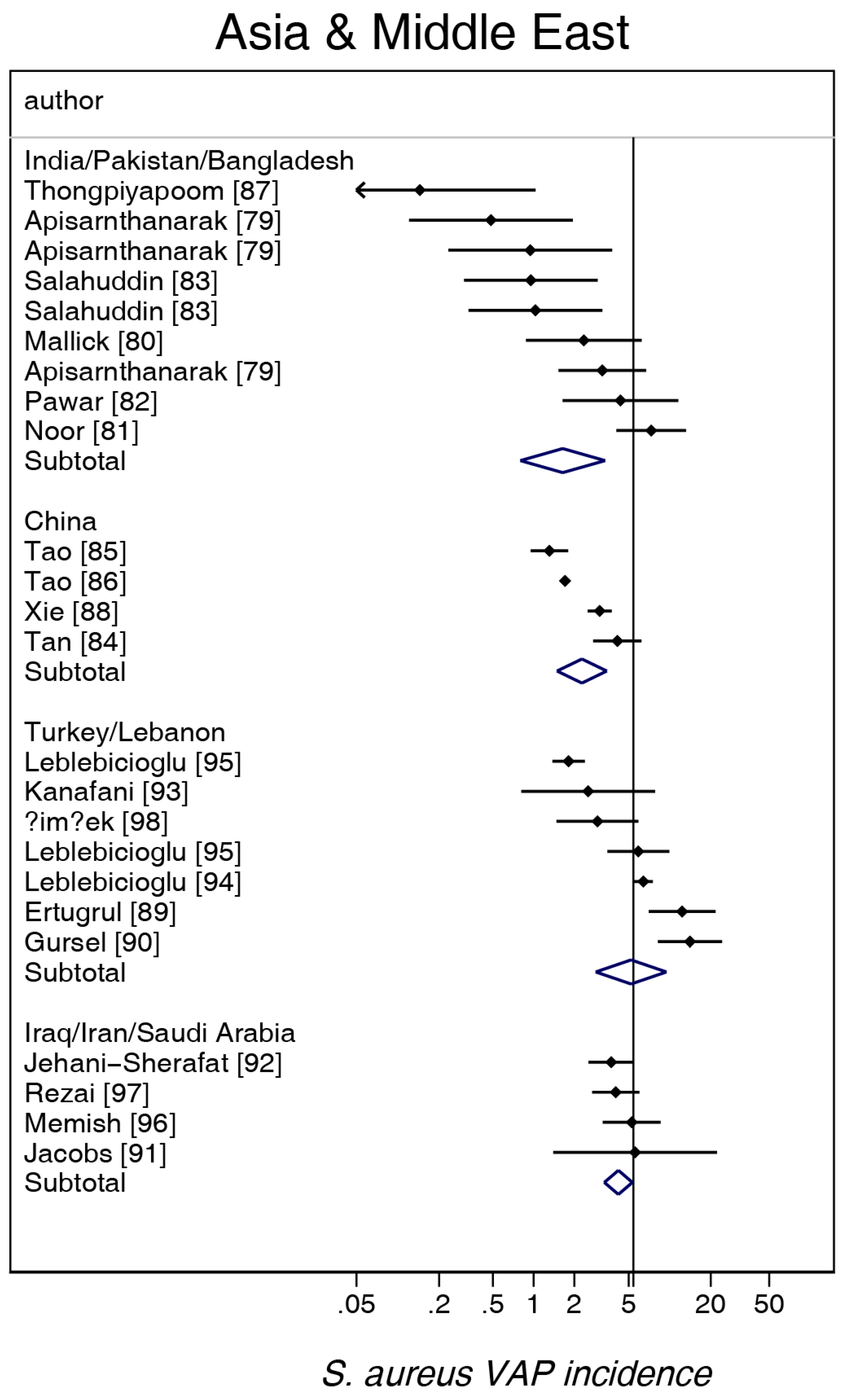
Figure 6.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the North and Central and South American studies. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
Figure 6.
Caterpillar plots of the group-specific (small diamonds) and summary (large open diamond) S aureus VAP incidence per 1000 mechanical ventilation days and 95% CI for groups from the North and Central and South American studies. For comparison, the summary S. aureus VAP incidence (vertical line) derived from the studies in Figure 2 is shown for reference. Studies are listed in Table S1 (see the additional file). Note that the x axis is a logarithmic scale.
