Towards Laser Driven Hadron Cancer Radiotherapy: A Review of Progress

Abstract
:1. Preamble
2. Introduction
3. Pulsed Ion Beams (Protons and Carbon Ions): Laser-Driven Source Features

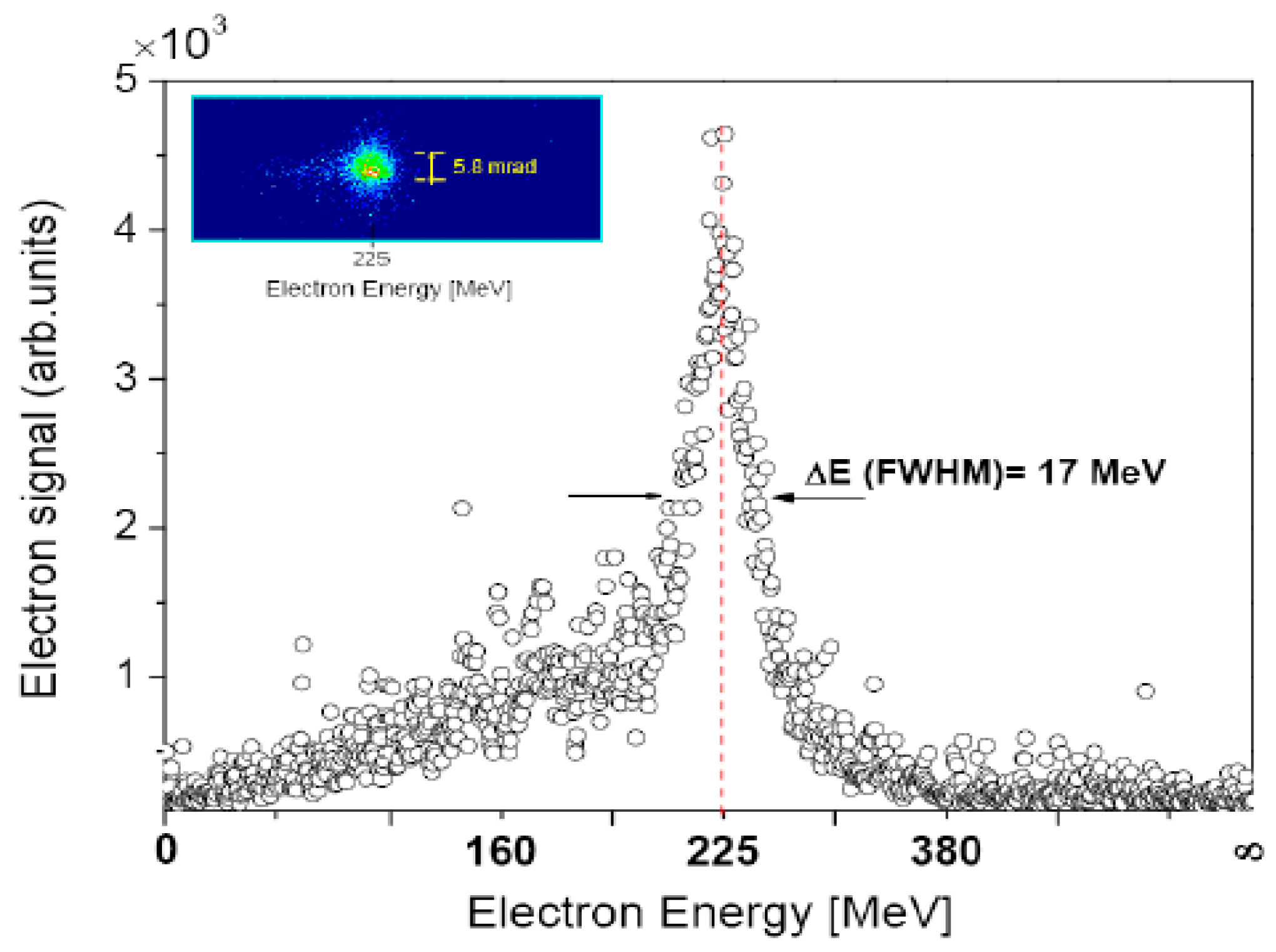
3.1. Typical Ion Energy Spectra




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3.2. Spectral Control (with Lasers and Targets)







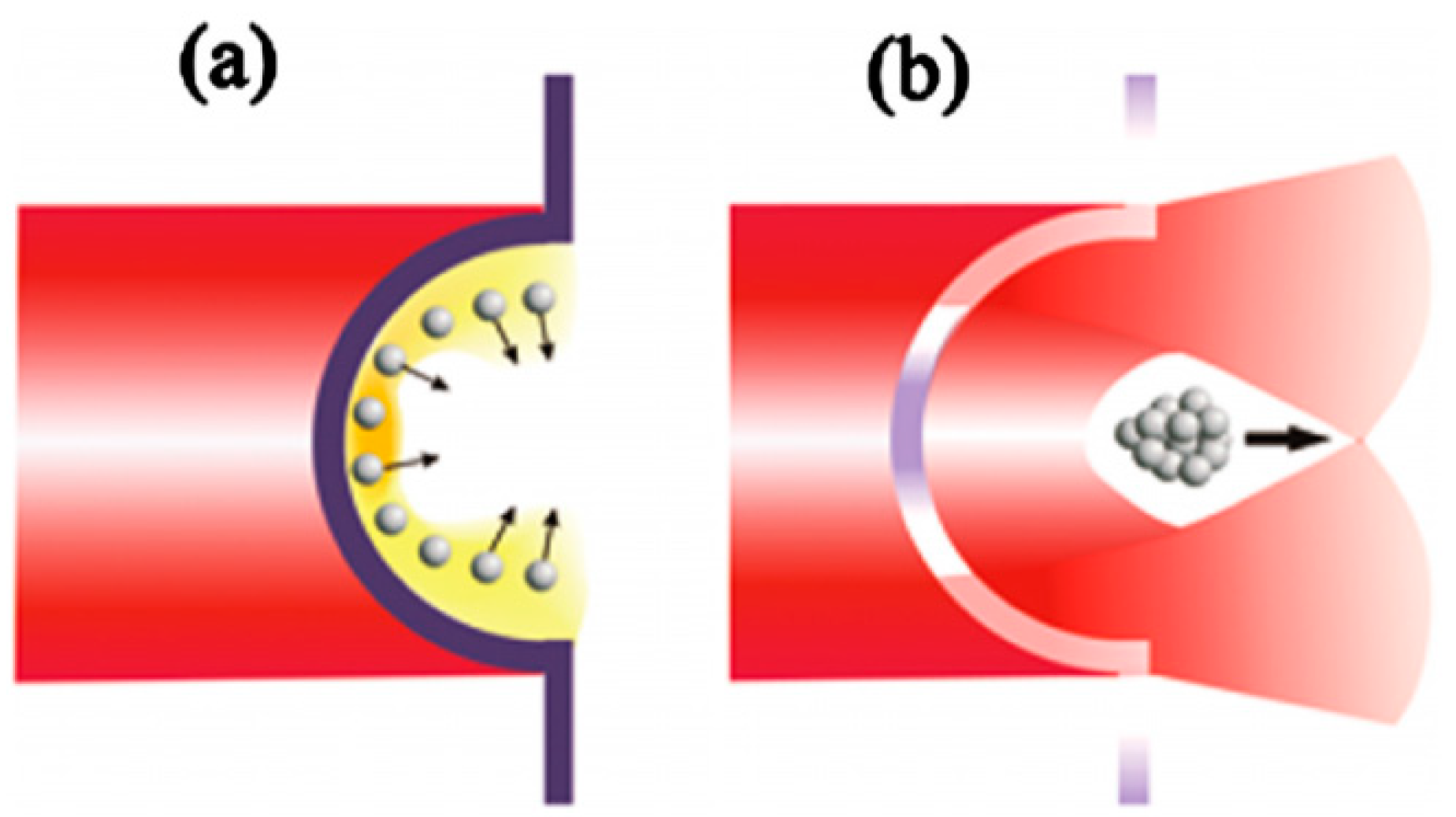
3.3. Angular Divergence Control (Target as an Ion Optic)

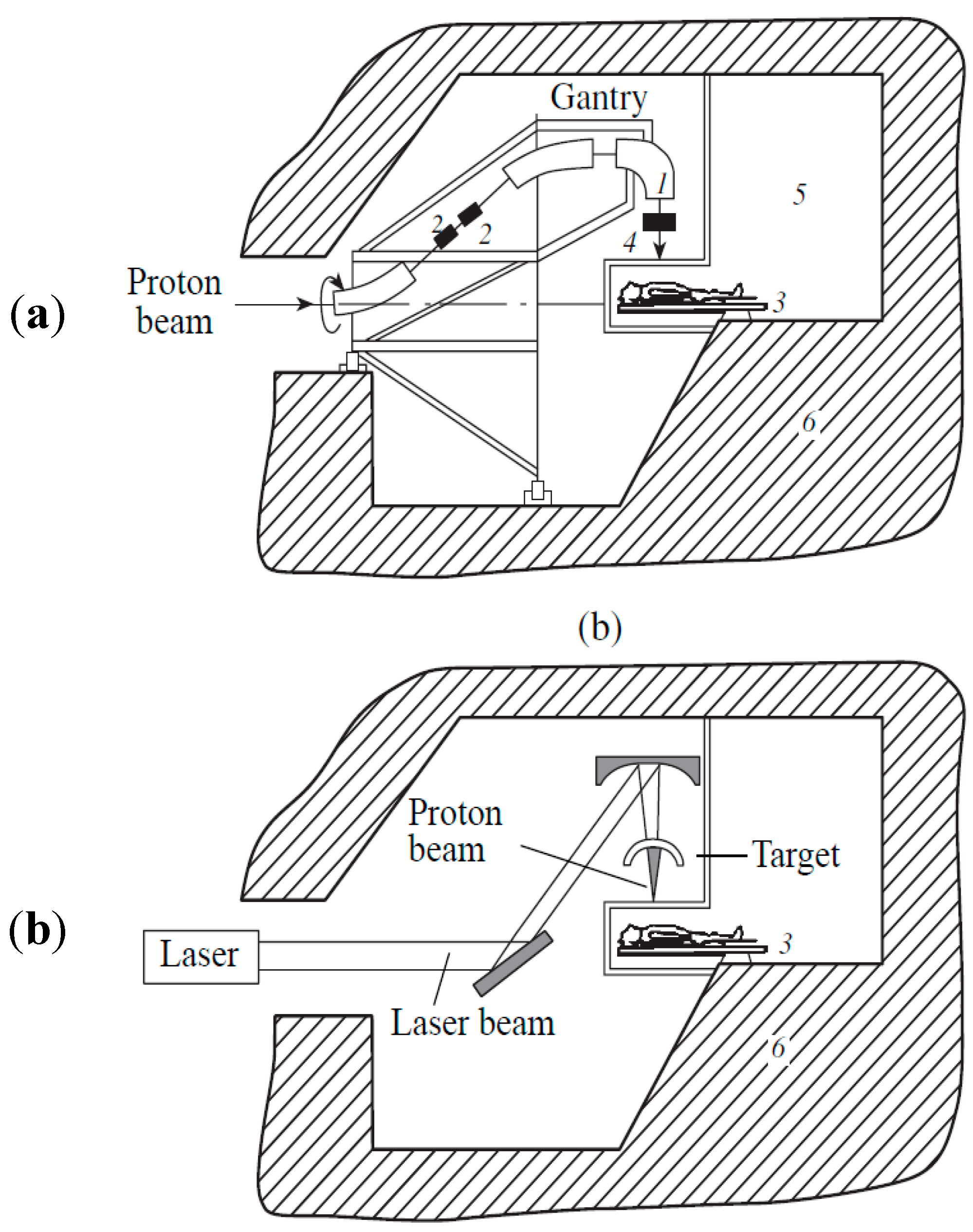
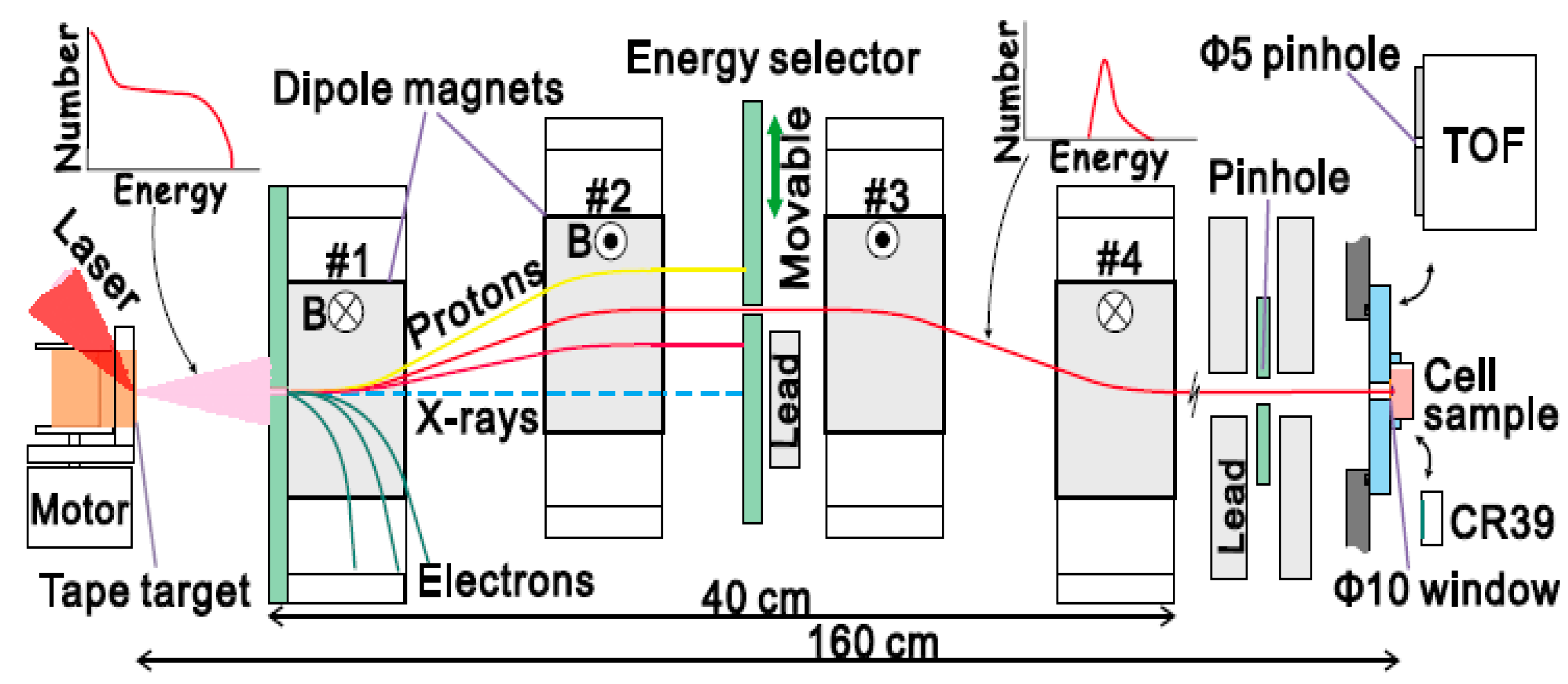
4. Beam Transport and Delivery Considerations


5. Laser Driven Electron Beams for Radiotherapy


