
Corticospinal Excitability in Children with Congenital Hemiparesis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study 1: Primed Low-Frequency Repetitive Transcranial Magnetic Stimulation and Constraint-Induced Movement Therapy in Pediatric Hemiparesis: A Randomized Trial (rTMS Study) (ClinicalTrials.gov # NCT01104064) [18]
2.2. Study 2: Synergistic Effect of Combined Transcranial Direct Current Stimulation/Constraint-Induced Movement Therapy in Children and Young Adults with Hemiparesis (tDCS Study) (ClinicalTrials.gov # NCT02250092) [26]
2.3. Data Management
2.4. Statistical Analysis
3. Results
3.1. Presence of MEP on the Lesioned and Non-Lesioned Hemispheres in Both the rTMS and tDCS Studies
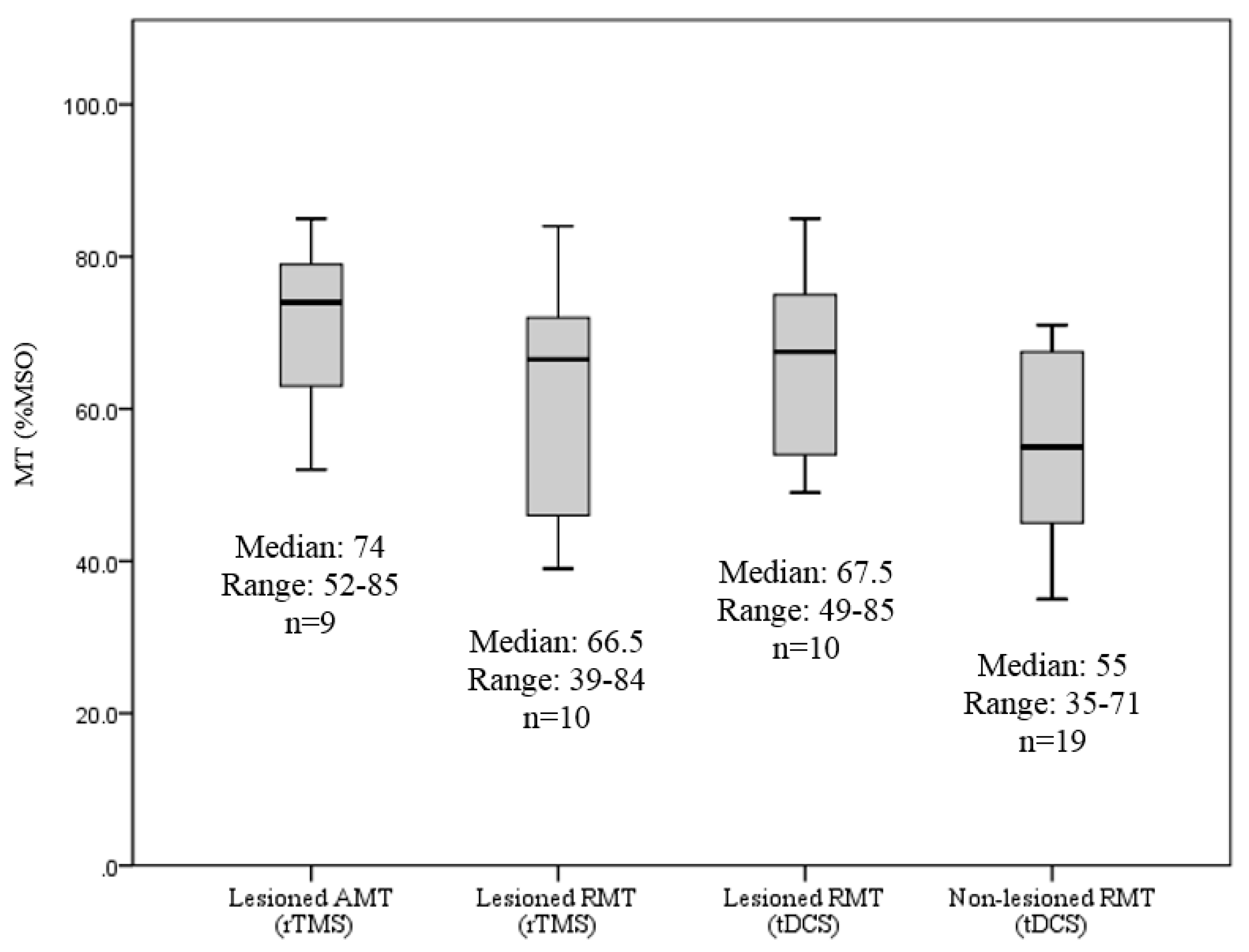
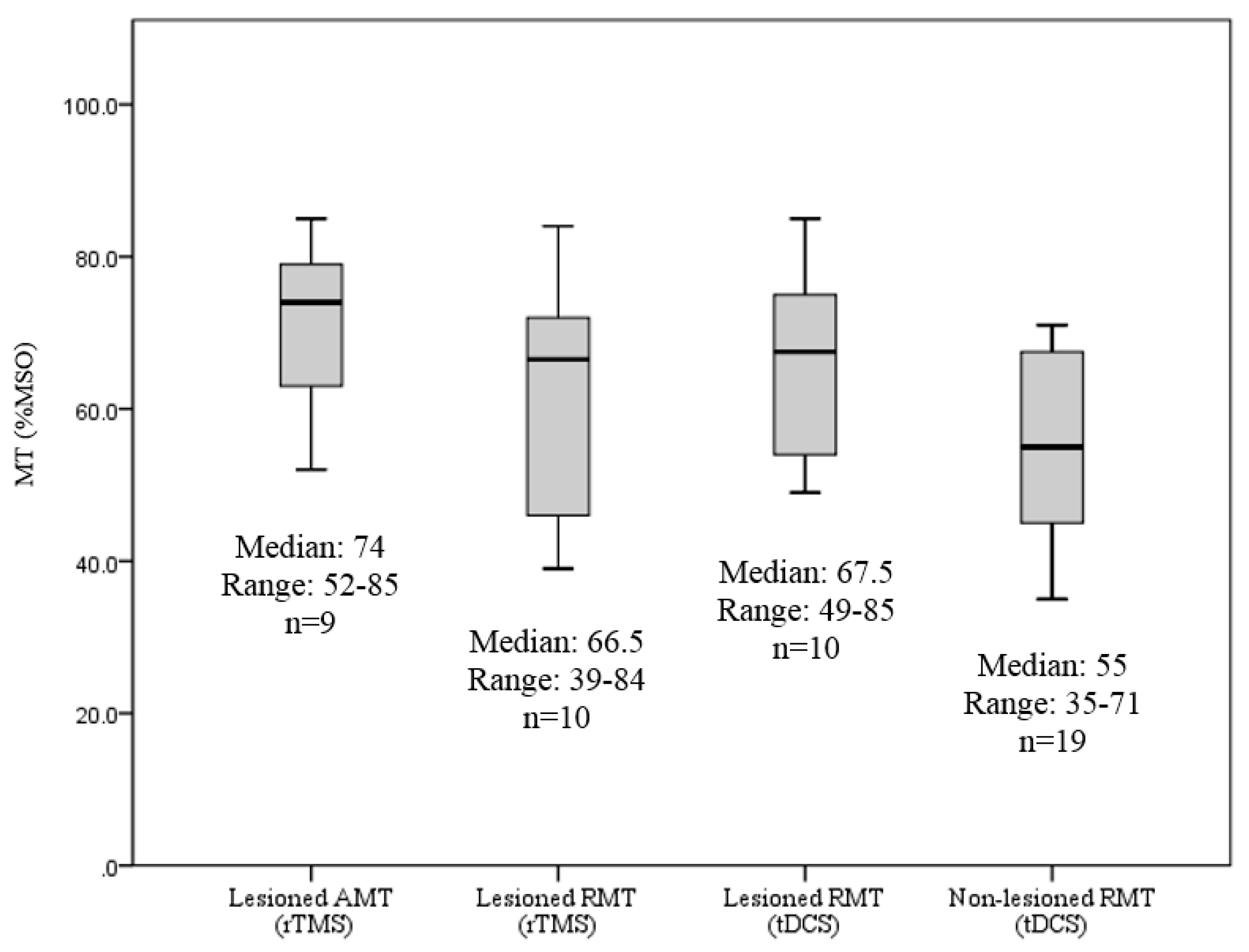
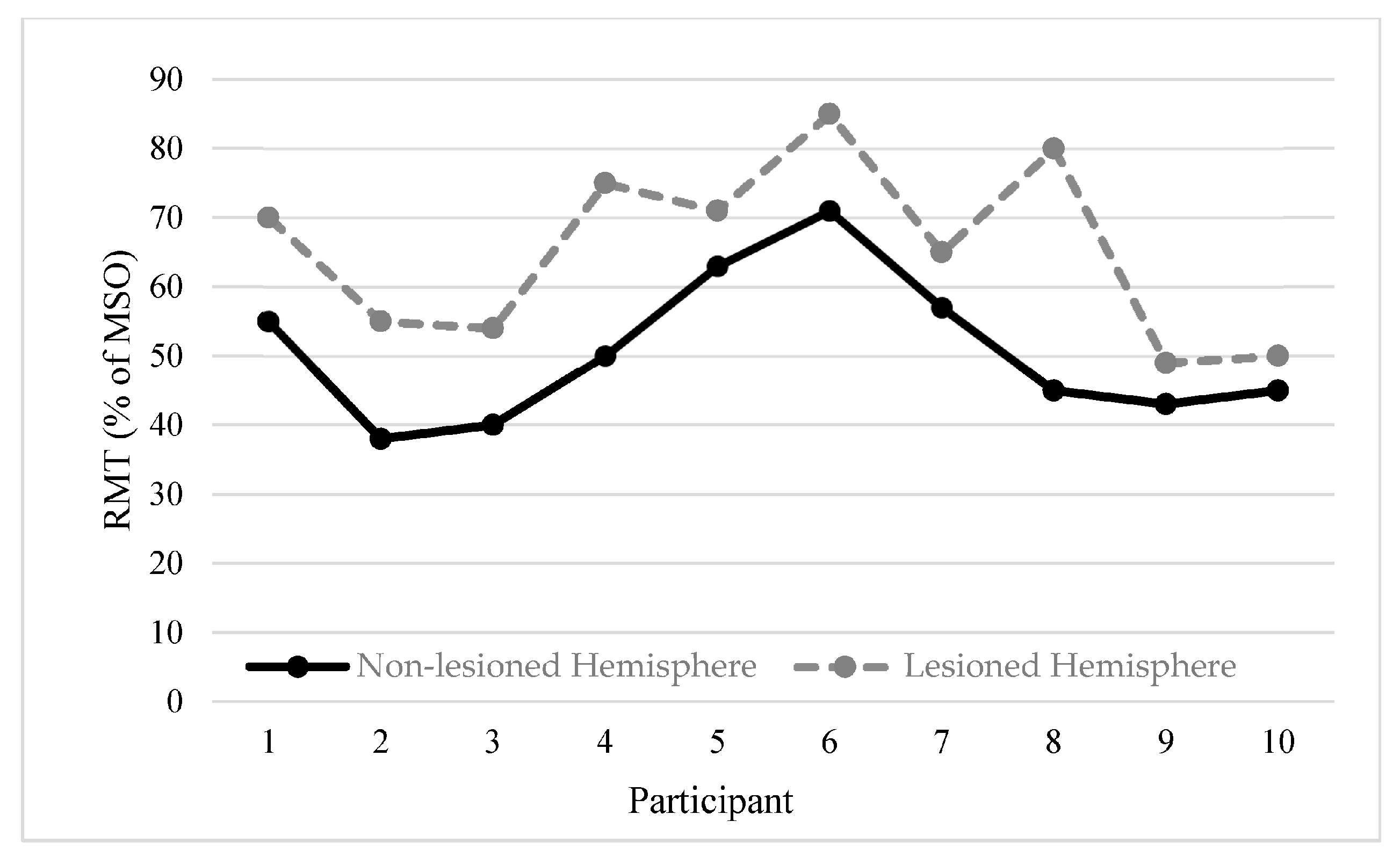
3.2. RMT Values between Lesioned and Non-Lesioned Hemispheres
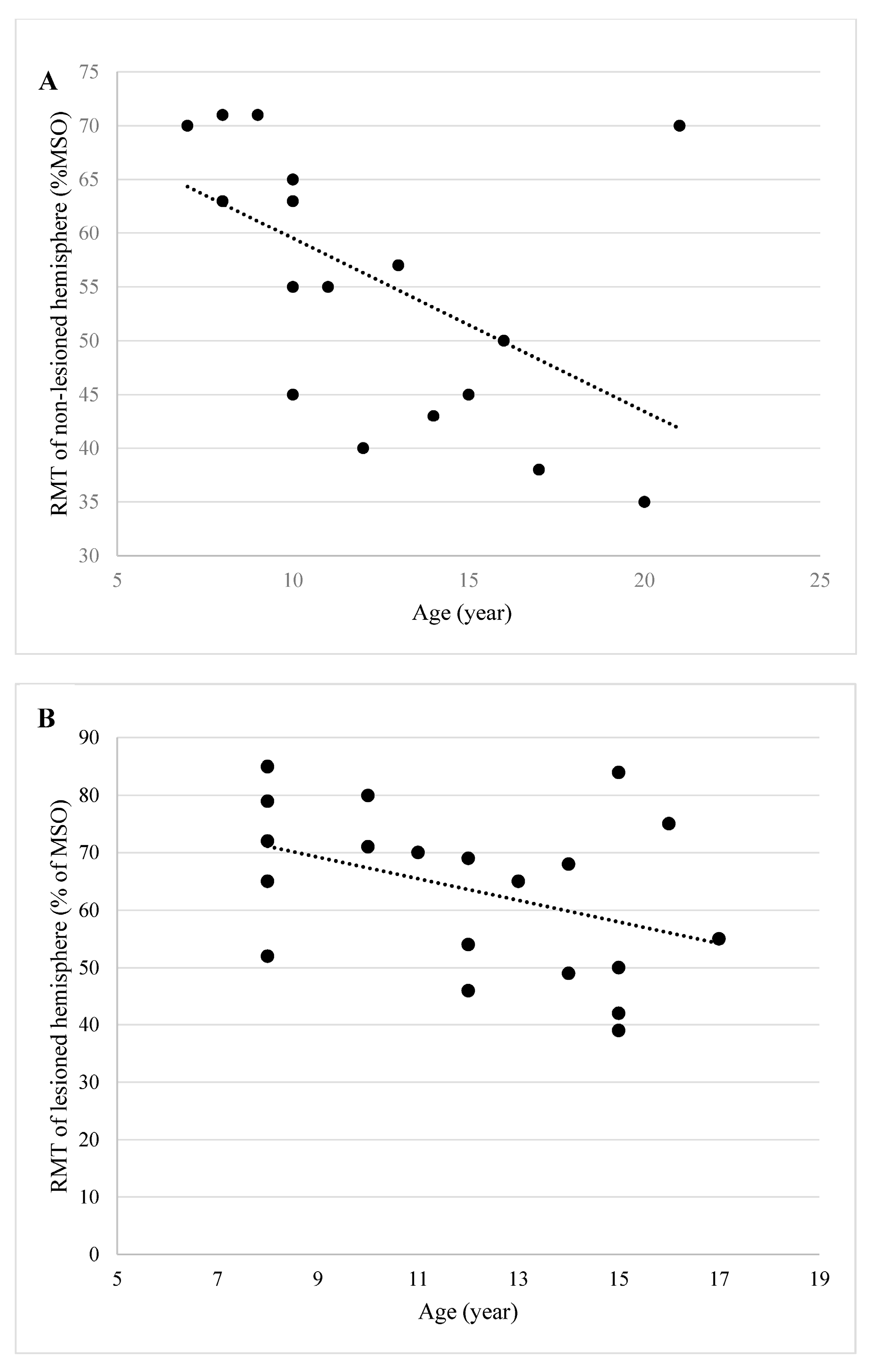
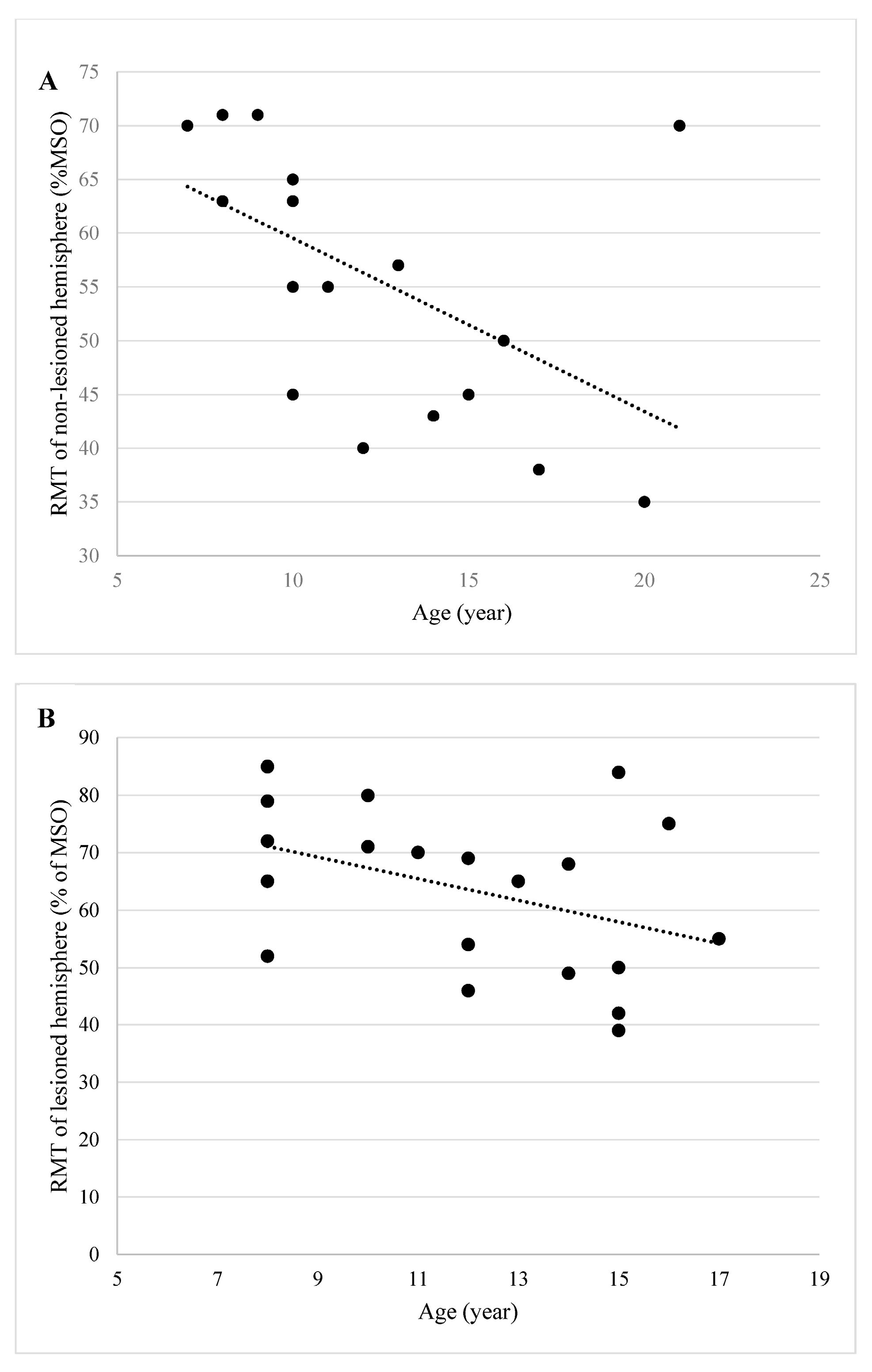
3.3. Influence of Age on RMT
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Raju, T.N.; Nelson, K.B.; Ferriero, D.; Lynch, J.K. Ischemic perinatal stroke: Summary of a workshop sponsored by the National Institute of Child Health and Human Development and the National Institute of Neurological Disorders and Stroke. Pediatrics 2007, 120, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Lehman, L.L.; Rivkin, M.J. Perinatal arterial ischemic stroke: Presentation, risk factors, evaluation, and outcome. Pediatr. Neurol. 