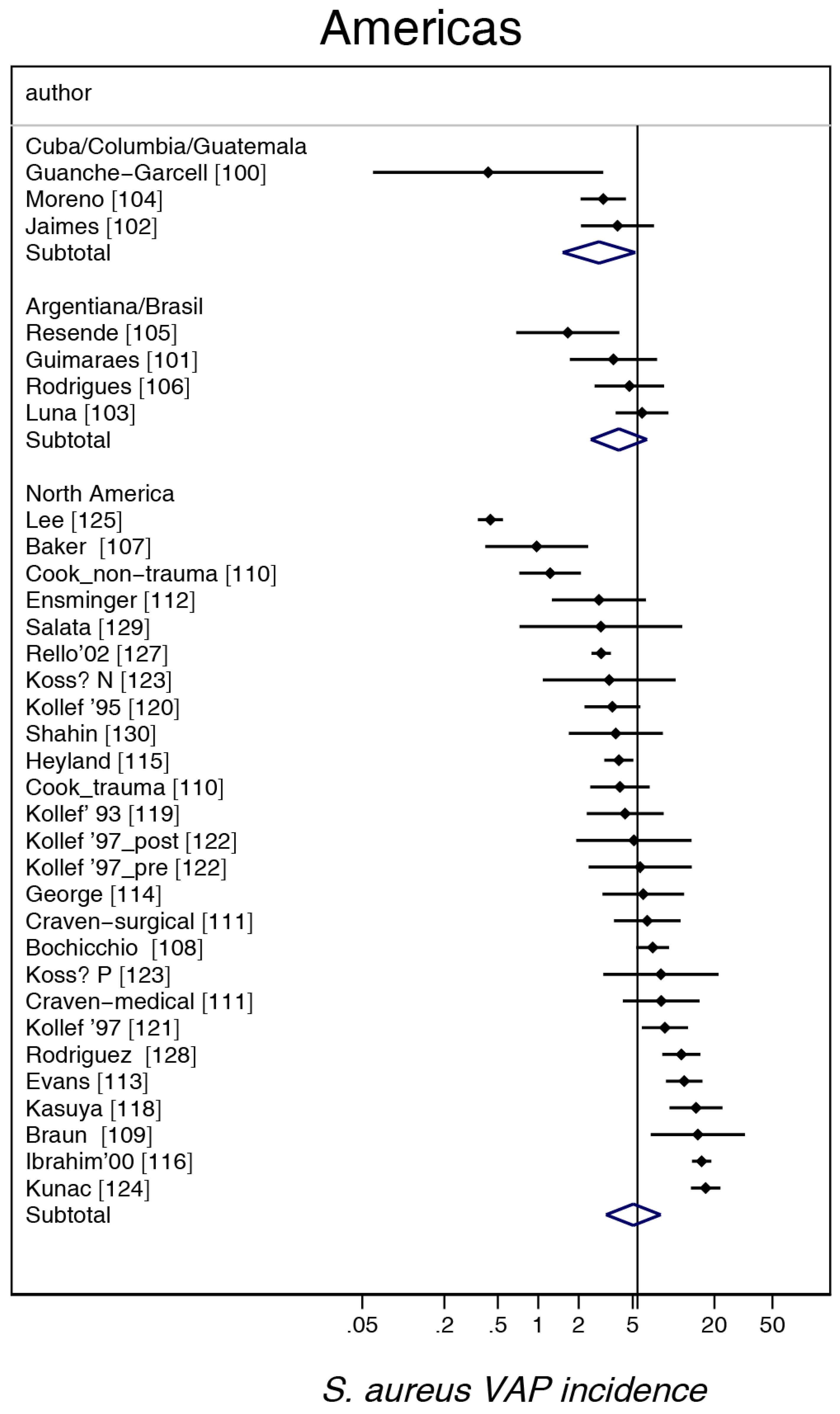
Figure 7.