6. Cellular Basis of Laser-driven Radiation Therapy
6.1. Important Factors for Determining Cellular Radiation Effect

6.2. DNA Damage Sequence and Biological Effects

6.3. Dose Rate Picture

6.4. Oxygen Effect and Dose Rate
6.5. Laser-driven Radiation in Radiobiological Studies
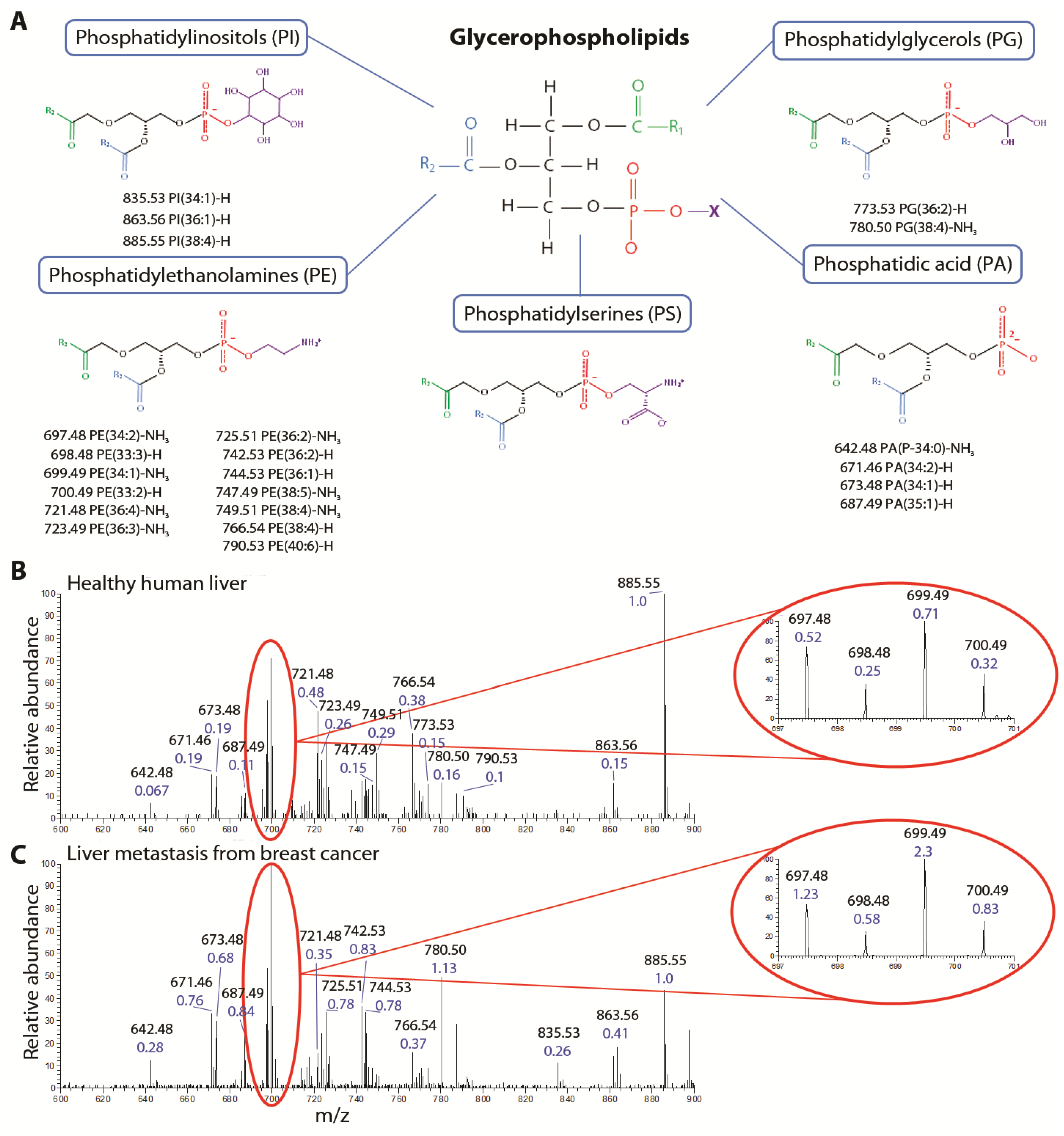
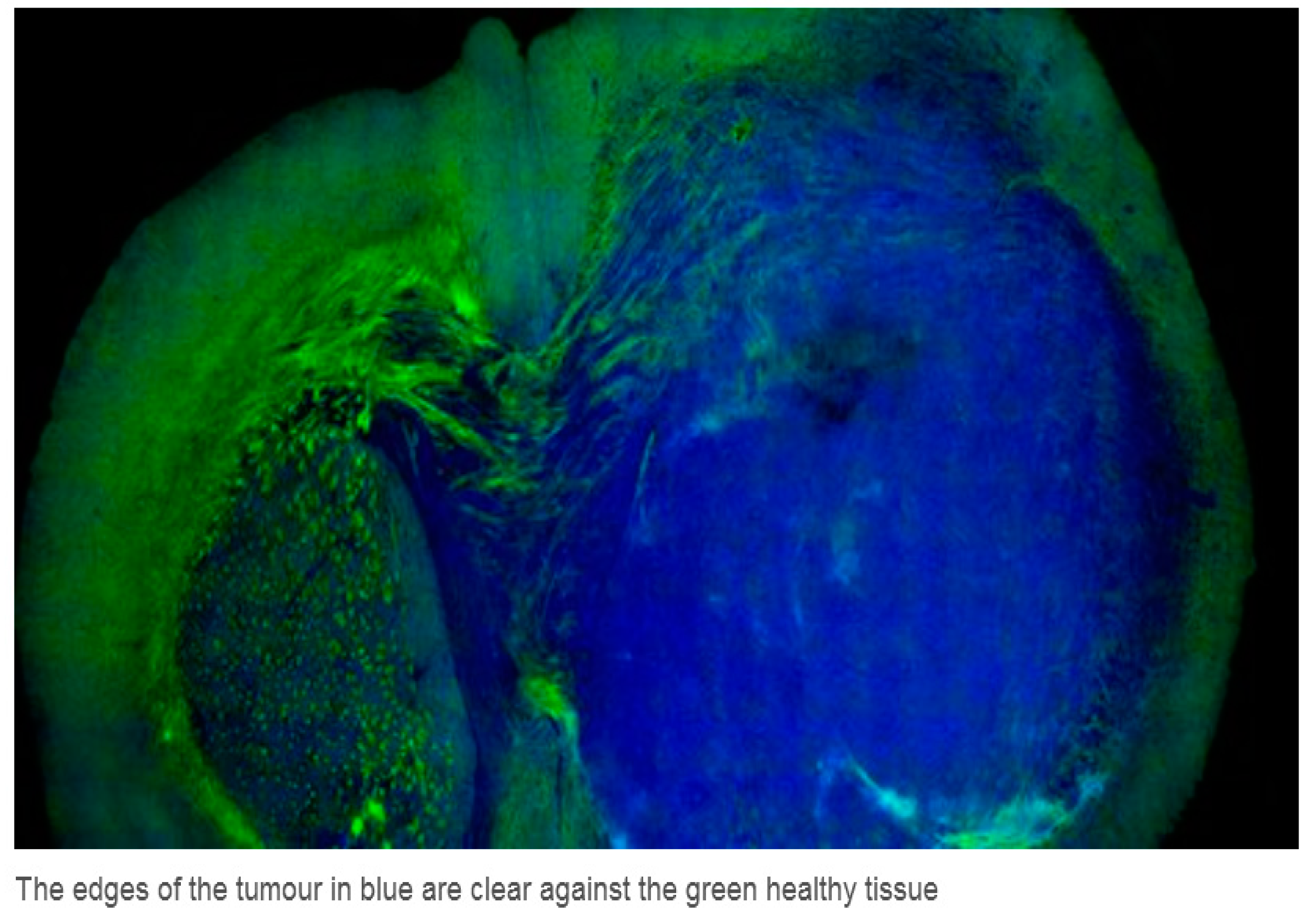
7. Real Time Identification of Healthy and Cancerous Tissue Using Laser Desorption Ionization Mass Spectrometry


8. Some Notable Sites (Current and Planned) Exploring Laser-Acceleration and Potential Medical Applications
8.1. Queens University Belfast Consortium
8.2. Laboratoire d’Optique Appliquée—LOA, Palaiseau, France
8.3. Ion Acceleration Program at BNL ATF and UCLA
8.4. OncoRay—National Center for Radiation Research in Oncology, Dresden
8.5. Laser-Acceleration Studies at JAEA in Japan
8.6. The Munich Centre for Advanced Photonics (MAP)
8.7. ELIMED Prague
8.8. Selcuk/Strathclyde Consortium Konya, Turkey
9. Comparative Radiotherapy Costs


10. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wilson, R.R. Radiological use of fast protons. Radiology 1946, 47, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Proton Therapy. Available online: http://en.wikipedia.org./wiki/Proton (accessed on 9 August 2014).
