Influence of the Self-Perception of Old Age on the Effect of a Healthy Aging Program

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Subjects
2.2. Assessment of Self-Perception of Old Age
2.3. Assessment of Anthropometric Measurements and Blood Pressure
2.4. Assessment of Biochemical Parameters
2.5. “Healthy Aging Program” Workshop
2.6. Statistical Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; WHO: Geneva, Switzerland, 2015; Available online: http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf (accessed on 27 March 2018).
- Instituto Nacional de Estadística y Geografía. Estadísticas a Propósito Deldía Mundial de la Población (11 de Julio). 7 de Julio de 2016; INEGI: Aguascalientes, Mexico, 2016; Available online: http://www.inegi.org.mx/saladeprensa/aproposito/2016/poblacion2016_0.pdf (accessed on 27 March 2018).
- Gutiérrez, J.P.; Rivera-Dommarco, J.; Shamah-Levy, T.; Villalpando-Hernandez, S.; Franco, A.; Cuevas-Nasu, L.; Romero-Martínez, M.; Hernández-Ávila, M. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales; Instituto Nacional de Salud Pública (MX): Cuernavaca, Mexico, 2013; Available online: http://ensanut.insp.mx/informes/ENSANUT2012ResultadosNacionales.pdf (accessed on 27 March 2018).
- Martínez-Maldonado, M.L.; Correa-Muñoz, E.; Mendoza-Núñez, V.M. Program of active aging in a rural Mexican community: A qualitative approach. BMC Public Health 2007, 7, 276. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.M.; Martínez-Maldonado, M.L.; Correa-Muñoz, E. Implementation of an active aging model in Mexico for prevention and control of chronic diseases in the elderly. BMC Geriatr. 2009, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, M.A.; Arronte-Rosales, A.; Mendoza-Núñez, V.M. Effect of a self-care program on oxidative stress and cognitive function in an older Mexican urban-dwelling population. J. Nutr. Health Aging 2009, 13, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballesteros, R.; Caprara, M.; Schettini, R.; Bustillos, A.; Mendoza-Nuñez, V.; Orosa, T. Effects of university programs for older adults: Changes in cultural and group stereotype, self-perception of aging, and emotional balance. Educ. Gerontol. 2013, 39, 119–131. [Google Scholar] [CrossRef]
