The Relationship between Sleep Problems, Neurobiological Alterations, Core Symptoms of Autism Spectrum Disorder, and Psychiatric Comorbidities

 ,
, {kind=link}
Abstract
:1. Introduction
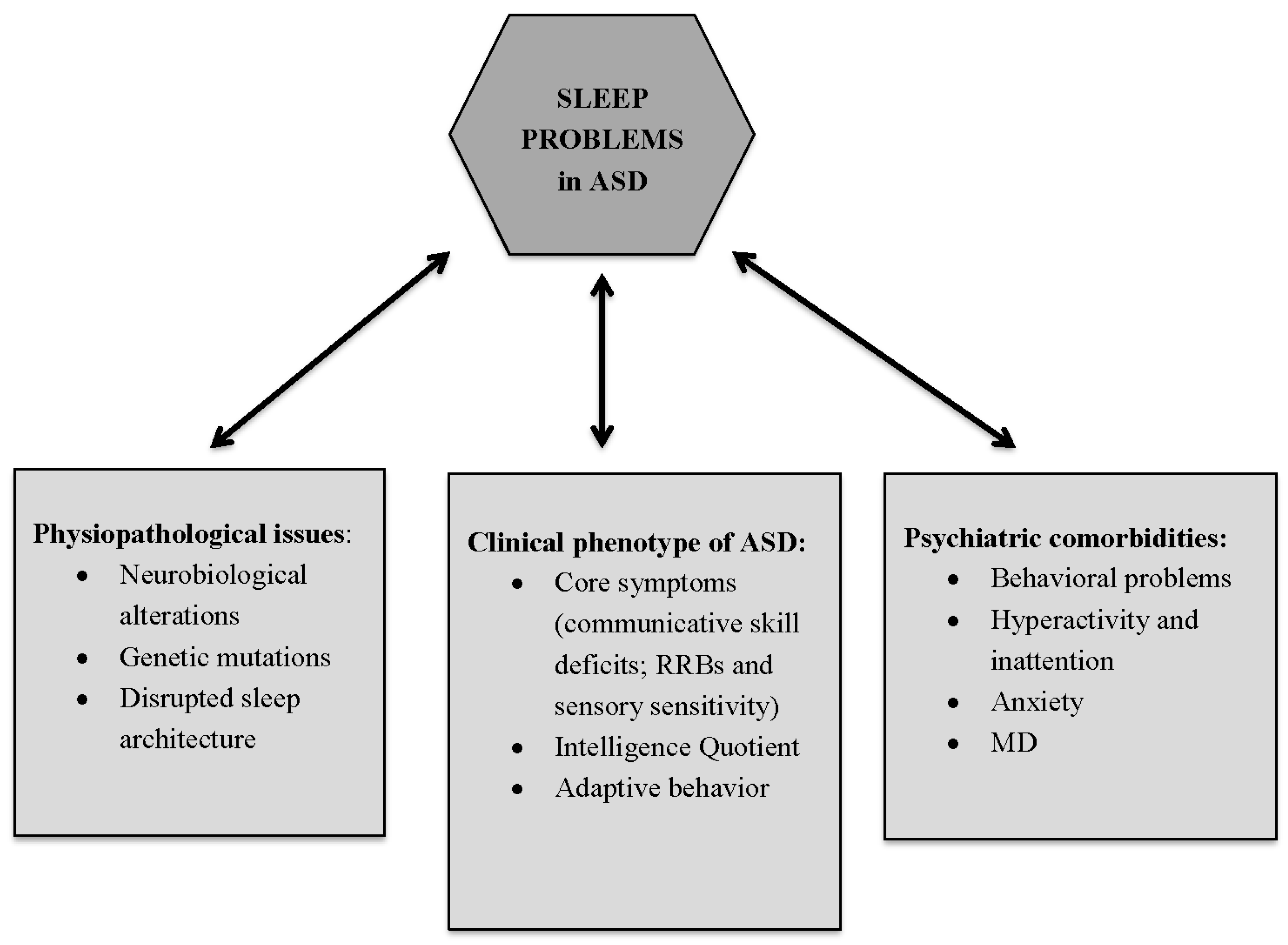
2. Are Sleep Problems a Consequence of Biological Abnormalities, Genetic Mutations, and Disrupted Sleep Architecture Present in Individuals with ASD?