- Amaldi, U.R.; Bonomi, S.; Braccini, M.; Crescenti, A.; Degiovanni, M.; Garlasché, A.; Garonna, G.; Magrin, C.; Mellace, P.; Pearce, G.; et al. Accelerators for hadron therapy: From lawrence cyclotrons to linacs. Nucl. Instrum. Methods A 2010, 620, 563–577. [Google Scholar] [CrossRef]
- Jones, B. The case for particle therapy. Br. J. Radiol. 2005, 78, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.M.; Maughan, R.L.; Orton, C. Within the next decade conventional cyclotrons for proton therapy will become obsolete and replaced by far less expensive machines using compact laser systems for the acceleration of the protons. Med. Phys. 2006, 33, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Ertner, D.; Jakel, O.; Schlegel, W. Radiation therapy with charged particles. Semin. Radiat. Oncol. 2006, 16, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Scholz, M. Heavy ion tumour therapy. Nucl. Instrum. Methods B 2000, 161–163, 76–82. [Google Scholar]
- Kraft, G. Tumortherapy with Ion Beams. Nucl. Instrum. Methods A 2000, 454, 1–10. [Google Scholar] [CrossRef]
- Schardt, D. Tumour therapy with high energy carbon ion beams. Nucl. Phys. 2007, A787, 633c–641c. [Google Scholar] [CrossRef]
- Fokas, E.; Kraft, G.; An, H.; Engenhart-Cabillic, R. Ion beam radiobiology and cancer: Time to update ourselves. Biochim. Biophys. Acta 2009, 1796, 216–229. [Google Scholar] [PubMed]
- Loeffler, J.S.; Durante, M. Charged particle therapy-optimisation, challenges and future directions. Nat. Rev. Clin. Oncol. 2013, 10, 411–424. [Google Scholar] [CrossRef] [PubMed]
- De Ruysscher, D.; Mark Lodge, M.; Jones, B.; Brada, M.; Munro, A.; Jefferson, T.; Pijls-Johannesma, M. Charged particles in radiotherapy: A 5-year update of a systematic review. Radiother. Oncol. 2012, 103, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Tajima, T.; Habs, D.; Yan, X. Laser acceleration of ions for radiation therapy. Rev. Accel. Sci. Technol. 2009, 2, 201–228. [Google Scholar] [CrossRef]
- Ledingham, K.W.D.; McKenna, P.; Singhal, R.P. Applications of nuclear phenomena generated by ultra-intense lasers. Science 2003, 300, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- Ledingham, K.W.D.; Galster, W. Laser-driven particle and photon beams and some applications. New J. Phys. 2010, 12, 45005–45071. [Google Scholar]
- Daido, H.; Nishiuchi, M.; Pirozhkov, A.S. Review of laser driven ion sources and their applications. Rep. Prog. Phys. 2012, 75. [Google Scholar] [CrossRef]
- Macchi, A.; Borghesi, M.; Passoni, M. Ion acceleration by superintense laser-plasma interaction. Rev. Mod. Phys. 2012, 85, 751–793. [Google Scholar] [CrossRef]
- Bulanov, S.V.; Esirkepov, T.Z.; Khoroshkov, V.S.; Kuznetsov, A.V.; Pegoraro, F. Oncological hadrontherapy with laser ion accelerators. Phys. Lett. A 2002, 229, 240–247. [Google Scholar] [CrossRef]
- Bulanov, S.S.; Bulanov, A.; Bychenkov, V.Y.; Chvykov, V.; Kalinchenko, G.; Matsuoka, T.; Rousseau, P.; Reed, S.; Yanovsky, V.; Krushelnick, K.; et al. Accelerating protons to therapeutic energies with ultraintense, ultraclean and ultrashort laser pulses. Med. Phys. 2008, 3, 1770–1776. [Google Scholar] [CrossRef]
- Ledingham, K. Desktop accelerators going up. Nat. Phys. 2006, 2, 11–12. [Google Scholar] [CrossRef]
- Ledingham, K.W.D.; Galster, W.; Sauerbrey, R. Laser driven proton oncology—A unique new cancer therapy. Br. J. Radiol. 2007, 80, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Martin, M. Laser accelerated radiotherapy: Is it on its way to the clinic? J. Natl. Cancer Inst. 2009, 101, 450–451. [Google Scholar] [CrossRef]
- Laschinsky, L.; Baumann, M.; Beyreuther, E.; Enghardt, W.; Kaluza, M.; Karsch, L.; Lessmann, E.; Naumburger, D.; Nicolai, M.; Richter, C.; et al. Radiobiological effectiveness of laser accelerated electrons in comparison to electron beams from a conventional linear accelerator. J. Radiat. Res. 2012, 55, 395–403. [Google Scholar]
- Malka, V.; Faure, J.; Gauduel, Y.A. Ultra-short Electron Beams based spatio-temporal radiation biology and radiotherapy. Mutat. Res. 2010, 704, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Yogo, A.; Maeda, T.; Hori, T.; Sakaki, H.; Ogura, K.; Nishiuchi, M.; Sagisaka, A.; Kiriyama, H.; Okada, H.; Kanazawa, S.; et al. Measurement of relative biological effectiveness of protons in human cancer cells using a laser driven quasi-monoenergetic proton beamline. Appl. Phys. Lett. 2011, 98, 053701. [Google Scholar] [CrossRef]
- Zeil, K.; Baumann, M.; Beyreuther, E.; Burris-Mog, T.; Cowan, T.E.; Enghardt, W.; Karsch, L.; Kraft, S.D.; Laschinsky, L.; Metzkes, J.; et al. Dose-Controlled irradiation of cancer cells with-laser-accelerated proton pulses. Appl. Phys. B Lasers Opt. 2013, 10, 437–444. [Google Scholar] [CrossRef]
- Metzkes, J.; Cowan, T.E.; Karsch, L.; Kraft, S.D.; Pawelke, J.; Richter, C.; Richter, T.; Zeil, K.; Schramm, U. Preparation of laser-accelerated proton beams for radiobiological applications. Nucl. Instrum. Methods Phys. Res. A 2011, 653, 172–175. [Google Scholar] [CrossRef]
- Linz, U.; Alonso, J. What will it take for laser driven proton accelerators to be applied to tumour therapy? Phys. Rev. ST Accel. Beams 2007, 10, 094801. [Google Scholar] [CrossRef]
- Badziak, J. Laser driven generation of fast particles. Opto-Electron. Rev. 2007, 15, 1–12. [Google Scholar]
- Hatchett, S.P.; Brown, C.G.; Cowan, T.E.; Henry, E.A.; Johnson, J.S.; Key, M.H.; Koch, J.A.; Langdon, A.B.; Lasinski, B.F.; Lee, R.W.; et al. Electron, photon and ion beams from the relativistic interaction of petawatt laser pulses with solid targets. Phys. Plasmas 2000, 7, 2076–2082. [Google Scholar] [CrossRef]
- Wilks, S.C.; Langdon, A.B.; Cowan, T.E.; Roth, M.; Singh, M.; Hatchett, S.; Key, M.H.; Pennington, D.; MacKinnon, A.; Snavely, R.A. Energetic proton generation in ultra-intense laser-solid interactions. Phys. Plasmas 2001, 8, 542–549. [Google Scholar]
- Spencer, I.; Ledingham, K.W.D.; Singhal, R.P.; McCanny, T.; McKenna, P.; Clark, E.L.; Krushelnick, K.; Zepf, M.; Beg, F.N.; Tatarakis, M.; et al. Laser generation of proton beams for the production of short-lived positron emitting radioisotopes. Nucl. Instrum. Methods Phys. Res. B 2001, 183, 449–458. [Google Scholar] [CrossRef]
- Robson, L.; Simpson, P.T.; Clarke, R.J.; Ledingham, K.W.D.; Lindau, F.; Lundh, O.; McCanny, T.; Mora, P.; Neely, D.; Wahlström, C.-G.; et al. Scaling of proton acceleration driven by petawatt-laser-plasma interactions. Nat. Phys. 2007, 3, 58–62. [Google Scholar] [CrossRef]
- Zeil, K.; Kraft, S.D.; Bock, S.; Bussmann, M.; Cowan, T.E.; Kluge, T.; Metzkes, J.; Richter, T.; Sauerbrey, R.; Schramm, U. The scaling of proton energies in ultra-short pulse laser plasma acceleration. New. J. Phys. 2010, 12, 045015. [Google Scholar] [CrossRef]
