An Overview of Recent Findings on Social Anxiety Disorder in Adolescents and Young Adults at Clinical High Risk for Psychosis


Abstract
:1. Introduction
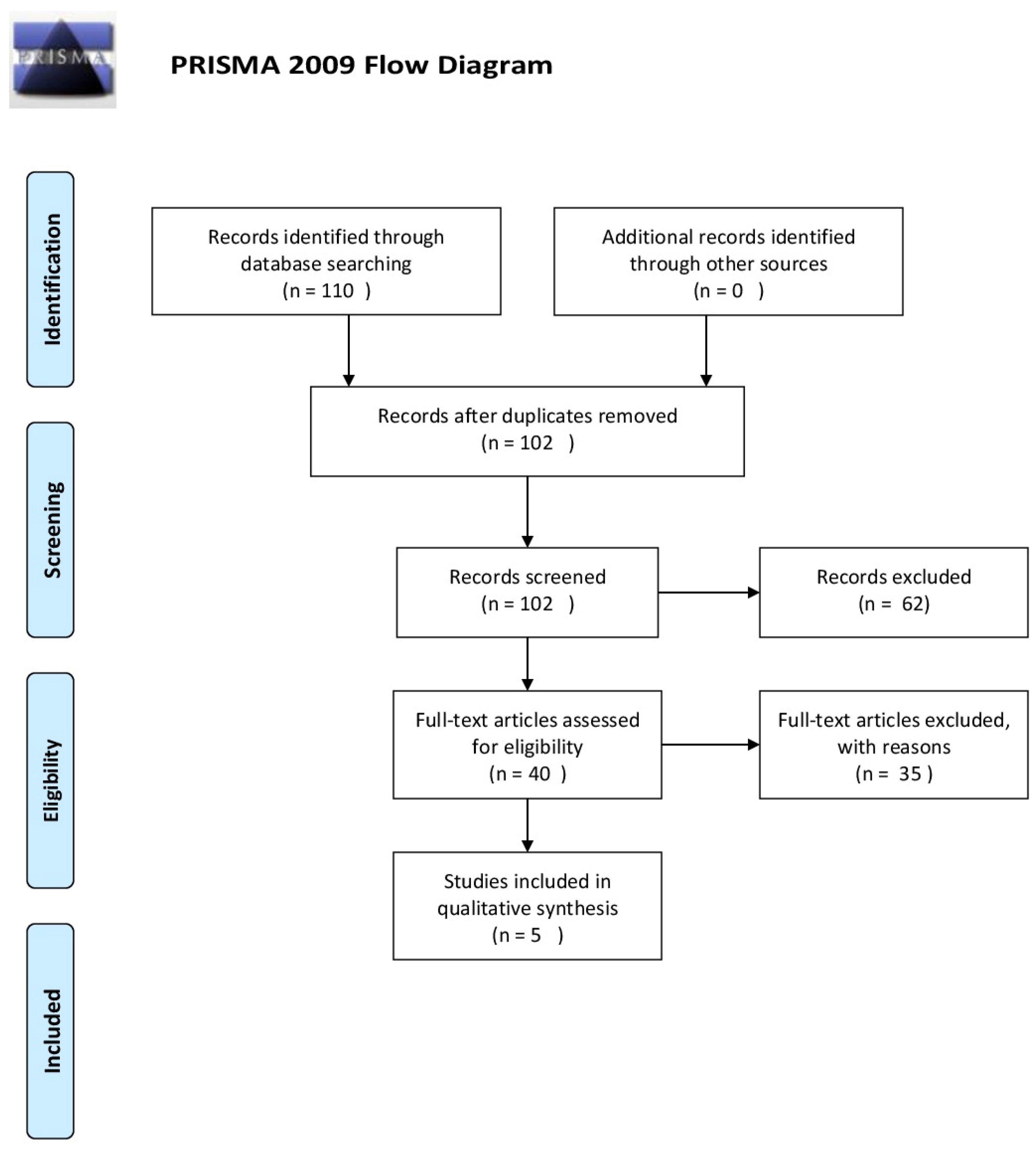
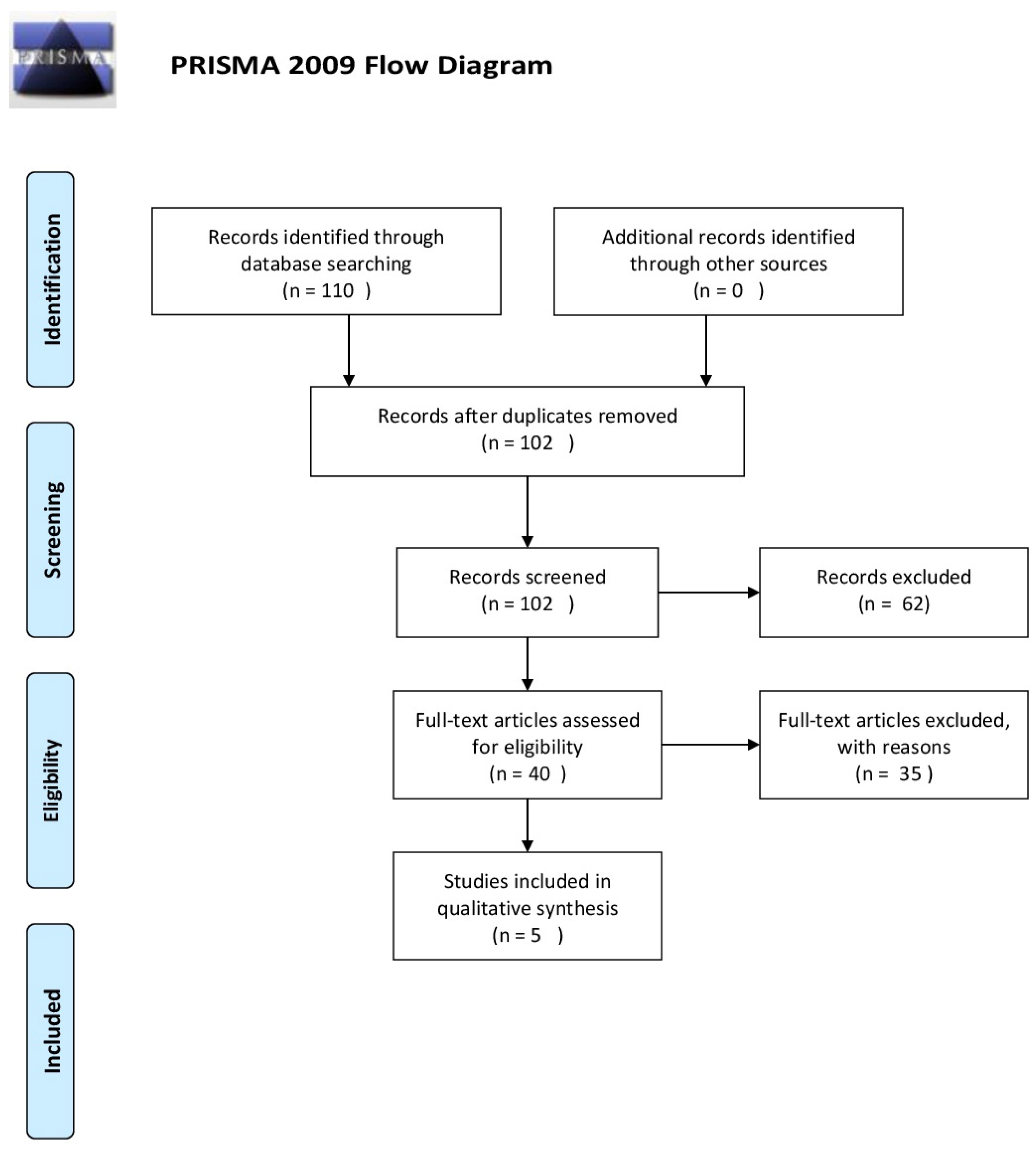
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Selection Procedure, Data Extraction and Data Management
3. Data Synthesis
4. Results
5. Discussion
6. Implications for Practice and Research
7. Limitations
8. Conclusions
Author Contributions
Conflicts of Interest
References
- Serafini, G.; Pompili, M.; Innamorati, M.; Rihmer, Z.; Sher, L.; Girardi, P. Can cannabis increase the suicide risk in psychosis? A critical review. Curr. Pharm. Des. 2012, 18, 5165–5187. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.W.; Addington, J.; Cadenhead, K.S.; Cannon, T.D.; Cornblatt, B.A.; Heinssen, R.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; Walker, E.F.; et al. Validity of the prodromal risk syndrome for first psychosis: Findings from the North American Prodrome Longitudinal Study. Schizophr. Bull. 2009, 35, 894–908. [Google Scholar] [CrossRef] [PubMed]
- Addington, J.; Cornblatt, B.A.; Cadenhead, K.S.; Cannon, T.D.; McGlashan, T.H.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; Walker, E.F.; Woods, S.W.; et al. At clinical high risk for psychosis: Outcome for nonconverters. Am. J. Psychiatry 2011, 168, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Nelson, B.; Valmaggia, L.; Yung, A.R.; McGuire, P.K. Comorbid depressive and anxiety disorders in 509 individuals with an at-risk mental state: Impact on psychopathology and transition to psychosis. Schizophr. Bull. 2014, 40, 120–131. [Google Scholar] [CrossRef] [PubMed]
- McAusland, L.; Buchy, L.; Cadenhead, K.S.; Cannon, T.D.; Cornblatt, B.A.; Heinssen, R.; McGlashan, T.H.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; et al. Anxiety in Youth at Clinical High Risk for Psychosis. Early Interv. Psychiatry 2017. [Google Scholar] [CrossRef] [PubMed]