2014, 51, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, E.; Byblow, W.D.; Feys, H.; Wenderoth, N. The corticospinal tract: A biomarker to categorize upper limb functional potential in unilateral cerebral palsy. Front. Pediatr. 2015, 3, 112. [Google Scholar] [CrossRef] [PubMed]
- Scheck, S.M.; Fripp, J.; Reid, L.; Pannek, K.; Fiori, S.; Boyd, R.N.; Rose, S.E. Extent of altered white matter in unilateral and bilateral periventricular white matter lesions in children with unilateral cerebral palsy. Res. Dev. Disabil. 2016, 55, 368–376. [Google Scholar] [PubMed]
- Welniarz, Q.; Dusart, I.; Gallea, C.; Roze, E. One hand clapping: Lateralization of motor control. Front. Neuroanat. 2015, 9, 75. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Thompson, A.K.; Chan, K.M.; Wilman, A.; Stein, R.B. Persistent mirror movements for over sixty years: The underlying mechanisms in a cerebral palsy patient. Clin. Neurophysiol. 2008, 119, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Talelli, P.; Greenwood, R.J.; Rothwell, J.C. Arm function after stroke: Neurophysiological correlates and recovery mechanisms assessed by transcranial magnetic stimulation. Clin. Neurophysiol. 2006, 117, 1641–1659. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Tian, L.; Liu, W.; Hu, J.; Xu, G.; Ma, M.; Fan, X.; Ye, R.; Jiang, Y.; Yin, Q.; et al. Effects of repetitive transcranial magnetic stimulation on motor recovery and motor cortex excitability in patients with stroke: A randomized controlled trial. Eur. J. Neurol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.; Summers, J.J.; Cauraugh, J.H. Non-Invasive Brain Stimulation Improves Paretic Limb Force Production: A Systematic Review and Meta-Analysis. Brain Stimul. 2016. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, X.W.; Zuo, Z.T.; Lu, J.; Meng, C.L.; Fang, H.Y.; Xue, R.; Fan, Y.; Guan, Y.Z.; Zhang, W.H. Cerebral Functional Reorganization in Ischemic Stroke after Repetitive Transcranial Magnetic Stimulation: An fMRI Study. CNS Neurosci Ther. 2016. [Google Scholar] [CrossRef] [PubMed]
- Eyre, J.A.; Smith, M.; Dabydeen, L.; Clowry, G.J.; Petacchi, E.; Battini, R.; Guzzetta, A.; Cioni, G. Is hemiplegic cerebral palsy equivalent to amblyopia of the corticospinal system? Ann. Neurol. 2007, 62, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Friel, K.M.; Kuo, H.C.; Fuller, J.; Ferre, C.L.; Brandao, M.; Carmel, J.B.; Bleyenheuft, Y.; Gowatsky, J.L.; Stanford, A.D.; Rowny, S.B.; et al. Skilled Bimanual Training