Structural and Neuronal Integrity Measures of Fatigue Severity in Multiple Sclerosis

Abstract
:1. Introduction
2. Methods
2.1. Participant Recruitment and Selection Criteria
2.2. MRI Image Acquisition
2.3. MRI Data Processing and Analysis
2.4. Statistical Methods
3. Results
3.1. Demographics and Clinical Data
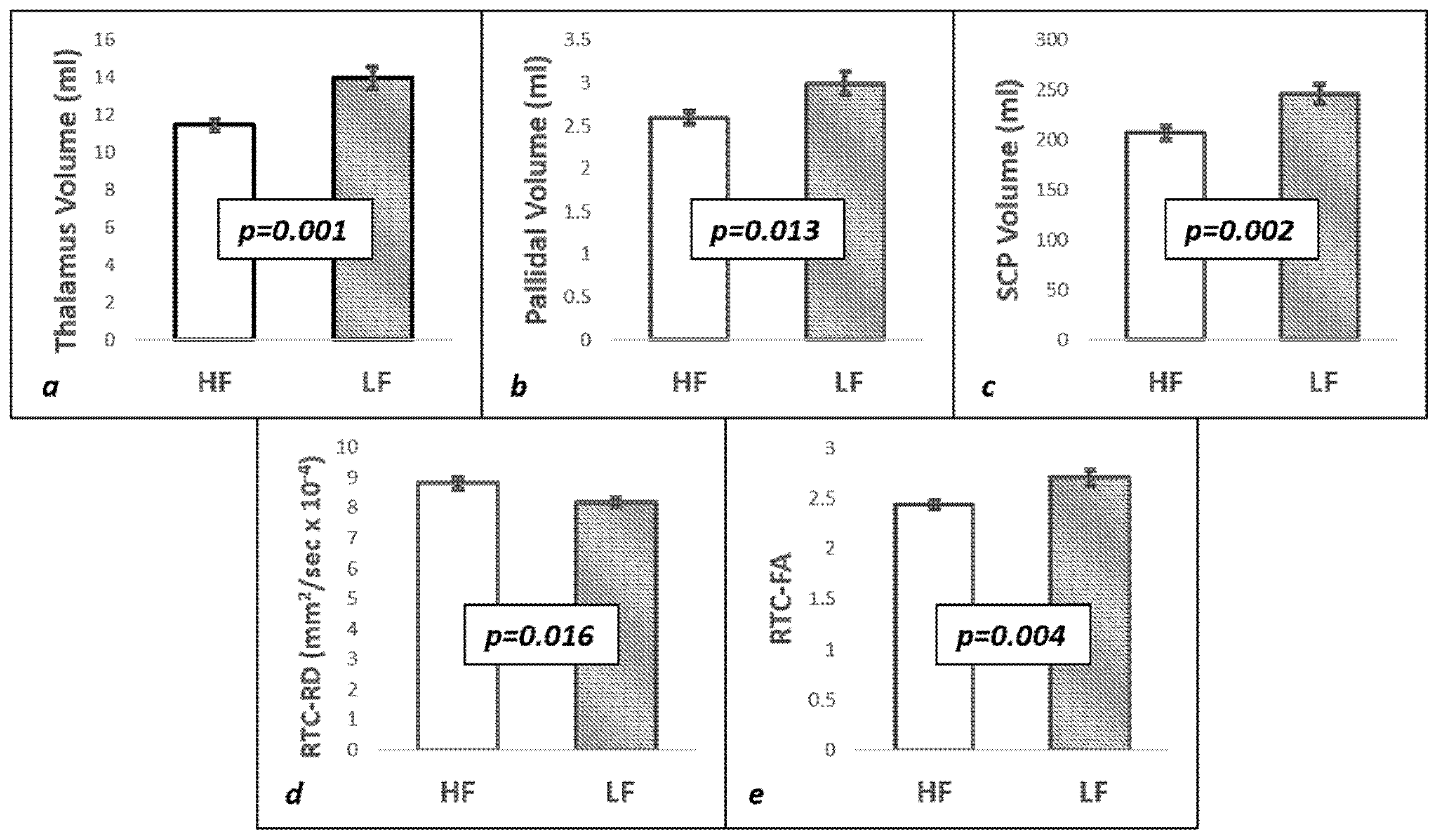
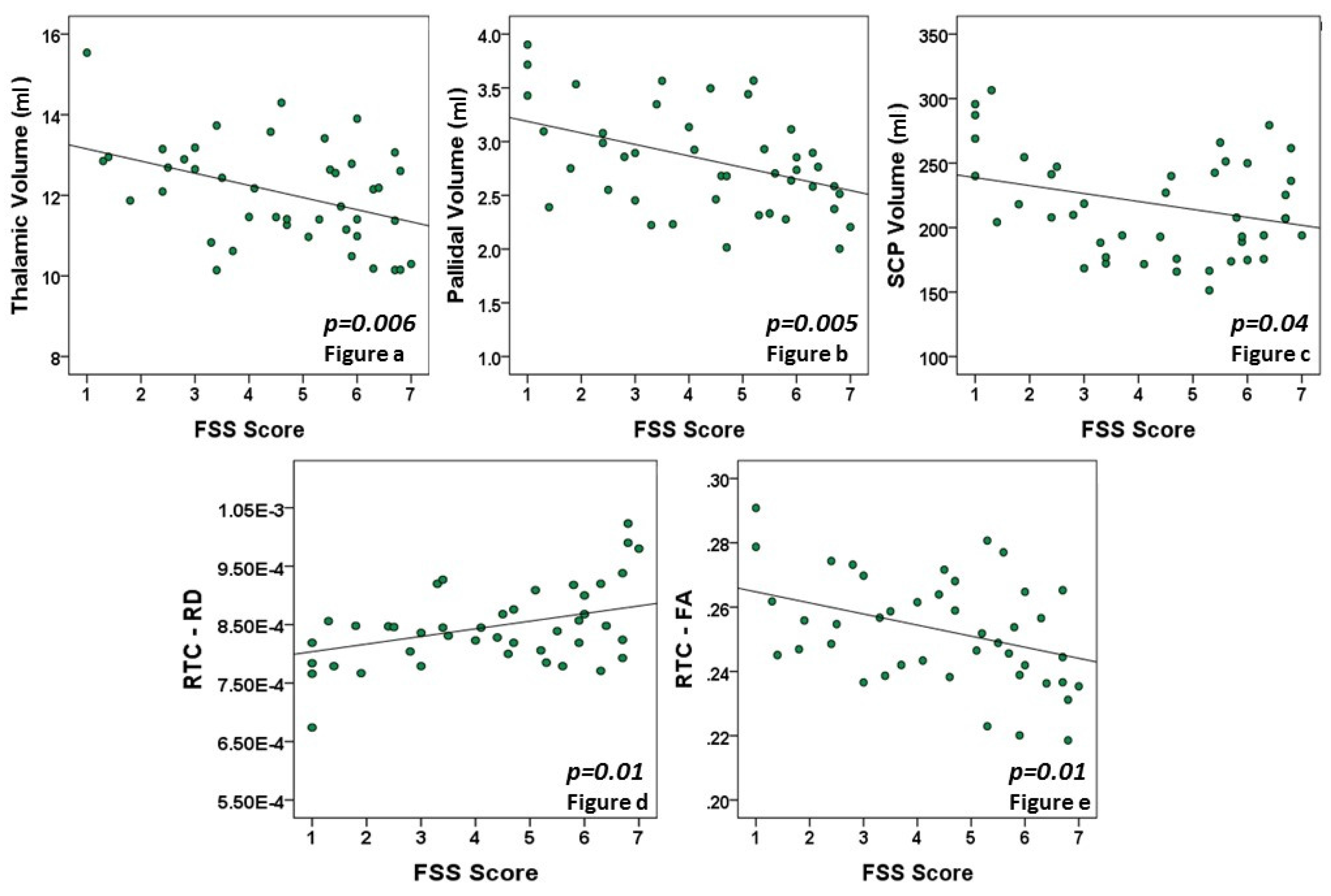
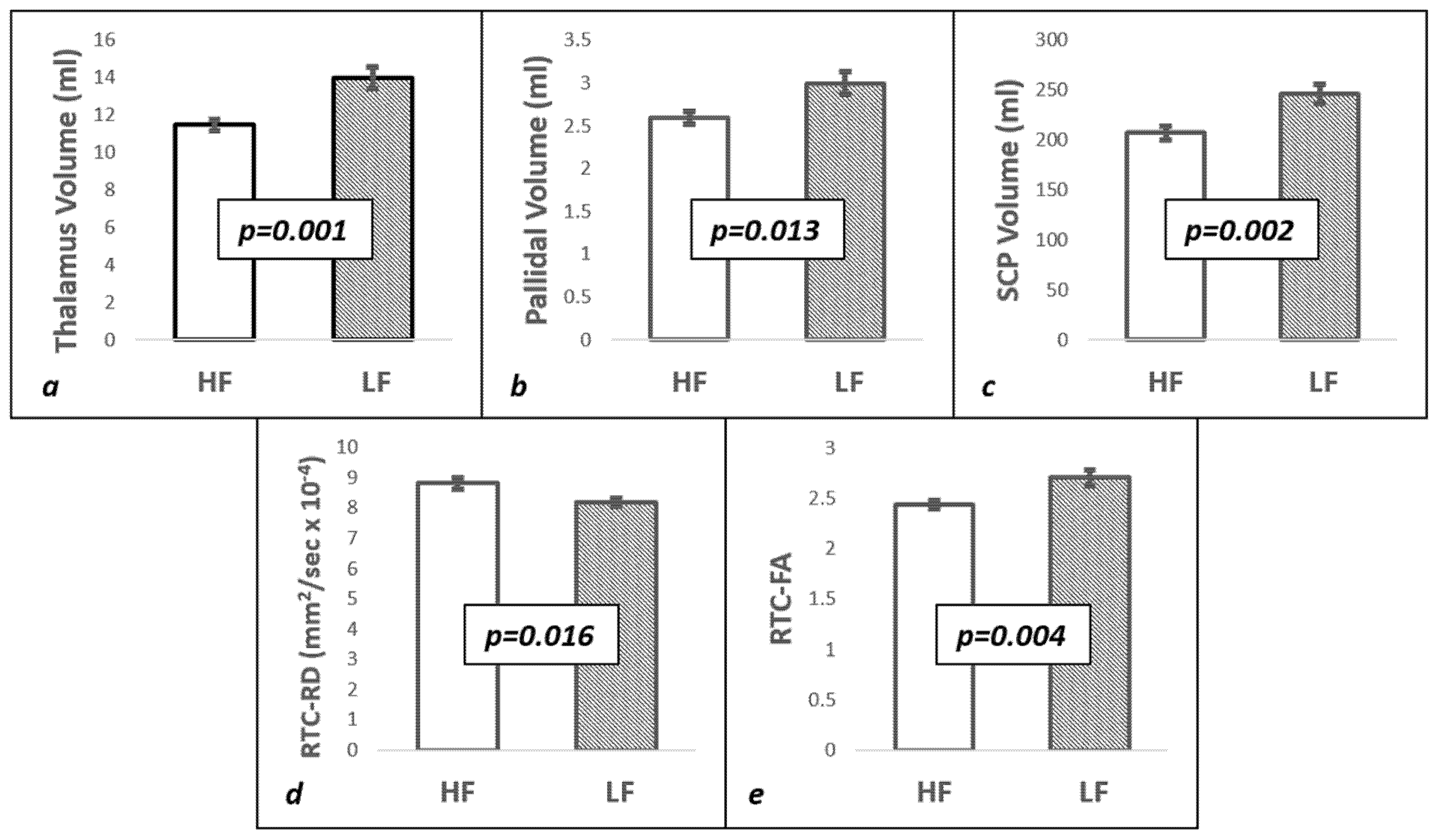
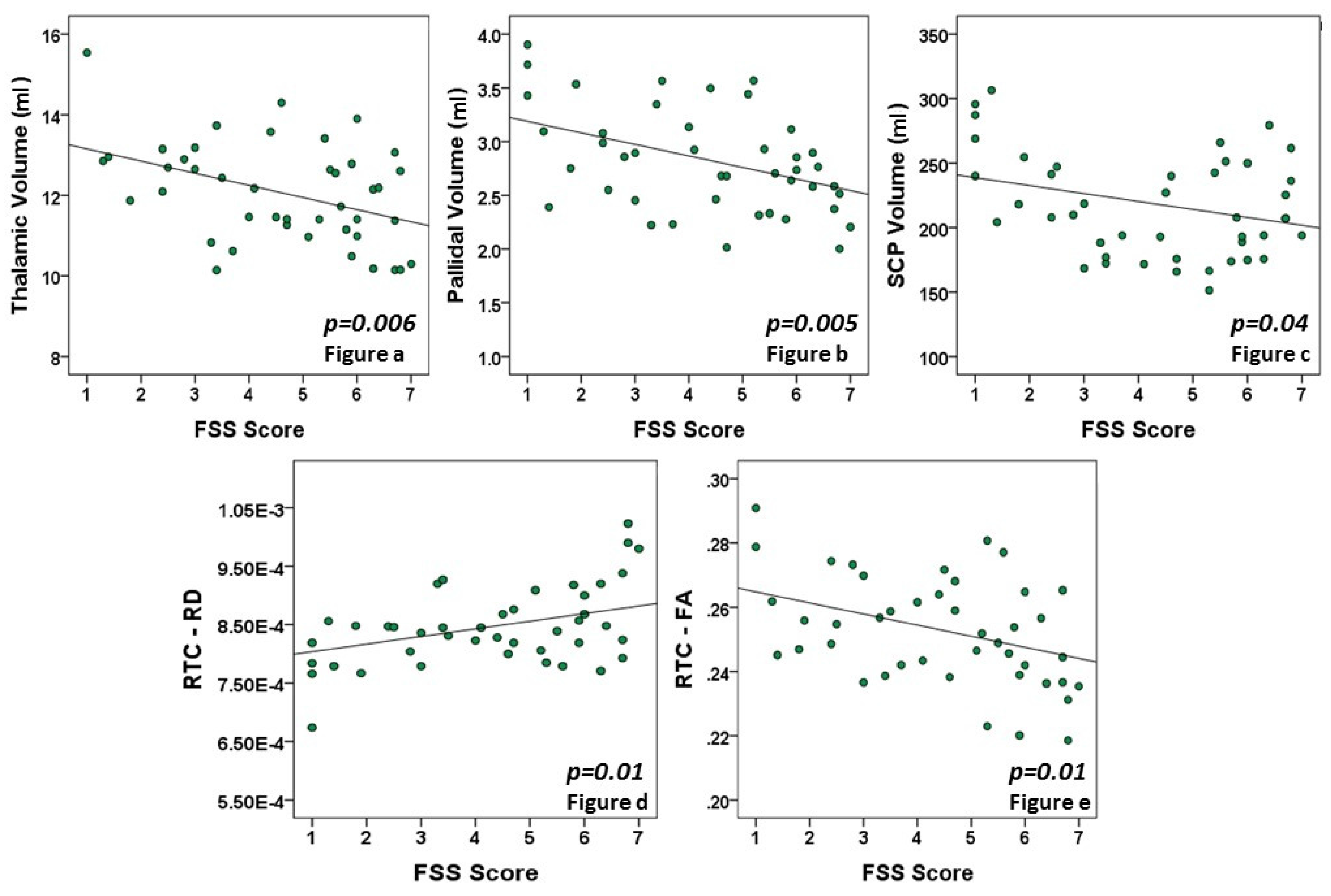
3.2. Structural Imaging Findings
3.3. Diffuse Tensor Imaging Findings
3.4. Multivariate Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Noseworthy, J.H.; Lucchinetti, C.; Rodriguez, M.; Weinshenker, B.G. Multiple sclerosis. N. Eng. J. Med. 2000, 343, 938–952. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, R. Fatigue associated with multiple sclerosis: Diagnosis, impact and management. Mult. Scler. J. 2003, 9, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Goodin, D.S.; Frohman, E.M.; Garmany, G.P., Jr.; Halper, J.; Likosky, W.H.; Lublin, F.D.; Donald, M.; Silberberg, H.; William, M.; Stuart, H.; et al. Disease modifying therapies in multiple sclerosis: Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology 2002, 58, 169–278. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Behan, P.O. Fatigue in neurological disorders. Lancet. 2004, 363, 978–988. [Google Scholar] [CrossRef]
- Mills, R.J.; Young, C.A. A medical definition of fatigue in multiple sclerosis. QJM Int. J. Med. 2008, 101, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Pardini, M.; Bonzano, L.; Mancardi, G.L.; Roccatagliata, L. Frontal networks play a role in fatigue perception in multiple sclerosis. Behav. Neurosci. 2010, 124, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Flachenecker, P.; Kumpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. J. 2002, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Tellez, N.; Rio, J.; Tintore, M.; Nos, C.; Galan, I.; Montalban, X. Does the Modified Fatigue Impact Scale offer a more comprehensive assessment of fatigue in MS? Mult. Scler. J. 2005, 11, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Van der Werf, S.P.; Jonge, J.; Lycklama a Nijeholt, G.J.; Barkhof, F.; Hommes, O.R.; Bleijenberg, G. Fatigue in multiple sclerosis: Interrelations between fatigue complaints, cerebral MRI abnormalities and neurological disability. J. Neurol. Sci. 1998, 160, 164–170. [Google Scholar] [CrossRef]
- Calabrese, M.; Rinaldi, F.; Grossi, P.; Mattisi, I.; Bernardi, V.; Favaretto, A. Basal ganglia and frontal/parietal cortical atrophy is associated with fatigue in relapsing-remitting multiple sclerosis. Mult. Scler. J. 2010, 16, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, C.; Gallo, A.; Li, X.; Ikonomidou, V.N.; Evangelou, I.E.; Ohayon, J.M.; Stern, S.K.; Ehrmantraunt, M.; Cantor, F.; McFarland, H.F.; et al. Relationship of cortical atrophy to fatigue in patients with multiple sclerosis. Arch. Neurol. 