3. Are Sleep Problems Intrinsic to the Clinical Phenotype of ASD?
4. ASD, Sleep Problems, and Other Psychiatric Features
4.1. Behavioral Problems
4.2. Hyperactivity and Inattention
4.3. Anxiety and Mood Disorders
5. Conclusions
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-5; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Krakowiak, P.; Goodlin-Jones, B.; Hertz-Picciotto, I.; Croen, L.A.; Hansen, R.L. Sleep problems in children with autism spectrum disorders; developmental delays, and typical development: A population-based study. J. Sleep Res. 2008, 17, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, J.S.; Gringras, P.; Blair, P.S.; Scott, N.; Henderson, J.; Fleming, P.J.; Emond, A.M. Sleep patterns in children with autistic spectrum disorders: A prospective cohort study. Arch. Dis. Child. 2014, 99, 114–118. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Maski, K.; Owens, J.A. Insomnia, parasomnias, and narcolepsy in children: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1170–1181. [Google Scholar] [CrossRef]
- Couturier, J.L.; Speechley, K.N.; Steele, M.; Norman, R.; Stringer, B.; Nicolson, R. Parental perception of sleep problems in children of normal intelligence with pervasive developmental disorders: Prevalence, severity, and pattern. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Richdale, A.L.; Schreck, K.A. Sleep problems in autism spectrum disorders: Prevalence, nature, possible biopsychosocial aetiologies. Sleep Med. Rev. 2009, 13, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Souders, M.C.; Mason, T.B.; Valladares, O.; Bucan, M.; Levy, S.E.; Mandell, D.S.; Weaver, T.E.; Pinto-Martin, J. Sleep behaviors and sleep quality in children with autism spectrum disorders. Sleep 2009, 32, 1566–1578. [Google Scholar] [CrossRef] [PubMed]
- Malow, B.E.; Katz, T.; Reynolds, A.M.; Shui, A.; Carno, M.; Connolly, H.V.; Coury, D.; Bennett, A.E. Sleep difficulties and medications in children with autism spectrum disorders: A registry study. Paediatrics 2016, 137, S98–S104. [Google Scholar] [CrossRef] [PubMed]
- Richdale, A.L.; Prior, M.R. The sleep/wake rhythm in children with autism. Eur. Child Adolesc. Psychiatry 1995, 4, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Schreck, K.A.; Mulick, J.A. Parental report of sleep problems in children with autism. J. Autism Dev. Disord. 2000, 30, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Polimeni, M.A.; Richdale, A.L.; Francis, A.J. A survey of sleep problems in autism, Asperger’s disorder and typically developing children. J. Intellect. Disabil. Res. 2005, 49, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Giannotti, F.; Cortesi, F.; Cerquiglini, A.; Miraglia, D.; Vagnoni, C.; Sebastiani, T.; Bernabei, P. An investigation of sleep characteristics, EEG abnormalities and epilepsy in developmentally regressed and non-regressed children with autism. J. Autism Dev. Disord. 2008, 38, 1888–1897. [Google Scholar] [CrossRef] [PubMed]
- Mayes, S.D.; Calhoun, S. Variables related to sleep problems in children with autism. Res. Autism Spectr. Disord. 2009, 3, 931–941. [Google Scholar] [CrossRef]