- Rietdijk, J.; Ising, H.K.; Dragt, S.; Klaassen, R.; Nieman, D.; Wunderink, L.; Cuijpers, P.; Linszen, D.; van der Gaag, M. Depression and social anxiety in help-seeking patients with an ultra- high risk for developing psychosis. Psychiatry Res. 2013, 209, 309–313. [Google Scholar] [CrossRef] [PubMed]
- McGlashan, T.H. Structured Interview for Prodromal Syndromes (SIPS); Yale University: New Haven, CT, USA, 2001. [Google Scholar]
- Yung, A.R.; Yuen, H.P.; McGorry, P.D.; Phillips, L.J.; Kelly, D.; Dell’Olio, M.; Francey, S.M.; Cosgrave, E.M.; Killackey, E.; Stanford, C.; et al. Mapping the onset of psychosis: The Comprehensive assessment of At Risk Mental States (CAARMS). Aust. N. Z. J. Psychiatry 2005, 39, 964–971. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10. Classification of Mental and Behavioural Disorders; WHO: Geneva, Switzerland, 1993. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Arlington, VA, USA, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Wigman, J.T.W.; van Nierop, M.; Vollebergh, W.A.M.; Lieb, R.; Beesdo-Baum, K.; Wittchen, H.; van Os, J. Evidence That Psychotic Symptoms Are Prevalent in Disorders of Anxiety and Depression, Impacting on Illness Onset, Risk, and Severity—Implications for Diagnosis and Ultra–High Risk Research. Schizophr. Bull. 2012, 38, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Madsen, H.K.; Nordholm, D.; Krakauer, K.; Randers, L.; Nordentoft, M. Psychopathology and social functioning of 42 subjects from a Danish ultra high-risk cohort. Early Interv. Psychiatry 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chudleigh, C.; Naismith, S.L.; Blaszczynski, A.; Hermens, D.F.; Redoblado Hodge, M.A.; Hickie, I.B. How does social functioning in the early stages of psychosis relate to depression and social anxiety? Early Interv. Psychiatry 2011, 5, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Mattick, R.P.; Clarke, J.C. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav. Res. Ther. 1998, 36, 455–470. [Google Scholar] [CrossRef]
