Regional Variations of Fertility Control Behavior among Rural Reproductive Women in Bangladesh: A Hierarchical Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size
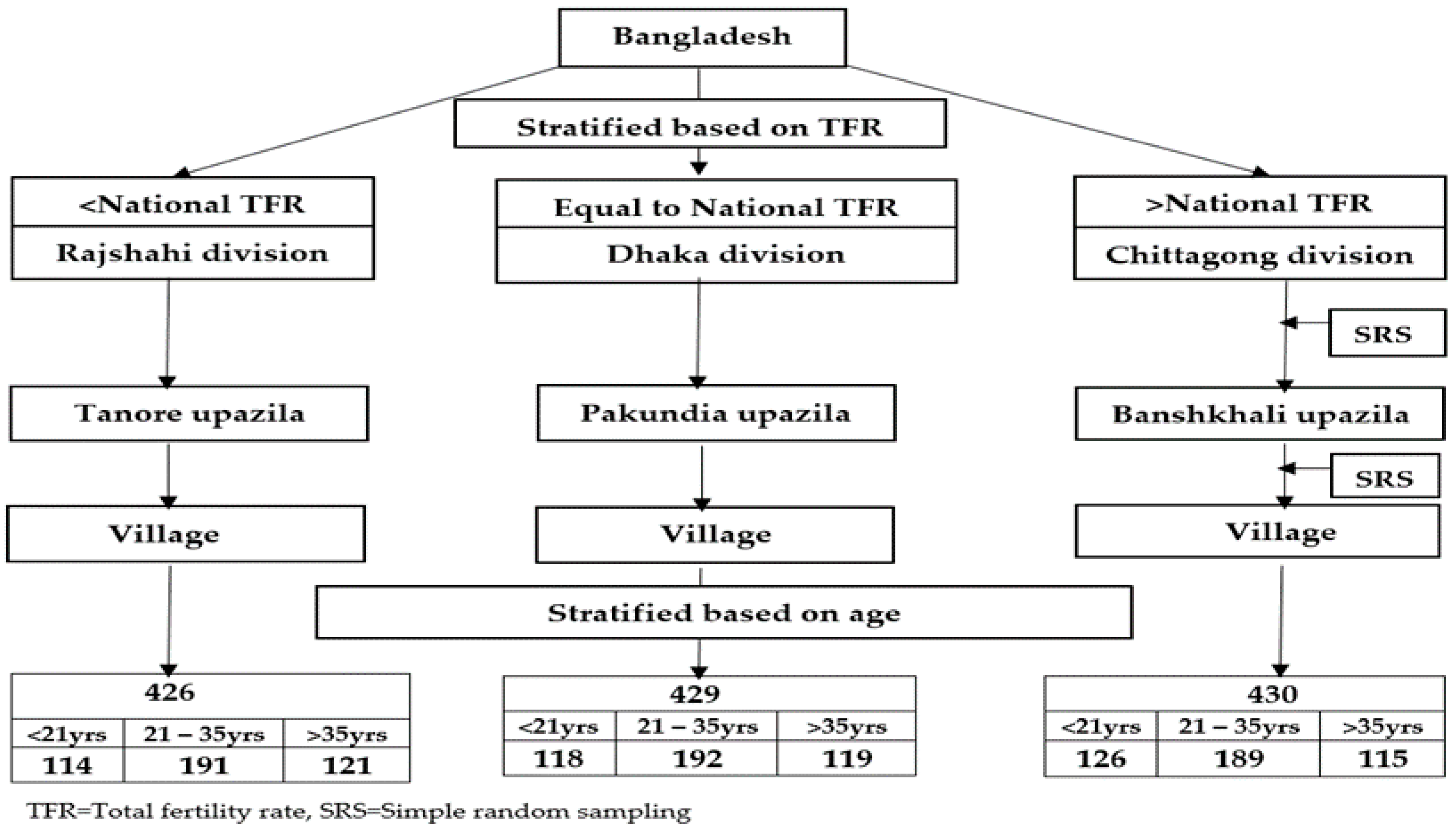
2.3. Sampling Method
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Contraception: Past, Present and Future and Why It Matters. Sexual and Reproductive Health Program. 2018. Available online: http://who.int/reproductivehealth/topics/family_planning/en/ (accessed on 9 May 2018).
- Picavet, C.; Leest, L.V.; Wijsen, C. Contraceptive decision-making: Background and outcomes of contraceptive methods. Rutgers World Population Foundation (WPF). 2011. Available online: https://www.rutgers.nl/sites/rutgersnl/files/PDF/Contraceptive_Decisions_Report-def.pdf (accessed on 5 May 2017).
