Conventional Structural Magnetic Resonance Imaging in Differentiating Chronic Disorders of Consciousness

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DOC | disorders of consciousness |
| UWS | unresponsive wakefulness syndrome |
| MCS | minimally conscious state |
| CRS-R | coma recovery scale revised |
| 18F-FDG PET | fluorine-18 fluorodeoxyglucose positron emission tomography |
| MRI | magnetic resonance imaging |
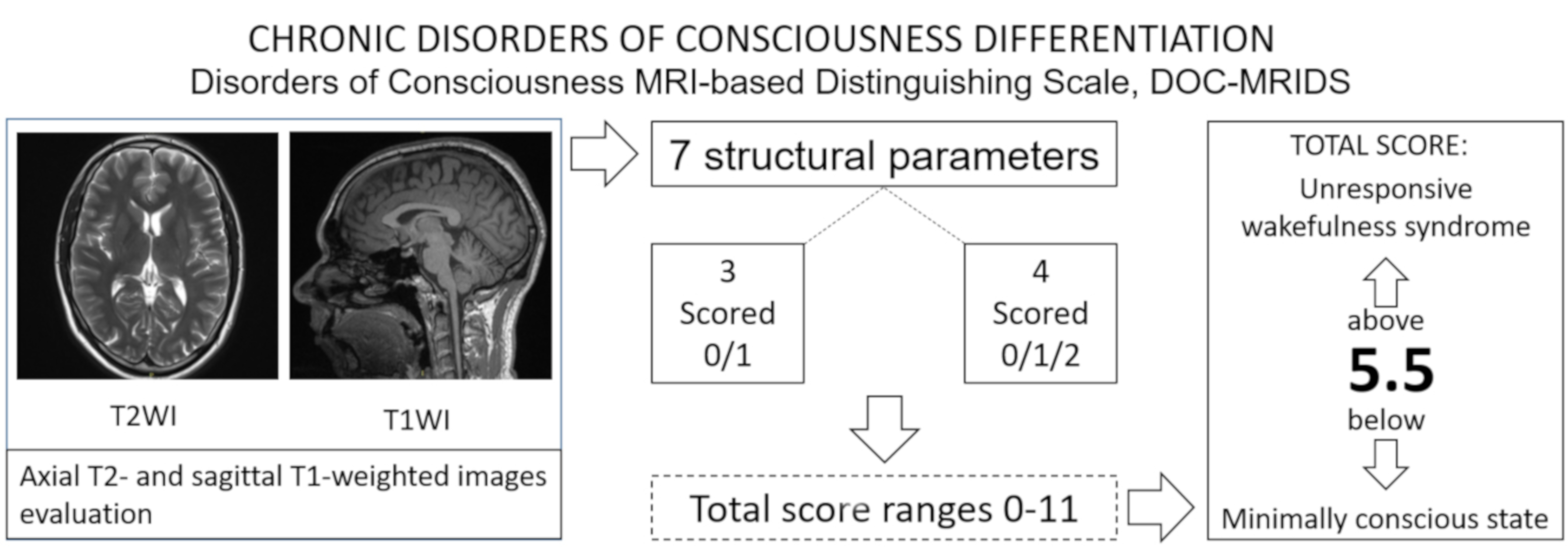
| DOC-MRIDS | disorders of consciousness MRI-based distinguishing scale |
| TR | repetition time |
| TE | echo tome |
| WI | weighted images |
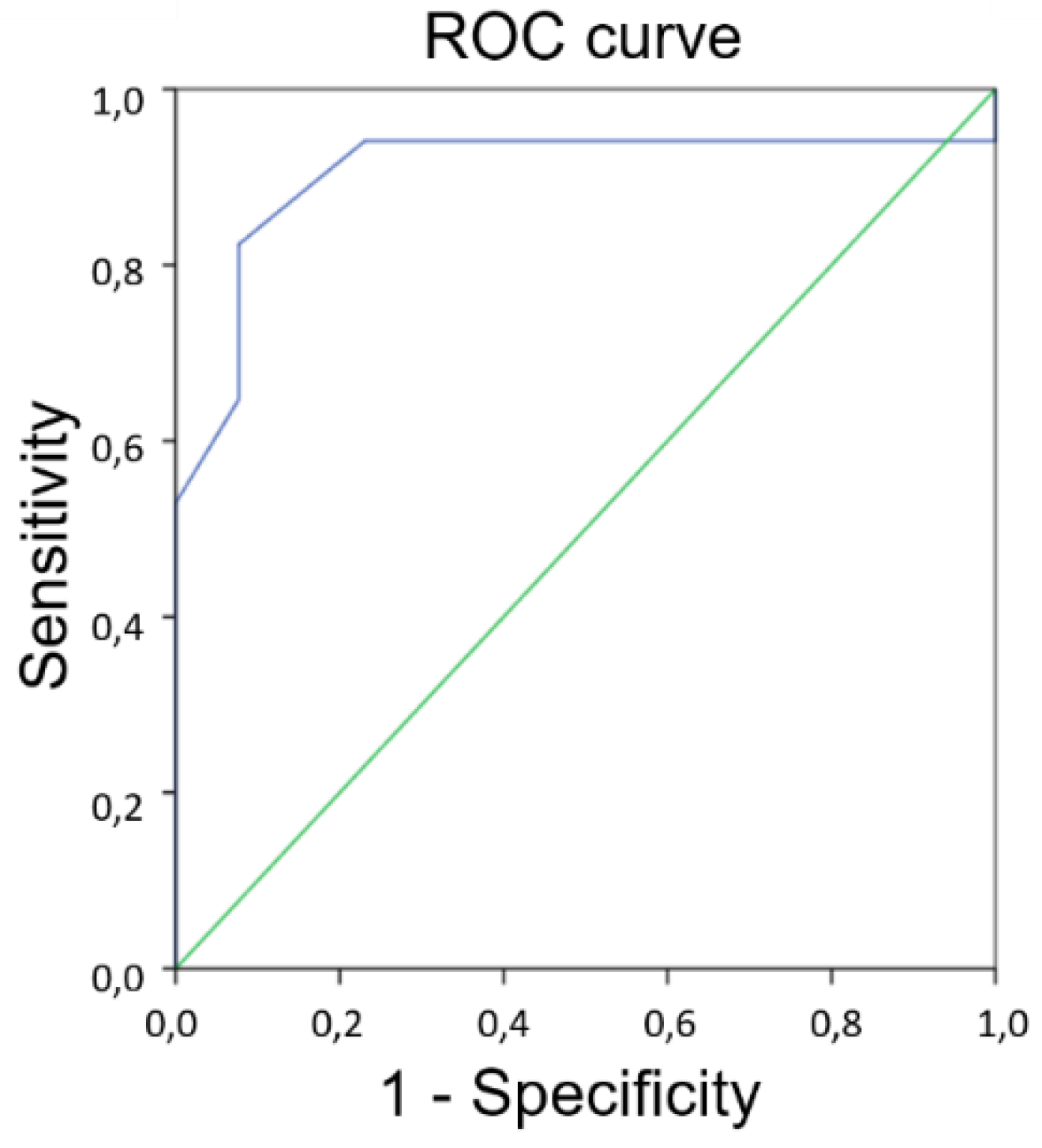
| ROC | receiver operating characteristic |
| AUC | area under the curve |
References
- Laureys, S. The neural correlate of (un)awareness: Lessons from the vegetative state. Trends Cogn. Sci. 2005, 12, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Laureys, S.; Boly, M.; Moonen, G.; Maquet, P. Coma. In Encyclopedia of Neuroscience; Squire, L., Ed.; Academic Press: Oxford, UK, 2009; Volume 2, pp. 1133–1142. [Google Scholar]
- Koch, C.; Massimini, M.; Boly, M.; Tononi, G. Neural correlates of consciousness: Progress and problems. Nat. Rev. Neurosci. 2016, 17, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Monti, M.M.; Laureys, S.; Owen, A.M. The vegetative state. J. Neurol. Neurosurg. Psychiatry 2010, 341, c3765. [Google Scholar] [CrossRef] [PubMed]
- Laurey, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Multi-Society Task Force on PVS. Medical Aspects of the Persistent Vegetative State. N. Engl. J. Med. 1994, 330, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T. The vegetative and minimally conscious states: Consensus-based criteria for establishing diagnosis and prognosis. Neurorehabilitation 2004, 19, 293–298. [Google Scholar] [PubMed]
- Gill-Thwaites, H. Lotteries, loopholes and luck: Misdiagnosis in the vegetative state patient. Brain Inj. 2006, 20, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Schnakers, C.; Vanhaudenhuyse, A.; Giacino, J.; Ventura, M.; Boly, M.; Majerus, S.; Moonen, G.; Laureys, S. Diagnostic accuracy of the vegetative and minimally conscious state: Clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- American Congress of Rehabilitation Medicine; Brain Injury-Interdisciplinary Special Interest Group; Disorders of Consciousness Task Force; Seel, R.T.; Sherer, M.; Whute, J.; Katz, D.I.; Giacino, J.T.; Rosenbaum, A.M.; Hammond, F.M.; et al. Assessment scales for disorders of consciousness: Evidence-based recommendations for clinical practice and research. Arch. Phys. Med. Rehabil. 