Cognitive Predictors of Verbal Memory in a Mixed Clinical Pediatric Sample

Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Measures
2.3. Analyses
3. Results
3.1. Sample Characteristics


{kind=link}
{kind=link}
{kind=link}
| Cognitive DomainTest Variable | Score Type | Mean | SD | n |
|---|---|---|---|---|
| Verbal Knowledge | ||||
| Vocabulary (WISC-IV) | ss | 8.47 | 3.07 | 195 |
| Similarities (WISC-IV) | ss | 9.28 | 3.24 | 195 |
| Comprehension (WISC-IV) | ss | 9.32 | 3.04 | 195 |
| Processing Speed | ||||
| Symbol Search (WISC-IV) | ss | 8.13 | 3.14 | 200 |
| Coding (WISC-IV) | ss | 7.32 | 3.32 | 201 |
| Attention | ||||
| Sky Search—Attention (TEA-Ch) | ss | 7.97 | 3.09 | 204 |
| Score! (TEA-Ch) | ss | 7.35 | 3.60 | 209 |
| Creature Counting—Total (TEA-Ch) | ss | 8.13 | 3.57 | 179 |
| Working Memory | ||||
| Digit Span Backward (WISC-IV) | ss | 7.73 | 3.01 | 136 |
| Verbal Memory | ||||
| Delayed Recall Score (CMS) | StS | 92.58 | 17.42 | 233 |
3.2. Exploratory Factor Analysis (EFA)
| Measure | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| Verbal Knowledge | Processing Speed | Attention | Working Memory | |
| Vocabulary (WISC-IV) | 0.92 * | |||
| Similarities (WISC-IV) | 0.93 * | −0.13 | ||
| Comprehension (WISC-IV) | 0.76 * | 0.13 | 0.14 | |
| Symbol Search (WISC-IV) | 0.11 | 0.78 * | 0.15 | |
| Coding (WISC-IV) | 0.88 * | |||
| Sky Search—Attention (TEA-Ch) | 0.43 | 0.59 * | −0.14 | |
| Score! (TEA-Ch) | 0.22 | 0.55 * | ||
| Creature Counting—Total (TEA-Ch) | −0.33 | 0.81 * | 0.16 | |
| Digit Span Backward (WISC-IV) | 0.10 | 0.97 * |
| Measure | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| Verbal Knowledge | Processing Speed | Attention | Working Memory | |
| Vocabulary (WISC-IV) | 0.91 * | 0.16 | 0.29 | 0.27 |
| Similarities (WISC-IV) | 0.89 * | 0.16 | 0.25 | 0.16 |
| Comprehension (WISC-IV) | 0.83 * | 0.30 | 0.27 | 0.40 |
| Symbol Search (WISC-IV) | 0.32 | 0.82 * | 0.26 | 0.27 |
| Coding (WISC-IV) | 0.14 | 0.86 * | 0.15 | |
| Sky Search—Attention (TEA-Ch) | 0.12 | 0.53 | 0.63 * | |
| Score! (TEA-Ch) | 0.21 | 0.34 | 0.59 * | |
| Creature Counting—Total (TEA-Ch) | 0.28 | −0.12 | 0.79 * | 0.31 |
| Digit Span Backward (WISC-IV) | 0.28 | 0.20 | 0.21 | 0.97 * |