- Neely, D.; Foster, P.; Robinson, A.; Lindau, F.; Lundh, O.; Persson, A.; Wahlström, C.-G.; McKenna, P. Enhanced proton beams from ultra thin targets driven by high contrast laser pulses. Appl. Phys. Lett. 2006, 89, 021502. [Google Scholar] [CrossRef]
- Yin, L.; Albright, B.J.; Hegelich, B.M.; Fernández, J.C. GeV laser ion acceleration from ultra thin targets: The laser break-out afterburner. Laser Part. Beams 2006, 24, 291–298. [Google Scholar] [CrossRef]
- Albright, B.J.; Yin, L.; Bowers, K.J.; Hegelich, B.M.; Flippo, K.A.; Kwan, T.J.T.; Fernández, J.C. Relativistic buneman instability in the laser breakout afterburner. Phys. Plasmas 2007, 14, 094502. [Google Scholar] [CrossRef]
- Yin, L.; Albright, B.J.; Jung, D.; Shah, R.C.; Palaniyappan, S.; Bowers, K.J.; Henig, A.; Fern´ndez, J.C.; Hegelich, B.M. Break-out afterburner ion acceleration in the longer pulse length regime. Phys. Plasmas 2011, 18, 063103. [Google Scholar] [CrossRef]
- Hegelich, B.M.; Pomerantz, I.; Yin, L.; Wu, H.C.; Jung, D.; Albright, B.J.; Gautier, D.C.; Letzring, S.; Palaniyappan, S.; Shah, R.; et al. Laser driven ion acceleration from relativistically transparent nanotargets. New J. Phys. 2013, 15, 085015. [Google Scholar] [CrossRef]
- Henig, A.; Kiefer, D.; Markey, K.; Gautier, D.C.; Flippo, K.A.; Letzring, S.; Johnson, R.P.; Shimada, T.; Yin, L.; Albright, B.J.; et al. Enhanced laser driven ion acceleration in the relativistic transparency regime. Phys. Rev. Lett. 2009, 103, 045002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, K.; Boucher, S.; O’Shea, F.H. Beam conditioning system for laser driven hadron therapy. In Proceedings of the IPAC2013, Shaghai, China 08 Applications of Accelerators U01 Medical Applications THPWA050, Shanghai, China, 14–19 April 2013.
- Jung, D.; Yin, L.; Albright, B.J.; Gautier, D.C.; Letzring, S.; Dromey, B.; Yeung, M.; Hörlein, R.; Shah, R.; Palaniyappan, S.; et al. Efficient carbon ion beam generation from laser driven volume acceleration. New J. Phys. 2013, 15, 023007. [Google Scholar] [CrossRef] [Green Version]
- Esirkepov, T.; Borghesi, M.; Bulanov, S.V.; Mourou, G.; Tajima, T. Highly efficient relativistic ion generation in the laser-piston regime. Phys. Rev. Lett. 2004, 92, 175003. [Google Scholar] [CrossRef] [PubMed]
- Esirkepov, T.; Yamagiwa, M.; Tajima, T. Laser ion acceleration scaling laws in multiparametric particle-in-cell simulations. Phys. Rev. Lett. 2006, 96, 105001. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.P.L.; Zepf, M.; Kar, S.; Evans, R.G.; Bellei, C. Radiation pressure acceleration of thin foils with circularly polarised laser pulses. New J. Phys. 2008, 10, 013021. [Google Scholar] [CrossRef] [Green Version]
- Qiao, B.; Kar, S.; Geissler, M.; Gibbon, P.; Zepf, M.; Borghesi, M. Dominance of radiation pressure in ion acceleration with linearly polarised pulses at intensities of 1021 W·cm−2. Phys. Rev. Lett. 2012, 108, 115002. [Google Scholar] [CrossRef] [PubMed]
- Haberberger, D.; Tochitsky, S.; Fiuza, F.; Gong, C.; Fonseca, R.A.; Silva, L.O.; Mori, W.B.; Joshi, C. Collisionless shocks in laser-produced plasma generate monoenergetic high-energy proton beams. Nat. Phys. 2012, 8, 95–98. [Google Scholar] [CrossRef]
- Palmer, C.A.J.; Dover, N.P.; Pogorelsky, I.; Babzien, M.; Dudnikova, G.I.; Ispiriyan, M.; Polyanskiy, M.N.; Schreiber, J.; Shkolnikov, P.; Yakimenko, V.; et al. Monoenergetic proton beams accelerated by a radiation pressure driven shock. Phys. Rev. Lett. 2012, 106, 014801. [Google Scholar] [CrossRef]
- Salamin, Y.I.; Harman, Z.; Keitel, C.H. Direct high power laser acceleration of ions for medical applications. Phys. Rev. Lett. 2008, 100, 155004. [Google Scholar] [CrossRef] [PubMed]
- Esirkepov, T.Z.; Bulanov, S.V.; Nishihara, K.; Tajima, T.; Pegoraro, F.; Khoroshkov, V.S.; Mima, K.; Daido, H.; Kato, Y.; Kitagawa, Y.; et al. Proposed double layer target for the generation of high quality laser accelerated ion beams. Phys. Rev. Lett. 2002, 89, 175003. [Google Scholar] [CrossRef] [PubMed]
- Schwoerer, H.; Pfotenhauer, S.; Jäckel, O.; Amthor, K.U.; Liesfeld, B.; Ziegler, W.; Sauerbrey, R.; Ledingham, K.W.; Esirkepov, T. Laser plasma acceleration of quasi-monoenergetic protons from microstructured targets. Nature 2006, 26, 445–452. [Google Scholar] [CrossRef]
- Pfotenhauer, S.M.; Jäckel, O.; Sachtleben, A.; Polz, J.; Ziegler, W.; Schlenvoigt, H.-P.; Amthor, K.-U.; Kaluza, M.C.; Ledingham, K.W.D.; Sauerbrey, R.; et al. Spectral shaping of laser generated proton beams. New J. Phys. 2008, 10, 033034. [Google Scholar] [CrossRef]
- Brantov, A.V.; Tikhonchuk, V.T.; Klimo, O.; Romanov, D.V.; Ter-Avetisyan, S.; Schnürer, M.; Sokollik, T.; Nickles, P.V. Quasi-monoenergetic ion acceleration from a homogeneous composite target by an intense laser pulse. Phys. Plasmas 2006, 13, 122705. [Google Scholar] [CrossRef]
- Robinson, A.P.L.; Gibbon, P. Production of proton beams with narrow band energy spectra from laser irradiated ultrathin foils. Phys. Rev. E 2007, 75, 015401(R). [Google Scholar]
- Toncian, T.; Borghesi, M.; Fuchs, J.; d’Humières, E.; Antici, P.; Audebert, P.; Brambrink, E.; Cecchetti, C.A.; Pipahl, A.; Romagnani, L.; et al. Ultrafast laser-driven microlens to focus and energy select mega-electron volt protons. Science 2006, 21, 410–413. [Google Scholar] [CrossRef]
- Schollmeier, M.; Becker, S.; Geißel, M.; Flippo, K.A.; Blažević, A.; Gaillard, S.A.; Gautier, D.C.; Grüner, F.; Harres, K.; Kimmel, M.; et al. Controlled transport and focusing of laser accelerated protons with miniature magnetic devices. Phys. Rev. Lett. 2008, 101, 055004. [Google Scholar] [CrossRef] [PubMed]
- Melone, J.J.; Ledingham, K.W.D.; McCanny, T.; Burris-Mog, T.; Schramm, U.; Grötzschel, R.; Akhmadaliev, S.; Hanf, D.; Spohr, K.M.; Bussmann, M.; et al. In situ characterisation of permanent magnetic quadrupoles for focussing proton beams. Nucl. Instrum. Methods Phys. Res. A 2012, 676, 126–134. [Google Scholar] [CrossRef]
- Burris-Mog, T.; Harres, K.; Nürnberg, F.; Busold, S.; Bussmann, M.; Deppert, O.; Hoffmeister, G.; Joost, M.; Sobiella, M.; Tauschwitz, A.; et al. Laser accelerated protons captured and transported by a pulse power solenoid. Phys. Rev. ST Accel. Beams 2011, 14, 121301. [Google Scholar] [CrossRef] [Green Version]
- Zigler, A.; Eisenman, S.; Botton, M.; Nahum, E.; Schleifer, E.; Baspaly, A.; Pomerantz, I.; Abicht, F.; Branzel, J.; Priebe, G.; et al. Enhanced proton acceleration by an ultrashort laser interaction with structured dynamic plasma targets. Phys. Rev. Lett. 2013, 110, 215004. [Google Scholar] [CrossRef] [PubMed]
- Botton, M.; Racah Institiute of Physics, Hebrew University, Jerusalem, Israel. Private communication, 2013.