- United Nations Population Division (UNPD). Trends in Contraceptive Use Worldwide 2015. Available online: http://www.un.org/en/development/desa/population/publications/pdf/family/trendsContraceptiveUse2015Report.pdf (accessed on 9 May 2018).
- United Nations Population Fund (UNFPA). The Global Program to Enhance Reproductive Health Commodity Security: Annual Report 2013. Available online: http://www.unfpa.org/publications/global-programme-enhance-reproductive-health-commodity-security-annual-report-2013 (accessed on 9 May 2018).
- Hodgson, E.J.; Collier, C.; Hayes, L.; Curry, L.; Fraenkel, L. Family planning and contraceptive decision-making by economically disadvantaged, African-American women. Contraception 2013, 88, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, K.D.; Anderson, R.T.; Creedon, D.; Montori, V.M.; Bachman, J.; Erwin, P.; LeBlanc, A. Women’s values in contraceptive choice: A systematic review of relevant attributes included in decision aids. BMC Women’s Health 2014, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- Bongaarts, J.; Cleland, J.; Townsend, J.W.; Bertrand, J.T.; Gupta, M.D. Family Planning Programs for the 21st Century: Rationale and Design. Population Council, 2012. Available online: http://www.popcouncil.org/uploads/pdfs/2012_FPfor21stCentury.pdf (accessed on 4 May 2018).
- Ministry of Health and Family Welfare (MOHFW), National Institute of Population Research and Training (NIPORT). Bangladesh Demographic and Health Survey 2014; NIPORT: Dhaka, Bangladesh, 2016.
- Rahman, M.M.; Mostofa, M.G.; Hoque, M.A. Women’s household decision-making autonomy and contraceptive behavior among Bangladeshi women. Sex. Reprod. Healthc. 2014, 5, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Li, Q.; Liu, L.; Tsui, A.O. Maternal deaths averted by contraceptive use: An analysis of 172 countries. Lancet 2012, 380, 111–125. [Google Scholar] [CrossRef]
- Ashraf, Q.H.; Weil, D.N.; Wilde, J. The Effect of Fertility Reduction on Economic Growth. Popul. Dev. Rev. 2013, 39, 97–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations (UN). World Fertility Patterns 2015. Available online: https://www.yumpu.com/en/document/view/54943353/world-fertility-patterns-2015 (accessed on 31 March 2017).
- The World Bank. World Bank Open Data: Population, Total; World Bank Group: Washington, DC, USA, 2016; Available online: http://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 22 April 2018).
- United Nations Population Division (UNPD). World Population Prospects, The 2015 Revision. 2015. Available online: https://esa.un.org/unpd/wpp (accessed on 22 November 2016).
- World Health Organization (WHO). Family Planning/Contraception: Fact Sheet; WHO: Geneva, Switzerland, May 2015; Available online: http://www.who.int/mediacentre/factsheets/fs351/en/ (accessed on 9 May 2018).
- McLaughlin, J. Family Planning in South Asia: Improving Equity of Access; The World Bank: Washington, DC, USA, 2012; Available online: http://blogs.worldbank.org/health/family-planning-in-south-asia-improving-equity-of-access (accessed on 16 March 2017).
- Population Reference Bureau (PRB). 2016 World Population Data Sheet; PRB: Washington, DC, USA, 2016; Available online: http://www.prb.org/Publications/Datasheets/2016/2016-world-population-data-sheet.aspx (accessed on 1 March 2017).