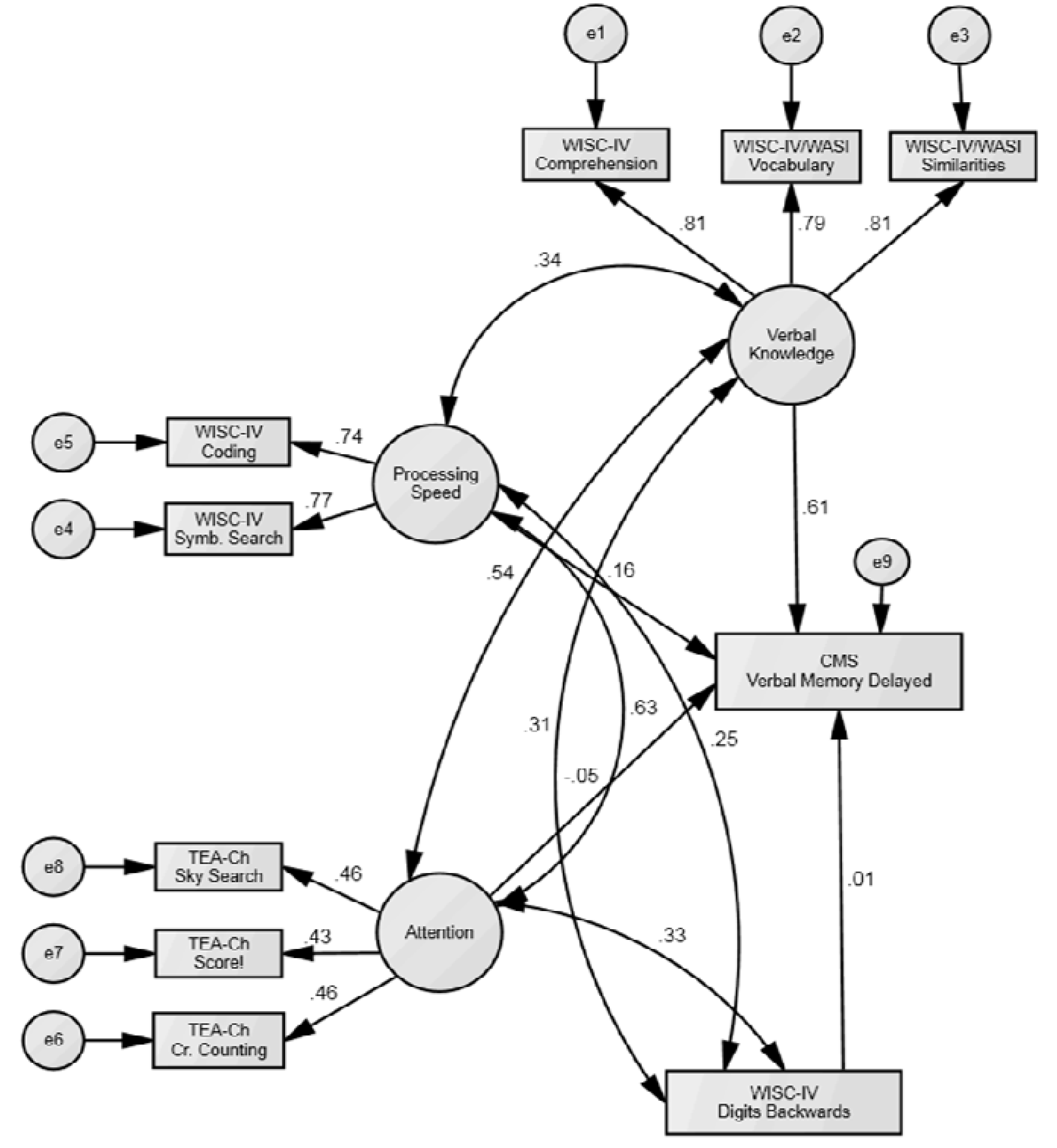
3.3. Structural Equation Model (SEM)

| Model | Χ2 | CMIN/DF | NFI | RFI | RMSEA | RMSEA sig. |
|---|---|---|---|---|---|---|
| Independence (Null) Model 1 | - | 10.41 | 0.00 | 0.00 | 0.20 | 0.00 |
| Specified Model 1 | 73.78 ** | 1.99 ** | 0.87 | 0.81 | 0.06 | 0.11 |
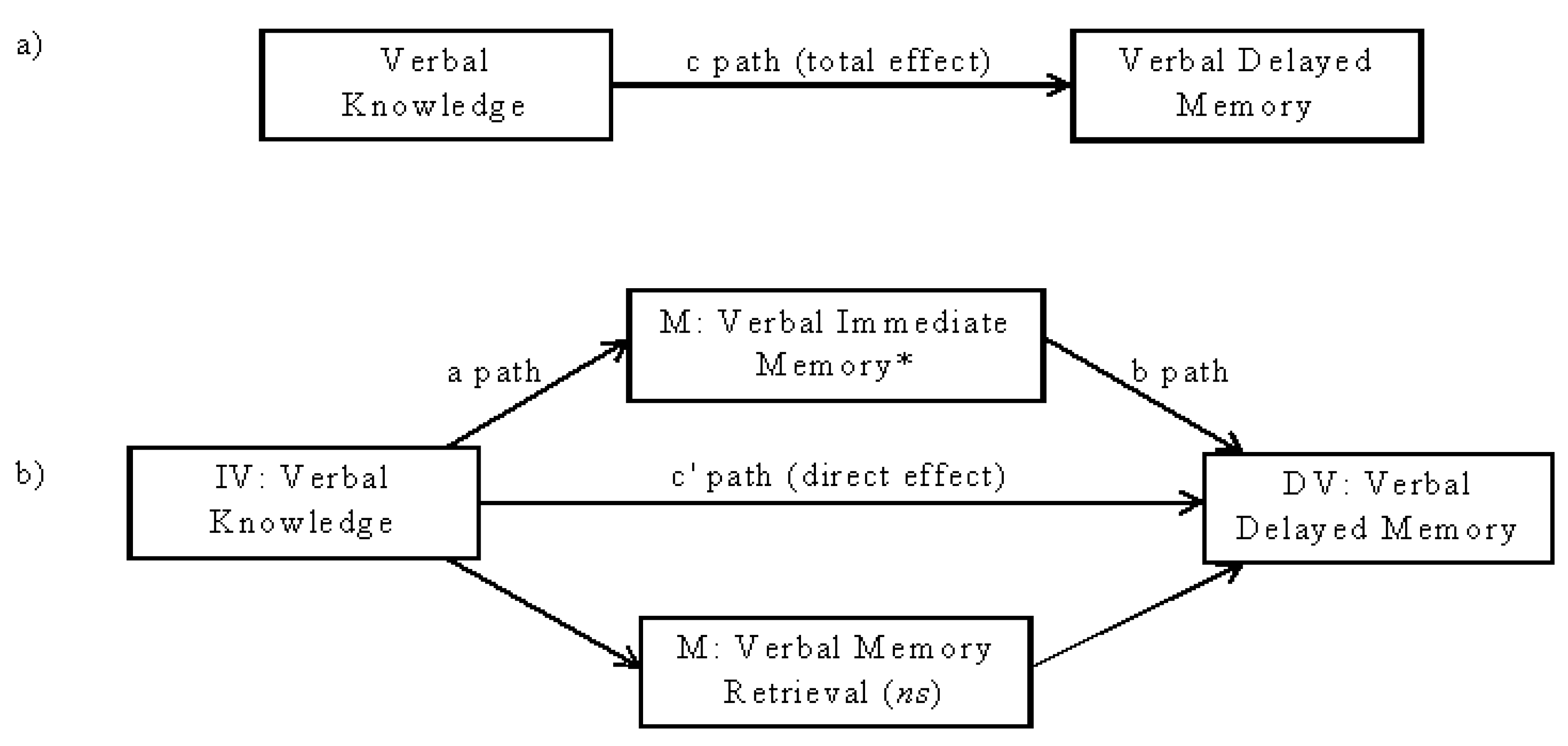
3.4. Correlation and Bootstrapping Analyses to Examine Possible Mediation
| Verbal Memory Process | Verbal Delayed Index (CMS) | Vocabulary (WISC-IV) | Similarities (WISC-IV) | Comprehension (WISC-IV) | ||||
|---|---|---|---|---|---|---|---|---|
| CMS Score | r | n | r | n | r | n | r | n |
| Encoding Immediate Memory | 0.77 ** | 232 | 0.51 ** | 193 | 0.49 ** | 193 | 0.51 ** | 193 |
| Retention Retention | 0.04 | 180 | −0.03 | 150 | 0.10 | 150 | −0.01 | 150 |
| Retrieval Delayed Memory Contrast | 0.44 ** | 212 | 0.06 | 176 | 0.15 * | 176 | 0.08 | 176 |

| Dependent variable | Total effect of IV on DV (path c) | Direct effect of IV on DV (path c’) | Total indirect effect of IV on DV via MV (path ab) |
|---|---|---|---|
| B (SE) | B (SE) | B (SE) | |
| Delayed Memory CMS Verbal Delayed Memory Index Score | 0.73 * (0.08) | 0.20 * (0.06) | 0.53 * (0.07) |
4. Discussion
4.1. Verbal Knowledge Significantly Contributes to Verbal Memory Performance
4.2. The Relationship between Verbal Knowledge and Verbal Memory Performance is Mediated by Verbal Encoding Abilities
4.3. Other Cognitive Factors Do Not Significantly Contribute to Verbal Memory Performance
4.4. Study Limitations
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Dehn, M.J. Long-Term Memory Problems in Children and Adolescents: Assessment, Intervention, and Effective Instruction; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Felix, L.; Hunter, S.J. Pediatric Aspects of Epilepsy. In Lifespan Developmental Neuropsychology; Donders, J., Hunter, S.J., Eds.; Cambridge University Press: Cambridge, UK, 2010; pp. 359–369. [Google Scholar]
- Westerveld, M. Childhood Epilepsy. In Pediatric Neuropsychology: Research, Theory, and Practice; Yeates, K.O., Ris, M.D., Taylor, H.G., Pennington, B.F., Eds.; The Guilford Press: New York, NY, USA, 2010; pp. 71–91. [Google Scholar]