2010, 67, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Sepulcre, J.; Masdeu, J.C.; Goni, J.; Arrondo, G.; Velez de Mendizabal, N.; Bejarano, B. Fatigue in multiple sclerosis is associated with the disruption of frontal and parietal pathways. Mult. Scler. J. 2009, 15, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, R.; Miletich, R.S.; Henschel, K.; Shaikh, Z.A.; Janardhan, V.; Wasay, M. Fatigue in multiple sclerosis: cross-sectional correlation with brain MRI findings in 71 patients. Neurology 1999, 53, 1151–1153. [Google Scholar] [CrossRef] [PubMed]
- Mainero, C.; Faroni, J.; Gasperini, C.; Filippi, M.; Giugni, E.; Ciccarelli, O. Fatigue and magnetic resonance imaging activity in multiple sclerosis. J. Neurol. 1999, 246, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S., Jr.; Tan, H.; Otahal, P.; Taylor, B.; Ponsonby, A.L.; Lucas, R.M.; Blizzard, L.; Valery, P.C.; Lechner-Scott, J.; Shaw, C.; et al. Anxiety, depression and fatigue at 5-year review following CNS demyelination. Acta Neurol. Scand. 2016, 134, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Hameau, S.; Zory, R.; Latrille, C.; Roche, N.; Bensmail, D. Relationship between Neuromuscular and Perceived Fatigue and Locomotor Performance in Patients with Multiple Sclerosis. Available online: https://www.ncbi.nlm.nih.gov/m/pubmed/27164538/ (accessed on 11 August 2017).
- Clerx, L.; Jacobs, H.I.; Burgmans, S.; Gronenschild, E.H.; Uylings, H.B.; Echavarri, C. Sensitivity of different MRI-techniques to assess gray matter atrophy patterns in Alzheimer’s disease is region-specific. Curr. Alzheimer Res. 2013, 10, 940–951. [Google Scholar] [CrossRef] [PubMed]
- FreeSurfer. Available online: http://surfer.nmr.mgh.harvard.edu/ (accessed on 11 August 2017).