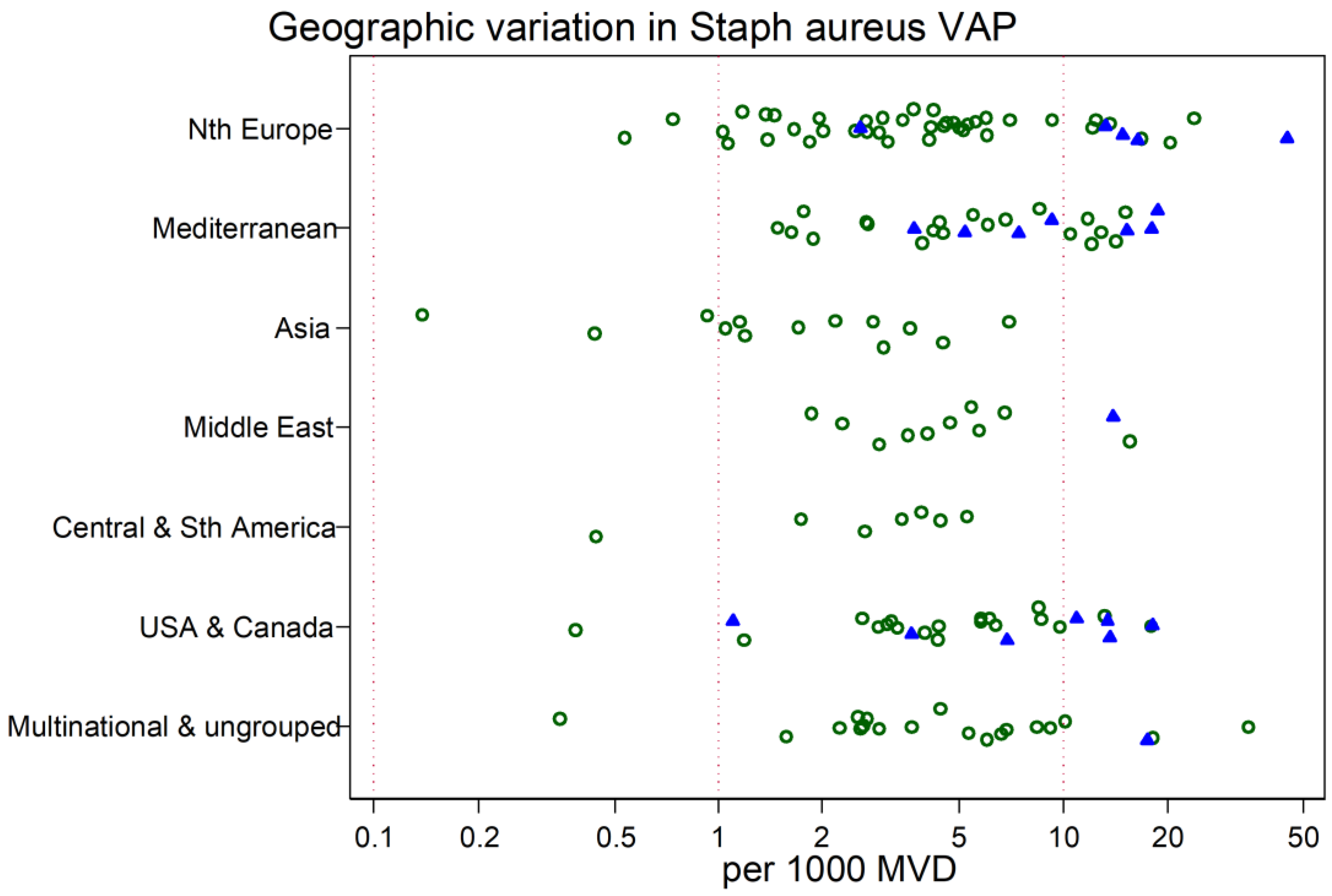
Scatter plot of S. aureus VAP incidence (per 1000 MV days) among published studies in seven geographic regions with rates for studies reporting from trauma ICUs (closed symbols) vs. other ICUs (open symbols). Note the logarithmic scale of incidence. The vertical lines are for reference at incidence rates of 0.1, 1 and 10 per 1000 MV days.
Figure 7.
Scatter plot of S. aureus VAP incidence (per 1000 MV days) among published studies in seven geographic regions with rates for studies reporting from trauma ICUs (closed symbols) vs. other ICUs (open symbols). Note the logarithmic scale of incidence. The vertical lines are for reference at incidence rates of 0.1, 1 and 10 per 1000 MV days.
