Impact of Cell-Free Fetal DNA Screening on Patients’ Choice of Invasive Procedures after a Positive California Prenatal Screen Result

Abstract
:1. Introduction
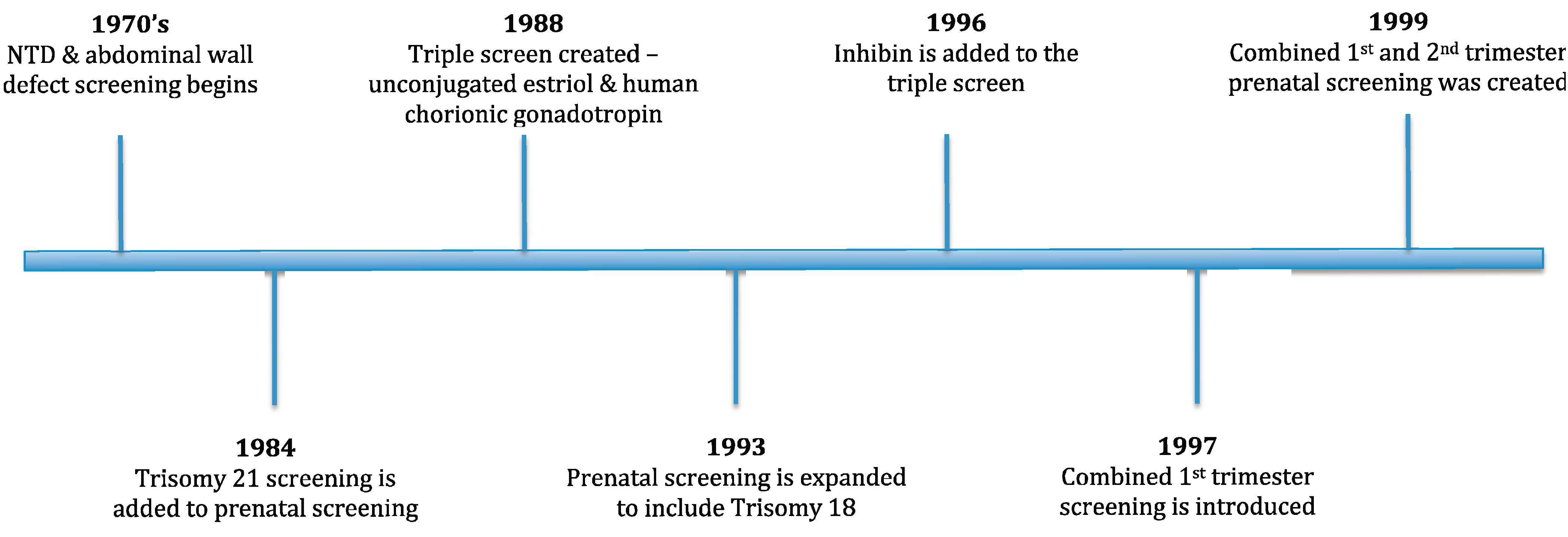
1.1. Basis and History of Prenatal Screening

1.2. California Prenatal Screening Program

{kind=link}
| Components | Detection Rates (%) [23,24] | Highest Detection Rates (%) | Lowest False Positive Rates (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Screening Category | 1st T Serum | NT | 2nd T Serum | T18 | T21 | T18 | T21 | T18 | T21 |
| First Trimester Combined | ♦ | ♦ | 69 | 75 | |||||
| Quadruple | ♦ | 67 | 80 | ||||||
| Quadruple + NT | ♦ | ♦ | 72 | 89 | |||||
| Serum Integrated | ♦ | ♦ | 79 | 85 | |||||
| Sequential Integrated | ♦ | ♦ | ♦ | 81 | 90 | ||||
| CPSP | 91 | 94 | 0.31 | 4.5 | |||||
| Cff-DNA Screening * | >99.9 | 99.1 | 0.4 | 0.1 | |||||
1.3. Cell-Free Fetal DNA Screening
1.4. Diagnostic Tests vs. Screening Tests
2. Experimental Section
2.1. Participants
2.2. Data Collected
2.3. Cell Free Fetal DNA Screening Laboratory
2.4. Genetic Counseling Session
2.5. Statistical Methods
3. Results
3.1. Cell-Free Fetal DNA Screening Impact on Testing Chosen
| Before Cell Free Fetal DNA Screening Was Offered (2011) | After Cell Free Fetal DNA Screening Was Offered (2012) | ||||||
|---|---|---|---|---|---|---|---|
| N | Mean | SD | N | Mean | SD | t-Test p-Value | |
| Age | 250 | 35.06 | 5.83 | 250 | 35.19 | 5.45 | 0.80 |
| Gestational Age | 242 | 17.37 | 2.54 | 240 | 17.66 | 2.45 | 0.20 |
| Positive Screen Risk for T21 | 243 | 3.88 | 7.02 | 243 | 3.40 | 5.43 | 0.40 |
| Positive Screen Risk for T18 | 13 | 10.75 | 11.37 | 11 | 6.42 | 9.70 | 0.33 |
| N | % | N | % | Chi-Squarep-Value | |||
| Ethnicity | 250 | 100.0 | 250 | 100.0 | 0.24 | ||
| Caucasian, Non-Hispanic | 100 | 40.0 | 86 | 34.4 | |||
| Hispanic | 104 | 41.6 | 97 | 38.8 | |||
| Asian | 37 | 14.8 | 51 | 20.4 | |||
| African American | 5 | 2.0 | 8 | 3.2 | |||
| Other | 4 | 1.6 | 8 | 3.2 | |||
| Gestational Trimester at Positive Screen | 250 | 100 | 250 | 100.0 | 0.75 | ||
| First Trimester | 55 | 22 | 58 | 23.2 | |||
| Second Trimester | 195 | 78 | 192 | 76.8 | |||
| Health Insurance | 250 | 100.0 | 250 | 100.0 | 0.51 | ||
| HMO | 55 | 22.0 | 42 | 16.8 | |||
| Medi-Cal | 83 | 33.2 | 89 | 35.6 | |||
| PPO | 100 | 40.0 | 108 | 43.2 | |||