2010, 12, 1795–1813. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.M.; Coleman, M.R.; Boly, M.; Davis, M.H.; Laureys, S.; Pickard, J.D. Detecting awareness in the vegetative state. Science 2006, 313, 1402. [Google Scholar] [CrossRef] [PubMed]
- Schnakers, C.; Giacino, J.T.; Lovstad, M.; Habbal, D.; Boly, M.; Di, H.; Majerus, S.; Laureys, S. Preserved covert cognition in noncommunicative patients with severe brain injury? Neurorehabil. Neural Repair 2015, 29, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Monti, M.M.; Vanhaudenhuyse, A.; Coleman, M.R.; Boly, M.; Pickard, J.D.; Tshibanda, L.; Owen, A.M.; Laureys, S. Willful modulation of brain activity in disorders of consciousness. N. Engl. J. Med. 2010, 362, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Stender, J.; Gosseries, O.; Bruno, M.A.; Charland-Verville, V.; Vanhaudenhuyse, A.; Demertzi, A.; Chatelle, C.; Thonnard, M.; Thibaut, A.; Heine, L.; et al. Diagnostic precision of PET imaging and functional MRI in disorders of consciousness: A clinical validation study. Lancet 2014, 384, 514–522. [Google Scholar] [CrossRef]
- Crone, J.S.; Bio, B.J.; Vespa, P.M.; Lutkenhoff, E.S.; Monti, M.M. Restoration of thalamo-cortical connectivity after brain injury: Recovery of consciousness, complex behavior, or passage of time. J. Neurosci. Res. 2018, 96, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Demertzi, A.; Antonopoulos, G.; Heine, L.; Voss, H.U.; Crone, J.S.; de Los Angeles, C.; Bahri, M.A.; Di Perri, C.; Vanhaudenhuyse, A.; Charland-Verville, V.; et al. Intrinsic functional connectivity differentiates minimally conscious from unresponsive patients. Brain 2015, 138, 2619–2631. [Google Scholar] [CrossRef] [PubMed]
- Lutkenhoff, E.S.; Chiang, J.; Tshibanda, L.; Kamau, E.; Kirsch, M.; Pickard, J.D.; Laureys, S.; Owen, A.M.; Monti, M.M. Thalamic and extrathalamic mechanisms of consciousness after severe brain injury. Ann. Neurol. 2015, 78, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Espejo, D.; Junque, C.; Bernabeu, M.; Roig-Rovira, T.; Vendrell, P.; Mercader, J.M. Reductions of thalamic volume and regional shape changes in the vegetative and the minimally conscious states. J. Neurotrauma 2010, 27, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Guldenmund, P.; Soddu, A.; Baquero, K.; Vanhaudenhuyse, A.; Bruno, M.