Drives Motor Cortex Plasticity in Children with Unilateral Cerebral Palsy. Neurorehabil. Neural Repair 2016, 30, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Kuhnke, N.; Juenger, H.; Walther, M.; Berweck, S.; Mall, V.; Staudt, M. Do patients with congenital hemiparesis and ipsilateral corticospinal projections respond differently to constraint-induced movement therapy? Dev. Med. Child Neurol. 2008, 50, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C.; Ferre, C.L.; Carmel, J.B.; Gowatsky, J.L.; Stanford, A.D.; Rowny, S.B.; Lisanby, S.H.; Gordon, A.M.; Friel, K.M. Using diffusion tensor imaging to identify corticospinal tract projection patterns in children with unilateral spastic cerebral palsy. Dev. Med. Child Neurol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mackey, A.; Stinear, C.; Stott, S.; Byblow, W.D. Upper limb function and cortical organization in youth with unilateral cerebral palsy. Front. Neurol. 2014, 5, 117. [Google Scholar] [CrossRef] [PubMed]
- Staudt, M.; Ticini, L.F.; Grodd, W.; Krageloh-Mann, I.; Karnath, H.O. Functional topography of early periventricular brain lesions in relation to cytoarchitectonic probabilistic maps. Brain Lang. 2008, 106, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.M.; Carey, J.R.; Lu, C.; Krach, L.E.; Feyma, T.; Durfee, W.K.; Gillick, B.T. Ipsilesional motor-evoked potential absence in pediatric hemiparesis impacts tracking accuracy of the less affected hand. Res. Dev. Disabil. 