- Fishbein, M. A Reasoned Action Approach to Health Promotion. Med. Decis. Making 2008, 28, 834–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyman, N.; Oakley, D. Effective contraceptive use: An exploration of theory-based influences. Health Educ. Res. 2009, 24, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I.; Klobas, J. Fertility Intentions: An Approach Based on the Theory of Planned Behavior. Demogr. Res. 2013, 29, 203–232. [Google Scholar]
- Kabir, A.; Ali, R.; Islam, M.S.; Kawsar, L.A.; Islam, M.A. A comparison of regional variations of fertility in Bangladesh. Int. Q. Community Health Educ. 2009, 29, 275–291. [Google Scholar] [CrossRef] [PubMed]
- Deb, S.; Kabir, A.; Kawsar, L.A. Women’s empowerment and regional variation of contraceptive norms in Bangladesh. Int. Q. Community Health Educ. 2010, 31, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Alpu, O.; Fidan, H. On the use of contraceptive methods among married women in Turkey. Eur. J. Contracept. Reprod. Health Care 2006, 11, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Thang, N.M.; Huong, V.T. Changes in contraceptive use in Vietnam. J. Biosoc. Sci. 2003, 35, 527–543. [Google Scholar] [CrossRef] [PubMed]
- Huda, F.A.; Robertson, Y.; Chowdhuri, S.; Sarker, B.K.; Reichenbach, L.; Somrongthong, R. Contraceptive practices among married women of reproductive age in Bangladesh: A review of the evidence. Reproductive Health 2017, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Anyanwu, M.; Alida, B.W.N. Uptake of long-acting reversible contraceptive devices in Western region of The Gambia. Afr. Health Sci. 2017, 17, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Kawsar, L.A; Kabir, A.; Islam, M.A. Sex preference and contraceptive norms among regions in Bangladesh. Int. Q. Community Health Educ. 2008, 29, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Woldemicael, G. Women’s autonomy and reproductive preferences in Eritrea. J. Biosoc. Sci. 2009, 41, 161–181. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, Y. Women’s autonomy and reproductive health care utilisation: Empirical evidence from Tajikistan. Health Policy 2011, 102, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Saleem, A.; Pasha, G.R. Women’s reproductive autonomy and barriers to contraceptive use in Pakistan. Eur. J. Contracept. Reprod. Health Care 2008, 13, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, A.; Mishra, V.; Arnold, F. The relationship of family size and composition to fertility desires, contraceptive adoption and method choice in South Asia. Int. Perspect. Sex Reprod. Health 2009, 35, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Keele, J.J.; Forste, R.; Flake, D.F. Hearing native voices: Contraceptive use in Matemwe Village, East Africa. Afr. J. Reprod. Health 2005, 9, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Tuladhar, H.; Marahatta, R. Awareness and practice of family planning methods in women attending gyne OPD at Nepal medical college teaching hospital. Nepal. Med. Coll. J. 2008, 10, 184–191. [Google Scholar] [PubMed]
- Dabral, S.; Malik, S.L. Demographic study of gujjars of Delhi:IV. KAP of family planning. J. Hum. Ecol. 2004, 16, 231–237. [Google Scholar] [CrossRef]
- Singh, A.; Singh, K.K.; Verma, P. Knowledge, attitude and practice GAP in family planning usage: An analysis of selected cities of Uttar Pradesh. Contracept. Reprod. Med. 2016, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- Kim, M. A Structural Equation Model Explaining Contraception Behaviors of Married Korean Women. J. Korean Acad. Womens Health Nurs. 2001, 7, 141–156. [Google Scholar]