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 1999, 9, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; van der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S.; et al. Whole brain segmentation: Automated labeling of neuroanatomical structures in the human brain. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef]
- Fischl, B.; Sereno, M.I.; Dale, A.M. Cortical surface-based analysis. II: Inflation, flattening, and a surface-based coordinate system. Neuroimage 1999, 9, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; van Zijl, P.C.; Kim, J.; Pearlson, G.D.; Mori, S. DtiStudio: Resource program for diffusion tensor computation and fiber bundle tracking. Comput. Methods Progr. Biomed. 2006, 81, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Govindan, R.M.; Asano, E.; Juhasz, C.; Jeong, J.W.; Chugani, H.T. Surface-based laminar analysis of diffusion abnormalities in cortical and white matter layers in neocortical epilepsy. Epilepsia 2013, 54, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Biberacher, V.; Schmidt, P.; Selter, R.; Pernpeinter, V.; Kowarik, M.; Knier, B.; Duck, D.; Hoshi, M.-M.; Korn, T.; Berthele, A.; Kirschke, J.S.; et al. Fatigue in multiple sclerosis: Association with clinical, MRI and CSF parameters. Mult. Scler. J. 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Alvarez, L.A.; LaRocca, N.G.; Scheinberg, L.C. Fatigue in multiple sclerosis. Arch Neurol. 1988, 45, 435–437. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, R.; Shaikh, Z.A.; Miletich, R.S. Fatigue in multiple sclerosis and its relationship to depression and neurological disability. Mult. Scler. J. 2000, 6, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Finke, C.; Schlichting, J.; Papazoglou, S.; Scheel, M.; Freing, A.; Soemmer, C.; Pech, L.M.; Pajkert, A.; Pfüller, C.; Wuerfel, J.T.; et al. Altered basal ganglia functional connectivity in multiple sclerosis patients with fatigue. Mult. Scler. J. 2015, 21, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Roelcke, U.; Kappos, L.; Lechner-Scott, J.; Brunnschweiler, H.; Huber, S.; Ammann, W.; Plohmann, A.; Dellas, S.; Maguire, R.P.; Missimer, J.; et al. Reduced glucose metabolism in the frontal cortex and basal ganglia of multiple sclerosis patients with fatigue: A 18F-fluorodeoxyglucose positron emission tomography study. Neurology 1997, 48, 1566–1571. [Google Scholar] [CrossRef] [PubMed]
- Rocca, M.A.; Parisi, L.; Pagani, E.; Copetti, M.; Rodegher, M.; Colombo, B. Regional but not global brain damage contributes to fatigue in multiple sclerosis. Radiology 2014, 273, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Wilting, J.; Rolfsnes, H.O.; Zimmermann, H.; Behrens, M.; Fleischer, V.; Zipp, F. Structural correlates for fatigue in early relapsing remitting multiple sclerosis. Eur. Radiol. 2016, 26, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Nourbakhsh, B.; Azevedo, C.; Nunah-Saah, J.; Maghzi, A.; Spain, R.; Pelletier, D.; Waubant, E. Longitudinal associations between brain structural changes and fatigue in early MS. Mult. Scler. Relat. Disord. 2016, 5, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Hanken, K.; Eling, P.; Klein, J.; Klaene, E.; Hildebrandt, H. Different cortical underpinnings for fatigue and depression in MS? Mult. Scler. Relat. Disord. 