- Wiggs, L.; Stores, G. Sleep patterns and sleep disorders in children with autistic spectrum disorders: Insights using parent-reports and actigraphy. Dev. Med. Child Neurol. 2004, 46, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.E.; Richdale, A.L.; Clemmons, T.; Malow, B.A. Parental sleep concerns in autism spectrum disorders: Variations from childhood to adolescence. J. Autism Dev. Disord. 2012, 42, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Posserud, M.; Lundervold, A.J.; Hysing, M. Sleep problems in children with autism spectrum problems: A longitudinal population-based study. Autism 2012, 16, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Hodge, D.; Carollo, T.M.; Lewin, M.; Hoffman, C.D.; Sweeney, D.P. Sleep patterns in children with and without autism spectrum disorders: Developmental comparisons. Res. Dev. Disabil. 2014, 35, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, F.; Giannotti, F.; Ivanenko, A.; Johnson, K. Sleep in children with autistic spectrum disorder. Sleep Med. 2010, 11, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.A.; Schreck, K.A.; Mulik, J.A. Sleep disruption as a correlate to cognitive and adaptive behavior problems in autism spectrum disorders. Res. Dev. Disabil. 2012, 33, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Patzold, L.M.; Richdale, A.; Tonge, B.J. An investigation into sleep characteristics of children with autism and Asperger’s Disorder. J. Paediatr. Child Health 1998, 34, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Diomedi, M.; Curatolo, P.; Scalise, A.; Placidi, F.; Caretto, F.; Gigli, G.L. Sleep abnormalities in mentally retarded autistic subjects: Down’s Syndrome with mental retardation, and normal subjects. Brain Dev. 1999, 21, 548–553. [Google Scholar] [CrossRef]
- Owens, J.; Opipari, L.; Nobile, C.; Spirito, A. Sleep and daytime behaviour in children with obstructive sleep apnea and behavioural sleep disorders. Pediatrics 1998, 102, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Accardo, J.A.; Malow, B.A. Sleep, Epilpesy and Autism. Epilepsy Behav. 2015, 47, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.M.; Malow, B.A. Sleep and autism spectrum disorders. Pediatr. Clin. N. Am. 2011, 58, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Zimmerman, A.W. Sleep in Autism Spectrum Disorder and Attention Deficit Hyperactivity Disorder. Semin. Pediatr. Neurol. 2015, 22, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Monti, J.M. Serotonin control of sleep-wake behavior. Sleep Med. Rev. 2011, 15, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Geoffray, M.M.; Nicolas, A.; Speranza, M.; Georgieff, N. Are circadian rhythms new pathways to understand Autism Spectrum Disorder? J. Physiol. Paris 2016, 110, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Mindell, J.A. Pediatric insomnia. Pediatr. Clin. N. Am. 2011, 58, 555–569. [Google Scholar] [CrossRef] [PubMed]
- Veatch, O.J.; Maxwell-Horn, A.C.; Malow, B.A. Sleep in Autism Spectrum Disorders. Curr. Sleep Med. Rep. 2015, 1, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Nir, I.; Meir, D.; Zilber, N.; Knobler, H.; Hadjez, J.; Lerner, Y. Brief report: Circadian melatonin, thyroid-stimulating hormone, prolactin, and cortisol levels in serum of young adults with autism. J. Autism Dev. Disord. 1995, 25, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Kulman, G.; Lissoni, P.; Rovelli, F.; Roselli, M.G.; Brivio, F.; Sequeri, P. Evidence of pineal endocrine hypofunction in autistic children. Neuro Endocrinol. Lett. 2000, 21, 31–34. [Google Scholar] [PubMed]
- Tordjman, S.; Anderson, G.M.; Pichard, N.; Charbuy, H.; Touitou, Y. Nocturnal excretion of 6–sulphatoxymelatonin in children and adolescents with autistic disorder. Biol. Psychiatry 2005, 57, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Alonso-Alconada, D.; Besag, F.; Biran, V.; Braam, W.; Cortese, S.; Moavero, R.; Parisi, P.; Smits, M.; Van der Heijden, K. Current role of melatonin in pediatric neurology: Clinical recommendations. Eur. J. Paediatr. Neurol. 