Disturbed Mental Imagery of Affected Body-Parts in Patients with Hysterical Conversion Paraplegia Correlates with Pathological Limbic Activity


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patients
3. Methods
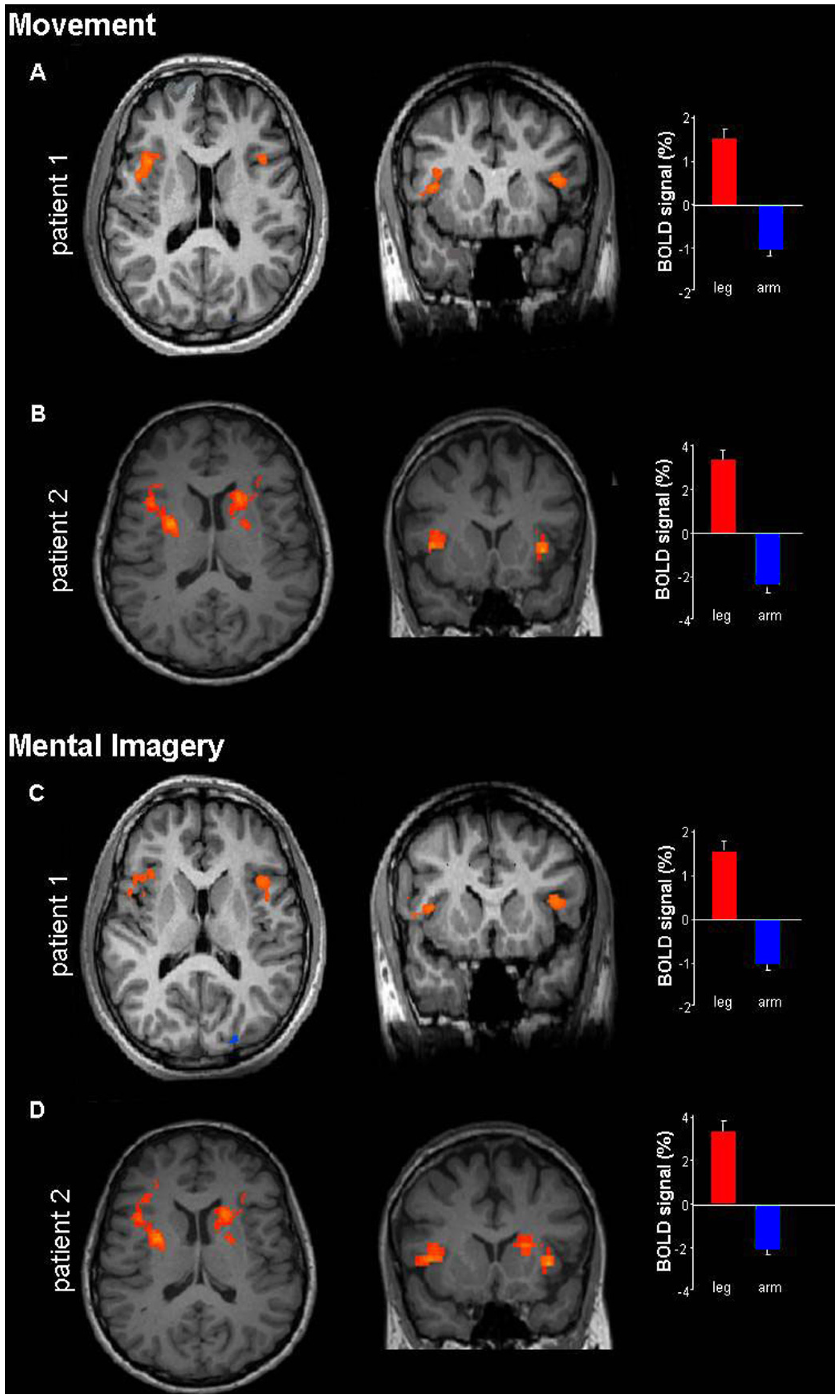
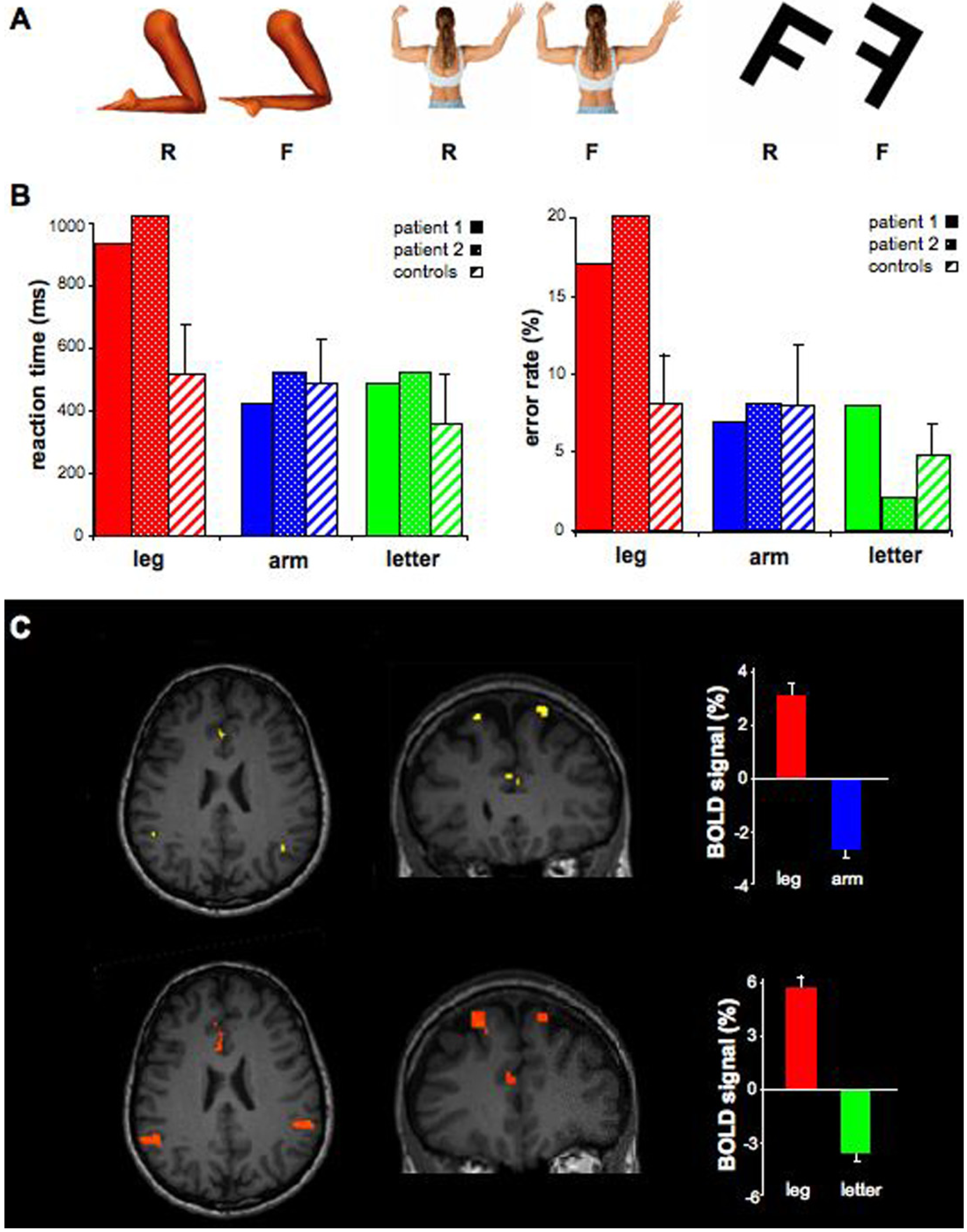
4. Results


5. Discussion
6. Conclusion
Supplementary Files
Acknowledgments
Conflicts of Interest
References
- Vuilleumier, P. Hysterical conversion and brain function. Prog. Brain Res. 2005, 150, 309–329. [Google Scholar] [CrossRef]
- Charcot, J.M. Clinical Lectures on the Diseases of the Nervous System; Routledge: London, UK, 1990. [Google Scholar]
- Janet, P. The Major Symptoms of Hysteria; Fifteen Lectures Given in the Medical School of Harvard University, 2nd ed.; The Macmillan Company: New York, NY, USA, 1920. [Google Scholar]
- Breuer, J.; Freud, S. Studies in Hysteria; Penguin: London, UK, 2004. [Google Scholar]
- Flor-Henry, P.; Fromm-Auch, D.; Tapper, M.; Schopflocher, D. A neuropsychological study of the stable syndrome of hysteria. Biol. Psychiatry 1981, 16, 601–626. [Google Scholar]
- Black, D.N.; Seritan, A.L.; Taber, K.H.; Hurley, R.A. Conversion hysteria: Lessons from functional imaging. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 245–251. [Google Scholar] [CrossRef]
- Mailis-Gagnon, A.; Giannoylis, I.; Downar, J.; Kwan, C.L.; Mikulis, D.J.; Crawley, A.P.; Nicholson, K.; Davis, K.D. Altered central somatosensory processing in chronic pain patients with “hysterical” anesthesia. Neurology 2003, 60, 1501–1507. [Google Scholar] [CrossRef]