| CPSP Screening Test | 250 | 100.0 | 250 | 100.0 | 0.85 | ||
| First Trimester Combined | 55 | 22.0 | 59 | 23.6 | |||
| Quadruple * | 66 | 26.4 | 67 | 26.8 | |||
| Serum Integrated | 60 | 24.0 | 52 | 20.8 | |||
| Sequential Integrated | 69 | 27.6 | 72 | 28.8 | |||
| Referral Reason | 250 | 100.0 | 250 | 100.0 | 0.60 | ||
| Positive Trisomy 18 Screen | 7 | 2.8 | 7 | 2.8 | |||
| Positive Trisomy 21 Screen | 237 | 94.8 | 240 | 96.0 | |||
| Positive T21 & T18 Screen | 6 | 2.4 | 3 | 1.2 | |||
| Before Cell-Free Screening Offered (2011) | After Cell-Free Screening Offered (2012) | Chi-square Test (2011 vs. 2012) | |||
|---|---|---|---|---|---|
| N | % | N | % | p-Value | |
| Testing Chosen | 250 | 100.0 | 250 | 100.0 | |
| No further testing | 110 | 44.0 | 79 | 31.6 | 0.006 a |
| Invasive testing | 117 | 46.8 | 72 | 28.8 | <0.001 b |
| CVS | 4 | 2 | |||
| Amniocentesis | 113 | 70 | |||
| Non-invasive testing | 23 | 9.2 | 99 | 39.6 | |
| Sequential Integrated | 23 | 24 | |||
| Cff-DNA Screening | NA | 75 | |||
| First Trimester test | 55 | 100.0 | 58 | 100.0 | |
| No further testing | 3 | 5.5 | 2 | 3.5 | 0.674 c |
| Invasive testing | 29 | 52.7 | 17 | 29.3 | 0.008 b |
| CVS | 4 | 2 | |||
| Amniocentesis | 25 | 15 | |||
| Non-invasive testing | 23 | 41.8 | 39 | 67.2 | |
| Sequential Integrated | 23 | 24 | |||
| cff-DNA Screening | NA | 15 | |||
| Second Trimester test | 195 | 100.0 | 192 | 100.0 | |
| No further testing | 107 | 54.9 | 77 | 40.1 | 0.004 a |
| Invasive testing | 88 | 45.1 | 55 | 28.6 | 0.004 b |
| CVS | NA | NA | |||
| Amniocentesis | 88 | 55 | |||
| Non-invasive testing | NA | 60 | 31.3 | ||
| Sequential Integrated | NA | NA | |||
| cff-DNA Screening | NA | 60 | |||
3.2. Cell-Free Fetal DNA Screening Impact on Testing Chosen by Trimester
3.3. Cell-Free Fetal DNA Screening Impact on Testing Chosen by Health Insurance
| Before Cell-Free Screening Offered (2011) | After Cell-Free Screening Offered (2012) | Chi-square Test (2011 vs. 2012) | |||
|---|---|---|---|---|---|
| N | % | N | % | p-Value | |
| No further testing | 44 | 53.0 | 45 | 50.6 | 0.748 a |
| Invasive testing | 32 | 38.6 | 27 | 30.3 | 0.038 b |
| CVS | 0 | 0 | |||
| Amniocentesis | 32 | 27 | |||
| Non-invasive testing | 7 | 8.4 | 17 | 19.1 | |
| Sequential Integrated | 7 | 3 | |||
| cff-DNA Screening | NA | 14 | |||
| Health Insurance—PPO | 100 | 100.0 | 108 | 100.0 | |