2015, 19, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Toma, C.; Rossi, M.; Sousa, I.; Blasi, F.; Bacchelli, E.; Alen, R.; Monaco, A.P.; Järvelä, I.; Maestrini, E. Is ASMT a susceptibility gene for autism spectrum disorders? A replication study in European populations. Mol. Psychiatry 2007, 12, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Cai, G.; Edelmann, L.; Goldsmith, J.E.; Cohen, N.; Nakamine, A.; Reichert, J.G.; Hoffman, E.J.; Zurawiecki, D.M.; Silverman, J.M. Multiplex ligation-dependent probe amplification for genetic screening in autism spectrum disorders: Efficient identification of known microduplications and identification of a novel microduplication in ASMT. BMC Med. Genom. 2008, 1, 50. [Google Scholar] [CrossRef] [PubMed]
- Melke, J.; Goubran Botros, H.; Chaste, P.; Betancur, C.; Nygren, G.; Anckarsäter, H.; Rastam, M.; Ståhlberg, O.; Gillberg, I.C.; Delorme, R.; et al. Abnormal melatonin synthesis in autism spectrum disorders. Mol. Psychiatry 2008, 13, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, L.; Ljunggren, E.; Bremer, A.; Pedersen, C.; Landén, M.; Thuresson, K.; Giacobini, M.; Melke, J. Mutation screening of melatonin-related genes in patients with autism spectrum disorders. BMC Med. Genom. 2010, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.B.; Grether, J.K.; Croen, L.A.; Dambrosia, J.M.; Dickens, B.F.; Jelliffe, L.L.; Hansen, R.L.; Phillips, T.M. Neuropeptides and neurotrophins in neonatal blood of children with autism or mental retardation. Ann. Neurol. 2001, 49, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Ferri, R.; Musumeci, S.A.; Del Gracco, S.; Bottitta, M.; Scuderi, C.; Miano, G.; Panerai, S.; Bertrand, T.; Grubar, J.C. Sleep in subjects with autistic disorder: A neurophysiological and psychological study. Brain Dev. 2000, 22, 88–92. [Google Scholar] [CrossRef]
- Thirumalai, S.S.; Shubin, R.A.; Robinson, R. Rapid eye movement sleep behavior disorder in children with autism. J. Child Neurol. 2002, 17, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Tani, P.; Lindberg, N.; Nieminen-von Wendt, T.; von Wendt, L.; Virkkala, J.; Appelberg, B.; Porkka-Heiskanen, T. Sleep in young adults with Asperger syndrome. Neuropsychobiology 2004, 50, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Limoges, E.; Mottron, L.; Bolduc, C.; Berthiaume, C.; Godbout, R. Atypycal sleep architecture and the autism phenotype. Brain 2005, 128, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Ferri, R.; Vittori, E.; Novelli, L.; Vignati, M.; Porfirio, M.C.; Aricò, D.; Bernabei, P.; Curatolo, P. Sleep architecture and NREM alterations in children and adolescents with Asperger syndrome. Sleep 2007, 30, 1577–1585. [Google Scholar] [CrossRef] [PubMed]
- Giannotti, F.; Cortesi, F.; Vagnoni, C.; Sebastiani, T.; Cerquiglini, A.; Bernabei, P. Polysomnographic characteristics in regressed and non-regressed autistic children. Sleep 2007, 30, 73. [Google Scholar]
- Miano, S.; Bruni, O.; Elia, M.; Trovato, A.; Smerieri, A.; Verrillo, E.; Roccella, M.; Terzano, M.G.; Ferri, R. Sleep in children with autistic spectrum disorder: A questionnaire and polysomnographic study. Sleep Med. 2007, 9, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.; Evans, V.; Hanvey, G.; Johnson, C. Assessment of Sleep in Children with Autism Spectrum Disorder. Children 2017, 4, 72. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Malow, B.; Marzec, M.; McGrew, S.; Wang, L.; Henderson, L.; Stone, W. Characterizing sleep in children with autism spectrum disorders: A multidimensional approach. Sleep 2006, 29, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Goodlin-Jones, B.L.; Sitnick, S.L.; Tang, K.; Liu, J.; Anders, T.F. The Children’s Sleep Habits Questionnaire in toddlers and preschool children. J. Dev. Behav. Pediatr. 2008, 29, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.R.; DeMand, A.; Lecavalier, L.; Smith, T.; Aman, M.G.; Foldes, E.; Scahill, L. Psychometric properties of the children’s sleep habits questionnaire in children with autism spectrum disorder. Sleep Med. 2016, 20, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Malow, B.A.; McGrew, S.G. Sleep disturbances and autism. Sleep Med. Clin. 2008, 3, 479–488. [Google Scholar] [CrossRef]