2016, 6, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Bisecco, A.; Caiazzo, G.; Dambrosio, A.; Sacco, R.; Bonavita, S.; Docimo, R.; Cirillo, M.; Pagani, E.; Filippi, M.; Esposito, F.; et al. Faitgue in multiple sclerosis: The contribution of occult white mattre damage. Mult. Scler. J. 2016, 22, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, G.; Dinacci, D.; Lavorgna, L.; Prinster, A.; Savettieri, G.; Quattrone, A.; Livera, P.; Messina, C.; Reggio, A.; Servillo, G.; et al. Correlation between fatigue and brain atrophy and lesion load in multiple sclerosis patients independent of disability. J. Neurol. Sci. 2007, 263, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Bester, M.; Lazar, M.; Petracca, M.; Babb, J.S.; Herbert, J.; Grossman, R.I. Tract-specific white matter correlates of fatigue and cognitive impairment in benign multiple sclerosis. J. Neurol. Sci. 2013, 330, 61–66. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| RRMS Population | HF Group | MF Group | LF Group | Total | p-Value |
|---|---|---|---|---|---|
| Number of patients | 15 | 14 | 14 | 43 | |
| Ethnicity (Cau vs. AA) | 9 vs. 6 | 6 vs. 8 | 9 vs. 5 | 24 vs. 19 | |
| Age (years) | 43 ± 2.9 | 39 ± 3 | 39 ± 1.7 | 41 ± 1.7 | 0.102 |
| Range | (23–55) | (26–45) | (29–47) | (23–55) | |
| Mean FSS score | 6 ± 0.12 | 4 ± 0.14 | 1.89 ± 0.2 | 4.35 ± 0.26 | |
| Range | (5.1–7) | (3.1–5) | (1–3) | (1–7) | |
| Median EDSS score | 2 | 2 | 1.5 | 2 | 0.754 |
| Range | (1–4) | (1–4) | (1–4) | (1–4) | |
| T2 lesion volume (mL) | 14 ± 2.5 | 18.8 ± 4.8 | 15.3 ± 5.9 | 15.6 ± 2.3 | 0.859 |
| Range | (7.4–27.16) | (2.6–40.5) | (1.8–39.7) | (1.8–40.5) | |
| Disease period (years) | 10 ± 1.7 | 9.2 ± 1.2 | 8.6 ± 1.9 | 9.3 ± 1 | 0.136 |
| Range | (0.5–19.17) | (0.67–14.4) | (0.25–15) | (0.25–19.17) |
| (a) | |||
| Standarized Beta Coefficient | Standard Error | p-Value | |
| Thalamic volume | −1.042 | 0.514 | 0.043 |
| Pallidal volume | 0.068 | 1.435 | 0.962 |
| SCP volume | −0.014 | 0.013 | 0.291 |
| FA-RTC | −82.839 | 36.316 | 0.023 |
| RD-RTC | −8567.04 | 10.782.51 | 0.427 |
| (b) | |||
| Standarized Beta Coefficient | Standard Error | p-Value | |
| Age | 0.119 | 0.061 | 0.058 |
| Thalamic volume | −0.96 | 0.505 | 0.050 |
| Pallidal volume | −0.14 | 1.474 | 0.924 |
| SCP volume | −0.027 | 0.016 | 0.099 |
| FA-RTC | −113.826 | 44.699 | 0.011 |
| RD-RTC | −11070.1 | 10884.88 | 0.309 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernitsas, E.; Yarraguntla, K.; Bao, F.; Sood, R.; Santiago-Martinez, C.; Govindan, R.; Khan, O.; Seraji-Bozorgzad, N. Structural and Neuronal Integrity Measures of Fatigue Severity in Multiple Sclerosis. Brain Sci. 2017, 7, 102. https://doi.org/10.3390/brainsci7080102
Bernitsas E, Yarraguntla K, Bao F, Sood R, Santiago-Martinez C, Govindan R, Khan O, Seraji-Bozorgzad N. Structural and Neuronal Integrity Measures of Fatigue Severity in Multiple Sclerosis. Brain Sciences. 2017; 7(8):102. https://doi.org/10.3390/brainsci7080102
Chicago/Turabian StyleBernitsas, Evanthia, Kalyan Yarraguntla, Fen Bao, Rishi Sood, Carla Santiago-Martinez, Rajkumar Govindan, Omar Khan, and Navid Seraji-Bozorgzad. 2017. "Structural and Neuronal Integrity Measures of Fatigue Severity in Multiple Sclerosis" Brain Sciences 7, no. 8: 102. https://doi.org/10.3390/brainsci7080102