- Zung, W.W. A rating instrument for anxiety disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Wittchen, H.; Pfister, H. DIA-X-Interviews: Manual fur Screening-Verfahren und Interview; Interviewheft, Langsschnittuntersuchung (DIA-X-Lifetime); Enganzungsheft (DIA-X-Lifetime); Interviewheft Querschnittsuntersuchung (DIA-X-Monatsversion); Erganzungsheft (DIA-X-12 Montasversion); PC-Programm zur Durchfuhrung der Interviews (Langsund Querschnittsuntersuchung); Ausertungsprogramm; Swets&Zeiltinger: Frankfurt, Germany, 1997. [Google Scholar]
- Morosini, P.L.; Magliano, L.; Brambilla, L.; Ugolini, S.; Pioli, R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr. Scand. 2000, 101, 323–329. [Google Scholar] [PubMed]
- Niendam, T.A.; Bearden, C.E.; Johnson, J.K.; Cannon, T.D. Global Functioning: Role Scale (GF: Role); University of California: Los Angeles, CA, USA, 2006. [Google Scholar]
- Auther, A.M.; Smith, C.W.; Cornblatt, B.A. Global Functioning: Social Scale (GF: Social); Zucker-Hillside Hospital: Glen Oaks, NY, USA, 2006. [Google Scholar]
- Davidson, J.R.; Potts, N.L.; Richichi, E.A.; Ford, S.M.; Krishnan, K.R.; Smith, R.D.; Wilson, W. The Brief Social Phobia Scale. J. Clin. Psychiatry 1991, 52, 48–51. [Google Scholar] [PubMed]
- Michail, M.; Birchwood, M. Social anxiety disorder in first-episode psychosis: Incidence, phenomenology and relationship with paranoia. Br. J. Psychiatry 2009, 195, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Rekhi, G.; Rapisarda, A.; Lam, M.; Kraus, M.; Keefe, R.S.; Lee, J. Impact of psychiatric comorbidity in individuals at Ultra High Risk of psychosis—Findings from the Longitudinal Youth at Risk Study (LYRIKS). Schizophr. Res. 2015, 164, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Schlosser, D.A.; Jacobson, S.; Chen, Q.; Sugar, C.A.; Niendam, T.A.; Li, G.; Bearden, C.E.; Cannon, T.D. Recovery from an at-risk state: Clinical and functional outcomes of putatively prodromal youth who do not develop psychosis. Schizophr. Bull. 2012, 38, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E.; Paino, M.; Lemos-Giráldez, S.; Muñiz, J. Schizotypal traits and depressive symptoms in nonclinical adolescents. Compr. Psychiatry 2011, 52, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Goritz, A.S.; McLean, B.; Westermann, S.; Brodbeck, J. Do