- Levy, B.R.; Slade, M.D.; Kasl, S.V. Longitudinal benefit of positive self perceptions of aging on functional health. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, 409–417. [Google Scholar] [CrossRef]
- Levy, B.R.; Slade, M.D.; Kunkel, S.R.; Kasl, S.V. Longevity increased by positive self-perceptions of aging. J. Pers. Soc. Psychol. 2002, 83, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.R.; Slade, M.D.; Murphy, T.E.; Gill, T.M. Association between positive age stereotypes and recovery from disability in older persons. JAMA 2012, 308, 1972–1973. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Pozo, M.R.; Torres, N.M.; Coronado, A.O.; Herrera, G.A.; Castillo, N.P.; Sánchez, V.A. Actitudes Negativas Hacia la vejez en Población Mexicana: Aspectos Psicométricos de una Escala; González-Celis, R.A.L., Ed.; Evaluación en Psicogerontología; Manual Moderno: Mexico City, Mexico, 2009; pp. 1–16. [Google Scholar]
- Mendoza-Núñez, V.M.; Martínez-Maldonado, M.L.; Vargas-Guadarrama, L.A. Gerontología Comunitaria; Facultad de Estudios Superiores Zaragoza, UNAM: Mexico City, Mexico, 2004; p. 522. [Google Scholar]
- Sundsli, K.; Söderhamn, U.; Espnes, G.A.; Söderhamn, O. Ability for self-care in urban living older people in southern Norway. J. Multidisci. Healthc. 2012, 5, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprara, M.; Fernández-Ballesteros, R.; Alessandri, G. Promoting aging well: Evaluation of Vital-Aging Multimedia program in Madrid, Spain. Health Promot. Int. 2016, 31, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Lima, K.C.; Caldas, C.P.; Veras, R.P.; Correa, R.F.; Bonfada, D.; de Souza, D.B.; Jerez-Roig, J. Health promotion and education: A study of the effectiveness of programs focusing on the aging process. Int. J. Health Serv. 2017, 47, 550–570. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.M.; Martínez-Maldonado, M.L.; Vargas-Guadarrama, L.A. Viejismo: Prejuicios y Estereotipos de la Vejez; FES Zaragoza, UNAM: Mexico City, Mexico, 2008; pp. 33–75. [Google Scholar]