2015, 47, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Gillick, B.T.; Krach, L.E.; Feyma, T.; Rich, T.L.; Moberg, K.; Thomas, W.; Cassidy, J.M.; Menk, J.; Carey, J.R. Primed low-frequency repetitive transcranial magnetic stimulation and constraint-induced movement therapy in pediatric hemiparesis: A randomized controlled trial. Dev. Med. Child Neurol. 2014, 56, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Grecco, L.A.; de Almeida Carvalho Duarte, N.; Mendonca, M.E.; Cimolin, V.; Galli, M.; Fregni, F.; Santos Oliveira, C. Transcranial direct current stimulation during treadmill training in children with cerebral palsy: A randomized controlled double-blind clinical trial. Res. Dev. Disabil. 2014, 35, 2840–2848. [Google Scholar] [CrossRef] [PubMed]
- Kirton, A.; Andersen, J.; Herrero, M.; Nettel-Aguirre, A.; Carsolio, L.; Damji, O.; Keess, J.; Mineyko, A.; Hodge, J.; Hill, M.D. Brain stimulation and constraint for perinatal stroke hemiparesis: The PLASTIC CHAMPS Trial. Neurology 2016, 86, 1659–1667. [Google Scholar] [CrossRef] [PubMed]
- Kirton, A.; Chen, R.; Friefeld, S.; Gunraj, C.; Pontigon, A.M.; Deveber, G. Contralesional repetitive transcranial magnetic stimulation for chronic hemiparesis in subcortical paediatric stroke: A randomised trial. Lancet Neurol. 2008, 7, 507–513. [Google Scholar] [CrossRef]