- Wang, H.Y.; Yan, X.Q.; Chen, J.E.; He, X.T.; Ma, W.J.; Bin, J.H.; Schreiber, J.; Tajima, T.; Habs, D. Efficient and stable proton acceleration by irradiating a two layer target with a linearly polarised laser pulse. Phys. Plasmas 2013, 20, 013101. [Google Scholar] [CrossRef]
- Patel, P.K.; Mackinnon, A.J.; Key, M.H.; Cowan, T.E.; Foord, M.E.; Allen, M.; Price, D.F.; Ruhl, H.; Springer, P.T.; Stephens, R. Isochoric heating of solid-density matter with an ultrafast proton beam. Phys. Rev. Lett. 2003, 91, 125004. [Google Scholar] [CrossRef] [PubMed]
- Snavely, R.A.; Zhang, B.; Akli, K.; Chen, Z.; Freeman, R.R.; Gu, P.; Hatchett, S.P.; Hey, D.; Hill, J.; Key, M.H.; et al. Laser generated proton beam focusing and high temperature isochoric heating of solid matter. Phys. Plasmas 2007, 14, 092703. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.Y.; Yan, X.Q.; Lu, Y.R.; Zheng, F.L.; Guo, Z.Y.; Ma, W.J.; He, X.T.; Tajima, T.; Habs, D.; Chen, J.E. Autofocused, enhanced proton acceleration from a nanometer-scale bulged foil. Phys. Plasmas 2010, 17, 113111. [Google Scholar] [CrossRef]
- Bin, J.H.; Ma, W.J.; Allinger, K.; Wang, H.Y.; Kiefer, D.; Reinhardt, S.; Hilz, P.; Khrennikov, K.; Karsch, S.; Yan, X.Q.; et al. On the small divergence of laser driven ion beams from nanometer thick foils. Phys. Plasmas 2013, 20, 073113. [Google Scholar] [CrossRef]
- Bartel, T.; Foord, M.E.; Bellei, C.; Key, M.H.; Flippo, K.A.; Gaillard, S.A.; Offermann, D.T.; Patel, P.K.; Jarrott, L.C.; Higginson, D.P.; et al. Focussing of short-pulse high intensity laser accelerated proton beams. Nat. Phys. 2012, 8, 139. [Google Scholar] [CrossRef]
- Tajima, T. Prospect for campact medical laser accelerators. J. Jpn. Soc. Ther. Radiol. Oncol. 1998, 9, 83–85. [Google Scholar]
- Bulanov, S.V.; Khoroshkov, V.S. Feasibility of using laser ion accelerators in proton therapy. Plasma Phys. Rep. 2002, 28, 453–456. [Google Scholar] [CrossRef]
- Malka, V.; Fritzler, S.; Lefebvre, E.; d’Humières, E.; Ferrand, R.; Grillon, G.; Albaret, C.; Meyroneinc, S.; Chambaret, J.-P.; Antonetti, A.; et al. Practicability of proton therapy using compact laser systems. Med. Phys. 2004, 31, 1587–1892. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.-M.; Tajima, T.; Shahine, B.; Lee, M.C.; Guerrero, T.; Boyer, A.L. Laser accelerated proton beams for radiation therapy. Med. Phys. 2001, 28, 1236. [Google Scholar] [CrossRef]
- Fourkal, E.; Li, J.S.; Ding, M.S.; Tajima, T.; Ma, C.-M. Particle selection for laser accelerated proton therapy feasibility study. Med. Phys. 2003, 30, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Fourkal, E.; Li, J.S.; Ma, C.-M. Particle selection and beam collimation for laser accelerated proton beam therapy. Med. Phys. 2005, 32, 794–806. [Google Scholar] [CrossRef] [PubMed]
- Nishiuchi, M.; Sakaki, H.; Hori, T.; Bolton, P.R.; Ogura, K.; Sagisaka, A.; Yogo, A.; Mori, M.; Orimo, S.; Pirozhkov, A.S.; et al. Measured and simulated transport of 1.9 MeV laser-accelerated proton bunches through an integrated test beam line at 1 Hz. Phys. Rev. Spec. Top. Accel. Beams 2010, 13, 071304. [Google Scholar]
- Fan, J.; Luo, W.; Fourkal, E.; Lin, T.; Li, J.S.; Veltchev, I.; Ipe, N.; Ma, C.-M. Shielding design for a laser accelerator proton therapy system. Phys. Med. Biol. 2007, 52, 3913–3930. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.-M.; Veltchev, I.; Fourkal, E.; Li, J.S.; Luo, W.; Fan, J.J.; Lin, T.; Pollack, A. Development of a laser driven proton accelerator for cancer therapy. Laser Phys. 2006, 16, 639–646. [Google Scholar] [CrossRef]
- Ma, C.-M. New Developments in Proton Therapy Systems, Laser Driven Relativistic Plasmas Applied to Science, Industry and Medicine 2nd International Symposium; Bolton, P.R., Bulanov, S.V., Daido, H., Eds.; American Institute of Physics: College Park, MD, USA, 2009; p. 388. [Google Scholar]
- Hoffman, I.; Meyer-ter-Vehn, J.; Yan, X.; Orzhekhovskaya, A.; Yaramyshev, S. Collection and focussing of laser accelerator ion beams for therapy applications. Phys. Rev. Spec. Top. Accel. Beams 2011, 14, 031304. [Google Scholar] [CrossRef]
- Hoffman, I.; Meyer-ter-Vehn, J.; Yan, X.; Al-Omari, H. Chromatic energy filter and characterisation of laser accelerated proton beams for particle therapy. NIM Phys. Res. A 2012, 681, 44–54. [Google Scholar] [CrossRef]
- Schell, S.; Wilkins, J.J. Advanced treatment planning methods for efficient radiation therapy with laser accelerated proton and ion beams. Med. Phys. 2010, 37, 5330–5340. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, K.M.; Schell, S.; Wilkens, J.J. Laser driven beam lines for delivering intensity modulated radiation therapy with particle beams. J. Biophotonics 2012, 5, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Hogstrom, K.R.; Almond, P.R. Review of electron beam therapy physics. Phys. Med. Biol. 2006, 5, R455–R489. [Google Scholar] [CrossRef]
- Faure, J.; Glinec, Y.; Pukhov, A.; Kiselev, S.; Gordienko, S.; Lefebvre, E.; Rousseau, J.-P.; Burgy, F.; Malka, V. A laser-plasma accelerator producing monoenergetic electron beams. Nature 2004, 431, 541–544. [Google Scholar] [CrossRef]
- Hafz, N.; Jeong, T.M.; Lee, S.K.; Pae, K.H.; Sung, J.H.; Choi, I.W.; Yu, T.J.; Jeong, Y.U.; Lee, J. Laser driven electron beam acceleration and future application to compact light sources. In Laser Driven Relativistic Plasmas Applied to Science, Industry and Medicine 2nd International Symposium; Bolton, P.R., Bulanov, S.V., Daido, H., Eds.; American Institute of Physics: College Park, MD, USA, 2009; p. 167. [Google Scholar]
- Glinec, Y.; Faure, J.; Malka, V.; Fuchs, T.; Szymanowski, H.; Oelfke, U. Radiotherapy with laser-plasma accelerators: Monte Carlo simulation of dose deposited by an experimental quasimonoenergetic electron beam. Med. Phys. 2006, 33, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, O.; Fortunel, N.O.; Vaigot, P.; Cadio, E.; Martin, M.T.; Lundh, O.; Faure, J.; Rechatin, C.; Malka, V.; Gauduel, Y.A. Exploring ultrashort high energy electron induced damage in human carcinoma cells. Cell Death Dis. 2010, 1, e73. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.; Szymanowski, H.; Oelfke, U.; Glinec, Y.; Rechatin, C.; Faure, J.; Malka, V. Treatment planning for laser accelerated very high energy electrons. Phys. Med. Biol. 2009, 54, 3315–3328. [Google Scholar] [CrossRef] [PubMed]