depressive symptoms predict paranoia or vice versa? J. Behav. Ther. Exp. Psychiatry 2017, 56, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Yung, A.R.; Phillips, L.J.; Yuen, H.P.; Francey, S.M.; McFarlane, C.A.; Hallgren, M.; McGorry, P.D. Psychosis prediction: 12-month follow up of a high-risk (“prodromal”) group. Schizophr. Res. 2003, 60, 21–32. [Google Scholar] [CrossRef]
- Russo, D.A.; Stochl, J.; Painter, M.; Jones, P.B.; Perez, J. Substance use in people at clinical high-risk for psychosis. BMC Psychiatry 2014, 14. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Sample | Methods | Criteria for Diagnosis | Measure | Results |
|---|---|---|---|---|---|
| Mc Ausland et al. (2017) [5] | n = 765 CHR | Multicentric experimental study | Clinical High Risk | SIPS-SOPS | Attenuated Psychotic Symptom scores were correlated with higher SIAS (rS = 0.12, p < 0.01) and SAS scores (rS = 0.18, p < 0.001) |
| 280 Controls | |||||
| Range age: 12–35 | SAS | ||||
| Severe negative symptoms were associated with higher SIAS (rS = 0.33, p < 0.001) and SAS score (rS = 0.18, p < 0.001) | |||||
| IQ > 70 | SIAS | ||||
| Rietdijk et al. (2011) [6] | n = 201 | Experimental | Clinical High Risk | PQ | Social Anxiety (SIAS > 36):42% CHR |
| CAARMS | |||||
| Mean age: 22.7 | BDI-II | Gender and Social Anxiety: | |||
| Personal Assessment and Crisis Evaluation (PACE) criteria | 35.4% male vs. 49% female (p = 0.05) | ||||
| SD = 5.52 | |||||
| CDS | In female patients anxiety predicted Positive Symptom Score (p = 0.038) | ||||
| SIAS | |||||
| Demographic questionnaire | |||||
| Wigman et al. (2012) [12] | n = 3021 (T0) | Longitudinal study | Disorders of Anxiety/Depression | (DIA-X/M-CIDI) | 27% of individuals with disorders of anxiety/depression reported psychotic symptoms at any time point (36% at T2; 19% at T3) vs. 14% in those without (p < 0.001). |
| SCL-90R | |||||
| M-CIDI: | |||||
| n = 2548 (T2) | -Caseness: | ||||
| -Help seeking Behaviour; | |||||
| n = 2210 (T3) | -Substance Use; | ||||
| -Trauma; | |||||
| Range age: 14–24 | -Recent Life Events; | ||||