- Kotagal, S.; Broomall, E. Sleep in children with Autism Spectrum Disorder. Pediatr. Neurol. 2012, 47, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef]
- Harvey, A.G.; Tang, N.K.; Browning, L. Cognitive approaches to insomnia. Clin. Psychol. Rev. 2005, 25, 593–611. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, L.V.; Kobak, K.; Swanson, A.; Wallace, L.; Warren, Z.; Stone, W.L. Enhancing Interactions during Daily Routines: A Randomized Controlled Trial of a Web-Based Tutorial for Parents of Young Children with ASD. Autism Res. 2018, 11, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.; Lane, S.J.; Thacker, L. Sensory processing, physiological stress, and sleep behaviors in children with and without autism spectrum disorders. OTJR 2012, 32, 246–257. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Petroski, G.F. Sleep problems in children with autism spectrum disorder: Examining the contributions of sensory over-responsivity and anxiety. Sleep Med. 2015, 16, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Veatch, J.O.; Sutcliffe, J.S.; Warren, Z.E.; Keenan, B.T.; Potter, M.H.; Malow, B.A. Shorter Sleep Duration is Associated with Social Impairment and Comorbidities in ASD. Autism Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.E.; Surdyka, K.; Cuevas, R.; Adkins, K.; Wang, L.; Malow, B.A. Defining the sleep phenotype in children with autism. Dev. Neuropsychol. 2009, 34, 560–573. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Conduit, R.; Lockley, S.W.; Rajaratnam, S.M.W.; Cornish, K.M. The relationship between sleep and behavior in autism spectrum disorder (ASD): A review. J. Neurodev. Disord. 2014, 6, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadini, C.C.; Lamonica, D.A.; Fett-Conte, A.C.; Osorio, E.; Zuculo, G.M.; Giacheti, C.M.; Pinato, L. Influence of sleep disorders on the behavior of individuals with autism spectrum disorder. Front. Hum. Neurosci. 2015, 9, 347. [Google Scholar] [CrossRef] [PubMed]
- May, T.; Cornish, K.; Conduit, R.; Rajaratnam, S.M.; Rinehart, N.J. Sleep in high-functioning children with autism: Longitudinal developmental change and associations with behavior problems. Behav. Sleep Med. 2015, 13, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Hirata, I.; Mohri, I.; Kato-Nishimura, K.; Tachibana, M.; Kuwada, A.; Kagitani-Shimono, K.; Ohno, Y.; Ozono, K.; Taniike, M. Sleep problems are more frequent and associated with problematic behaviors in preschoolers with autism spectrum disorder. Res. Dev. Disabil. 2016, 49–50, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, M.O.; Sohl, K. Sleep and behavioral problems in children with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 1906–1915. [Google Scholar] [CrossRef] [PubMed]
- Malow, B.A. Sleep disorders, epilepsy, and autism. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Hollway, J.A.; Aman, M.G. Sleep correlates of pervasive developmental disorders: A review of the literature. Res. Dev. Disabl. 2011, 32, 1399–1421. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.; Leader, G.; Healy, O. An investigation of comorbid psychological disorders, sleep problems, gastrointestinal symptoms and epilepsy in children and adolescents with Autism Spectrum Disorder. Res. Autism Spectr. Disord. 2013, 7, 35–42. [Google Scholar] [CrossRef]