- Dionigi, R.A. Stereotypes of aging: Their effects on the health of older adults. J. Geriatr. 2015. [Google Scholar] [CrossRef]
- Freeman, A.T.; Santini, Z.I.; Tyrovolas, S.; Rummel-Kluge, C.; Haro, J.M.; Koyanagi, A. Negative perceptions of ageing predict the onset and persistence of depression and anxiety: Findings from a prospective analysis of the Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2016, 199, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Moser, C.; Spagnoli, J.; Santos-Eggimann, B. Self-perception of aging and vulnerability to adverse outcomes at the age of 65–70 years. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.; Chol, H.; Lee, C.; Cha, M.; Jo, I. Association between knowledge and attitude about aging and life satisfaction among older Koreans. Asian Nurs. Res. 2012, 6, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Yaghoobzadeh, A.; Sharif Nia, H.; Pahlevan Sharif, S.; Hosseinigolafshani, S.Z.; Mohammadi, F.; Oveisi, S.; Allen, K.A. Role of sex, socioeconomic status, and emotional support in predicting aging perception among older adults. Int. J. Aging Hum. Dev. 2017, 1. [Google Scholar] [CrossRef] [PubMed]
- Moreno, X.; Sánchez, H.; Huerta, M.; Albala, C.; Márquez, C. Social representations of older adults among Chilean elders of three cities with different historical and sociodemographic background. J. Cross Cult. Gerontol. 2016, 31, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.O. Ageism as a risk factor for chronic disease. Gerontologist 2015. [Google Scholar] [CrossRef] [PubMed]
- Ory, M.; Kinney Hoffman, M.; Hawkins, M.; Sanner, B.; Mockenhaupt, R. Challenging aging stereotypes: Strategies for creating a more active society. Am. J. Prev. Med. 2003, 25 (Suppl. 2), 164–171. [Google Scholar] [CrossRef]
- Fernández-Ballesteros, R.; Bustillos, A.; Huici, C. Positive perception of aging and performance in a memory task: Compensating for Stereotype Threat? Exp. Aging Res. 2015, 41, 410–425. [Google Scholar] [CrossRef] [PubMed]