- Tiihonen, J.; Kuikka, J.; Viinamaki, H.; Lehtonen, J.; Partanen, J. Altered cerebral blood flow during hysterical paresthesia. Biol. Psychiatry 1995, 37, 134–135. [Google Scholar] [CrossRef]
- Vuilleumier, P. Hysterical conversion and brain function. Prog. Brain Res. 2005, 150, 309–329. [Google Scholar] [CrossRef]
- Yazici, K.M.; Kostakoglu, L. Cerebral blood flow changes in patients with conversion disorder. Psychiatry Res. 1998, 83, 163–168. [Google Scholar] [CrossRef]
- Hoechstetter, K.; Meinck, H.M.; Henningsen, P.; Scherg, M.; Rupp, A. Psychogenic sensory loss: Magnetic source imaging reveals normal tactile evoked activity of the human primary and secondary somatosensory cortex. Neurosci. Lett. 2002, 323, 137–140. [Google Scholar] [CrossRef]
- Ghaffar, O.; Staines, W.R.; Feinstein, A. Unexplained neurologic symptoms: An fMRI study of sensory conversion disorder. Neurology 2006, 67, 2036–2038. [Google Scholar]
- Marshall, J.C.; Halligan, P.W.; Fink, G.R.; Wade, D.T.; Frackowiak, R.S. The functional anatomy of a hysterical paralysis. Cognition 1997, 64, B1–B8. [Google Scholar] [CrossRef]
- Spence, S.A.; Crimlisk, H.L.; Cope, H.; Ron, M.A.; Grasby, P.M. Discrete neurophysiological correlates in prefrontal cortex during hysterical and feigned disorder of movement. Lancet 2000, 355, 1243–1244. [Google Scholar] [CrossRef]
- Stone, J.; Zeman, A.; Simonotto, E.; Meyer, M.; Azuma, R.; Flett, S.; Sharpe, M. FMRI in patients with motor conversion symptoms and controls with simulated weakness. Psychosom. Med. 2007, 69, 961–969. [Google Scholar] [CrossRef]
- De Lange, F.P.; Roelofs, K.; Toni, I. Increased self-monitoring during imagined movements in conversion paralysis. Neuropsychologia 2007, 45, 2051–2058. [Google Scholar] [CrossRef]