- Brooks, B.L.; Iverson, G.L.; Sherman, E.M.S.; Holdnack, J.A. Healthy children and adolescents obtain some low scores across a battery of memory tests. J. Int. Neuropsychol. Soc. 2009, 15, 613–617. [Google Scholar] [CrossRef]
- Baddeley, A. Short-Term and Working Memory. In The Oxford Handbook of Memory; Tulving, E., Craik, F.I.M., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 77–92. [Google Scholar]
- Wilson, B. Memory Rehabilitation: Integrating Theory and Practice; The Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Ornstein, P.A.; Haden, C.A.; Elischberger, H.B. Children’s Memory Development: Remembering the Past and Preparing for the Future. In Lifespan Cognition: Mechanisms of Change; Bialystok, E., Craik, F.I.M., Eds.; Oxford University Press: Oxford, UK, 2006; pp. 143–161. [Google Scholar]
- Brown, S.C.; Craik, F.I.M. Encoding and Retrieval of Information. In The Oxford Handbook of Memory; Tulving, E., Craik, F.I.M., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 93–107. [Google Scholar]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W. Neuropsychological Assessment, 4th ed.; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Hitch, G.J. Working Memory in Children: A Cognitive Approach. In Lifespan Cognition: Mechanisms of Change; Bialystok, E., Craik, F.I.M., Eds.; Oxford University Press: Oxford, UK, 2006; pp. 112–127. [Google Scholar]
- Cohen, M.J. Children’s Memory Scale Manual; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Cohen, M.J.; Gainesville, Florida. >Personal Communications. 6 September 2011 & 15 May 2012.
- Standardization data from the Children’s Memory Scale; [used with permission of publisher]; NCS Pearson, Inc.: Bloomington, MN, USA, 1997.
- Wecshler, D. Wecshler Intelligence Scale for Children, 4th ed.; The Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Manly, T.; Robertson, I.H.; Anderson, V.; Nimmo-Smith, I. The Test of Everyday Attention for Children; Thames Valley Test Company: London, UK, 1999. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; SAGE: London, UK, 2009. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Arbuckle, J.L. Amos 17.0, [computer software]; SPSS: Chicago, IL, USA, 2008.