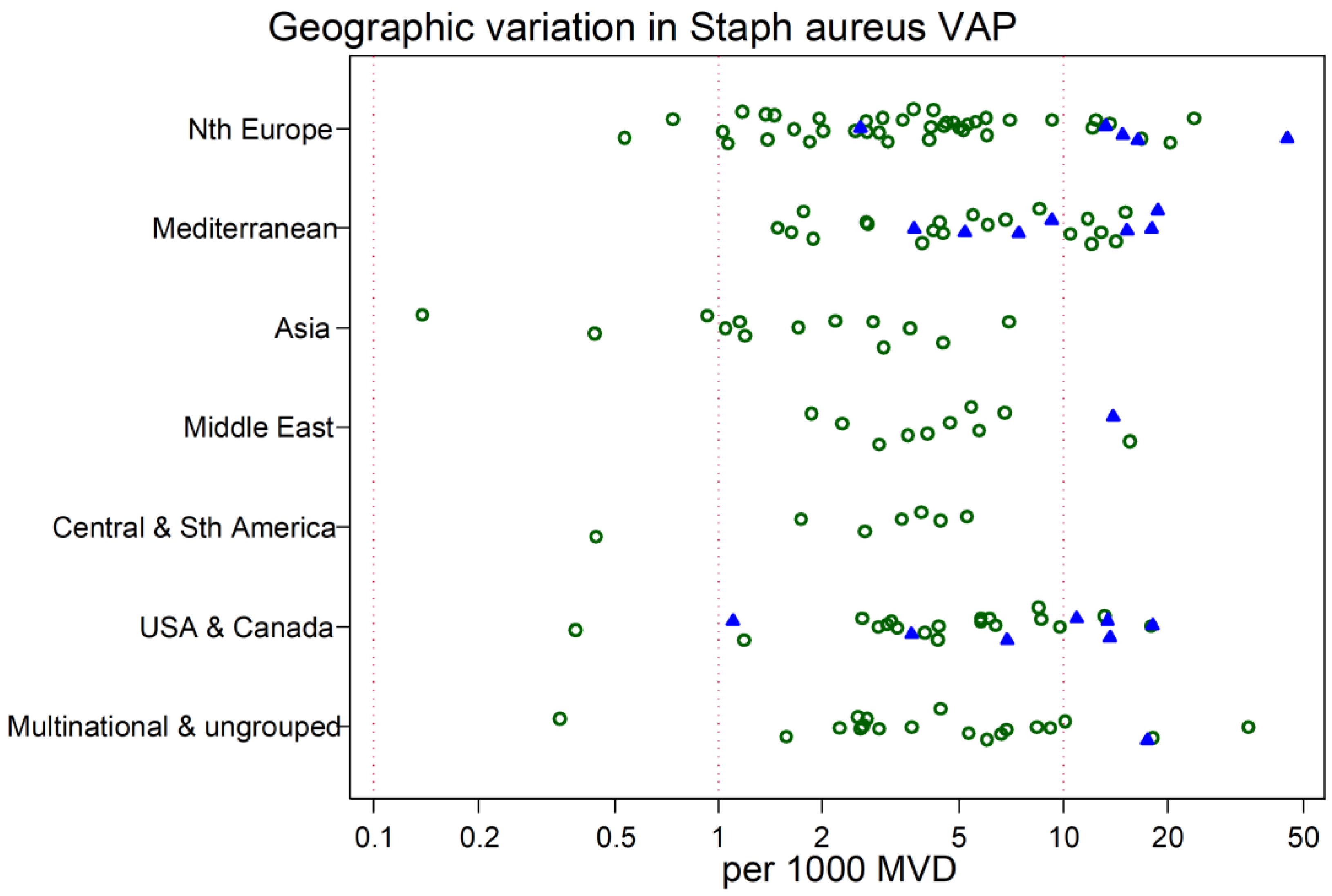
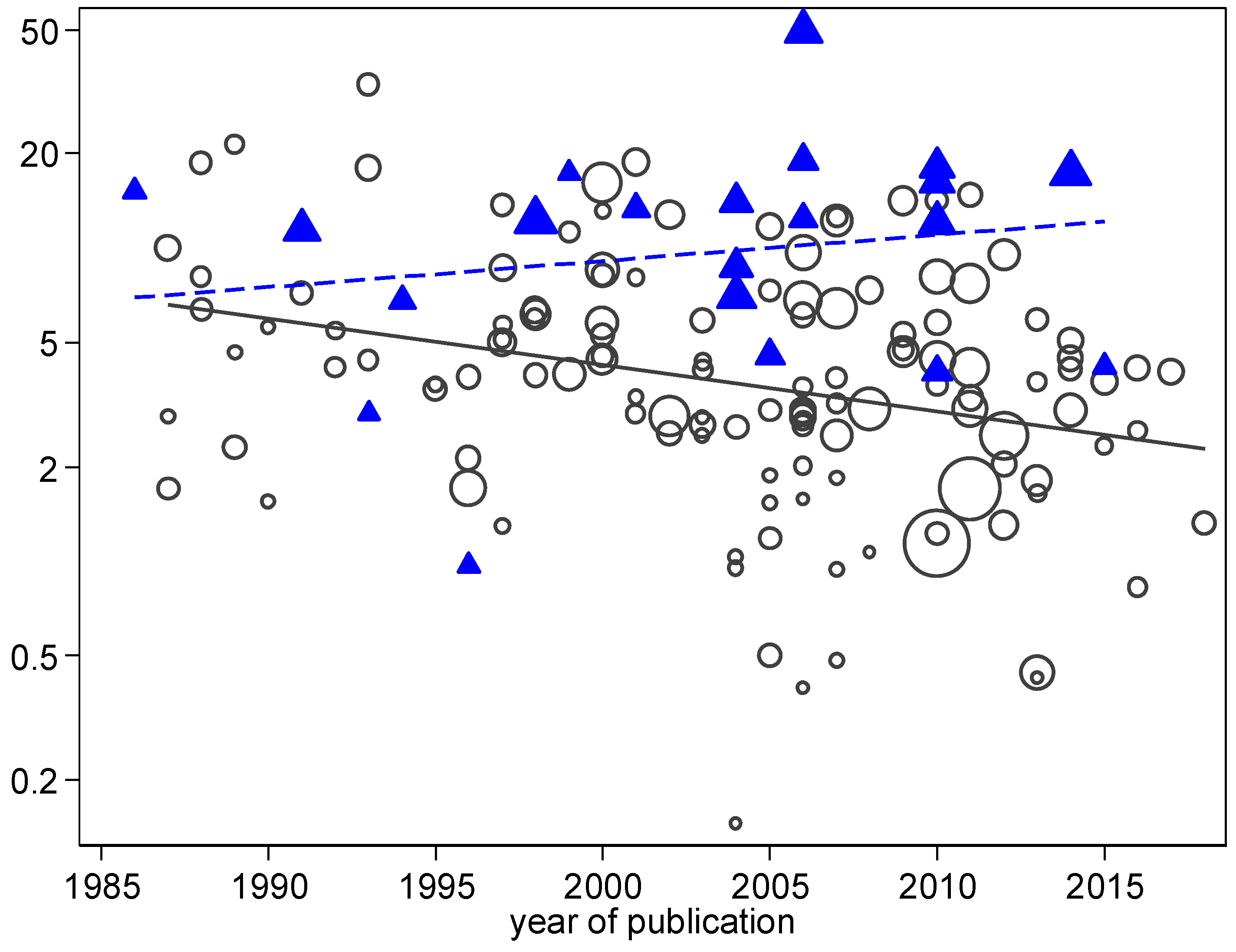
Figure 8.
Scatter plot and linear regression of S. aureus VAP incidence (per 1000 MV days) versus year of study publication for studies reporting from trauma ICUs (triangles, broken line) versus non-trauma ICUs (circles, unbroken line). Note