Efficacy of Denosumab for Osteoporosis in Two Patients with Adult-Onset Still’s Disease—Denosumab Efficacy in Osteoporotic Still’s Disease Patients


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
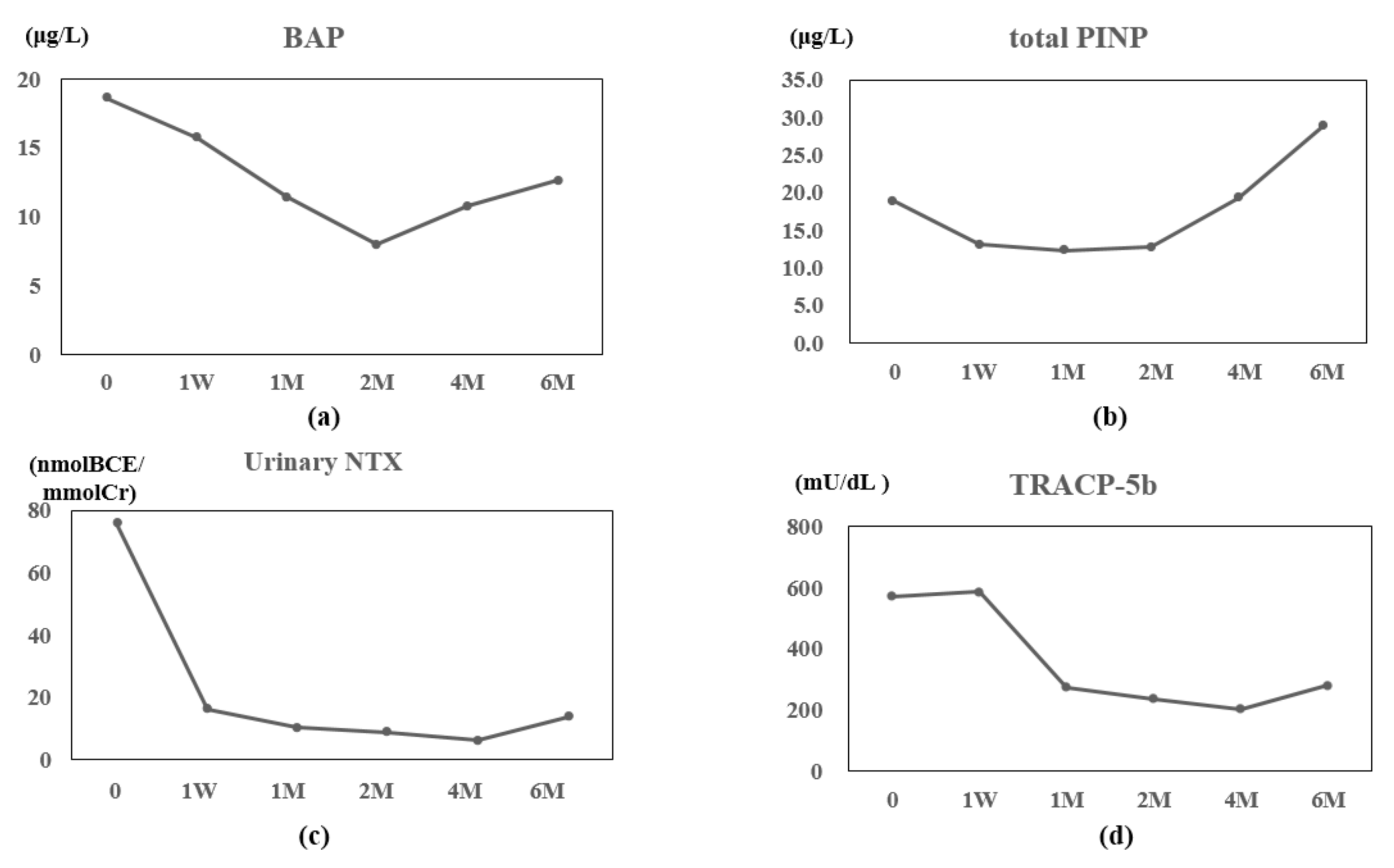
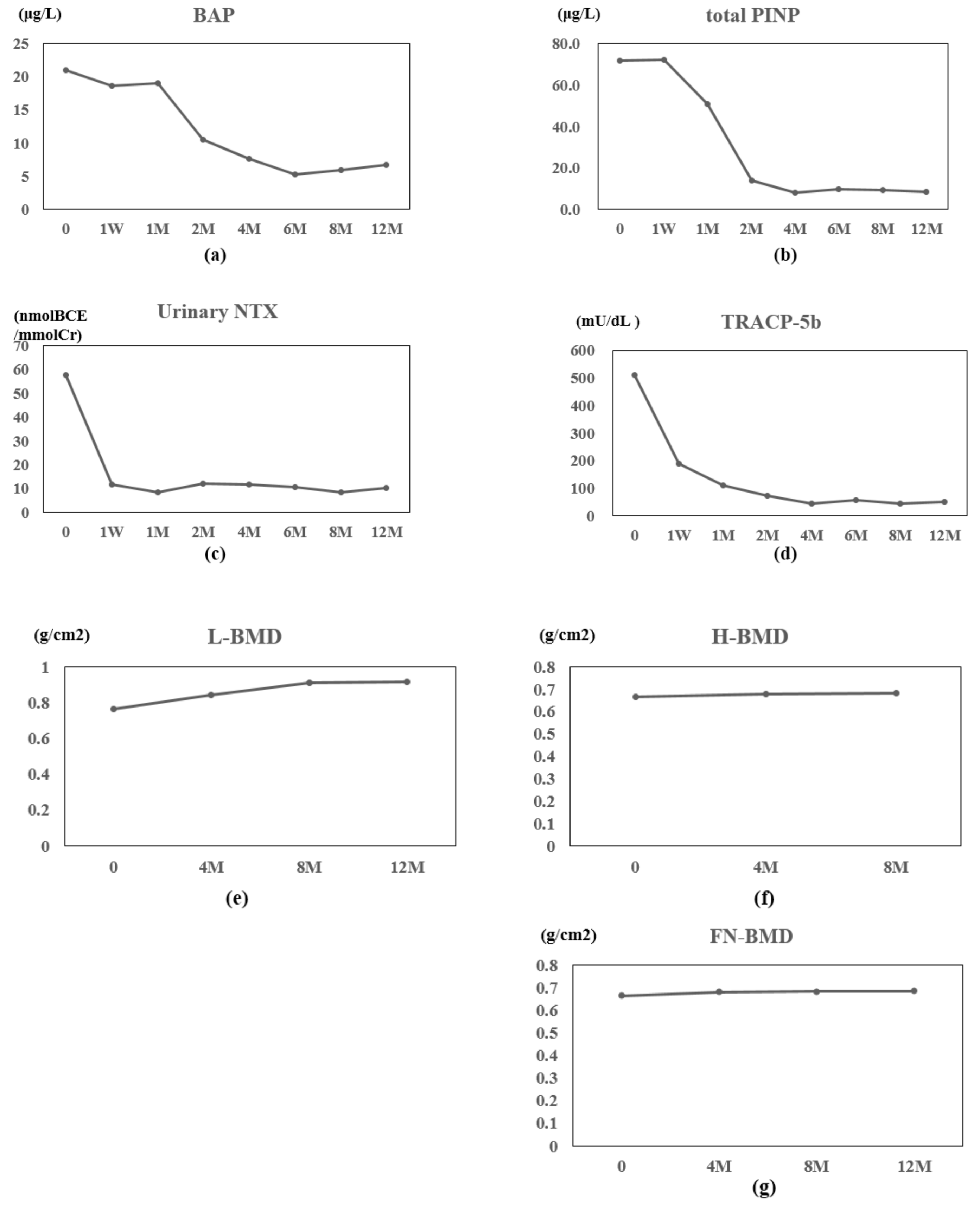
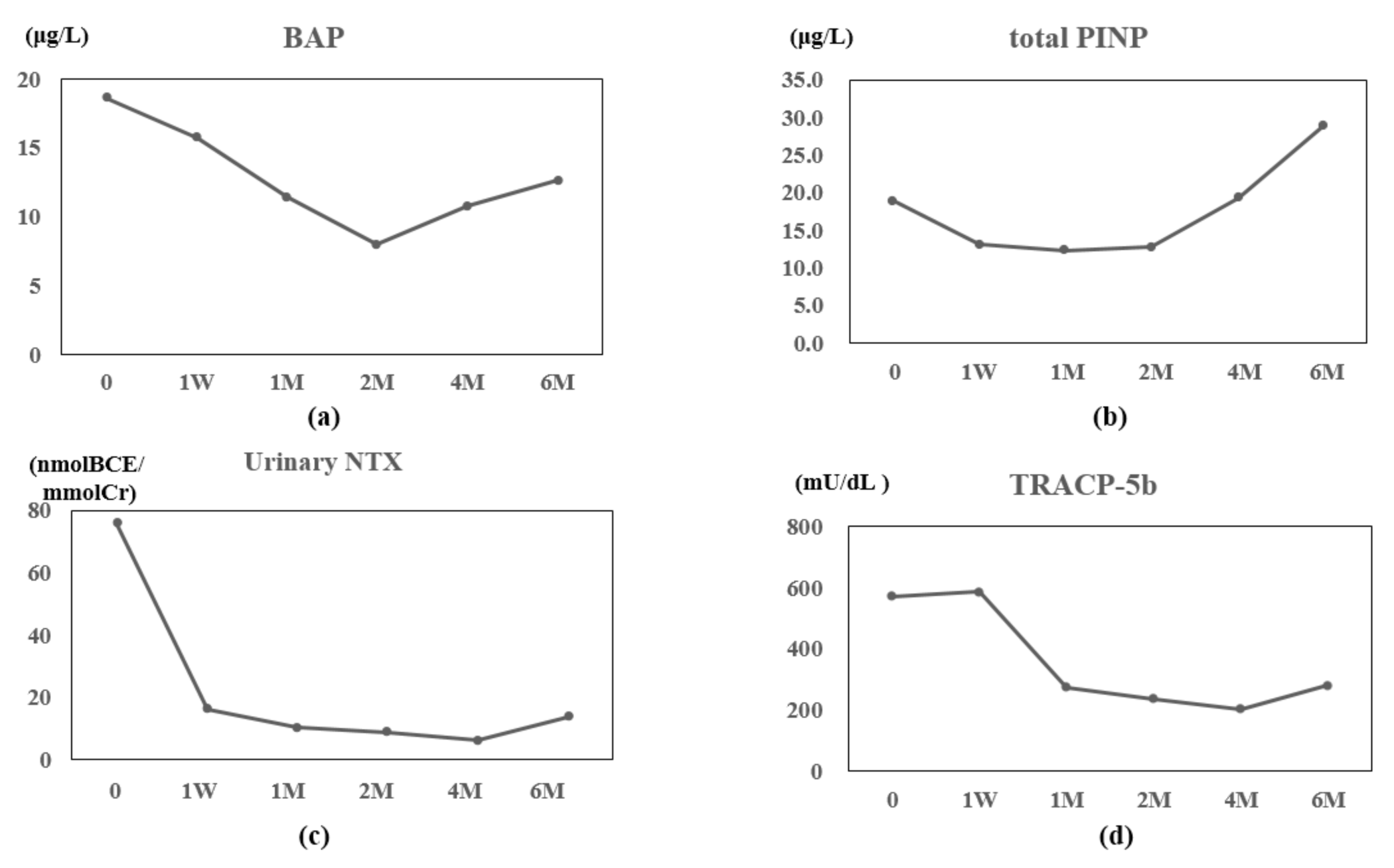
2.1. Case 1
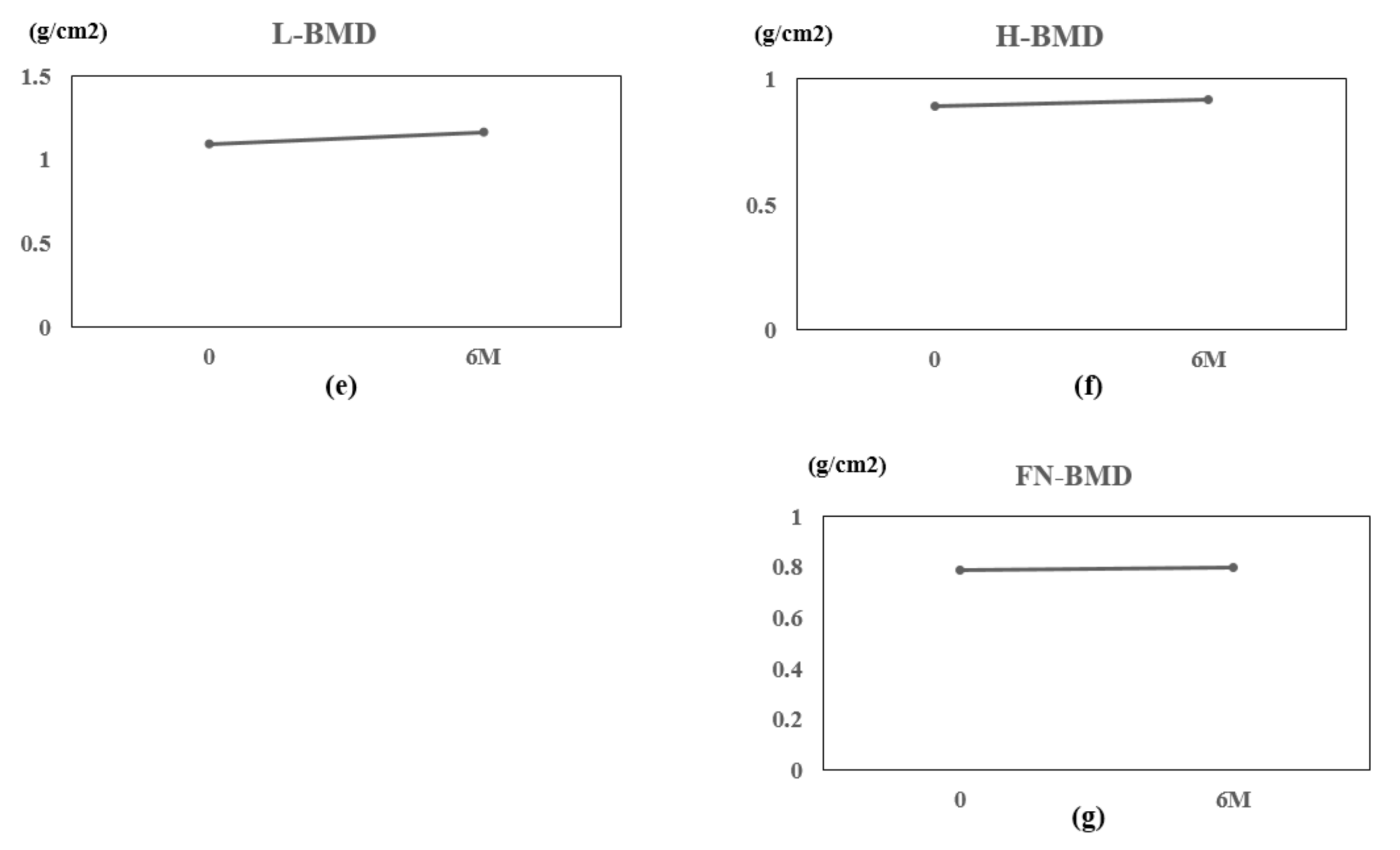
2.2. Case 2
3. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bywaters, E.G. Still’s disease in the adult. Ann. Rheum. Dis. 1971, 30, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, Y.F.; Mimura, T.; Tsuboi, H.; Noma, H.; Miyoshi, F.; Yamamoto, K.; Sumida, T. Nationwide epidemiological survey of 169 patients with adult Still’s disease in Japan. Mod. Rheumatol. 2015, 25, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Magadur-Joly, G.; Billaud, E.; Barrier, J.H.; Pennec, Y.L.; Masson, C.; Renou, P.; Prost, A. Epidemiology of adult Still’s disease: Estimate of the incidence by a retrospective study in west France. Ann. Rheum. Dis. 1995, 54, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Cagatay, Y.; Gul, A.; Cagatay, A.; Kamali, S.; Karadeniz, A.; Inanc, M.; Ocal, L.; Aral, O.; Konice, M. Adult-onset Still’s disease. Int. J. Clin. Pract. 