- Arzy, S.; Overney, L.S.; Landis, T.; Blanke, O. Neural mechanisms of embodiment: Asomatognosia due to premotor cortex damage. Arch. Neurol. 2006, 63, 1022–1025. [Google Scholar] [CrossRef]
- Roelofs, K.; van Galen, G.P.; Keijsers, G.P.J.; Hoogduin, C.A.L. Motor initiation and execution in patients with conversion paralysis. Acta Psychol. 2002, 110, 21–34. [Google Scholar] [CrossRef]
- Zeharia, N.; Hertz, U.; Flash, T.; Amedi, A. Negative blood oxygenation level dependent homunculus and somatotopic information in primary motor cortex and supplementary motor area. Proc. Natl. Acad. Sci. USA 2012, 109, 18565–18570. [Google Scholar] [CrossRef]
- Halligan, P.W.; Athwal, B.S.; Oakley, D.A.; Frackowiak, R.S. Imaging hypnotic paralysis: Implications for conversion hysteria. Lancet 2000, 355, 986–987. [Google Scholar] [CrossRef]
- Saj, A.; Arzy, S.; Vuilleumier, P. Functional brain imaging in a woman with spatial neglect due to conversion disorder. JAMA 2009, 302, 2552–2554. [Google Scholar]
- Augustine, J.R. Circuitry and functional aspects of the insular lobe in primates including humans. Brain Res. Brain Res. Rev. 1996, 22, 229–244. [Google Scholar] [CrossRef]
- Nagai, M.; Kishi, K.; Kato, S. Insular cortex and neuropsychiatric disorders: A review of recent literature. Eur. Psychiatry 2007, 22, 387–394. [Google Scholar] [CrossRef]
- Aybek, S.; Kanaan, R.A.; David, A.S. The neuropsychiatry of conversion disorder. Curr. Opin. Psychiatry 2008, 21, 275–280. [Google Scholar] [CrossRef]
- Liepert, J.; Hassa, T.; Tüscher, O.; Schmidt, R. Electrophysiological correlates of motor conversion disorder. Mov. Disord. 2008, 23, 2171–2176. [Google Scholar] [CrossRef]