the logarithmic scale of incidence. The slopes of the linear regression lines are significantly different (test for interaction p < 0.001; Poisson regression).
Figure 8.
Scatter plot and linear regression of S. aureus VAP incidence (per 1000 MV days) versus year of study publication for studies reporting from trauma ICUs (triangles, broken line) versus non-trauma ICUs (circles, unbroken line). Note the logarithmic scale of incidence. The slopes of the linear regression lines are significantly different (test for interaction p < 0.001; Poisson regression).
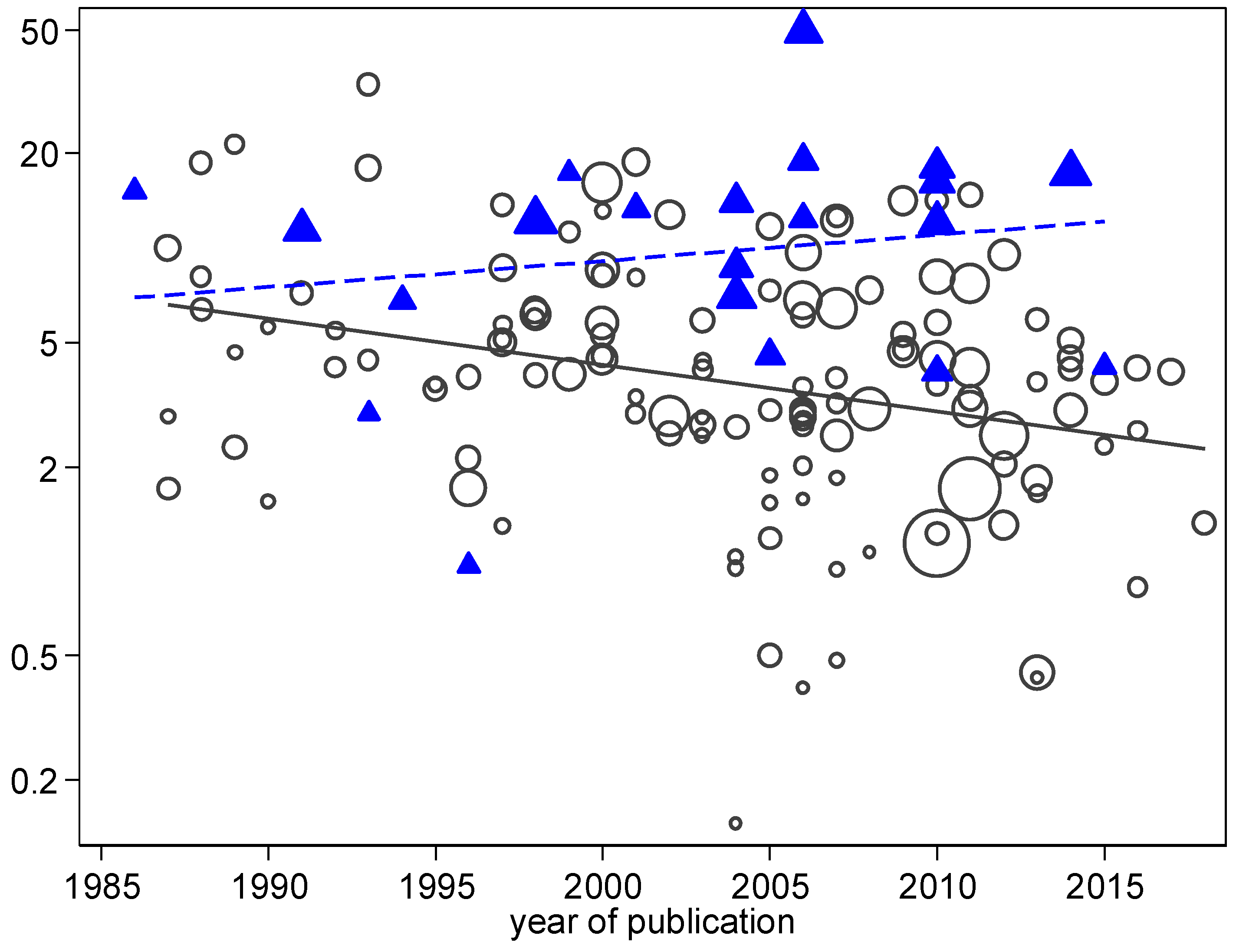
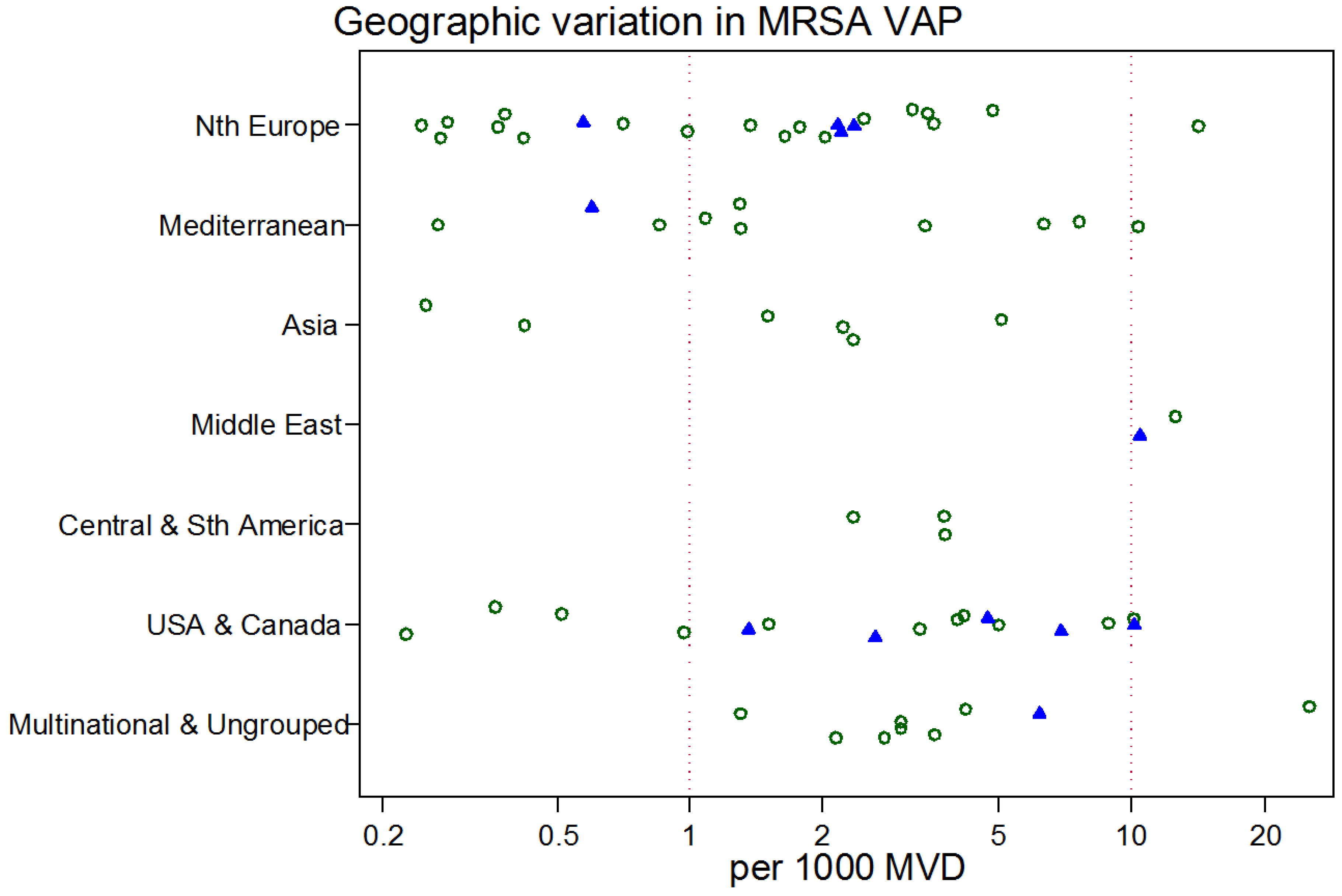
Figure 9.