- Valle, A.C.; Dionisio, K.; Pitskel, N.B.; Pascual-Leone, A.; Orsati, F.; Ferreira, M.J.; Boggio, P.S.; Lima, M.C.; Rigonatti, S.P.; Fregni, F. Low and high frequency repetitive transcranial magnetic stimulation for the treatment of spasticity. Dev. Med. Child Neurol. 2007, 49, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Bhanpuri, N.H.; Bertucco, M.; Young, S.J.; Lee, A.A.; Sanger, T.D. Multiday Transcranial Direct Current Stimulation Causes Clinically Insignificant Changes in Childhood Dystonia: A Pilot Study. J. Child Neurol. 2015, 30, 1604–1615. [Google Scholar] [CrossRef] [PubMed]
- Young, S.J.; Bertucco, M.; Sanger, T.D. Cathodal transcranial direct current stimulation in children with dystonia: A sham-controlled study. J. Child Neurol. 2014, 29, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.S.; Jang, S.H.; Son, S.M. The different maturation of the corticospinal tract and corticoreticular pathway in normal brain development: Diffusion tensor imaging study. Front. Hum. Neurosci. 2014, 8, 573. [Google Scholar] [CrossRef] [PubMed]
- Gillick, B.; Menk, J.; Mueller, B.; Meekins, G.; Krach, L.E.; Feyma, T.; Rudser, K. Synergistic effect of combined transcranial direct current stimulation/constraint-induced movement therapy in children and young adults with hemiparesis: Study protocol. BMC Pediatr. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Kirton, A.; Deveber, G.; Gunraj, C.; Chen, R. Cortical excitability and interhemispheric inhibition after subcortical pediatric stroke: Plastic organization and effects of rTMS. Clin. Neurophysiol. 2010, 121, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.P.; Nakonezny, P.A.; Ameis, S.H.; Vande Voort, J.L.; Husain, M.M.; Emslie, G.J.; Daskalakis, Z.J.; Croarkin, P.E. Cortical inhibitory and excitatory correlates of depression severity in children and adolescents. J. Affect Disord. 2016, 190, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Garvey, M.A.; Mall, V. Transcranial magnetic stimulation in children. Clin. Neurophysiol. 2008, 119, 973–984. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, A.; Radhu, N.; Farzan, F.; Mulsant, B.H.; Rajji, T.K.; Daskalakis, Z.J.; Blumberger, D.M. A meta-analysis of the effects of aging on motor cortex neurophysiology assessed by transcranial magnetic stimulation. Clin. Neurophysiol. 2016, 127, 2834–2845. [Google Scholar] [CrossRef] [PubMed]
- Eyre, J.A.; Taylor, J.P.; Villagra, F.; Smith, M.; Miller, S. Evidence of activity-dependent withdrawal of corticospinal projections during human development. Neurology 2001, 57, 1543–1554. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| - | rTMS (n = 30) | tDCS (n = 20) |