- Lundh, O.; Rechatin, C.; Faure, J.; Ben-Ismaïl, A.; Lim, J.; de Wagter, C.; de Neve, W.; Malka, V. Comparison of mesured with calculated dose distribution from 120 MeV electron beam from a laser plasma accelerator. Med. Phys. 2012, 39, 3501–3508. [Google Scholar] [CrossRef] [PubMed]
- Mothersill, C.; Seymour, C. Are epigenetic mechanisms involved in radiation-induced bystander effects? Front. Genet. 2012, 3, 74. [Google Scholar]
- Butterworth, K.T.; McMahon, S.J.; Hounsell, A.R.; O’Sullivan, J.M.; Prise, K.M. Bystander signalling: Exploring clinical relevance through new approaches and new models. Clin. Oncol. R. Coll. Radiol. 2013, 25, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J.; Giaccia, A.J. Radiobiology for the Radiologist; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Goodhead, D.T. Initial events in the cellular effects of ionizing radiations: Clustered damage in DNA. Int. J. Radiat. Biol. 1994, 65, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.F. The complexity of DNA damage: Relevance to biological consequences. Int. J. Radiat. Biol. 1994, 66, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Mozumder, A.; Hatano, Y. Charged Particle and Photon Interactions with Matter: Chemical, Physicochemical, and Biological Consequences with Applications; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Berlin, Y.A.; Siebbeles, D.A. Radiation Chemistry: From Basics to Applications in Material and Life Sciences; EDP Sciences: Les Ulis, France, 2008. [Google Scholar]
- Roots, R.; Okada, S. Estimation of life times and diffusion distances of radicals involved in X-ray-induced DNA strand breaks of killing of mammalian cells. Radiat. Res. 1975, 64, 306–320. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, K.; Nakano, H.; Miyazaki, N.; Tago, M.; Kodama, R. Effects of single-pulse (<or =1 ps) X-rays from laser-produced plasmas on mammalian cells. J. Radiat. Res. 2004, 45, 509–514. [Google Scholar]
- Hill, M.A.; Stevens, D.L.; Marsden, S.J.; Allott, R.; Turcu, I.C.E.; Goodhead, D.T. Is the increased relative biological effectiveness of high LET particles due to spatial or temporal effects? Characterization and OER in V79-4 cells. Phys. Med. Biol. 2002, 47, 3543–3555. [Google Scholar] [CrossRef] [PubMed]
- Tillman, C.; Grafström, G.; Jonsson, A.C.; Jönsson, B.A.; Mercer, I.; Mattsson, S.; Strand, S.E.; Svanberg, S. Survival of mammalian cells exposed to ultrahigh dose rates from a laser-produced plasma X-ray source. Radiology 1999, 213, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Kreipl, M.S.; Friedland, W.; Paretzke, H.G. Interaction of ion tracks in spatial and temporal proximity. Radiat. Environ. Biophys. 2009, 48, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Doria, D.; Kakolee, K.F.; Kar, S.; Litt, S.K.; Fiorini, F.; Ahmed, H.; Green, S.; Jeynes, J.C.G.; Kavanagh, J.; Kirby, D.; et al. Biological effectiveness on live cells of laser driven proton exceeding 109 Gy/s. AIP Adv. 2012, 2, 011209. [Google Scholar] [CrossRef] [Green Version]
- Fourkal, E.; Velchev, I.; Ma, C.-M.; Fan, J. Linear energy transfer of proton clusters. Phys. Med. Biol. 2011, 56, 3123–3136. [Google Scholar] [CrossRef] [PubMed]
- Kainz, K.K.; Hogstrom, K.R.; Antolak, J.A.; Almond, P.R.; Bloch, C.D.; Chiu, C.; Fomytskyi, M.; Raischel, F.; Downer, M.; Tajima, T. Dose properties of a laser accelerated electron beam and prospects for clinical application. Med. Phys. 2004, 31, 2053–2067. [Google Scholar] [CrossRef] [PubMed]
- Kainz, K.K.; Hogstrom, K.R.; Antolak, J.A.; Almond, P.R.; Bloch, C.D. Dose properties of X-ray beams produced by laser wake-field-accelerated electrons. Phys. Med. Biol. 2005, 50, N1–N10. [Google Scholar] [CrossRef] [PubMed]
- Schell, S.; Wilkens, J.J. Dosimetric effects of energy spectrum uncertainties in radiation therapy with laser driven particle beams. Phys. Med. Biol. 2012, 57, N47–N53. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.-M.; Fourkal, E.; Veltchev, I.; Li, J.S.; Fan, J.; Lin, T.; Tafo, A. Development of laser accelerated proton beams for radiation therapy. In Proceedings of the WC 2009, IFMBE Proceedings 25/XIII, Munich, Germany, 7–12 September 2009; Dössel, O., Schlegel, W.C., Eds.; Springer: Heidelberg, Germany, 2009; pp. 66–69. [Google Scholar]
- Wilson, P.; Jones, B.; Yokoi, T.; Hill, M.; Vojnovic, B. Revisiting the ultra-high dose rate effect: Implications for charged particle radiotherapy using protons and light ions. Br. J. Radiol. 2012, 85, e933–e939. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, V. Free-Radical Induced DNA Damage and Its Repair: A Chemical Perspective; Springer: Berlin, Germany, 2006. [Google Scholar]
- Bin, J.; Allinger, K.; Assmann, W.; Dollinger, G.; Drexler, G.A.; Friedl, A.A.; Habs, D.; Hilz, P.; Hoerlein, R.; Humble, N.; et al. A laser driven nanosecond proton source for radiobiological studies. Appl. Phys. Lett. 2012, 101, 243701. [Google Scholar] [CrossRef]
- Auer, S.; Hable, V.; Greubel, C.; Drexler, G.A.; Schmid, T.E.; Belka, C.; Dollinger, G.; Friedl, A.A. Survival of tumour cells after proton irradiation with ultra-high dose rates. Radiat. Oncol. 2011, 6, 139. [Google Scholar] [CrossRef] [PubMed]
- Ledingham, K.W.D.; Singhal, R.P. High intensity laser mass spectrometry—A review. Int. J. Mass Spectrom. Ion Processes 1997, 163, 149–168. [Google Scholar] [CrossRef]
- Takats, Z.; Wiseman, J.M.; Gologan, B.; Cooks, R.G. Mass spectrometry sampling under ambient conditions with desorption electrospray ionization. Science 2004, 306, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, K.-C.; Dénes, J.; Albrecht, K.; Szaniszló, T.; Balog, J.; Skoumal, R.; Katona, M.; Tóth, M.; Balogh, L.; Takáts, Z. In vivo, in situ tissue analysis using rapid evaporative ionization mass spectrometry. Angew. Chem. Int. Ed. 2009, 48, 8240–8242. [Google Scholar] [CrossRef]
- Balog, J.; Szaniszlo, T.; Schaefer, K.C.; Denes, J.; Lopata, A.; Godorhazy, L.; Szalay, D.; Balogh, L.; Sasi-Szabo, L.; Toth, M.; et al. Identification of biological tissue by rapid evaporative ionization mass spectrometry. Anal. Chem. 2010, 82, 7343–7350. [Google Scholar] [CrossRef] [PubMed]
- Sächfer, K.C.; Szaniszló, T.; Günther, S.; Balog, J.; Dénes, J.; Keseru, M.; Dezso, B.; Tóth, M.; Spengler, B.; Takáts, Z. In situ, real-time identification of biological tissue by ultraviolet and infrared laser desorption ionization mass spectrometry. Anal. Chem. 2011, 83, 1632–1640. [Google Scholar] [CrossRef] [PubMed]