| No further testing | 37 | 37.0 | 18 | 16.7 | 0.009 a |
| Invasive testing | 53 | 53.0 | 32 | 29.6 | <0.001 b |
| CVS | 3 | 2 | |||
| Amniocentesis | 50 | 30 | |||
| Non-invasive testing | 10 | 10.0 | 58 | 53.7 | |
| Sequential Integrated | 10 | 15 | |||
| cff-DNA Screening | NA | 43 | |||
| Health Insurance—HMO | 55 | 100.0 | 42 | 100.0 | |
| No further testing | 21 | 38.2 | 10 | 23.8 | 0.133 a |
| Invasive testing | 28 | 50.9 | 11 | 26.2 | <0.001 b |
| CVS | 1 | 0 | |||
| Amniocentesis | 27 | 11 | |||
| Non-invasive testing | 6 | 10.9 | 21 | 50.0 | |
| Sequential Integrated | 6 | 6 | |||
| cff-DNA Screening | NA | 15 | |||
| Health Insurance—Unknown | 12 | 100.0 | 11 | 100.0 | |
| No further testing | 8 | 66.7 | 6 | 54.5 | 0.529 a |
| Invasive testing | 4 | 33.3 | 2 | 18.2 | 0.167 c |
| CVS | 0 | 0 | |||
| Amniocentesis | 4 | 2 | |||
| Non-invasive testing | 0 | 0.00 | 3 | 27.3 | |
| Sequential Integrated | 0 | 0 | |||
| cff-DNA Screening | NA | 3 | |||
| Χ2 (df = 3) test for difference in % who chose additional testing vs. no further testing by health insurance type | p = 0.046 | p < 0.001 | |||
3.4. Cell-Free Fetal DNA Screening Impact on Testing Chosen by Presence of Ultrasound Abnormalities
| Before Cell-Free Screening Offered (2011) | After Cell-Free Screening Offered (2012) | Chi-square Test (2011 vs. 2012) | |||
|---|---|---|---|---|---|
| N | % | N | % | p-Value | |
| Abnormalities Present on 2nd Trimester Ultrasound | 53 | 100.0 | 52 | 100.0 | |
| No further testing | 19 | 35.8 | 23 | 44.2 | 0.381 a |
| Invasive testing | 32 | 60.4 | 17 | 32.7 | 0.002 c |
| CVS | NA | NA | |||
| Amniocentesis | 32 | 17 | |||
| Non-invasive testing | 2 | 3.8 | 12 | 23.1 | |
| Sequential Integrated | 2 | 0 | |||
| cff-DNA Screening | NA | 12 | |||
| No Abnormalities Present on 2nd Trimester Ultrasound | 148 | 100.0 | 147 | 100.0 | |
| No further testing | 88 | 59.5 | 55 | 37.4 | <0.001 a |
| Invasive testing | 60 | 40.5 | 41 | 27.9 | |
| CVS | NA | NA | |||
| Amniocentesis | 0 | 41 | |||
| Non-invasive testing | 0 | 0.00 | 51 | 34.7 | <0.001 c |
| Sequential Integrated | 0 | 2 | |||
| cff-DNA Screening | NA | 49 | |||
| Χ2 (df = 1) test for difference in % who chose additional testing vs. no further testing by presence of U.S. abnormality | p = 0.003 | p = 0.387 | |||