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Bollen, K.; Long, S. Testing Structural Equation Models; Sage: Newbury Park, CA, USA, 1993. [Google Scholar]
- Wecshler, D. WISC-IV Technical and Interpretive Manual; The Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Williams, P.E.; Weiss, L.G.; Rolfhus, E.L. WISC-IV Technical Report #2 Psychometric Properties. In The Psychological Corporation’s WISC-IV Technical Manual #2; The Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Blank, M. Cognitive functions of language in the preschool years. Dev. Psychol. 1974, 10, 229–245. [Google Scholar] [CrossRef]
- De Alwis, D.; Myerson, J.; Hershey, T.; Hale, S. Children’s higher order cognitive abilities and the development of secondary memory. Psychon. Bull. Rev. 2009, 16, 925–930. [Google Scholar] [CrossRef]
- Diamond, A. The Early Development of Executive Functions. In Lifespan Cognition: Mechanisms of Change; Bialystok, E., Craik, F.I.M., Eds.; Oxford University Press: Oxford, UK, 2006; pp. 70–95. [Google Scholar]
- Moscovitch, M. Memory and Working with Memory: Evaluation of a Component Process Model and Comparisons with Other Models. In Memory Systems; Schacter, D., Tulving, E., Eds.; The MIT Press: Cambridge, MA, USA, 1994; pp. 407–451. [Google Scholar]
- Schneider, W.; Pressley, M. Memory Development Between 2 and 20; Springer-Verlag: New York, NY, USA, 1989. [Google Scholar]
- Mottram, L.; Donders, J. Cluster subtypes on the California Verbal Learning Test-Children’s Version after pediatric traumatic brain injury. Dev. Neuropsychol. 2006, 30, 865–883. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Jordan, L.L.; Tyner, C.E.; Heaton, S.C. Cognitive Predictors of Verbal Memory in a Mixed Clinical Pediatric Sample. Behav. Sci. 2013, 3, 522-535. https://doi.org/10.3390/bs3030522
Jordan LL, Tyner CE, Heaton SC. Cognitive Predictors of Verbal Memory in a Mixed Clinical Pediatric Sample. Behavioral Sciences. 2013; 3(3):522-535. https://doi.org/10.3390/bs3030522
Chicago/Turabian StyleJordan, Lizabeth L., Callie E. Tyner, and Shelley C. Heaton. 2013. "Cognitive Predictors of Verbal Memory in a Mixed Clinical Pediatric Sample" Behavioral Sciences 3, no. 3: 522-535. https://doi.org/10.3390/bs3030522