- Bodner, E. On the origins of ageism among older and younger adults. Int. Psychogeriatr. 2009, 21, 1003–1014. [Google Scholar] [CrossRef] [PubMed]
- Stephan, Y.; Sutin, A.R.; Terracciano, A. How old do you feel? The role of age discrimination and biological aging in subjective age. PLoS ONE 2015, 10, e0119293. [Google Scholar] [CrossRef] [PubMed]
- Palmore, E. Ageism comes of age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 873–875. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Ruvalcaba, N.M.; Fernández-Ballesteros, R. Effectiveness of the Vital Aging program to promote active aging in Mexican older adults. Clin. Interv. Aging 2016, 11, 1631–1644. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cuevas, R.; Doubova, S.V.; Bazaldúa-Merino, L.A.; Reyes-Morales, H.; Martínez, D.; Karam, R.; Gamez, C.; Muñoz-Hernández, O. A social health services model to promote active ageing in Mexico: Design and evaluation of a pilot programme. Ageing Soc. 2015, 35, 1457–1480. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. | Item |
|---|---|
| 1 | It makes me sad to be elderly. |
| 2 | It is unpleasant to have wrinkles. |
| 3 | Old age scares me. |
| 4 | I do not like having graying hair. |
| 5 | The elderly have bad breath. |
| 6 | It is awful losing mental abilities with old age. |
| 7 | Older people become fools and repeat themselves. |
| 8 | With aging comes sadness and loneliness. |
| 9 | Women with graying hair are unattractive. |
| 10 | Older people are abandoned. |
| 11 | Men with age-related baldness are unattractive. |
| 12 | Elderly women should take steps to look younger. |
| 13 | Being old is depressing. |
| 14 | Older people are smelly. |
| 15 | It is easy to fool old people. |
| 16 | With aging, independence is lost. |
| 17 | The elderly cause many problems. |
| 18 | The elderly do not have skills such as driving cars. |
| 19 | The elderly are greedy. |
| 20 | Nursing homes are depressing. |
| 21 | I fear being useless when I am old. |
| Topics |
|---|
|
| Frequencies, n = 64 (%) | |
|---|---|
| Age (mean ± SD) | 66 ± 3 |