Scatter plot of MRSA-VAP incidence (per 1000 MV days) among published studies in seven geographic regions with rates for studies reporting from trauma ICUs (closed symbols) versus other ICUs (open symbols). Note the logarithmic scale of incidence. The vertical lines at incidences of 1 and 10 per 1000 MVD are for reference.
Figure 9.
Scatter plot of MRSA-VAP incidence (per 1000 MV days) among published studies in seven geographic regions with rates for studies reporting from trauma ICUs (closed symbols) versus other ICUs (open symbols). Note the logarithmic scale of incidence. The vertical lines at incidences of 1 and 10 per 1000 MVD are for reference.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of the studies a.
| Multinational and Ungrouped | Northern Europe b | Mediterranean c | Asia d | Middle East e | Central and South America f | USA/Canada g | |
|---|---|---|---|---|---|---|---|
| Sources [ref] | [1,2,3,4,5,6,131,132,133] | [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49] | [50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78] | [79,80,81,82,83,84,85,86,87,88] | [89,90,91,92,93,94,95,96,97,98] | [99,100,101,102,103,104,105,106] | [107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130] |
| Number of groups | 20 | 45 | 27 | 13 | 11 | 7 | 26 |
| Trauma ICUs h | 1 | 5 | 7 | 0 | 1 | 0 | 7 |
| Bronchoscopic sampling i | 2 | 27 | 16 | 0 | 2 | 1 | 10 |
| Intervention period j | 1 | 2 | 1 | 4 | 1 | 1 | 2 |
| Study publication year (range) | 1987–2014 | 1988–2018 | 1987–2016 | 2003–2016 | 1990–2017 | 2003–2013 | 1986–2014 |
| Numbers of patients per study group; median (IQR) | 1194; 411–2339 | 439; 175–1004 | 184; 101–318 | 618; 344–1076 | 448; 92–2584 | 274; 180–712 | 327; 223–521 |
| Duration of MV (days); median (IQR) | 7.4; 5–9.2 | 10.7; 8.0–13 | 8.0; 7–11 | 6.0; 2.5–9 | 9.8; 8.9–13.5 | 9.6; 7.6–10 | 6.0; 5–8 |
| VAP incidence per 1000 MV days | |||||||
| mean | 25.0 | 17.8 | 26.8 | 18.2 | 24.0 | 21.8 | 20.5 |
| 95% CI | 20.7–30.2 | 14.0–22.4 | 20.9–34.1 | 14.3–23.1 | 18.2–31.2 | 13.6–34.8 | 14.0–30.6 |
| S. aureus VAP incidence per 1000 MV days | |||||||
| mean | 5.4 | 4.4 | 6.1 | 2.1 | 4.9 | 3.5 | 5.1 |
| 95% CI | 3.9–7.5 | 3.2–6.1 | 4.4–8.5 | 1.5–3.0 | 3.3–7.3 | 2.4–5.0 | 3.2–8.0 |
| MRSA VAP incidence per 1000 MV days k | |||||||
| mean | 3.7 | 1.4 | 2.3 | 1.8 | 2.5 | ||
| 95% CI | 2.2–6.1 | 0.8–2.5 | 1.1–4.5 | 0.9–3.3 | 1.2–5.3 | ||
| n | 9 | 22 | 10 | 6 | 2 | 3 | 16 |
a Abbreviations; ICU, Intensive Care Unit; MV, Mechanical Ventilation; NA, Not Applicable; VAP, Ventilator-Associated Pneumonia; IQR, Interquartile Range; b Northern Europe includes France, Germany, the United Kingdom, Switzerland, Sweden, Iceland and Poland; c Mediterranean includes Spain, Italy, Greece and Tunisia; d Asia includes China, India, Pakistan and Bangladesh; e Middle East includes Turkey, Iraq, Lebanon and Saudi Arabia; f Central and South America includes Argentina, Brazil, Chile, Colombia, Cuba and Guatemala; g Northern America includes USA and Canada; h Trauma ICU defined as an ICU with >50% of patient admissions for trauma; i bronchoscopic vs. tracheal sampling toward the diagnosis of VAP; j number of groups that were studied during a period of an infection control intervention; k summary MRSA VAP incidences are not reported for regions with fewer than four reports.