- Maruff, P.; Velakoulis, D. The voluntary control of motor imagery. Imagined movements in individuals with feigned motor impairment and conversion disorder. Neuropsychologia 2000, 38, 1251–1260. [Google Scholar] [CrossRef]
- Cojan, Y.; Waber, L.; Carruzzo, A.; Vuilleumier, P. Motor inhibition in hysterical conversion paralysis. Neuroimage 2009, 47, 1026–1037. [Google Scholar] [CrossRef]
- Harris, S.; Kaplan, J.T.; Curiel, A.; Bookheimer, S.Y.; Iacoboni, M.; Cohen, M.S. The neural correlates of religious and nonreligious belief. PLoS One 2009, 4, e0007272. [Google Scholar]
- Kapogiannis, D.; Barbey, A.K.; Su, M.; Zamboni, G.; Krueger, F.; Grafman, J. Cognitive and neural foundations of religious belief. Proc. Natl. Acad. Sci. USA 2009, 106, 4876–4881. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Saj, A.; Raz, N.; Levin, N.; Ben-Hur, T.; Arzy, S. Disturbed Mental Imagery of Affected Body-Parts in Patients with Hysterical Conversion Paraplegia Correlates with Pathological Limbic Activity. Brain Sci. 2014, 4, 396-404. https://doi.org/10.3390/brainsci4020396
Saj A, Raz N, Levin N, Ben-Hur T, Arzy S. Disturbed Mental Imagery of Affected Body-Parts in Patients with Hysterical Conversion Paraplegia Correlates with Pathological Limbic Activity. Brain Sciences. 2014; 4(2):396-404. https://doi.org/10.3390/brainsci4020396
Chicago/Turabian StyleSaj, Arnaud, Noa Raz, Netta Levin, Tamir Ben-Hur, and Shahar Arzy. 2014. "Disturbed Mental Imagery of Affected Body-Parts in Patients with Hysterical Conversion Paraplegia Correlates with Pathological Limbic Activity" Brain Sciences 4, no. 2: 396-404. https://doi.org/10.3390/brainsci4020396