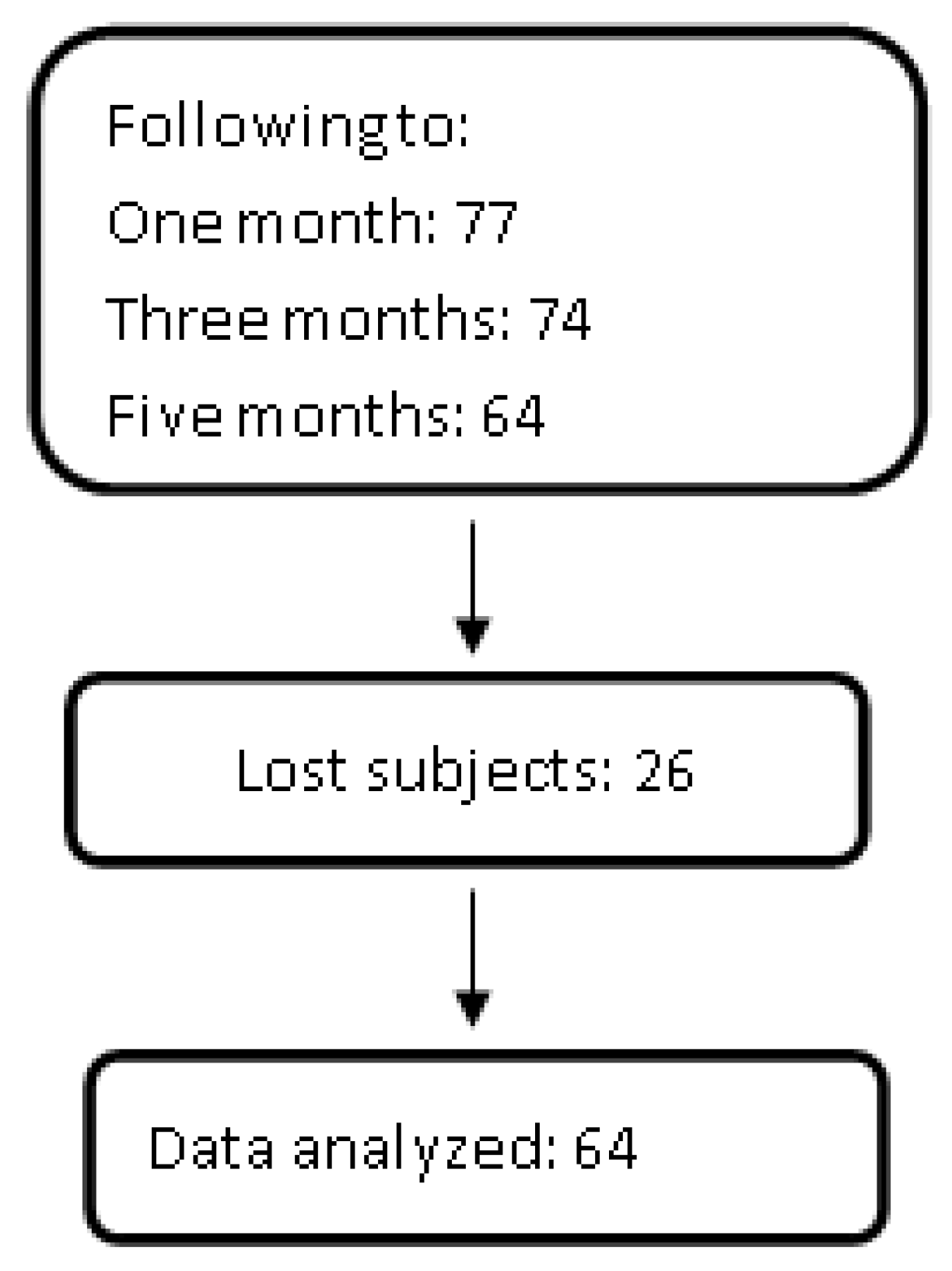
| 60 a 69 years | 49 (77) |
| ≥70 years | 15 (23) |
| Sex | |
| Woman | 52 (81) |
| Man | 12 (19) |
| Civil status | |
| Single | 20 (31) |
| Married | 30 (47) |
| Widower | 14 (22) |
| School years (mean ± SD) | 7 ± 5 |
| Literacy | 3 (4) |
| 1–6 years | 35 (55) |
| 7–9 years | 11 (18) |
| ≥10 years | 15 (23) |
| Diagnosis | 23 (36) |
| Healthy | 9 (15) |
| DM | 13 (29) |
| HBP | 19 (30) |
| DM + HBP |
| Self-Perception of Aging | Baseline | Post-Intervention |
|---|---|---|
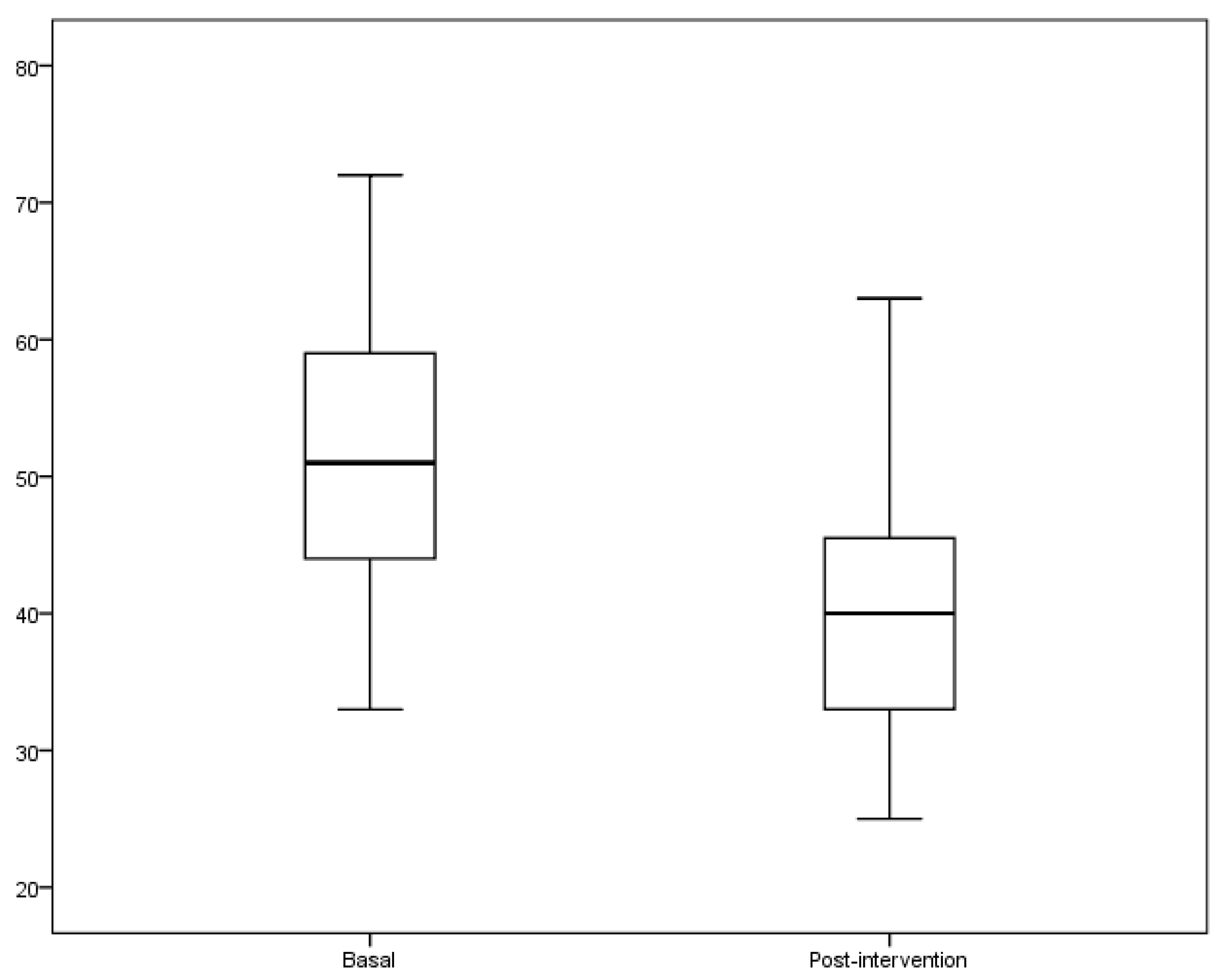
| Total (n = 64) | 51 ± 10 | 40 ± 9 *** |
| Q1 (n = 18) | 39 ± 3 | 33 ± 4 *** |
| Q2 (n = 17) | 48 ± 2 | 46 ± 5 |
| Q3 (n = 10) | 55 ± 1 | 40 ± 9 *** |
| Q4 (n = 19) | 63 ± 4 | 46 ± 10 *** |
| Total n = 64 | Q1 (n = 18) Positive Self-Perception | Q4 (n = 19) Negative Self-Perception | |
|---|---|---|---|
| Glucose (mg/dL) | |||
| Baseline | 137 ± 50 | 134 ± 47 | 144 ± 46 |
| Post-intervention | 124 ± 45 ** | 114 ± 29 * | 137 ± 53 |
| Cholesterol (mmo/dL) | |||
| Baseline | 224 ± 42 | 223 ± 37 | 234 ± 35 |
| Post-intervention | 218 ± 44 | 202 ± 41 * | 229 ± 38 |
| Tryglicerides (mg/dL) | |||
| Baseline | 165 ± 92 | 139 ± 52 | 160 ± 92 |
| Post-intervention | 159 ± 75 | 132 ± 66 | 158 ± 73 |
| LDL (mg/dL) | |||
| Baseline | 153 ± 48 | 159 ± 40 | 164 ± 56 |
| Post-intervention | 130 ± 36 ** | 116 ± 32 * | 140 ± 32 |
| HDL (mg/dL) | |||
| Baseline | 56 ± 15 | 53 ± 14 | 58 ± 14 |
| Post-intervention | 58 ± 14 | 58 ± 13 | 61 ± 17 |
| Weight (kg) | |||
| Baseline | 67 ± 12 | 66 ± 13 | 66 ± 10 |
| Post-intervention | 66 ± 10 | 65 ± 11 | 66 ± 10 |
| BMI (weight/height2) | |||
| Baseline | 29 ± 4 | 27 ± 3 | 30 ± 5 |
| Post-intervention | 28 ± 3 * | 27 ± 3 | 29 ± 4 |
| SBP | |||
| Baseline | 131 ± 20 | 124 ± 7 | 133 ± 15 |
| Post-intervention | 119 ± 12 ** | 115 ± 7 * | 124 ± 9 ** |
| DBP | |||
| Baseline | 76 ± 9 | 74 ± 7 | 74 ± 10 |
| Post-intervention | 73 ± 7 * | 72 ± 8 | 75 ± 6 |
| Healthy Lifestyles (n = 64) | Baseline | Post-Intervention | p Value |
|---|---|---|---|
| Health care | 7.7 ± 1.2 | 8.2 ± 1.2 | 0.040 |