- Libbus, K.; Kridli, S.A. Contraceptive decision making in a sample of Jordanian Muslim women: Delineating salient beliefs. Health Care Women Int. 1997, 18, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Bawah, A.A. Spousal communication and family planning behavior in Navrongo: A longitudinal assessment. Stud. Fam. Plan. 2002, 33, 185–194. [Google Scholar] [CrossRef]
- Kimuna, S.R.; Adamchak, D.J. Gender relation: Husband-wife fertility and family planning decisions in Kenya. J. Biosoc. Sci. 2001, 33, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Yue, K.; O’Donnel, C.; Sparks, P.L. The effect of spousal communication on contraceptive use in Central Terai, Nepal. Patient Educ. Couns. 2010, 81, 402–408. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Block 1 | Block 2 | Block 3 | Outcome |
|---|---|---|---|
| Background Factors | Components from TPB | Regional Effect | |
| Age Educational level Monthly family income Number of children Women’s empowerment Fertility preference Fertility control knowledge | FP attitude Social influence PBC Fertility control intention Spousal status (actual behavioral control) | Region | Fertility control behavior |
| Socio-Demographic Characteristics | Number | Percentage |
|---|---|---|
| Age of respondents (years) | ||
| ≤20 | 358 | 27.9 |
| 21–35 | 572 | 44.5 |
| ≥36 | 355 | 27.6 |
| Mean (SD) | 27.7 (±7.8) years | |
| Min–Max | 18–46 years | |
| Age of husbands (years) | ||
| ≤25 | 151 | 11.8 |
| 26–35 | 672 | 52.2 |
| ≥36 | 462 | 36.0 |
| Mean (SD) | 34.8 (±8.7) years | |
| Min–Max | 21–60 years | |
| Religion | ||
| Islam | 1153 | 89.7 |
| Hindu | 132 | 10.3 |
| Educational level of respondents | ||
| Illiterate | 281 | 21.9 |
| Primary | 628 | 48.9 |
| Junior School Certificate | 275 | 21.4 |
| Secondary School Certificate and above | 101 | 7.8 |
| Educational level of husbands | ||
| Illiterate | 343 | 26.7 |
| Primary | 529 | 41.2 |
| Junior School Certificate | 219 | 17.0 |
| Secondary School Certificate and above | 194 | 15.1 |
| Family income (Taka) | ||
| ≤8000 | 489 | 38.1 |
| 8001–12,000 | 602 | 46.8 |
| ≥12,001 | 194 | 15.1 |
| Mean (SD) | 10,480 (±5261) Taka | |
| Min–Max | 5000–60,000 Taka | |
| Occupational status of respondents | ||
| Housewife | 1152 | 89.6 |
| Day laborer | 66 | 5.1 |
| Factory worker | 29 | 2.3 |
| Business | 16 | 1.3 |
| Govt./private employee | 22 | 1.7 |
| Occupational status of husbands | ||
| Agricultural worker | 710 | 55.2 |
| Day laborer | 223 | 17.4 |
| Factory worker | 89 | 6.9 |
| Business | 181 | 14.1 |
| Govt./private employee | 82 | 6.4 |
| Family type | ||
| Nuclear | 478 | 37.2 |
| Extended | 807 | 62.8 |
| Number of family members | ||
| ≤4 | 326 | 25.3 |
| 5–6 | 646 | 50.3 |
| ≥7 | 313 | 24.4 |
| Mean (SD) | 5.5 (±1.6) | |
| Min–Max | 3–11 | |
| Reproductive Characteristics | Number | Percentage |
|---|---|---|
| Age at 1st marriage of respondents (years) | ||
| ≤15 | 223 | 17.4 |
| 16–17 | 790 | 61.5 |
| ≥18 | 272 | 21.1 |
| Mean (SD) | 16.6 (±1.1) years | |
| Min–Max | 14–20 years | |
| Age at 1st pregnancy of respondents (years) | ||
| ≤17 | 357 | 27.8 |
| 18–19 | 652 | 50.8 |
| ≥20 | 276 | 21.4 |
| Mean (SD) | 18.2 (±1.3) years | |
| Min–Max | 16–22 years | |
| Number of pregnancies | ||
| 1 | 422 | 32.9 |
| 2 | 309 | 24.0 |
| 3–4 | 389 | 30.3 |
| >4 | 165 | 12.8 |
| Mean (SD) | 2.5 (±1.5) | |
| Min–Max | 1–8 | |
| Number of deliveries | ||
| 1 | 425 | 33.1 |
| 2 | 316 | 24.6 |
| 3–4 | 423 | 32.9 |
| >4 | 121 | 9.4 |
| Mean (SD) | 2.5 (±1.3) | |
| Min–Max | 1–8 | |
| Number of living children | ||
| 1 | 433 | 33.7 |
| 2 | 323 | 25.1 |
| 3–4 | 457 | 35.6 |
| >4 | 72 | 5.6 |
| Mean (SD) | 2.4 (±1.3) | |
| Min–Max | 1–7 | |
| Initial gap before 1st pregnancy (Years) | ||
| <2 | 618 | 48.1 |
| ≥2 | 667 | 51.9 |
| Mean (SD) | 1.6 (±0.7) years | |