- Tureck, K.; Matson, J.L.; May, A.; Turygin, N. Externalizing and tantrum behaviours in children with ASD and ADHD compared to children with ADHD. Dev. Neurorehabil. 2013, 16, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, J.M.; Arnold, E.B.; Keene, A.C.; Collier, A.B.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. Frequency and clinical correlates of sleep-related problems among anxious youth with autism spectrum disorders. Child Psychiatry Hum. Dev. 2015, 46, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Postorino, V.; Sharp, W.G.; McCracken, C.E.; Bearss, K.; Burrell, T.L.; Evans, A.N.; Scahill, L. A Systematic Review and Meta-analysis of Parent Training for Disruptive Behavior in Children with Autism Spectrum Disorder. Clin. Child Fam. Psychol. Rev. 2017, 20, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Mugno, D.; Ruta, L.; D’Arrigo, V.G.; Mazzone, L. Impairment of quality of life in parents of children and adolescents with pervasive developmental disorder. Health Qual. Life Outcomes 2007, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Dabrowska, A.; Pisula, E. Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. J. Intellect. Disabil. Res. 2010, 54, 266–280. [Google Scholar] [CrossRef] [PubMed]
- Sikora, D.M.; Johnson, K.; Clemons, T.; Katz, T. The relationship between sleep problems and daytime behavior in children of different ages with autism spectrum disorders. Pediatrics 2012, 130 (Suppl. 2), S83–S90. [Google Scholar] [CrossRef] [PubMed]
- SPark, S.; Cho, S.C.; Cho, I.H.; Kim, B.N.; Kim, J.W.; Shin, M.S.; Chung, U.S.; Park, T.W.; Son, J.W.; Yoo, H.J. Sleep Problems and Their Correlates and Comorbid Psychopathology of Children with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2012, 6, 1068–1072. [Google Scholar]
- Malow, B.A.; Byars, K.; Johnson, K.; Weiss, S.; Bernal, P.; Goldman, S.E.; Panzer, R.; Coury, D.L.; Glaze, D.G. A practice pathway for the identification, evaluation, and management of insomnia in children and adolescents with autism spectrum disorders. Pediatrics 2012, 130, S106–S124. [Google Scholar] [CrossRef] [PubMed]
- Friman, P.C.; Hoff, K.E.; Schnoes, C.; Freeman, K.A.; Woods, D.W.; Blum, N. The bedtime pass: An approach to bedtime crying and leaving the room. Arch. Pediatr. Adolesc. Med. 1999, 153, 1027–1029. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.A.; Friman, P.C.; Fruzzetti, A.E.; MacAleese, K. Brief report: Evaluating the Bedtime Pass Program for child resistance to bedtime—A randomized, controlled trial. J. Pediatr. Psychol. 2007, 32, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Weiskop, S.; Richdale, A.; Matthews, J. Behavioural treatment to reduce sleep problems in children with autism or fragile X syndrome. Dev. Med. Child Neurol. 2005, 47, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.R.; Turner, K.S.; Foldes, E.; Brooks, M.M.; Kronk, R.; Wiggs, L. Behavioral parent training to address sleep disturbances in young children with autism spectrum disorder: A pilot trial. Sleep Med. 2013, 14, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population derived sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- DeVincent, C.J.; Gadow, K.D.; Delosh, D.; Geller, L. Sleep disturbance and its relation to DSM-IV psychiatric symptoms in preschool-age children with pervasive developmental disorder and community controls. J. Child Neurol. 2007, 22, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Sangal, R.B.; Owens, J.; Allen, A.J.; Sutton, V.; Schuh, K.; Kelsey, D. Effects of atomoxetine and methylphenidate on sleep in children with ADHD. Sleep 2006, 29, 1573–1585. [Google Scholar] [CrossRef] [PubMed]