|---|---|---|
| Sex (Male:Female) | 18:12 | 9:11 |
| Age (Mean (range)) | 10.4 (7–16) | 12.2 (7–21) |
| Lesioned Hemisphere (Right:Left) | 10:20 | 5:15 |
| MACS levels | I, II and III a | I, II, III and IV |
| Hemispheres | rTMS (n = 30) | tDCS (n = 20) | ||
|---|---|---|---|---|
| Lesioned | Non-lesioned | Lesioned | Non-Lesioned | |
| N of MEP presence (%) | 19 (63.3%) | NA | 12 (60.0%) | 20 (100.0%) |
| N of RMT presence (%) | 10 (33.3%) | NA | 10 (50.0%) | 19 (95.0%) * |
| N of AMT presence (%) | 9 (30.0%) | NA | 2 (10.0%) | 1 (5.0%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-Y.; Rich, T.L.; Cassidy, J.M.; Gillick, B.T. Corticospinal Excitability in Children with Congenital Hemiparesis. Brain Sci. 2016, 6, 49. https://doi.org/10.3390/brainsci6040049
Chen C-Y, Rich TL, Cassidy JM, Gillick BT. Corticospinal Excitability in Children with Congenital Hemiparesis. Brain Sciences. 2016; 6(4):49. https://doi.org/10.3390/brainsci6040049
Chicago/Turabian StyleChen, Chao-Ying, Tonya L. Rich, Jessica M. Cassidy, and Bernadette T. Gillick. 2016. "Corticospinal Excitability in Children with Congenital Hemiparesis" Brain Sciences 6, no. 4: 49. https://doi.org/10.3390/brainsci6040049