-A.; Gosseries, O.; Laureys, S.; Gуmez, F. Structural brain injury in patients with disorders of consciousness: A voxel-based morphometry study. Brain Inj. 2016, 30, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Kampfl, A.; Schmutzhard, E.; Franz, G.; Pfausler, B.; Haring, H.-P.; Ulmer, H.; Felber, S.; Golaszewski, S.; Aichner, F. Prediction of recovery from post-traumatic vegetative state with cerebral magnetic-resonance imaging. Lancet 1998, 351, 1763–1767. [Google Scholar] [CrossRef]
- Annen, J.; Frasso, G.; Crone, J.S.; Heine, L.; di Perri, C.; Martial, C.; Cassol, H.; Demertzi, A.; Naccache, L.; Laureys, S.; et al. Regional brain volumetry and brain function in severely brain-injured patients. Ann. Neurol. 2018, 83, 842–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoelper, B.M.; Soldner, F.; Choné, L.; Wallenfang, T. Effect of intracerebral lesions detected in early MRI on outcome after acute brain injury. Acta Neurochir. Suppl. 2000, 76, 265–267. [Google Scholar] [PubMed]
- Evans, W.A. An encephalographic ratio for estimating ventricular enlargement and cerebral atrophy. Arch. Neurol. Psychiatry 1942, 47, 931–937. [Google Scholar] [CrossRef]
- Ber, M.; Frotscher, M. Topical Diagnosis in Neurology; Suslina, Z.A., Ed.; Practical Medicine: Moscow, Russia, 2009; p. 608. ISBN 978-5-98811-306-5. [Google Scholar]
- Biryukov, A.N.; Medvedeva, Y.I.; Khazov, P.D. Age and sex aspects of MRI callosometry. Vestnik St. Petersburg Med. Acad. Postgrad. Educ. 2011, 4, 59–63. [Google Scholar]
- Bruno, M.A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Casarotto, S.; Comanducci, A.; Rosanova, M.; Sarasso, S.; Fecchio, M.; Napolitani, M.; Pigorini, A.; Casali, A.; Trimarchi, P.D.; Boly, M.; et al. Stratification of unresponsive patients by an independently validated index of brain complexity. Ann. Neurol. 2016, 80, 718–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Score | |||
|---|---|---|---|---|
| Absence | Presence | Moderate Changes Presence | Severe Changes Presence | |
| diffuse cortical atrophy | 0 | 1 | - | - |
| brainstem and/or thalamus degeneration | 0 | 1 | - | - |
| corpus callosum lesions | 0 | 1 | - | - |
| ventricular enlargement | 0 | - | 1 | 2 |
| sulcal widening | 0 | - | 1 | 2 |
| leukoaraiosis | 0 | - | 1 | 2 |