| Self-esteem | 8.3 ± 1.1 | 8.4 ± 1.5 | 0.814 |
| Healthy food | 7.9 ± 1.3 | 8.1 ± 1.4 | 0.216 |
| Physical exercise | 8.0 ± 1.6 | 8.5 ± 1.2 | 0.21 |
| Sleep hygiene | 7.4 ± 2.0 | 8.2 ± 1.5 | 0.015 |
| Body hygiene | 8.4 ± 1.4 | 8.9 ± 1.1 | 0.060 |
| Healthy environmental | 8.4 ± 1.4 | 8.5 ± 1.3 | 0.585 |
| Baseline | Post-Intervention | p Value | |
|---|---|---|---|
| Positive self-perception of old age (score ≤ 44) | |||
| Health care | 8.0 ± 1.0 | 8.9 ± 0.8 | 0.004 |
| Self-esteem | 8.0 ± 0.8 | 9.2 ± 1.0 | 0.008 |
| Healthy food | 7.9 ± 1.0 | 8.5 ± 1.0 | 0.145 |
| Physical exercise | 8.4 ± 1.0 | 8.4 ± 1.0 | 1.000 |
| Sleep hygiene | 7.7 ± 1.0 | 8.5 ± 1.0 | 0.154 |
| Body hygiene | 8.9 ± 1.0 | 9.2 ± 1.0 | 0.205 |
| Healthy environmental | 8.9 ± 1.0 | 9.0 ± 1.0 | 0.668 |
| Negative self-perception of old age (score ≥ 59) | |||
| Health care | 7.0 ± 1.0 | 7.0 ± 1.0 | 1.000 |
| Self-esteem | 8.0 ± 1.0 | 8.0 ± 1.0 | 1.000 |
| Healthy food | 8.0 ± 1.0 | 7.0 ± 1.0 | 0.440 |
| Physical exercise | 8.0 ± 1.0 | 8.0 ± 1.0 | 1.000 |
| Sleep hygiene | 6.0 ± 2.0 | 7.0 ± 1.0 | 0.538 |
| Body hygiene | 8.0 ± 1.0 | 8.0 ± 1.0 | 1.000 |
| Healthy environmental | 8.0 ± 1.0 | 8.0 ± 1.0 | 1.000 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza-Núñez, V.M.; Sarmiento-Salmorán, E.; Marín-Cortés, R.; Martínez-Maldonado, M.D.l.L.; Ruiz-Ramos, M. Influence of the Self-Perception of Old Age on the Effect of a Healthy Aging Program. J. Clin. Med. 2018, 7, 106. https://doi.org/10.3390/jcm7050106
Mendoza-Núñez VM, Sarmiento-Salmorán E, Marín-Cortés R, Martínez-Maldonado MDlL, Ruiz-Ramos M. Influence of the Self-Perception of Old Age on the Effect of a Healthy Aging Program. Journal of Clinical Medicine. 2018; 7(5):106. https://doi.org/10.3390/jcm7050106
Chicago/Turabian StyleMendoza-Núñez, Víctor Manuel, Elia Sarmiento-Salmorán, Regulo Marín-Cortés, María De la Luz Martínez-Maldonado, and Mirna Ruiz-Ramos. 2018. "Influence of the Self-Perception of Old Age on the Effect of a Healthy Aging Program" Journal of Clinical Medicine 7, no. 5: 106. https://doi.org/10.3390/jcm7050106