2009, 63, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Kádár, J.; Petrovicz, E. Adult-onset Still’s disease. Best Pract. Res. Clin. Rheumatol. 2004, 8, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Tong, K.H.; To, C.H.; Siu, Y.P.; Ma, K.M. Risedronate for prevention of bone mineral density loss in patients receiving high-dose glucocorticoids: A randomized double-blind placebo-controlled trial. Osteoporos. Int. 2008, 19, 357–364. [Google Scholar] [CrossRef] [PubMed]
- McClung, M.R.; Lewiecki, E.M.; Cohen, S.B.; Bolognese, M.A.; Woodson, G.C.; Moffett, A.H.; Peacock, M.; Miller, P.D.; Lederman, S.N.; Chesnut, C.H.; et al. Denosumab in postmenopausal women with low bone mineral density. N. Engl. J. Med. 2006, 354, 821–831. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Nawata, H.; Soen, S.; Fujiwara, S.; Nakayama, H.; Tanaka, I.; Ozono, K.; Sagawa, A.; Takayanagi, R.; Tanaka, H.; et al. Guidelines on the management and treatment of glucocorticoid-induced osteoporosis of the Japanese Society for Bone and Mineral Research: 2014 update. J. Bone Miner. Metab. 2014, 32, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Efthimiou, P.; Georgy, S. Pathogenesis and management of adult-onset Still’s disease. Semin. Arthritis Rheum. 2006, 36, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Ohta, A.; Tsunematsu, T.; Kasukawa, R.; Mizushima, Y.; Kashiwagi, H.; Kashiwazaki, S.; Tanimoto, K.; Matsumoto, Y.; Ota, T.; et al. Preliminary criteria for classification of adult Still’s disease. J. Rheumatol. 1992, 19, 424–430. [Google Scholar] [PubMed]
- Karmakar, S.; Kay, J.; Gravallese, E.M. Bone damage in rheumatoid arthritis: Mechanistic insights and approaches to prevention. Rheum. Dis. Clin. N. Am. 2010, 36, 385–404. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Gu, L.; Wang, X.; Guo, L.; Shi, H.; Yang, C.; Chen, S. A pilot study on Tocilizumab for treating refractory adult-onset Still’s disease. Sci. Rep. 2017, 7, 13477. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, S.; Ito, K.; Nakagawa, S.; Hataji, O.; Sudo, A. The clinical benefits of denosumab for prophylaxis of steroid-induced osteoporosis in patients with pulmonary disease. Arch. Osteoporos. 