| -Urbanicity | |||||
| -Familial History of Help Seeking | |||||
| Madsen et al. (2017) [13] | n = 42 | Experimental study | Children High Risk | CAARMS SCID-I | Social and Occupational Functioning Assessment Scale (SOFAS): Mean 43.1 (SD6.4), (p = 0.87). |
| Range age: 18–40 | SCID-II | ||||
| Mean age = 23.8 | SOFAS | GF: Role: Mean 4.6 (SD 1.12), (p = 0.97). | |||
| SD = 4.7 | YMRS | ||||
| YMRS BPRS | GF: Social: Mean 43.1 (SD 5.8), (p = 0.045). | ||||
| SANS | |||||
| MADRS | |||||
| ASSIST | CHR presented major depressive disorders (79%), anxiety (74%), alcohol (31%) and cannabis (24%). | ||||
| GF: Role | |||||
| GF: Social | |||||
| Chudleigh et al. (2011) [14] | 20 FEP | Experimental study | CHR | CAARMS | FEP and CHR participants significantly different from control on quantitative (p = 0.000) and qualitative (p < 0.001) social functioning (SFS). |
| 20 CHR | BPRS | ||||
| 20 controls | |||||
| SFS | |||||
| FEP | SOFAS | Only in the FEP group (p < 0.01), social anxiety symptoms were associated with both qualitative and quantitative social functioning outcomes | |||
| Range Age: 16–30 | WHODAS | ||||
| DASS |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pontillo, M.; Guerrera, S.; Santonastaso, O.; Tata, M.C.; Averna, R.; Vicari, S.; Armando, M. An Overview of Recent Findings on Social Anxiety Disorder in Adolescents and Young Adults at Clinical High Risk for Psychosis. Brain Sci. 2017, 7, 127. https://doi.org/10.3390/brainsci7100127
Pontillo M, Guerrera S, Santonastaso O, Tata MC, Averna R, Vicari S, Armando M. An Overview of Recent Findings on Social Anxiety Disorder in Adolescents and Young Adults at Clinical High Risk for Psychosis. Brain Sciences. 2017; 7(10):127. https://doi.org/10.3390/brainsci7100127
Chicago/Turabian StylePontillo, Maria, Silvia Guerrera, Ornella Santonastaso, Maria Cristina Tata, Roberto Averna, Stefano Vicari, and Marco Armando. 2017. "An Overview of Recent Findings on Social Anxiety Disorder in Adolescents and Young Adults at Clinical High Risk for Psychosis" Brain Sciences 7, no. 10: 127. https://doi.org/10.3390/brainsci7100127