| corpus callosum degeneration | 0 | - | 1 | 2 |
| No. | Age | Sex | Aetiol * | CRS-R | Aud | Vis | Mot | Ver | Comm | Arous | DOC | DOC-MRIDS | DCA | VE | SW | Leu | BTD | CCD | CCL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 23 | M | TR | 20 | 4 | 5 | 5 | 2 | 1 | 3 | MCS | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 1 |
| 2 | 50 | M | ANOX | 10 | 2 | 1 | 3 | 1 | 1 | 2 | MCS | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 3 | 21 | M | ANOX | 4 | 0 | 0 | 1 | 1 | 0 | 2 | UWS | 8 | 1 | 2 | 0 | 2 | 1 | 2 | 0 |
| 4 | 31 | F | ANOX | 7 | 1 | 1 | 2 | 1 | 0 | 2 | UWS | 8 | 1 | 2 | 1 | 2 | 1 | 1 | 0 |
| 5 | 61 | F | ANOX | 5 | 0 | 0 | 2 | 1 | 0 | 2 | UWS | 9 | 1 | 1 | 1 | 2 | 1 | 2 | 1 |
| 6 | 31 | F | ANOX | 18 | 4 | 4 | 5 | 1 | 2 | 2 | MCS | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 7 | 49 | F | TR | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 7 | 0 | 2 | 0 | 1 | 1 | 2 | 1 |
| 8 | 22 | M | ANOX | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 8 | 1 | 2 | 1 | 2 | 1 | 1 | 0 |
| 9 | 19 | F | TR | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 5 | 0 | 2 | 0 | 1 | 1 | 1 | 0 |
| 10 | 26 | M | TR | 11 | 2 | 3 | 3 | 1 | 0 | 2 | MCS | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 1 |
| 11 | 23 | M | TR | 8 | 1 | 1 | 2 | 2 | 0 | 2 | UWS | 5 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| 12 | 22 | M | TR | 3 | 0 | 0 | 1 | 1 | 0 | 1 | UWS | 8 | 1 | 2 | 0 | 2 | 1 | 2 | 0 |
| 13 | 50 | M | ANOX | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 6 | 1 | 1 | 2 | 1 | 0 | 1 | 0 |
| 14 | 24 | F | TR | 21 | 4 | 5 | 5 | 1 | 2 | 3 | MCS | 2 | 0 | 1 | 0 | 1 | 0 | 0 | 0 |
| 15 | 55 | M | ANOX | 15 | 2 | 2 | 4 | 2 | 2 | 3 | MCS | 3 | 0 | 1 | 1 | 1 | 0 | 0 | 0 |
| 16 | 55 | M | ANOX | 4 | 0 | 1 | 1 | 1 | 0 | 1 | UWS | 6 | 1 | 1 | 1 | 2 | 1 | 0 | 0 |
| 17 | 56 | F | DEM | 18 | 3 | 4 | 4 | 2 | 2 | 3 | MCS | 5 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| 18 | 22 | F | TR | 7 | 1 | 1 | 2 | 1 | 0 | 2 | UWS | 7 | 1 | 2 | 0 | 1 | 1 | 1 | 1 |
| 19 | 32 | M | ANOX | 18 | 4 | 4 | 5 | 1 | 2 | 2 | MCS | 2 | 0 | 1 | 0 | 0 | 0 | 1 | 0 |
| 20 | 28 | F | ANOX | 4 | 0 | 0 | 1 | 1 | 0 | 2 | UWS | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 21 | 51 | M | ANOX | 5 | 1 | 0 | 1 | 1 | 0 | 2 | UWS | 9 | 1 | 1 | 2 | 2 | 1 | 2 | 0 |
| 22 | 24 | F | ANOX | 4 | 0 | 0 | 1 | 1 | 0 | 2 | UWS | 8 | 1 | 1 | 2 | 2 | 1 | 1 | 0 |