Table 2.
Log VAP incidence per thousand MV days; meta-regression models a.
| Overall VAP | S. aureus VAP | MRSA VAP | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Factor | Coefficient b | 95% CI | p | Coefficient b | 95% CI | p | Coefficient b | 95% CI | p |
| Multinational and Ungrouped (reference group) | +3.60 | +3.12–+4.08 | +2.16 | +1.54–+2.79 | +1.99 | +0.68–+3.31 | |||
| Geographic region | |||||||||
| Northern Europe | −0.37 | −0.73–−0.01 | 0.05 | −0.27 | −0.74–+0.20 | 0.26 | −1.09 | −1.97–−0.21 | 0.02 |
| Mediterranean | −0.06 | −0.45–+0.34 | 0.78 | −0.12 | −0.63–+0.39 | 0.64 | −0.69 | −1.71–+0.33 | 0.18 |
| Asia | −0.23 | −0.69–+0.22 | 0.32 | −0.79 | −1.4–−0.18 | 0.01 | −0.75 | −1.95–+0.45 | 0.21 |
| Middle East | −0.04 | −0.51–+0.43 | 0.87 | −0.04 | −0.65–+0.56 | 0.88 | +0.95 | −0.66–+2.56 | 0.24 |
| Central and South America | −0.08 | −0.61–+0.44 | 0.76 | −0.45 | −1.17–+0.28 | 0.23 | −0.22 | −1.60–+1.16 | 0.75 |
| USA and Canada | −0.35 | −0.75–+0.05 | 0.08 | −0.33 | −0.83–+0.18 | 0.20 | −0.62 | −1.53–+0.29 | 0.18 |
| Trauma c | +0.38 | +0.07–+0.68 | 0.02 | +0.82 | +0.43–+1.21 | 0.001 | +0.29 | −0.43–+1.00 | 0.42 |
| Year of publication d | −0.01 | −0.03–+0.01 | 0.065 | −0.02 | −0.04–−0.01 | 0.04 | −0.02 | −0.06–+0.02 | 0.26 |
| Mode of diagnosis e | −0.07 | −0.31–+0.16 | 0.53 | +0.01 | −0.30–+0.31 | 0.95 | +0.13 | −0.44–+0.70 | 0.65 |
| Intervention period f | −0.35 | −0.74–+0.04 | 0.075 | −0.50 | −1.03–+0.04 | 0.068 | −0.54 | −1.67–+1.58 | 0.34 |
a This table displays the results of meta-regression analyses for log VAP, log S. aureus-associated VAP and log MRSA VAP incidence per thousand MV days. b Interpretation. The reference group is the composite group of multinational and ungrouped studies, and this coefficient equals the difference in log from 0 (a log equal to 0 equates to a rate of 1). The other coefficients represent the difference in log for groups positive for that factor vs. the reference group. c The coefficient for trauma represents the increment in log for an ICU having a majority of admissions for trauma. d The coefficient for year of publication represents the linear increment in log for each year after 1980. e For sampling using bronchoscopic versus tracheal sampling. f Studies undertaken during an infection control intervention.
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hurley, J.C. World-Wide Variation in Incidence of Staphylococcus aureus Associated Ventilator-Associated Pneumonia: A Meta-Regression. Microorganisms 2018, 6, 18. https://doi.org/10.3390/microorganisms6010018
AMA Style
Hurley JC. World-Wide Variation in Incidence of Staphylococcus aureus Associated Ventilator-Associated Pneumonia: A Meta-Regression. Microorganisms. 2018; 6(1):18. https://doi.org/10.3390/microorganisms6010018
Chicago/Turabian StyleHurley, James C. 2018. "World-Wide Variation in Incidence of Staphylococcus aureus Associated Ventilator-Associated Pneumonia: A Meta-Regression" Microorganisms 6, no. 1: 18. https://doi.org/10.3390/microorganisms6010018
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.