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wald, N.; Brock, D.; Bonnar, J. Prenatal diagnosis of spina bifida and anencephaly by maternal serum-alpha-fetoprotein measurement. A controlled study. Lancet 1974, 1, 765–767. [Google Scholar] [CrossRef]
- Brock, D.; Bolton, A.; Scrimgeour, J. Prenatal diagnosis of spina bifida and anencephaly through maternal plasma-alpha-fetoprotein measurement. Lancet 1974, 1, 767–769. [Google Scholar]
- Burton, B. Elevated maternal serum alpha-fetoprotein (MSAFP): Interpretation and follow-up. Clin. Obstet. Gynecol. 1988, 31, 293–305. [Google Scholar] [CrossRef]
- Genetics, A.S.H. Maternal serum alpha-fetoprotein screening programs and quality control for laboratories performing maternal serum and amniotic fluid a-fetoprotein assays: Policy statement. Can. Med. Assoc. 1987, 136, 1253–1256. [Google Scholar]
- Wald, N.; Hackshaw, A. Combining ultrasound and biochemistry in first-trimester screening for Down’s syndrome. Prenat. Diagn. 1997, 17, 821–829. [Google Scholar] [CrossRef]
- Wald, N.J.; Watt, H.C.; Hackshaw, A.K. Integrated screening for Down’s syndrome on the basis of tests performed during the first and second trimesters. N. Engl. J. Med. 1999, 341, 461–467. [Google Scholar] [CrossRef]
- Cuckle, H.; Wald, N.; Lindenbaum, R. Maternal serum alpha-fetoprotein measurement: A screening test for Down syndrome. Lancet 1984, 323, 926–929. [Google Scholar] [CrossRef]
- Canick, J.; Knight, G. Low second trimester maternal serum unconjugated oestriol in pregnancies with Down’s syndrome. J. Obstet. 1988, 95, 330–333. [Google Scholar] [CrossRef]
- Bogart, M.H.; Pandian, M.R.; Jones, O.W. Abnormal maternal serum chorionic gonadotropin levels in pregnancies with fetal chromosome abnormalities. Prenat. Diagn. 1987, 7, 623–630. [Google Scholar] [CrossRef]
- Barkai, G.; Goldman, B.; Reis, L.; Chaki, R.; Zer, T.; Cuckle, H. Expaning multiple marker screening for Down’s syndrome to include Edward’s syndrome. Prenat. Diagn. 1993, 13, 843–850. [Google Scholar] [CrossRef]
- Simpson, J.L. Invasive procedures for prenatal diagnosis: Any future left? Best Pract. Res. Clin. Obstet. Gynaecol. 2012, 26, 625–638. [Google Scholar] [CrossRef]
- Emory University School of Medicine about Amniocentesis. Available online: http://genetics.emory.edu/docs/Emory_Human_Genetics_Amniocentesis.PDF (accessed on 30 January 2013).