- Bolag, J.; Sasi-Szabó, L.; Kinross, J.; Lewis, M.R.; Muirhead, L.J.; Veselkov, K.; Mirnezami, R.; Dezső, B.; Damjanovich, L.; Darzi, A.; et al. Intraoperative tissue identification using rapid evaporative ionization mass spectrometry. Sci. Transl. Med. 2013, 5, 194ra93. [Google Scholar]
- Ji, M.; Orringer, D.A.; Freudiger, C.W.; Ramkissoon, S.; Liu, X.; Lau, D.; Golby, A.J.; Norton, I.; Hayashi, M.; Agar, N.Y.R.; et al. Rapid, label-free detection of brain tumors with stimulated raman scattering microscopy. Sci. Transl. Med. 2013, 5, 201ra119. [Google Scholar] [CrossRef] [PubMed]
- Leemans, W.; Chou, W.; Uesaka, M. High power laser for accelerator. ICFA Beam Dyn. Newsl. 2011, 56, 51–60. [Google Scholar]
- D’Humieres, E.; Lefebvre, E.; Gremillet, L.; Malka, V. Proton acceleration mechanisms in high-intensity laser interaction with thin foils. Phys. Plasmas 2005, 12, 062704. [Google Scholar] [CrossRef]
- Fiuza, F.; Stockem, A.; Boella, E.; Fonseca, R.A.; Silva, L.O.; Haberberger, D.; Tochitsky, S.; Mori, W.B.; Joshi, C. Ion acceleration from laser-driven electrostatic shocks. Phys. Plasmas 2013, 20, 056304. [Google Scholar] [CrossRef]
- Yogo, A.; Sato, K.; Nishikino, M.; Mori, M.; Teshima, T.; Numasaki, H.; Murakami, M.; Demizu, Y.; Akagi, S.; Nagayama, S.; et al. Application of laser-accelerated protons to the demonstration of DNA double-strand breaks in human cancer cells. Appl. Phys. Lett. 2009, 94, 181502. [Google Scholar] [CrossRef]
- Ogura, K.; Nishiuchi, M.; Pirozhkov, A.S.; Tanimoto, T.; Sagisaka, A.; Esirkepov, T.Z.; Kando, M.; Shizuma, T.; Hayakawa, T.; Kiriyama, H.; et al. Proton acceleration to 40 MeV using a high intensity, high contrast OPCPA/Ti: Sapphire hybrid laser system. Opt. Lett. 2012, 37, 2868. [Google Scholar] [CrossRef] [PubMed]
- Sinigardi, S.; Turchetti, G.; Rossi, F.; Londrillo, P.; Giove, D.; de Martinis, C.; Bolton, P.R. High quality proton beams from hybrid integrated laser-driven ion acceleration systems. NIM 2014, 740, 99–104. [Google Scholar] [CrossRef]
- Kacperek, A.; Clatterbridge Centre, Liverpool, UK. Private communication, 2013.
- Peeters, A.; Grutters, J.P.; Pijls-Johannesma, M.; Reimoser, S.; de Ruysscher, D.; Severens, J.L.; Joore, M.A.; Lambin, P. How costly is particle therapy? Cost analysis of external beam therapy with carbon-ions, protons and photons. Radiother. Oncol. 2010, 95, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Lodge, M.; Pijls-Johannesma, M.; Stirk, L.; Munro, A.J.; de Ruysscher, D.; Jefferson, T. A systematic literature review of the clinical and cost-effectiveness of hadron therapy in cancer. Radiother. Oncol. 2007, 83, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Malka, V.; Faure, J.; Gauduel, Y.A.; Lefebvre, E.; Rousse, A.; Phuoc, K.T. Principles and applications of compact-plasma accelerators. Nat. Phys. 2008, 4, 447–453. [Google Scholar] [CrossRef]
- Sheenan, M.; Timlin, C.; Peach, K.; Binik, A.; Puthenparampil, W.; Lodge, M.; Kehoe, S.; Brada, M.; Burnet, N.; Clarke, S.; et al. Position statement on ethics, equipoise, and research on charged particle radiation therapy. J. Med. Eth. 2013, 17. [Google Scholar] [CrossRef]
- Miller, R.C.; Lodge, M.; Murad, M.H.; Jones, B. Controversies in clinical trials in proton radiotherapy: The present and the future. Semin. Radiat. Oncol. 2013, 23, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Epstein, K. Is spending on proton beam therapy for cancer going too far, too fast? BMJ 2012, 344, 20–21. [Google Scholar]
- Burnet, N.G.; Taylor, R.E.; Kirkby, K.J.; Thorp, N.; Mackay, R.I.; McKenna, G. Re: Is spending on proton beam therapy for cancer going too far, too fast? BMJ 2012, 344, e2488. Available online: http://www.bmj.com/content/344/bmj.e2488/rr/581410 (accessed on 9 August 2014). [Google Scholar] [CrossRef]
- Girault-Rime, M. Towards Compact Proton Therapy; CNRS International Magzine: Paris, France, 2006. No. 2. Available online: http://www2.cnrs.fr/en/518.htm 2013 (accessed on 9 August 2014).
- Leemans, W.; Laurence Berkeley National Lab, Berkeley, CA, USA. Private communication, 2013.
- Freeman, T. Pulsed Lasers Could Make Proton Therapy More Accessible. Available online: http://physicsworld.com/cws/article/news/2013/jan/16/pulsed-lasers-could-make-proton-therapy-more-accessible (accessed on 9 August 2014).
- McEntee, J. Laser-based Acceleration: Designs on Proton Therapy. Available online: http://medicalphysicsweb.org/cws/article/opinion/47765 (accessed on 9 August 2014).
- Hayes, T. Lasers Bring Proton Therapy within Easier Reach. Available online: http://optics.org/news/10/154 (accessed on 9 December 2013).
- Cowan, T.; Schramm, U.; Burris-Mog, T.; Fiedler, F.; Kraft, S.D.; Zeil, K.; Baumann, M.; Bussmann, M.; Enghardt, W.; Flippo, K.; et al. Advanced Accelerator Concepts: 14th Advanced Accelerator Concepts Workshop, AIP Conference Proceedings; American Institute of Physics: College Park, MD, USA, 2010; Volume 1299, pp. 721–726.
- Kleeven, W.J.G.M. The IBA superconducting synchrocyclotron project S2C2. In Proceedings of the Cyclotrons’13 20th International Conference on Cyclotrons and their Applications, Vancouver, BC, Canada, 16–20 September 2013.
- Nuttens, V.; Kleeven, W.J.G.M.; L’Abbate, C.; Nuttens, V.; Paradis, Y.; Conjat, M.; Mandrillon, J.; Mandrillon, P. Mapping of the new IBA superconducting synchrocyclotron (S2C2) for proton therapy. In Proceedings of the Cyclotrons’13 20th International Conference on Cyclotrons and their Applications, Vancouver, BC, Canada, 16–20 September 2013.
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ledingham, K.W.D.; Bolton, P.R.; Shikazono, N.; Ma, C.-M.C. Towards Laser Driven Hadron Cancer Radiotherapy: A Review of Progress. Appl. Sci. 2014, 4, 402-443. https://doi.org/10.3390/app4030402
Ledingham KWD, Bolton PR, Shikazono N, Ma C-MC. Towards Laser Driven Hadron Cancer Radiotherapy: A Review of Progress. Applied Sciences. 2014; 4(3):402-443. https://doi.org/10.3390/app4030402
Chicago/Turabian StyleLedingham, Ken W. D., Paul R. Bolton, Naoya Shikazono, and C.-M. Charlie Ma. 2014. "Towards Laser Driven Hadron Cancer Radiotherapy: A Review of Progress" Applied Sciences 4, no. 3: 402-443. https://doi.org/10.3390/app4030402