- Van Steensel, F.J.; Bögels, S.M.; Perrin, S. Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clin. Child Fam. Psychol. Rev. 2011, 14, 302–317. [Google Scholar] [CrossRef] [PubMed]
- Monk, C.; Kovelenko, P.; Ellman, L.M.; Sloan, R.P.; Bagiella, E.; Gorman, J.M.; Pine, D.S. Enhanced stress reactivity in paediatric anxiety disorders: Implications for future cardiovascular health. Int. J. Neuropsychopharmacol. 2001, 4, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Krämer, M.; Seefeldt, W.L.; Heinrichs, N.; Tuschen-Caer, B.; Schmitz, J.; Wolf, O.T.; Blechert, J. Subjective, autonomic, and endocrine reactivity during social stress in children with social phobia. J. Abnorm. Child Psychol. 2012, 40, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Jones, C.R.; Pickles, A.; Happé, F.; Baird, G.; Charman, T. Severe mood problems in adolescents with autism spectrum disorder. J. Child Psychol. Psychiatry 2012, 53, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Gold, A.K.; Sylvia, L.G. The role of sleep in bipolar disorder. Nat. Sci. Sleep 2016, 8, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Ginsburg, G.S.; Kingery, J.N. Sleep-related problems among children and adolescents with anxiety disorders. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Storch, E.A.; Murphy, T.K.; Lack, C.W.; Geffken, G.R.; Jacob, M.L.; Goodman, W.K. Sleep-related problems in pediatric obsessive–compulsive disorder. J. Anxiety Disord. 2008, 22, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Chase, R.M.; Pincus, D.B. Sleep-related problems in children and adolescents with anxiety disorders. Behav. Sleep Med. 2011, 9, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.; Linton, S.J. The role of anxiety and depression in the development of insomnia: Cross-sectional and prospective analyses. Psychol. Health 2006, 21, 383–397. [Google Scholar] [CrossRef]
- Johnson, E.O.; Roth, T.; Breslau, N. The association of insomnia with anxiety disorders and depression: Exploration of the direction of risk. J. Psychiatr. Res. 2006, 40, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Tani, P.; Lindberg, N.; Nieminen-von Wendt, T.; von Wendt, L.; Alanko, L.; Appelberg, B.; Porkka-Heiskanen, T. Insomnia is a frequent finding in adults with Asperger syndrome. BMC Psychiatry 2003, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paavonen, E.J.; Vehkalahti, K.; Vanhala, R.; von Wendt, L.; Nieminen-von Wendt, T.; Aronen, E.T. Sleep in children with Asperger syndrome. J. Autism Dev. Disord. 2008, 38, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Quine, L. Sleep problems in children with mental handicap. J. Ment. Defic. Res. 1991, 35, 269–290. [Google Scholar] [CrossRef] [PubMed]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzone, L.; Postorino, V.; Siracusano, M.; Riccioni, A.; Curatolo, P. The Relationship between Sleep Problems, Neurobiological Alterations, Core Symptoms of Autism Spectrum Disorder, and Psychiatric Comorbidities. J. Clin. Med. 2018, 7, 102. https://doi.org/10.3390/jcm7050102
Mazzone L, Postorino V, Siracusano M, Riccioni A, Curatolo P. The Relationship between Sleep Problems, Neurobiological Alterations, Core Symptoms of Autism Spectrum Disorder, and Psychiatric Comorbidities. Journal of Clinical Medicine. 2018; 7(5):102. https://doi.org/10.3390/jcm7050102
Chicago/Turabian StyleMazzone, Luigi, Valentina Postorino, Martina Siracusano, Assia Riccioni, and Paolo Curatolo. 2018. "The Relationship between Sleep Problems, Neurobiological Alterations, Core Symptoms of Autism Spectrum Disorder, and Psychiatric Comorbidities" Journal of Clinical Medicine 7, no. 5: 102. https://doi.org/10.3390/jcm7050102