- Emory University. About Chorionic Villus Sampling. 2008; 18–20. [Google Scholar]
- Simpson, J.L. Choosing the best prenatal screening protocol. N. Engl. J. Med. 2005, 353, 2068–2070. [Google Scholar] [CrossRef]
- Rhoads, G.G.; Jackson, L.G.; Schlesselman, S.E.; de la Cruz, F.F.; Desnick, R.J.; Golbus, M.S.; Ledbetter, D.H.; Lubs, H.A.; Mahoney, M.J.; Pergament, E. The safety and efficacy of chorionic villus sampling for early prenatal diagnosis of cytogenetic abnormalities. N. Engl. J. Med. 1989, 320, 609–617. [Google Scholar] [CrossRef]
- Alfirevic, Z.; Sundberg, K.; Brigham, S. Amniocentesis and chorionic villus sampling for prenatal diagnosis. Cochrane Database Syst. Rev. 2003, 1–23. [Google Scholar]
- Currier, R.; Wu, N.; van Meter, K.; Goldman, S.; Lorey, F.; Flessel, M. Integrated and first trimester prenatal screening in California: Program implementation and patient choice for follow-up services. Prenat. Diagn. 2012, 32, 1077–1083. [Google Scholar] [CrossRef]
- Flessel, M.C.; Lorey, F.W. The California Prenatal Screening Program: “Options and choices” not “coercion and eugenics”. Genet. Med. 2011, 13, 711–713. [Google Scholar] [CrossRef]
- Nicolaides, K.H.; Azar, G.; Byrne, D.; Mansur, C.; Marks, K. Fetal nuchal translucency: Ultrasound screening for chromosomal defects in first trimester of pregnancy. BMJ 1992, 304, 867–869. [Google Scholar] [CrossRef]
- Pandya, P.P.; Snijders, R.J.; Johnson, S.P.; de Lourdes Brizot, M.; Nicolaides, K.H. Screening for fetal trisomies by maternal age and fetal nuchal translucency thickness at 10 to 14 weeks of gestation. Br. J. Obstet. Gynaecol. 1995, 102, 957–962. [Google Scholar] [CrossRef]
- California Department of Public Health. The California Prenatal Screening Program; California Department of Public Health: Sacramento, CA, USA, 2011. [Google Scholar]
- Ehrich, M.; Deciu, C.; Zwiefelhofer, T.; Tynan, J.A.; Cagasan, L.; Tim, R.; Lu, V.; McCullough, R.; McCarthy, E.; Nygren, A.O.H.; et al. Noninvasive detection of fetal trisomy 21 by sequencing of DNA in maternal blood: A study in a clinical setting. Am. J. Obstet. Gynecol. 2011, 204. [Google Scholar] [CrossRef]
- Genetic Disease Screening Progrsm. The California Prenatal Screening Program Provider Handbook; California Department of Public Health: Sacramento, CA, USA, 2009; pp. 1–48. [Google Scholar]
- California Department of Public Health. California Department of Public Health PNS Program Expansion Summary; California Department of Public Health: Sacramento, CA, USA, 2008. [Google Scholar]
- Sequenom Center For Molecular MaterniT21(TM) Noninvasive Prenatal Test for Down Syndrome. Available online: http://www.thefreelibrary.com/Sequenom+Center+for+Molecular+Medicine+Announces+Launch+of...-a0269927244 (accessed on 29 January 2013).
- Allyse, M.; Sayres, L.C.; King, J.S.; Norton, M.E.; Cho, M.K. Cell-free fetal DNA testing for fetal aneuploidy and beyond: Clinical integration challenges in the U.S. context. Hum. Reprod. 2012, 27, 3123–3131. [Google Scholar] [CrossRef]
- Chan, K.C.A. Clinical applications of the latest molecular diagnostics in noninvasive prenatal diagnosis in maternal plasma. Top. Curr. Chem. 2014, 336, 47–65. [Google Scholar] [CrossRef]
- Norton, M.E.; Brar, H.; Weiss, J.; Karimi, A.; Laurent, L.C.; Caughey, A.B.; Rodriguez, M.H.; Williams, J.; Mitchell, M.E.; Adair, C.D.; et al. Non-Invasive Chromosomal Evaluation (NICE) Study: Results of a multicenter prospective cohort study for detection of fetal trisomy 21 and trisomy 18. Am. J. Obstet. Gynecol. 2012, 207. [Google Scholar] [CrossRef]
- Palomaki, G.E.; Deciu, C.; Kloza, E.M.; Lambert-Messerlian, G.M.; Haddow, J.E.; Neveux, L.M.; Ehrich, M.; van den Boom, D.; Bombard, A.T.; Grody, W.W.; et al. DNA sequencing of maternal plasma reliably identifies trisomy 18 and trisomy 13 as well as Down syndrome: An international collaborative study. Genet. Med. 2012, 14, 296–305. [Google Scholar] [CrossRef]
- Sequenom Laboratories MaterniT21 Plus. Available online: http//non-invasivetesting.com/PDF/en-provider.pdf (accessed on 23 May 2013).