| 23 | 33 | M | ANOX | 12 | 1 | 2 | 3 | 2 | 1 | 3 | MCS | 3 | 0 | 1 | 0 | 0 | 1 | 0 | 1 |
| 24 | 53 | M | ANOX | 12 | 2 | 3 | 3 | 1 | 1 | 2 | MCS | 5 | 1 | 1 | 0 | 2 | 1 | 0 | 0 |
| 25 | 43 | F | ANOX | 13 | 3 | 3 | 3 | 1 | 1 | 2 | MCS | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| 26 | 56 | M | ANOX | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 8 | 1 | 1 | 2 | 2 | 1 | 1 | 0 |
| 27 | 46 | F | ANOX | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 11 | 1 | 2 | 2 | 2 | 1 | 2 | 1 |
| 28 | 47 | M | ANOX | 10 | 2 | 3 | 2 | 1 | 0 | 2 | MCS | 7 | 1 | 1 | 2 | 2 | 0 | 1 | 0 |
| 29 | 22 | M | TR | 12 | 3 | 3 | 3 | 1 | 0 | 2 | MCS | 3 | 0 | 1 | 0 | 0 | 1 | 0 | 1 |
| 30 | 47 | M | ANOX | 6 | 1 | 0 | 2 | 1 | 0 | 2 | UWS | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Parameters | Prevalence in UWS/MCS Patients, % | |||
|---|---|---|---|---|
| Absent | Present | Moderate Changes | Severe Changes | |
| diffuse cortical atrophy | 29.4/85.0 | 70.6/15.0 | - | - |
| brainstem and/or thalamus degeneration | 11.8/69.2 | 88.2/30.8 | - | - |
| corpus callosum lesions | 64.7/46.2 | 35.3/53.8 | - | - |
| ventricular enlargement | 5.9/0.0 | - | 47.0/100 | 47.0/0.0 |
| sulcal widening | 35.3/53.8 | - | 35.3/38.5 | 29.4/7.7 |
| leukoaraiosis | 5.9/69.2 | - | 35.3/15.4 | 58.8/15.4 |
| corpus callosum degeneration | 11.8/77.0 | - | 52.9/23.0 | 35.3/0.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morozova, S.; Kremneva, E.; Sergeev, D.; Sinitsyn, D.; Legostaeva, L.; Iazeva, E.; Krotenkova, M.; Ryabinkina, Y.; Suponeva, N.; Piradov, M. Conventional Structural Magnetic Resonance Imaging in Differentiating Chronic Disorders of Consciousness. Brain Sci. 2018, 8, 144. https://doi.org/10.3390/brainsci8080144
Morozova S, Kremneva E, Sergeev D, Sinitsyn D, Legostaeva L, Iazeva E, Krotenkova M, Ryabinkina Y, Suponeva N, Piradov M. Conventional Structural Magnetic Resonance Imaging in Differentiating Chronic Disorders of Consciousness. Brain Sciences. 2018; 8(8):144. https://doi.org/10.3390/brainsci8080144
Chicago/Turabian StyleMorozova, Sofya, Elena Kremneva, Dmitry Sergeev, Dmitry Sinitsyn, Lyudmila Legostaeva, Elizaveta Iazeva, Marina Krotenkova, Yulia Ryabinkina, Natalia Suponeva, and Michael Piradov. 2018. "Conventional Structural Magnetic Resonance Imaging in Differentiating Chronic Disorders of Consciousness" Brain Sciences 8, no. 8: 144. https://doi.org/10.3390/brainsci8080144