| Min–Max | 1–4 years | |
| Use of contraceptives | ||
| Never | 515 | 40.1 |
| Sometimes | 112 | 8.7 |
| Very often | 34 | 2.6 |
| Always | 624 | 48.6 |
| Types of modern methods (n = 770) | ||
| Oral pill | 417 | 54.2 |
| Injection | 173 | 22.5 |
| Norplant | 28 | 3.6 |
| Copper-T | 21 | 2.7 |
| Condom | 58 | 7.5 |
| Vasectomy/ligation | 73 | 9.5 |
| Variable | Model1 | Model2 | Model3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE (B) | β | B | SE (B) | β | B | SE (B) | β | |
| Constant | −13.66 | 0.78 | −20.00 | 0.88 | −19.77 | 0.88 | |||
| Age | 0.10 | 0.06 | 0.17 *** | 0.06 | 0.02 | 0.10 * | 0.04 | 0.02 | 0.07 |
| Family income | 3.8 × 10−5 | 0.00 | 0.04 * | 2.2 × 10−5 | 0.00 | 0.03 | 1.8 × 10−5 | 0.20 | 0.02 |
| Educational level | |||||||||
| Up to primary | 1.33 | 0.30 | 0.15 | 0.71 | 0.27 | 0.08 | 0.61 | 0.27 | 0.07 |
| Above primary | 1.49 | 0.37 | 0.15 | 0.44 | 0.33 | 0.04 | 0.26 | 0.33 | 0.03 |
| Number of children | 0.02 | 0.15 | 0.01 | 0.12 | 0.13 | 0.04 | 0.19 | 0.13 | 0.05 |
| Empowerment | 0.20 | 0.02 | 0.23 *** | 0.08 | 0.02 | 0.09 *** | 0.08 | 0.02 | 0.09 *** |
| Fertility preference | 0.28 | 0.03 | 0.21 *** | 0.03 | 0.03 | 0.03 | 0.04 | 0.03 | 0.03 |
| Fertility knowledge | 1.02 | 0.06 | 0.39 | 0.53 | 0.06 | 0.20 *** | 0.54 | 0.06 | 0.20 *** |
| FP attitude | 0.17 | 0.03 | 0.12 *** | 0.17 | 0.03 | 0.12 *** | |||
| Social influence | 0.16 | 0.03 | 0.12 *** | 0.15 | 0.03 | 0.11 *** | |||
| PBC | 0.23 | 0.03 | 0.22 *** | 0.23 | 0.03 | 0.22 *** | |||
| Spousal status | 0.02 | 0.03 | 0.02 | 0.02 | 0.03 | 0.01 | |||
| Fertility control intention | 0.25 | 0.03 | 0.20 *** | 0.25 | 0.03 | 0.20 *** | |||
| Regional status | |||||||||
| Dhaka division | 0.46 | 0.19 | 0.05 * | ||||||
| Rajshahi division | 0.51 | 0.20 | 0.05 * | ||||||
| R2 | 0.556 | 0.664 | 0.666 | ||||||
| F for R2 change | 199.49 *** | 81.98 *** | 4.06 * | ||||||
| Characteristics | Mean Score ± (SD) | p-Value | |||
|---|---|---|---|---|---|
| National (n = 1285) | Rajshahi (n = 426) | Dhaka (n = 429) | Chittagong (n = 430) | ||
| Fertility control behavior | 8.9 (4.6) | 9.7 (4.5) | 9.1 (4.7) | 7.8 (4.3) | <0.001 *** |
| FP attitude | 30.1 (3.3) | 30.6 (3.3) | 30.1 (3.2) | 29.5 (3.4) | <0.001 *** |
| Social influence | 29.0 (3.6) | 29.6 (3.3) | 29.3 (3.5) | 28.0 (3.4) | <0.001 *** |
| PBC | 21.6 (4.3) | 22.2 (4.1) | 21.6 (4.3) | 20.9 (4.5) | <0.001 *** |
| Fertility control intention | 20.9 (3.6) | 21.5 (3.2) | 20.8 (3.4) | 20.2 (4.0) | <0.001 *** |
| Spousal status | 7.6 (3.1) | 8.0 (3.1) | 7.8 (3.2) | 6.9 (2.8) | <0.001 *** |
| Fertility preference | 20.1 (3.5) | 20.5 (3.4) | 20.1 (3.4) | 19.7 (3.6) | <0.01 ** |
| Fertility control knowledge | 5.6 (1.7) | 5.8 (1.7) | 5.6 (1.6) | 5.5 (1.8) | 0.120 |
| Women’s empowerment | 34.3 (5.2) | 35.7 (5.0) | 34.1 (5.4) | 33.1 (4.8) | <0.001 *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.A.; Chamroonsawasdi, K.; Chansatitporn, N.; Munsawaengsub, C.; Islam, M.S. Regional Variations of Fertility Control Behavior among Rural Reproductive Women in Bangladesh: A Hierarchical Analysis. Behav. Sci. 2018, 8, 68. https://doi.org/10.3390/bs8080068
Alam MA, Chamroonsawasdi K, Chansatitporn N, Munsawaengsub C, Islam MS. Regional Variations of Fertility Control Behavior among Rural Reproductive Women in Bangladesh: A Hierarchical Analysis. Behavioral Sciences. 2018; 8(8):68. https://doi.org/10.3390/bs8080068
Chicago/Turabian StyleAlam, Muhammed Ashraful, Kanittha Chamroonsawasdi, Natkamol Chansatitporn, Chokchai Munsawaengsub, and Md Shafiqul Islam. 2018. "Regional Variations of Fertility Control Behavior among Rural Reproductive Women in Bangladesh: A Hierarchical Analysis" Behavioral Sciences 8, no. 8: 68. https://doi.org/10.3390/bs8080068