- Jensen, T.J.; Zwiefelhofer, T.; Tim, R.C.; Džakula, Ž.; Kim, S.K.; Mazloom, A.R.; Zhu, Z.; Tynan, J.; Lu, T.; McLennan, G.; et al. High-Throughput Massively parallel sequencing for fetal aneuploidy detection from maternal plasma. PLoS One 2013, 8, e57381. [Google Scholar]
- Zoppi, M.A.; Ibba, R.M.; Putzolu, M.; Floris, M.; Monni, G. Nuchal translucency and the acceptance of invasive prenatal chromosomal diagnosis in women aged 35 and older. Obstet. Gynecol. 2001, 97, 916–920. [Google Scholar] [CrossRef]
- Chasen, S.T.; McCullough, L.B.; Chervenak, F.A. Is nuchal translucency screening associated with different rates of invasive testing in an older obstetric population? Am. J. Obstet. Gynecol. 2004, 190, 769–774. [Google Scholar] [CrossRef]
- Blumenfeld, Y.J.; Taylor, J.; Lee, H.C.; Hudgins, L.; Sung, J.F.; El-Sayed, Y.Y. Utilization of available prenatal screening and diagnosis: Effects of the California screen program. J. Perinatol. 2012, 32, 907–912. [Google Scholar] [CrossRef]
- De Graaf, I.M.; Tijmstra, T.; Bleker, O.P.; van Lith, J.M.M. Womens’ preference in Down syndrome screening. Prenat. Diagn. 2002, 22, 624–629. [Google Scholar] [CrossRef]
- Spencer, K. Point-of-Care screening for chromosomal anomalies in the first trimester of pregnancy. Clin. Chem. 2002, 48, 403–404. [Google Scholar]
- Hall, J.; Fiebig, D.G.; King, M.T.; Hossain, I.; Louviere, J.J. What influences participation in genetic carrier testing? Results from a discrete choice experiment. J. Health Econ. 2006, 25, 520–537. [Google Scholar] [CrossRef]
- Wilson, R.D.; Chitayat, D.; McGillivray, B.C. Fetal ultrasound abnormalities: Correlation with fetal karyotype, autopsy findings, and postnatal outcome—Five-year prospective study. Am. J. Med. Genet. 1992, 44, 586–590. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Shah, F.T.; French, K.S.; Osann, K.E.; Bocian, M.; Jones, M.C.; Korty, L. Impact of Cell-Free Fetal DNA Screening on Patients’ Choice of Invasive Procedures after a Positive California Prenatal Screen Result. J. Clin. Med. 2014, 3, 849-864. https://doi.org/10.3390/jcm3030849
Shah FT, French KS, Osann KE, Bocian M, Jones MC, Korty L. Impact of Cell-Free Fetal DNA Screening on Patients’ Choice of Invasive Procedures after a Positive California Prenatal Screen Result. Journal of Clinical Medicine. 2014; 3(3):849-864. https://doi.org/10.3390/jcm3030849
Chicago/Turabian StyleShah, Forum T., Kathryn Steinhaus French, Kathryn E. Osann, Maureen Bocian, Marilyn C. Jones, and Lauren Korty. 2014. "Impact of Cell-Free Fetal DNA Screening on Patients’ Choice of Invasive Procedures after a Positive California Prenatal Screen Result" Journal of Clinical Medicine 3, no. 3: 849-864. https://doi.org/10.3390/jcm3030849