2017, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, M.; Komatsuda, A.; Togashi, M.; Wakui, H.; Takahashi, N. Effects of denosumab on bone metabolic markers and bone mineral density in patients treated with glucocorticoids. Intern. Med. 2017, 56, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nakamura, Y.; Kato, H. Significant improvement of bone mineral density by denosumab without bisphosphonate pre-treatment in glucocorticoid-induced osteoporosis. Mod. Rheumatol. 2018, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Ito, M.; Hayashi, Y.; Hirota, T.; Tanigawara, Y.; Sone, T.; Fukunaga, M.; Shiraki, M.; Nakamura, T. A new active vitamin D3 analog, eldecalcitol, prevents the risk of osteoporotic fractures—A randomized, active comparator, double-blind study. Bone 2011, 49, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Mukaiyama, K.; Uchiyama, S.; Nakamura, Y.; Ikegami, S.; Taguchi, A.; Kamimura, M.; Kato, H. Eldecalcitol, in combination with bisphosphonate, is effective for treatment of Japanese osteoporotic patients. Tohoku J. Exp. Med. 2015, 237, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nakamura, Y.; Tanaka, M.; Kamimura, M.; Ikegami, S.; Uchiyama, S.; Kato, H. Comparison of the effects of denosumab with either active vitamin D or native vitamin D on bone mineral density and bone turnover markers in postmenopausal osteoporosis. Mod. Rheumatol. 2017, 28, 376–379. [Google Scholar] [CrossRef] [PubMed]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumaki, D.; Nakamura, Y.; Suzuki, T.; Kato, H. Efficacy of Denosumab for Osteoporosis in Two Patients with Adult-Onset Still’s Disease—Denosumab Efficacy in Osteoporotic Still’s Disease Patients. J. Clin. Med. 2018, 7, 63. https://doi.org/10.3390/jcm7040063
Kumaki D, Nakamura Y, Suzuki T, Kato H. Efficacy of Denosumab for Osteoporosis in Two Patients with Adult-Onset Still’s Disease—Denosumab Efficacy in Osteoporotic Still’s Disease Patients. Journal of Clinical Medicine. 2018; 7(4):63. https://doi.org/10.3390/jcm7040063
Chicago/Turabian StyleKumaki, Daiki, Yukio Nakamura, Takako Suzuki, and Hiroyuki Kato. 2018. "Efficacy of Denosumab for Osteoporosis in Two Patients with Adult-Onset Still’s Disease—Denosumab Efficacy in Osteoporotic Still’s Disease Patients" Journal of Clinical Medicine 7, no. 4: 63. https://doi.org/10.3390/jcm7040063